
Beyond Seasickness: A Motivated Call for a New Motion Sickness Standard across Motion Environments

{kind=link}
Abstract
:1. Introduction
1.1. Origin and Historical Background of the ISO 2631-1 Standard
1.2. Predictive Model of Seasickness
1.3. Limitations of the Current Standard
2. Underlying Mechanism of Motion Sickness
2.1. Theories
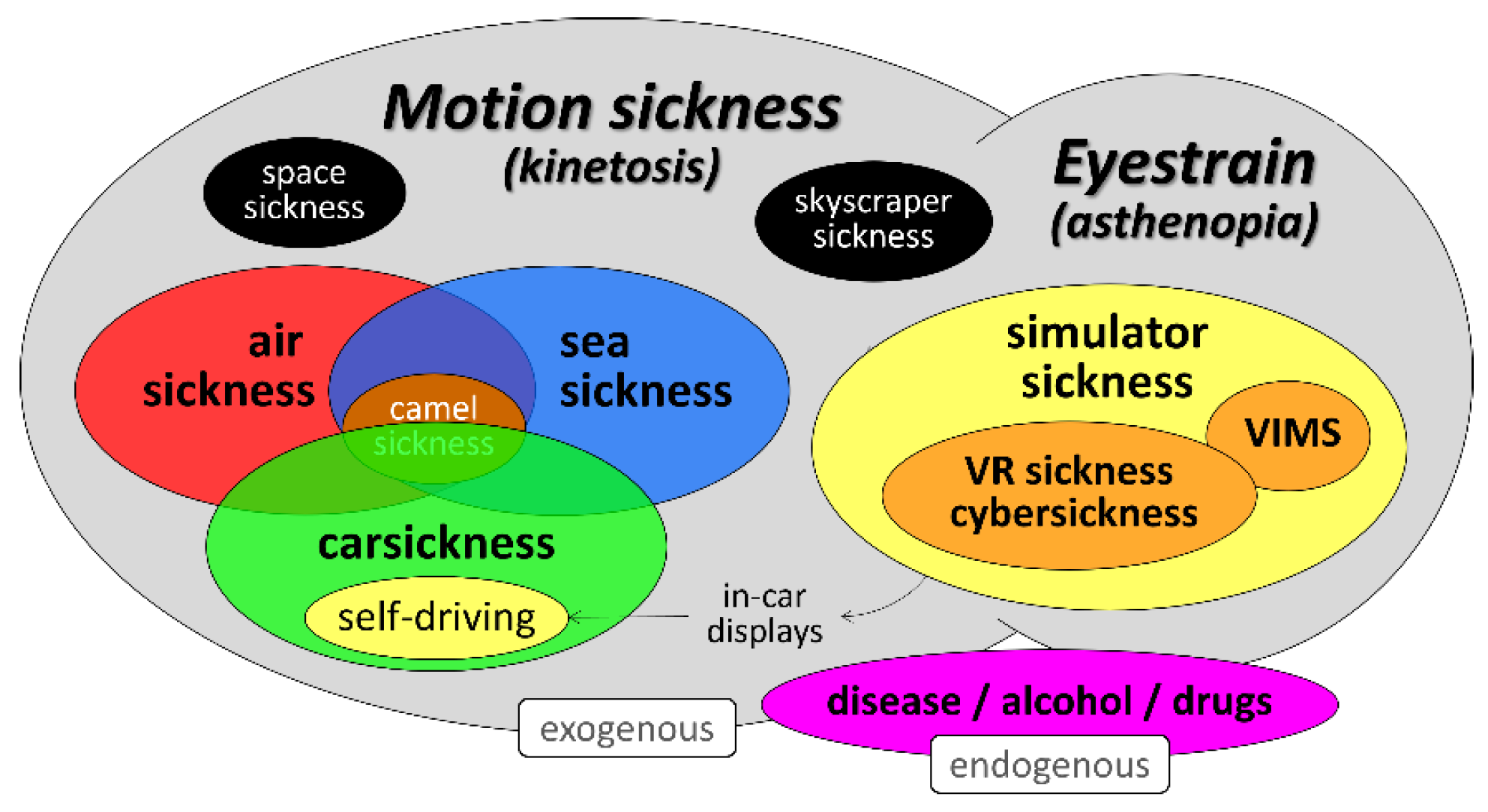
2.2. Sickness versus Eyestrain
3. Methodological Considerations
3.1. Measuring Motion Sickness
3.2. Motion Sickness Susceptibility
3.2.1. Gender
3.2.2. Age
3.2.3. Measuring Susceptibility
3.2.4. Impact of Susceptibility
4. Knowledge Gaps and Steps towards an Enhanced Motion Sickness Standard
4.1. Motion Axes and Interactions
4.1.1. Linear Accelerations
4.1.2. Angular Motions
4.1.3. Interactions
4.2. Temporal Dynamics
4.3. Modulating Factors
4.3.1. Vision
4.3.2. Anticipation and Expectation
4.3.3. Body Orientation and Reclination
5. Discussion and Conclusions
- Contribution of inertial acceleration amplitude and frequency along vertical and horizontal axes, including potential interactions;
- Contribution of visual (image) factors (a simple statement that may even be more complex than determining the contribution of the inertial factors);
- Prediction of sickness including the pre-emesis symptoms;
- Integration of various forms of motion sickness into one single prediction model;
- Time course of motion sickness (accumulation, habituation, recovery, retention);
- Inclusion of individual differences;
- Standardization of methodology for motion sickness research (sickness rating scales, motion stimuli, and individual difference and susceptibility ratings);
- Contribution of moderating factors besides vision, such as posture/orientation, anticipation/predictability, temperature, odors, etc.
Author Contributions
Funding
Conflicts of Interest
References
- ISO 2631-1; Mechanical Vibration and Shock—Evaluation of Human Exposure to Whole-Body Vibration—Part 1: General Requirements. International Organization for Standardization: Geneva, Switzerland, 1997.
- Lackner, J.R. Motion sickness: More than nausea and vomiting. Exp. Brain Res. 2014, 232, 2493–2510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertolini, G.; Straumann, D. Moving in a Moving World: A Review on Vestibular Motion Sickness. Front. Neurol. 2016, 7, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proietti, P.; Allsop, J.; Bloch, M.; Bos, J.E.; Burov, O.; Clement, D.; French, J.; Kirollos, R.; Lawson, B.D.; Leoncini, P.; et al. Guidelines for Mitigating Cybersickness in Virtual Reality Systems; Technical Report NATO Science and Technology Organisation, Human Factors and Medicine & Modeling and Simulation Group Specialist Team 323 2021 NATO STO-TR-HFM-MSG-323; NATO: Brussels, Belgium, 2021. [Google Scholar]
- Keshavarz, B.; Golding, J.F. Motion sickness: Current concepts and management. Curr. Opin. Neurol. 2022, 35, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Alexander, S.J.; Cotzin, M.; Hill, C.J., Jr.; Ricciuti, E.A.; Wendt, G.R. Weslean University studies of motion sickness: I. The effects of variation of time intervals between accelerations upon sickness rates. J. Psychol. 1945, 19, 49–62. [Google Scholar] [CrossRef]
- Alexander, S.J.; Cotzin, M.; Hill, C.J., Jr.; Ricciuti, E.A.; Wendt, G.R. Weslean University studies of motion sickness: II. A second approach to the problem of the effects of the variation of time intervals between accelerations upon sickness rates. J. Psychol. 1945, 19, 63–68. [Google Scholar] [CrossRef]
- Alexander, S.J.; Cotzin, M.; Hill, C.J., Jr.; Ricciuti, E.A.; Wendt, G.R. Weslean University studies of motion sickness: III. The effects of various accelerations upon sickness rates. J. Psychol. 1945, 20, 3–8. [Google Scholar] [CrossRef]
- Alexander, S.J.; Cotzin, M.; Hill, C.J., Jr.; Ricciuti, E.A.; Wendt, G.R. Weslean University studies of motion sickness: IV. The effects of waves containing two acceleration levels upon sickness. J. Psychol. 1945, 20, 9–18. [Google Scholar] [CrossRef]
- Alexander, S.J.; Cotzin, M.; Hill, C.J., Jr.; Ricciuti, E.A.; Wendt, G.R. Weslean University studies of motion sickness: V. Incidence of sickness at various hours of the day. J. Psychol. 1945, 20, 19–24. [Google Scholar] [CrossRef]
- Alexander, S.J.; Cotzin, M.; Hill, C.J., Jr.; Ricciuti, E.A.; Wendt, G.R. Weslean University studies of motion sickness: VI. Prediction of sickness on a vertical acceleration by means of a motion sickness history questionnaire. J. Psychol. 1945, 20, 25–30. [Google Scholar] [CrossRef]
- Alexander, S.J.; Cotzin, M.; Hill, C.J., Jr.; Ricciuti, E.A.; Wendt, G.R. Weslean University studies of motion sickness: VII. The effects of sickness upon performance. J. Psychol. 1945, 20, 31–39. [Google Scholar] [CrossRef]
- Alexander, S.J.; Cotzin, M.; Klee, M.; Wendt, G.R. Studies of motion sickness. XVI. The effects upon sickness rates of waves of various frequencies but identical acceleration. J. Exp. Psychol. 1947, 37, 440–448. [Google Scholar] [CrossRef]
- O’Hanlon, J.F.; McCauley, M.E. Motion sickness incidence as a function of the frequency and acceleration of vertical sinusoidal motion. Aerosp. Med. 1974, 45, 366–369. [Google Scholar]
- McCauley, M.E.; Royal, J.W.; Wylie, C.D.; O’Hanlon, J.F.; Mackie, R.R. Motion Sickness Incidence: Exploratory Studies of Habituation, Pitch and Roll, and the Refinement of a Mathematical Model; Technical Report; Human Factors Research, Inc.: Goleta, CA, USA, 1976; Volume 1733–2, pp. 1–61. [Google Scholar]
- Guignard, J.C.; McCauley, M.E. Motion sickness incidence induced by complex periodic waveforms. Aviat. Space Environ. Med. 1982, 53, 554–563. [Google Scholar] [CrossRef]
- Lawther, A.; Griffin, M.J. The motion of a ship at sea and the consequent motion sickness amongst passengers. Ergonomics 1986, 29, 535–552. [Google Scholar] [CrossRef]
- Lawther, A.; Griffin, M.J. Prediction of the incidence of motion sickness from the magnitude, frequency and duration of vertical oscillation. J. Acoust. Soc. Am. 1987, 82, 957–966. [Google Scholar] [CrossRef] [Green Version]
- Lawther, A.; Griffin, M.J. A survey of the occurrence of motion sickness amongst passengers at sea. Aviat. Space Environ. Med. 1988, 59, 399–406. [Google Scholar]
- Lawther, A.; Griffin, M.J. Motion sickness and motion characteristics of vessels at sea. Ergonomics 1988, 31, 1373–1394. [Google Scholar] [CrossRef]
- BS 6841; Guide to Measurement and Evaluation of Human Exposure to Whole-Body Mechanical Vibration and Repeated Shock. British Standards Institution: London, UK, 2020.
- Griffin, M.J.; Newman, M.M. An experimental study of low-frequency motion in cars. Proc. Inst. Mech. Eng. Part D J. Automob. Eng. 2004, 218, 1231–1238. [Google Scholar] [CrossRef]
- Rolnick, A.; Lubow, R.E. Why is the driver rarely motion sick? The role of controllability in motion sickness. Ergonomics 1991, 34, 867–879. [Google Scholar] [CrossRef]
- Diels, C. Will autonomous vehicles make us sick? In Contemporary Ergonomics and Human Factors; Sharples, S.M., Shorrock, S., Eds.; Taylor & Francis: Abingdon, UK, 2014; pp. 301–307. [Google Scholar]
- Diels, C.; Bos, J.E. Self-driving carsickness. Appl. Ergon. Part B 2016, 53, 374–382. [Google Scholar] [CrossRef]
- Schmidt, E.A.; Kuiper, O.X.; Wolter, S.; Diels, C.; Bos, J.E. An international survey on the incidence and modulating factors of carsickness. Transp. Res. Part F Traffic Psychol. Behav. 2020, 71, 76–87. [Google Scholar] [CrossRef]
- Reason, J.T.; Brand, J.J. Motion Sickness; Academic Press: London, UK, 1975. [Google Scholar]
- Bos, J.E. Motion sickness, simulator sickness, and automated vehicles. In Proceedings of the Driving Simulation and Virtual Reality Conference Europe, Antibes, France, 5–7 September 2018. [Google Scholar]
- Bos, J.E.; Damala, D.; Lewis, C.; Ganguly, A.; Turan, O. Susceptibility to seasickness. Ergonomics 2007, 50, 890–901. [Google Scholar] [CrossRef] [PubMed]
- Irwin, J.A. The pathology of seasickness. Lancet 1881, 2, 907–909. [Google Scholar] [CrossRef]
- James, W. The sense of dizziness in deaf-mutes. Am. J. Otol. 1882, 4, 239–254. [Google Scholar]
- Kennedy, R.S.; Graybiel, A.; McDonough, R.C.; Beckwith, F.D. Symptomatology under storm conditions in the North Atlantic in control subjects and in persons with bilateral labyrinthine defects. Acta Otolaryngol. 1968, 66, 533–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graybiel, A. Susceptibility to acute motion sickness in blind persons. Aerosp. Med. 1970, 41, 650–653. [Google Scholar]
- Hettinger, L.J.; Kennedy, R.S.; Berbaum, K.S. Tracing the etiology of simulator sickness. Simul. Ser. 1987, 18, 105–108. [Google Scholar]
- Gower, D.W.; Lilienthal, M.G.; Kennedy, R.S.; Fowlkes, J.E. Simulator sickness in U.S. Army and Navy fixed- and rotary-wing flight simulators. In Proceedings of the AGARD Medical Panel Symposium on Motion Cues in Flight Simulation and Simulator Induced Sickness, Brussels, Belgium, 28 September–2 October 1987. [Google Scholar]
- Kennedy, R.S.; Lilienthal, M.G.; Berbaum, K.S.; Baltzley, D.R.; McCauley, M.E. Simulator sickness in U.S. Navy flight simulators. Aviat. Space Environ. Med. 1989, 60, 10–16. [Google Scholar]
- Stanney, K.; Lawson, B.D.; Rokers, B.; Dennison, M.; Fidopiastis, C.; Stoffregen, T.; Weech, S.; Fulvio, J.M. Identifying causes of and solutions for cybersickness in immersive technology: Reformulation of a research and development agenda. Int. J. Hum. Comput. Interact. 2020, 36, 1783–1803. [Google Scholar] [CrossRef]
- Caserman, P.; Garcia-Agundez, A.; Gamez Zerban, A.; Goebel, S. Cybersickness in current-generation virtual reality head-mounted displays: Systematic review and outlook. Virtual Real. 2021, 25, 1153–1170. [Google Scholar] [CrossRef]
- Reed, N.; Diels, C.; Parkes, A.M. Simulator sickness management: Enhanced familiarisation and screening processes. In Proceedings of the 1st International Symposium of Visually Induced Motion Sickness, Hong Kong, China, 10–11 December 2007; pp. 156–162. [Google Scholar]
- Cordes, C.; Heutink, J.; Brookhuis, K.A.; Brouwer, W.H.; Melis-Dankers, B.J.M. Driving slow motorised vehicles with visual impairment—A simulator study. Cogent Psychol. 2018, 5, 1485473. [Google Scholar] [CrossRef]
- Von Holst, E.; Mittelstaedt, H. Das Reafferenzprinzip. Naturwissenschaften 1950, 37, 464–476. [Google Scholar] [CrossRef]
- Reason, J.T. Motion sickness adaptation: A neural mismatch model. J. R. Soc. Med. 1978, 71, 819–829. [Google Scholar] [CrossRef] [Green Version]
- Oman, C.M. A heuristic mathematical model for the dynamics of sensory conflict and motion sickness. Acta Otolaryngol. Suppl. 1982, 392, 1–44. [Google Scholar] [CrossRef]
- Oman, C.M. Sensory conflict in motion sickness: An observer theory approach. In Pictorial Communication in Virtual and Real Environments, 2nd ed.; Ellis, S.R., Kaiser, M.K., Grunwald, A.J., Eds.; Taylor & Francis: London, UK, 1993; pp. 362–376. [Google Scholar]
- Bles, W.; Bos, J.E.; De Graaf, B.; Groen, E.; Wertheim, A.H. Motion sickness: Only one provocative conflict? Brain Res. Bull. 1998, 47, 481–487. [Google Scholar] [CrossRef]
- Bos, J.E.; Bles, W.; Groen, E.L. A theory on visually induced motion sickness. Displays 2008, 29, 47–57. [Google Scholar] [CrossRef]
- Bos, J.E.; Bles, W. Modelling motion sickness and subjective vertical mismatch detailed for vertical motions. Brain Res. Bull. 1998, 47, 537–542. [Google Scholar] [CrossRef]
- Kamiji, N.; Kurata, Y.; Wada, T.; Doi, S. Modeling and validation of carsickness mechanism. In Proceedings of the Annual International Conference on Instrumentation, Control and Information Technology, Takamatsu, Japan, 17–20 September 2007; pp. 1138–1143. [Google Scholar]
- Ukita, R.; Okafuji, Y.; Wada, T. A simulation study on lane-change control of automated vehicles to reduce motion sickness based on a computational model. In Proceedings of the IEEE International Conference on Systems, Man, and Cybernetics, Melbourne, Australia, 17–20 October 2020. [Google Scholar]
- Wada, T. Computational model of motion sickness describing the effects of learning exogenous motion dynamics. Front. Syst. Neurosci. 2021, 15, 634604. [Google Scholar] [CrossRef]
- Wada, T.; Fujisawa, S.; Doi, S. Analysis of driver’s head tilt using a mathematical model of motion sickness. Int. J. Ind. Ergon. 2018, 63, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Wada, T.; Kawano, J.; Okafuji, Y.; Takamatsu, A.; Mitsuhiro, M. A computational model of motion sickness considering visual and vestibular information. In Proceedings of the IEEE International Conference on Systems, Man, and Cybernetics, Melbourne, Australia, 17–20 October 2020. [Google Scholar]
- Riccio, G.E.; Stoffregen, T.A. An ecological theory of motion sickness and postural instability. Ecol. Psychol. 1991, 3, 195–240. [Google Scholar] [CrossRef]
- Stoffregen, T.A.; Riccio, G.E. An ecological critique of the sensory conflict theory of motion sickness. Ecol. Psychol. 1991, 3, 159–194. [Google Scholar] [CrossRef]
- Bos, J.E. Nuancing the relationship between motion sickness and postural stability. Displays 2011, 32, 189–193. [Google Scholar] [CrossRef]
- Bos, J.E.; Lawson, B.D.; Allsop, J.; Rigato, P.; Secci, S. Chapter 2: Introduction. In Guidelines for Mitigating Cybersickness in Virtual Reality Systems; NATO STO, Report of the Human Factors and Medicine Panel/Modelling and Simulation Group 2021a, Activity number 323, NATO STO-TR-HFM-MSG-323; Proietti, P., Ed.; NATO: Brussels, Belgium, 2021. [Google Scholar]
- Rushton, S.K.; Riddell, P.M. Developing visual systems and exposure to virtual reality and stereo displays: Some concerns and speculations about the demands on accommodation and vergence. Appl. Ergon. 1999, 30, 69–78. [Google Scholar] [CrossRef]
- Lambooij, M.; Fortuin, M.; Heynderickx, I.; IJsselsteijn, W. Visual Discomfort and Visual Fatigue of Stereoscopic Displays: A Review. J. Imaging Sci. Technol. 2009, 53, 30201-1. [Google Scholar] [CrossRef] [Green Version]
- Bos, J.E.; MacKinnon, S.N.; Patterson, A. Motion Sickness Symptoms in a Ship Motion Simulator: Effects of Inside, Outside, and No View. Aviat. Space Environ. Med. 2005, 76, 1111–1118. [Google Scholar] [PubMed]
- Lawson, B.D. Motion Sickness Symptomatology and Origins. In Handbook of Virtual Environments: Design, Implementation, and Applications, 2nd ed.; Hale, K.S., Stanney, K.M., Eds.; CRC Press: Boca Raton, FL, USA, 2014; pp. 531–600. [Google Scholar]
- Reuten, A.J.C.; Nooij, S.A.E.; Bos, J.E.; Smeets, J.B.J. How feelings of unpleasantness develop during the progression of motion sickness symptoms. Exp. Brain Res. 2021, 239, 3615–3624. [Google Scholar] [CrossRef]
- Muth, E.R.; Stern, R.M.; Thayer, J.F.; Koch, K.L. Assessment of the multiple dimensions of nausea: The Nauea Profile (NP). J. Psychosom. Res. 1996, 40, 511–520. [Google Scholar] [CrossRef]
- Balaban, C.D.; Yates, B.J. What is nausea? A historical analysis of changing views. Auton. Neurosci. Basic Clin. 2017, 202, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Cha, Y.H.; Golding, J.F.; Keshavarz, B.; Furman, J.; Kim, J.S.; Lopez-Escamez, J.A.; Magnusson, M.; Yates, B.J.; Lawson, B.D. Motion sickness diagnostic criteria: Consensus document of the classification committee of the Barany Society. J. Vestib. Res. 2021, 31, 327–344. [Google Scholar] [CrossRef]
- Graybiel, A.; Wood, C.D.; Miller, E.F.; Dewy, B.; Cramer, D.B. Diagnostic criteria for grading the severity of acute motion sickness. Aerosp. Med. 1968, 39, 453–455. [Google Scholar]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator Sickness Questionnaire: An enhanced method for quantifying simulator sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Gianaros, P.J.; Muth, E.R.; Mordkoff, J.T.; Levine, M.E.; Stern, R.M. A Questionnaire for the Assessment of the Multiple Dimensions of Motion Sickness. Aviat. Space Environ. Med. 2001, 72, 115–119. [Google Scholar] [PubMed]
- Graybiel, A.; Knepton, J. Sopite syndrome: A sometimes sole manifestation of motion sickness. Aviat. Space Environ. Med. 1976, 47, 873–882. [Google Scholar] [PubMed]
- Matsangas, P.; McCauley, M.E. Sopite syndrome: A revised definition. Aviat. Space Environ. Med. 2014, 85, 672–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawson, B.D. Motion sickness scaling. In Handbook of Virtual Environments: Design, Implementation and Applications, 2nd ed.; Hale, K.S., Stanney, K.M., Eds.; CRC Press: Boca Raton, FL, USA, 2014; pp. 601–623. [Google Scholar]
- Wertheim, A.H.; Bos, J.E.; Bles, W. Contributions of roll and pitch to sea sickness. Brain Res. Bull. 1998, 47, 517–524. [Google Scholar] [CrossRef]
- Shupak, A.; Gordon, C.R. Motion Sickness: Advances in Pathogenesis, Prediction, Prevention, and Treatment. Aviat. Space Environ. Med. 2006, 77, 1213–1223. [Google Scholar]
- Keshavarz, B.; Hecht, H. Validating an Efficient Method to Quantify Motion Sickness. Hum. Factors J. Hum. Factors Ergon. Soc. 2011, 53, 415–426. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, R.S.; Frank, L.H. Review of motion sickness with special reference to simulator sickness. Transp. Res. Rec. 1985, 1059, 75–79. [Google Scholar]
- Gavgani, A.M.; Nesbitt, K.V.; Blackmore, K.L.; Nalivaiko, E. Profiling subjective symptoms and autonomic changes associated with cybersickness. Auton. Neurosci. 2017, 203, 41–50. [Google Scholar] [CrossRef]
- Romano, F.; Caramia, N.; Straumann, D.; Nalivaiko, E.; Bertolini, G. Cross-coupling vestibular stimulation: Motion sickness and the vestibulo-sympathetic reflex. J. Neurol. 2017, 264 (Suppl. S1), 96–103. [Google Scholar] [CrossRef]
- Irmak, T.; Pool, D.M.; Happee, R. Objective and subjective responses to motion sickness: The group and the individual. Exp. Brain Res. 2021, 239, 515–531. [Google Scholar] [CrossRef]
- Keshavarz, B.; Peck, K.; Rezaei, S.; Taati, B. Detecting and predicting visually induced motion sickness with physiological measures in combination with machine learning techniques. Int. J. Psychophysiol. 2022, 176, 14–26. [Google Scholar] [CrossRef]
- Li, C.; Zhang, Z.; Liu, Y.; Zhang, T.; Zhang, X.; Wang, H.; Wang, X. Multi-Dimensional and Objective Assessment of Motion Sickness Susceptibility Based on Machine Learning. Front. Neurol. 2022, 13, 824670. [Google Scholar] [CrossRef]
- Stout, C.S.; Toscano, W.B.; Cowings, P.S. Reliability of Autonomic Responses and Malaise across Multiple Motion Sickness Stimulation Tests; NASA-TM-108787; NASA Ames Research Center: Mountain View, CA, USA, 1993. [Google Scholar]
- Dahlman, J.; Sjörs, A.; Lindström, J.; Ledin, T.; Falkmer, T. Performance and Autonomic Responses during Motion Sickness. Hum. Factors J. Hum. Factors Ergon. Soc. 2009, 51, 56–66. [Google Scholar] [CrossRef]
- Smyth, J.; Birrell, S.; Woodman, R.; Jennings, P. Exploring the utility of EDA and skin temperature as individual physiological correlates of motion sickness. Appl. Ergon. 2021, 92, 103315. [Google Scholar] [CrossRef]
- Koohestani, A.; Nahavandi, D.; Asadi, H.; Kebria, P.M.; Khosravi, A.; Alizadehsani, R.; Nahavandi, S. A Knowledge Discovery in Motion Sickness: A Comprehensive Literature Review. IEEE Access 2019, 7, 85755–85770. [Google Scholar] [CrossRef]
- Lee, J.D.; Alsaid, A. A Machine Vision Approach for Estimating Motion Discomfort in Simulators and in Self-Driving; SAFER-SIM University Transport Center: Iowa City, IA, USA; University of Madison: Madison, WI, USA, 2019. [Google Scholar]
- Money, K.E. Motion Sickness. Physiol. Rev. 1970, 50, 1–39. [Google Scholar] [CrossRef]
- Cheung, B.S.K.; Howard, I.P.; Money, K.E. Visually-induced sickness in normal and bilaterally labyrinthine-defective subjects. Aviat. Space Environ. Med. 1991, 62, 527–531. [Google Scholar]
- Golding, J.F. Motion sickness susceptibility. Auton. Neurosci. 2006, 129, 67–76. [Google Scholar] [CrossRef]
- Golding, J.F. Predicting individual differences in motion sickness susceptibility by questionnaire. Personal. Individ. Differ. 2006, 41, 237–248. [Google Scholar] [CrossRef]
- Sharma, K. Susceptibility to Motion Sickness. Acta Genet. Med. Gemellol. Twin Res. 1980, 29, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Reavley, C.M.; Golding, J.F.; Cherkas, L.F.; Spector, T.D.; MacGregor, A.J. Genetic Influences on Motion Sickness Susceptibility in Adult Women: A Classical Twin Study. Aviat. Space Environ. Med. 2006, 77, 1148–1152. [Google Scholar] [PubMed]
- Hromatka, B.S.; Tung, J.Y.; Kiefer, A.K.; Do, C.B.; Hinds, D.A.; Eriksson, N. Genetic variants associated with motion sickness point to roles for inner ear development, neurological processes, and glucose homeostasis. Hum. Mol. Genet. 2015, 24, 2700–2708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittelstaedt, J.M. Individual predictors of the susceptibility for motion-related sickness: A systematic review. J. Vestib. Res. 2020, 30, 165–193. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.; Griffin, M.J. Motion Sickness Incidence during a Round-The-World Yacht Race. Aviat. Space Environ. Med. 1995, 66, 849–856. [Google Scholar]
- Dobie, T.; McBride, D.; Dobie, T., Jr.; May, J. The effects of age and sex on susceptibility to motion sickness. Aviat. Space Environ. Med. 2001, 72, 13–20. [Google Scholar]
- Flanagan, M.B.; Alvarado, E.; May, J.G.; Dobie, T.G. Sex differences in tolerance to visually induced motion sickness. Aviat. Space Environ. Med. 2001, 76, 642–646. [Google Scholar]
- Golding, J.F.; Kadzere, P.; Gresty, M.A. Motion Sickness Susceptibility Fluctuates through the Menstrual Cycle. Aviat. Space Environ. Med. 2005, 76, 970–973. [Google Scholar]
- Grunfeld, E.; Gresty, M.A. Relationship between motion sickness, migraine and menstruation in crew members of a “round the world” yacht race. Brain Res. Bull. 1998, 47, 433–436. [Google Scholar] [CrossRef]
- Paillard, A.C.; Quarck, G.; Paolino, F.; Denise, P.; Paolino, M.; Golding, J.F.; Ghulyan-Bedikian, V. Motion sickness susceptibility in healthy subjects and vestibular patients: Effects of gender, age and trait-anxiety. J. Vestib. Res. 2013, 23, 203–209. [Google Scholar] [CrossRef]
- Turner, M.; Griffin, M.J. Motion sickness in public road transport: Passenger behaviour and susceptibility. Ergonomics 1999, 42, 444–461. [Google Scholar] [CrossRef]
- Huppert, D.; Grill, E.; Brandt, T. Survey of motion sickness susceptibility in children and adolescents aged 3 months to 18 years. J. Neurol. 2019, 266 (Suppl. S1), 65–73. [Google Scholar] [CrossRef]
- Besnard, S.; Bois, J.; Hitier, M.; Vogt, J.; Laforet, P.; Golding, J.F. Motion Sickness Lessons from the Southern Ocean. Aerosp. Med. Hum. Perform. 2021, 92, 720–727. [Google Scholar] [CrossRef]
- Saredakis, D.; Szpak, A.; Birckhead, B.; Keage, H.A.D.; Rizzo, A.; Loetscher, T. Factors Associated with Virtual Reality Sickness in Head-Mounted Displays: A Systematic Review and Meta-Analysis. Front. Hum. Neurosci. 2020, 14, 96. [Google Scholar] [CrossRef]
- Hurter, J.; Maraj, C.; Murphy, S. Commercial virtual reality displays: Issues of performance and simulator sickness from exocentric depth-perception tasks. Displays 2021, 70, 102095. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhang, J.; Fang, F. Vergence-accommodation conflict in optical see-through display: Review and prospect. Results Opt. 2021, 5, 100160. [Google Scholar] [CrossRef]
- Golding, J.F. Motion sickness susceptibility questionnaire revised and its relationship to other forms of sickness. Brain Res. Bull. 1998, 47, 507–516. [Google Scholar] [CrossRef]
- Lamb, S.; Kwok, K.C.S. MSSQ-Short Norms May Underestimate Highly Susceptible Individuals: Updating the MSSQ-Short Norms. Hum. Factors J. Hum. Factors Ergon. Soc. 2015, 57, 622–633. [Google Scholar] [CrossRef]
- Kennedy, R.S.; Graybiel, A. The Dial Test: A Standardized Procedure for the Experimental Production of Canal Sickness Symptomatology in a Rotating Environment; U.S. Naval School of Aviation Medicine: Pensacola, FL, USA, 1965; NSAM 113. [Google Scholar]
- Stanney, K.M.; Hale, K.S.; Nahmens, I.; Kennedy, R.S. What to Expect from Immersive Virtual Environment Exposure: Influences of Gender, Body Mass Index, and Past Experience. Hum. Factors J. Hum. Factors Ergon. Soc. 2003, 45, 504–520. [Google Scholar] [CrossRef]
- Nooij, S.A.E.; Bockisch, C.J.; Bülthoff, H.H.; Straumann, D. Beyond sensory conflict: The role of beliefs and perception in motion sickness. PLoS ONE 2021, 16, e0245295. [Google Scholar] [CrossRef]
- Howarth, P.A.; Hodder, S.G. Characteristics of habituation to motion in a virtual environment. Displays 2008, 29, 117–123. [Google Scholar] [CrossRef]
- Golding, J.F.; Markey, H.M.; Stott, J.R.R. The effects of motion direction, body axis, and posture on motion sickness induced by low frequency linear oscillation. Aviat. Space Environ. Med. 1995, 66, 1046–1051. [Google Scholar] [PubMed]
- Golding, J.F.; Markey, H.M. Effect of frequency of horizontal linear oscillation on motion sickness and somatogravic illusion. Aviat. Space Environ. Med. 1996, 67, 121–126. [Google Scholar] [PubMed]
- Golding, J.F.; Finch, M.I.; Stott, J.R.R. Frequency effect of 0.35–1.0 hz horizontal translational oscillation on motion sickness and the somatogravic illusion. Aviat. Space Environ. Med. 1997, 68, 396–402. [Google Scholar] [PubMed]
- Golding, J.F.; Phil, D.; Mueller, A.G.; Gresty, M.A. A motion sickness maximum around the 0.2 Hz frequency range of horizontal translational oscillation. Aviat. Space Environ. Med. 2001, 72, 188–192. [Google Scholar]
- Griffin, M.J.; Mills, K.L. Effect of frequency and direction of horizontal oscillation on motion sickness. Aviat. Space Environ. Med. 2002, 73, 537–543. [Google Scholar]
- Griffin, M.J.; Mills, K.L. Effect of magnitude and direction of horizontal oscillation on motion sickness. Aviat. Space Environ. Med. 2002, 73, 640–646. [Google Scholar]
- Donohew, B.E.; Griffin, M.J. Motion sickness: Effect of the frequency of lateral oscillation. Aviat. Space Environ. Med. 2004, 75, 649–656. [Google Scholar]
- Butler, C.; Griffin, M.J. Motion sickness with combined fore-aft and pitch oscillation: Effect of phase and the visual scene. Aviat. Space Environ. Med. 2009, 80, 946–954. [Google Scholar] [CrossRef]
- Howarth, H.V.C.; Griffin, M.J. Effect of roll oscillation frequency on motion sickness. Aviat. Space Environ. Med. 2003, 74, 326–331. [Google Scholar]
- Joseph, J.A.; Griffin, M.J. Motion sickness: Effect of the magnitude of roll and pitch oscillation. Aviat. Space Environ. Med. 2008, 79, 390–396. [Google Scholar] [CrossRef]
- Donohew, B.E.; Griffin, M.J. Motion sickness with combined lateral and roll oscillation: Effect of percentage compensation. Aviat. Space Environ. Med. 2010, 81, 22–29. [Google Scholar] [CrossRef]
- Bles, W. Coriolis effects and motion sickness modelling. Brain Res. Bull. 1998, 47, 543–549. [Google Scholar] [CrossRef]
- Bos, J.E. Less sickness with more motion and/or mental distraction. J. Vestib. Res. 2015, 25, 23–33. [Google Scholar] [CrossRef] [Green Version]
- Golding, J.F.; Stott, J.R.R. Effect of sickness severity on habituation to repeated motion challenges in aircrew referred for airsickness treatment. Aviat. Space Environ. Med. 1995, 66, 625–630. [Google Scholar]
- Kuiper, O.X.; Bos, J.E.; Schmidt, E.A.; Diels, C.; Wolter, S. Knowing what’s coming: Unpredictable motion causes more sickness. Hum. Factors 2020, 62, 1339–1348. [Google Scholar] [CrossRef] [Green Version]
- Probst, T.; Krafczyk, S.; Buchele, W.; Brandt, T. Visuelle Praevention der Bewegungskrankheit im Auto. Arch. Psychiatr. Nervenkrankh. 1982, 231, 409–421. [Google Scholar] [CrossRef]
- Kuiper, O.X.; Bos, J.E.; Diels, C. Looking forward: In-vehicle auxiliary display positioning affects carsickness. Appl. Ergon. 2018, 68, 169–175. [Google Scholar] [CrossRef]
- Bohrmann, D.; Bengler, K. Reclined posture for enabling autonomous driving. In Proceedings of the International Conferance on Human Systems Engineering and Design (IHSE 2019), Munchen, Germany, 1–18 September 2020; Ahram, T., Ed.; Springer Nature: Cham, Switzerland, 2020; pp. 1–7. [Google Scholar]
- Kuiper, O.X.; Bos, J.E.; Schmidt, E.A.; Diels, C. Knowing what’s coming: Anticipatory audio cues can mitigate motion sickness. Appl. Ergon. 2020, 85, 103068. [Google Scholar] [CrossRef]
- Diels, C.; Bos, J.E. Great Expectations: On the Design of Predictive Motion Cues to Alleviate Carsickness. In HCI in Mobility, Transport, and Automotive Systems. HCII 2021, Proceedings of the International Conference on Human-Computer Interaction, Malaga, Spain, 22–24 September 2021; Lecture Notes in Computer Science; Krömker, H., Ed.; Springer: Cham, Switzerland, 2021; p. 12791. [Google Scholar]
- Asch, S.E.; Witkin, H.A. Studies in space orientation: I. Perception of the upright with displaced visual fields. J. Exp. Psychol. 1948, 38, 325–337. [Google Scholar] [CrossRef]
- Bos, J.E.; Nooij, S.A.E.; Souman, J.L. (Im)possibilities of studying carsickness in a driving simulator. In Proceedings of the Driving Simulator Conference Europe, Munich, Germany, 14–17 September 2021; pp. 59–63. [Google Scholar]
- Correia Gracio, B.J.; Bos, J.E.; Van Paassen, M.M.; Mulder, M. Perceptual scaling of visual and inertial cues. Effects of field of view, image size, depth cues, and degree of freedom. Exp. Brain Res. 2014, 232, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Bos, J.E. Skyscraper sickness: Three reasons why tall buildings can be more sickening than ships. In Proceedings of the Motion Sickness Conference, Akureyri, Iceland, 8–10 July 2019. [Google Scholar]
- Salter, S.; Diels, C.; Herriotts, P.; Kanarachos, S.; Thake, D. Motion Sickness in Automated Vehicles with Forward and Rearward Facing Seating Orientations. Appl. Ergon. 2019, 78, 54–61. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bos, J.E.; Diels, C.; Souman, J.L. Beyond Seasickness: A Motivated Call for a New Motion Sickness Standard across Motion Environments. Vibration 2022, 5, 755-769. https://doi.org/10.3390/vibration5040044
Bos JE, Diels C, Souman JL. Beyond Seasickness: A Motivated Call for a New Motion Sickness Standard across Motion Environments. Vibration. 2022; 5(4):755-769. https://doi.org/10.3390/vibration5040044
Chicago/Turabian StyleBos, Jelte E., Cyriel Diels, and Jan L. Souman. 2022. "Beyond Seasickness: A Motivated Call for a New Motion Sickness Standard across Motion Environments" Vibration 5, no. 4: 755-769. https://doi.org/10.3390/vibration5040044