


Biomechanical Behavior of Lithium-Disilicate-Modified Endocrown Restorations: A Three-Dimensional Finite Element Analysis

Abstract
:1. Introduction
2. Materials and Methods
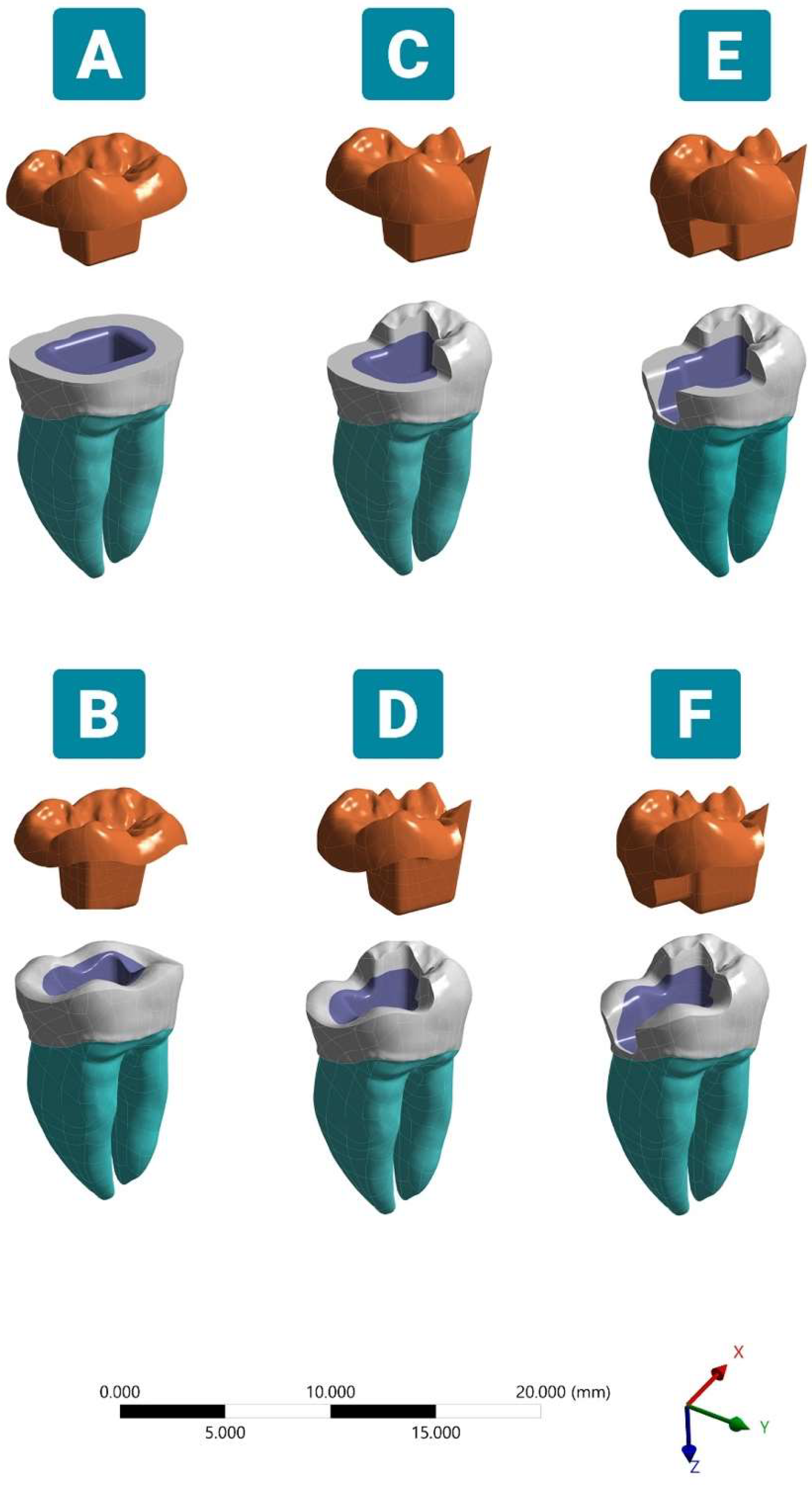
2.1. Generation of the 3D Geometrical Model
2.2. Endocrown Designs
2.3. Finite Element Analysis
3. Results
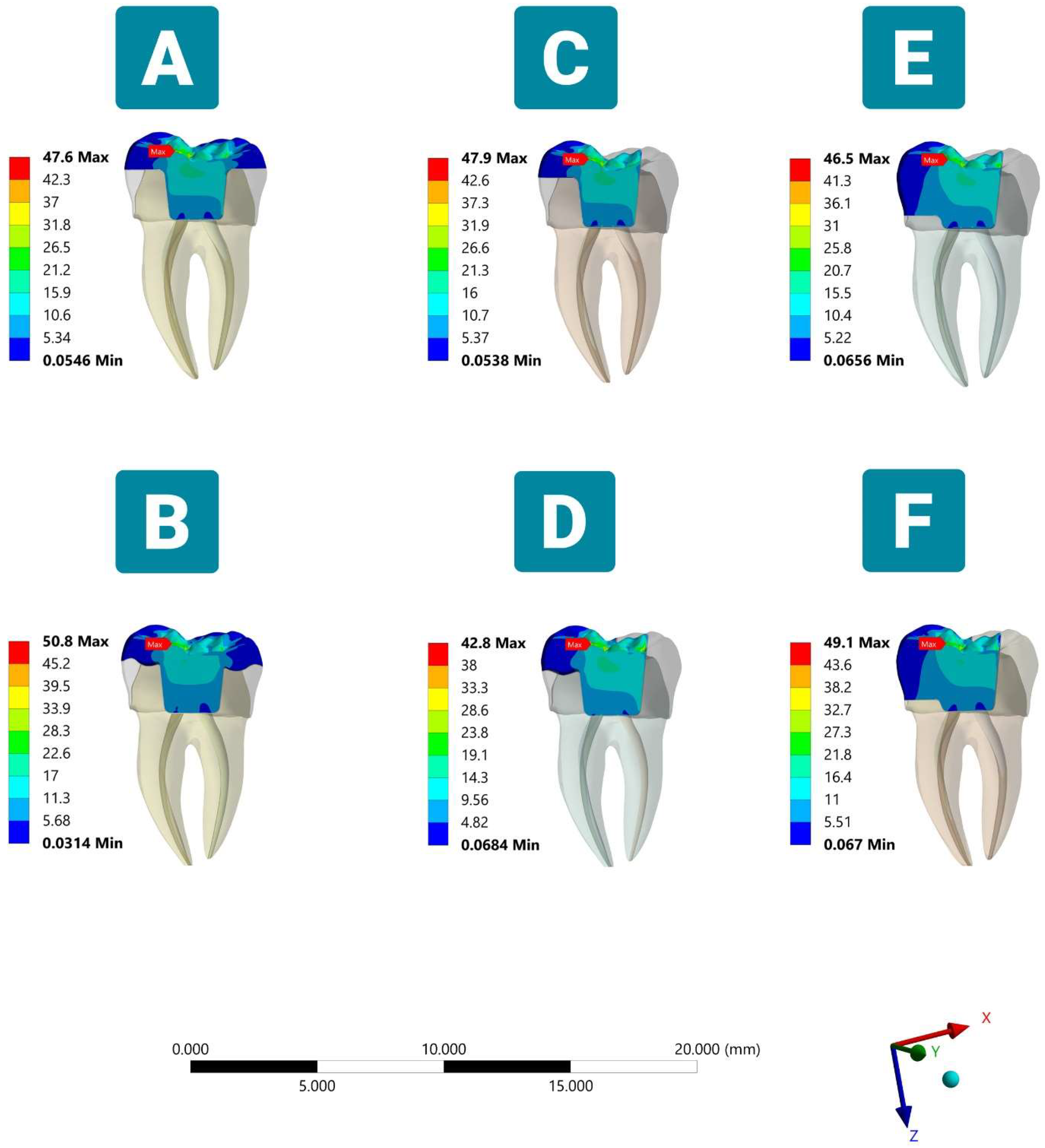
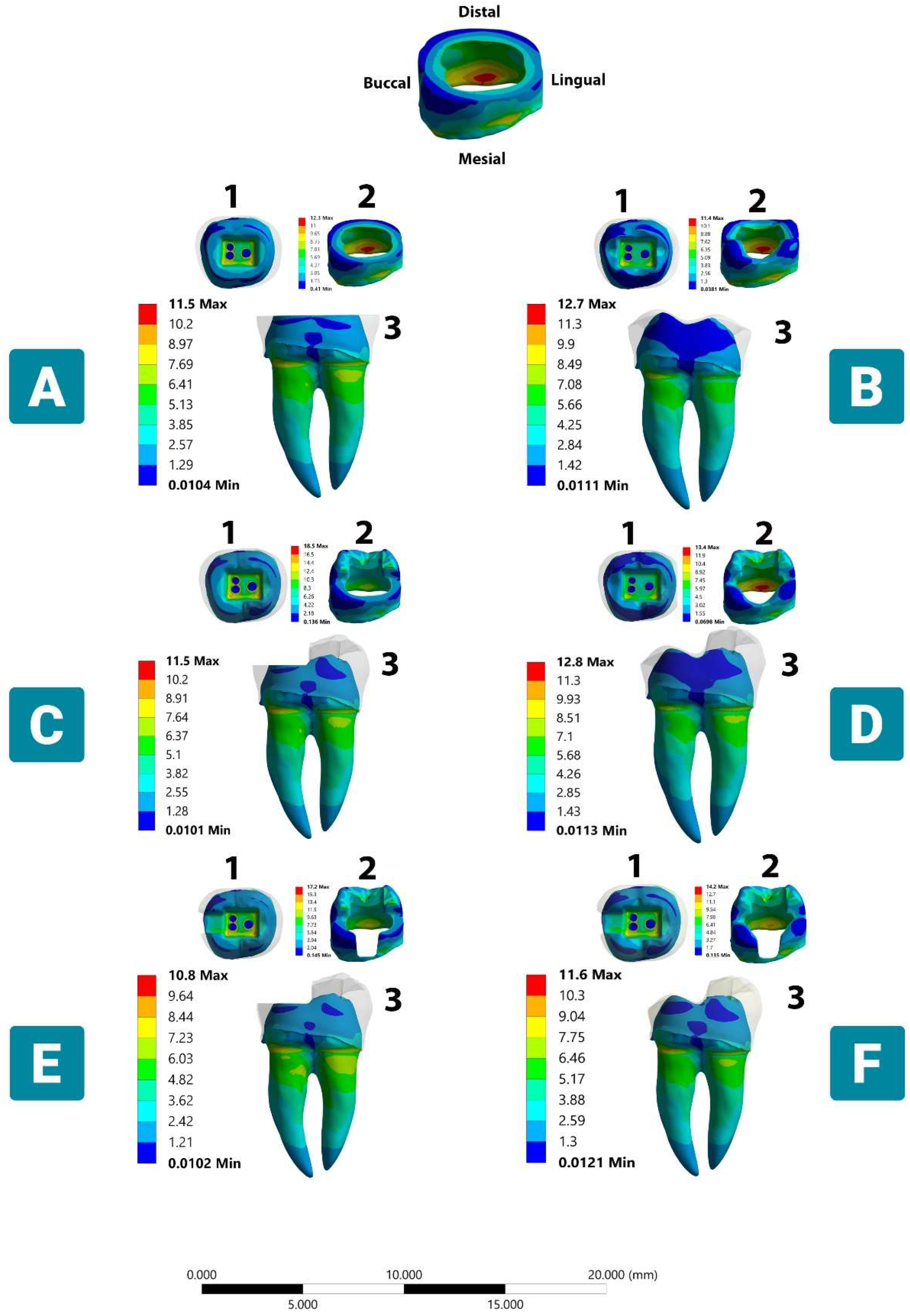
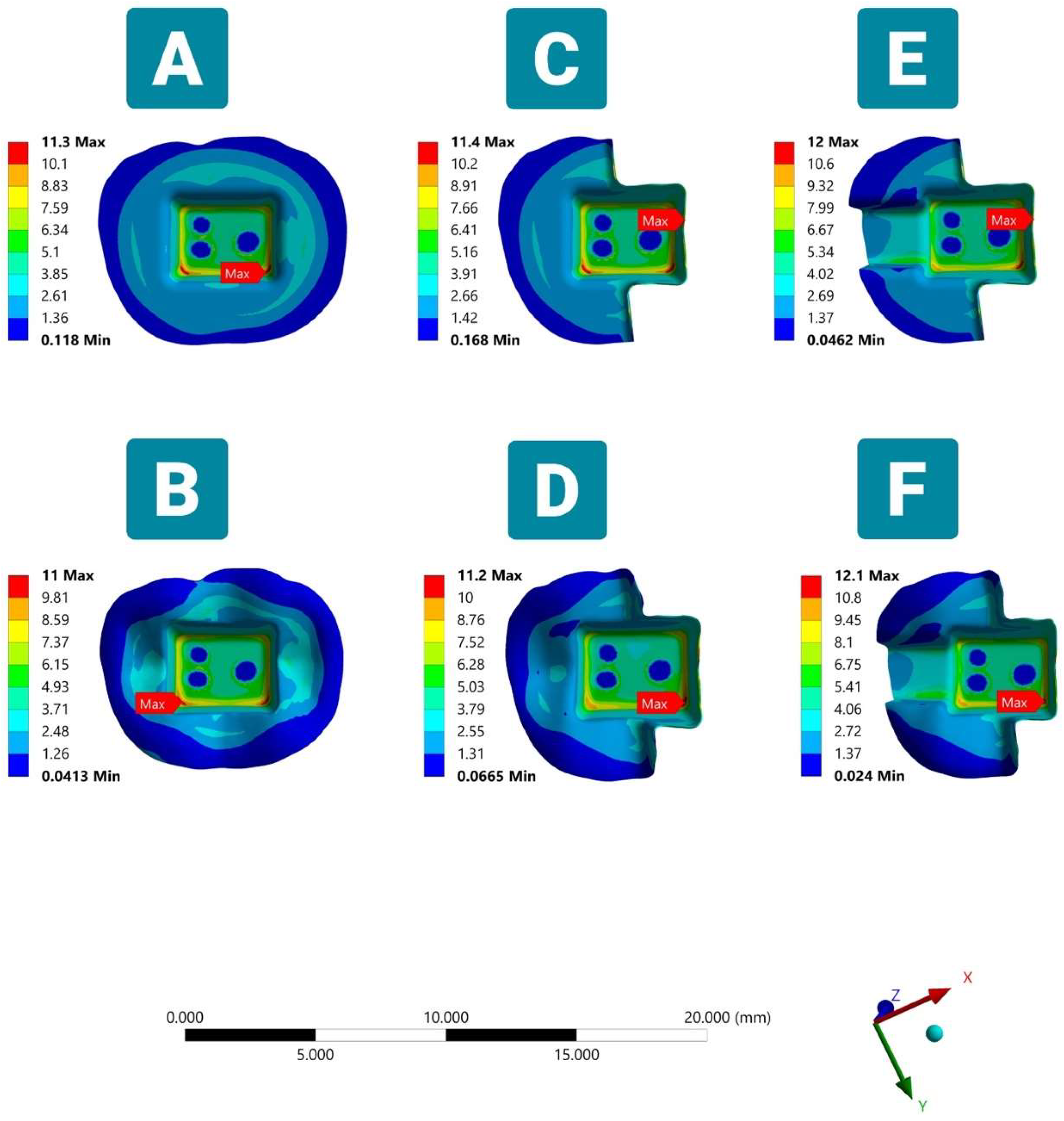
3.1. Stress Distribution under Vertical Load
3.1.1. Endocrown Restoration

3.1.2. Tooth Structure
3.1.3. Cement Layer

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model Preparation Design | Endocrown Restoration | Cement Layer | Tooth Structure | |
|---|---|---|---|---|
| Enamel | Dentin | |||
| Model A | 47.6 | 11.3 | 12.3 | 11.5 |
| Model B | 50.8 | 11.0 | 11.4 | 12.7 |
| Model C | 47.9 | 11.4 | 18.4 | 11.5 |
| Model D | 42.7 | 11.2 | 20.2 | 12.8 |
| Model E | 46.5 | 12 | 17.2 | 10.8 |
| Model F | 49.0 | 12.1 | 14.2 | 11.6 |


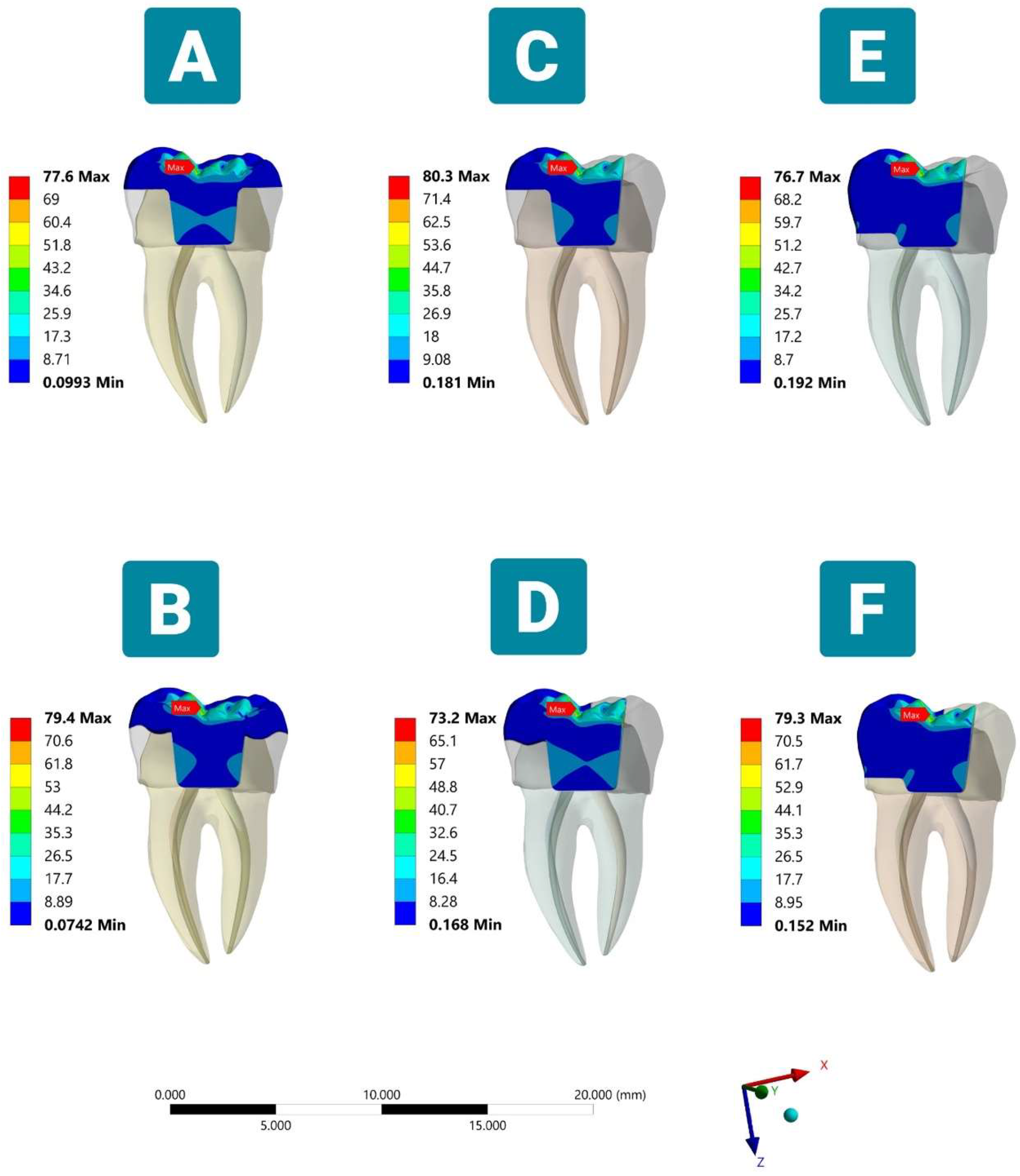
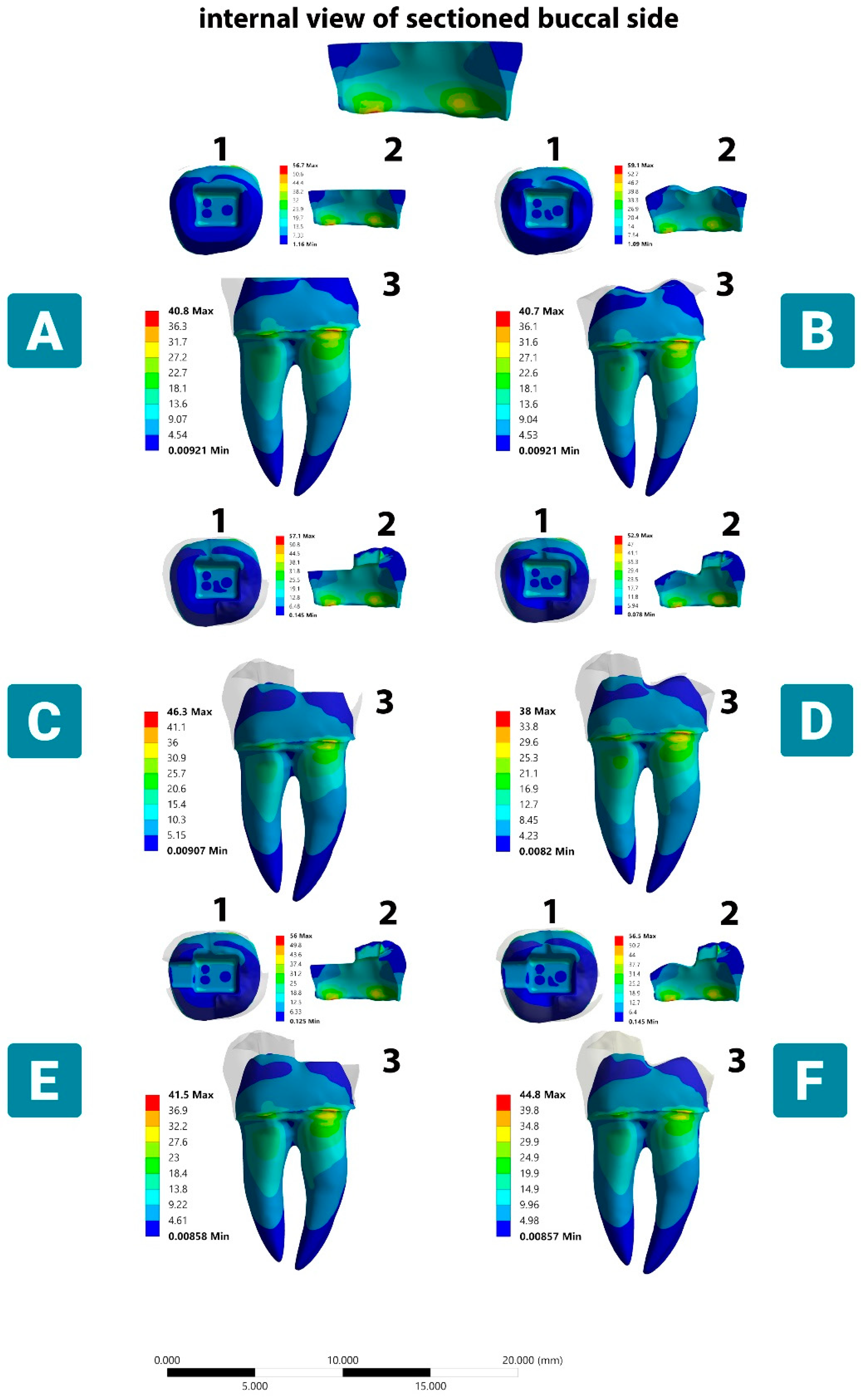
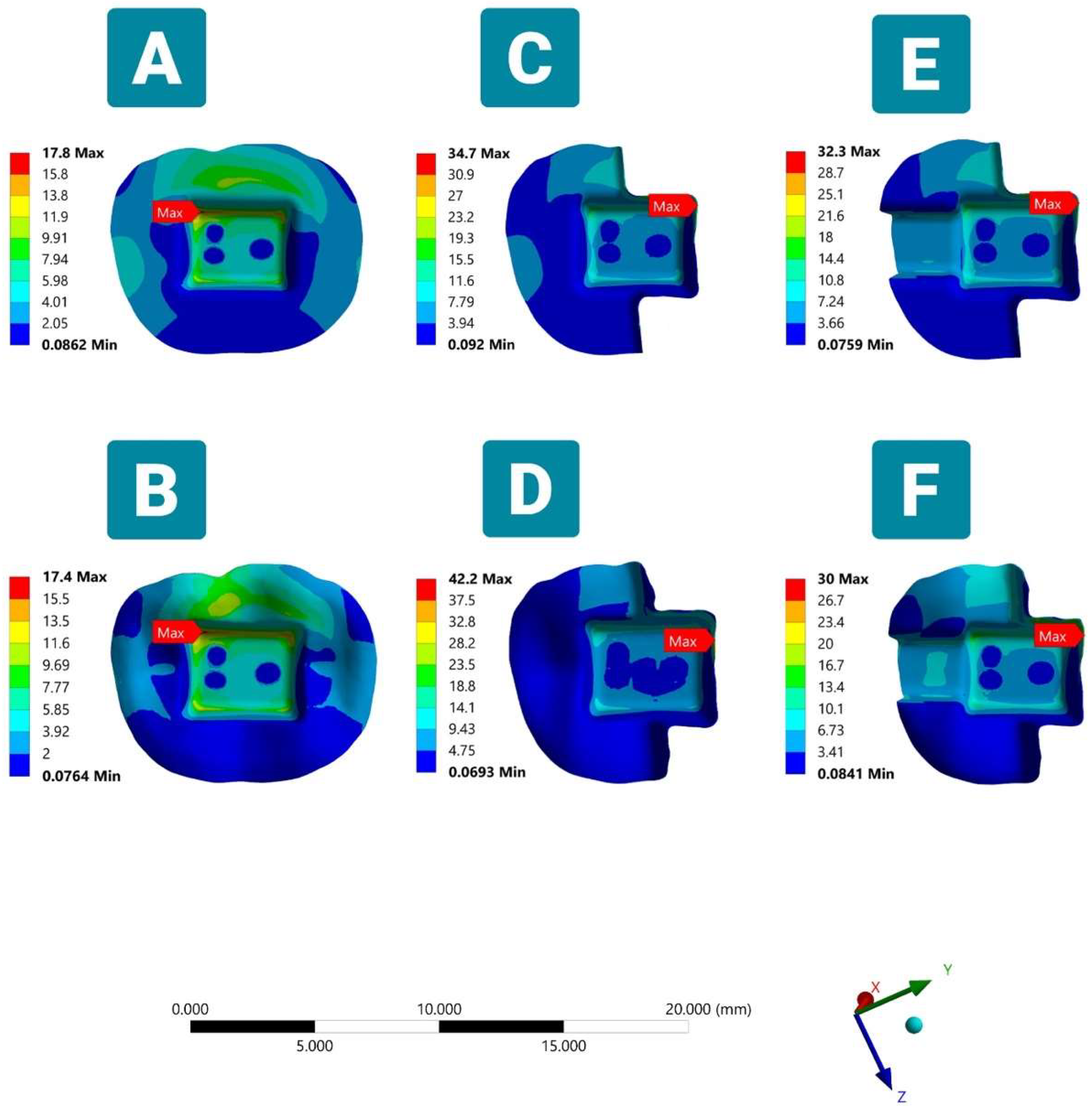
3.2. Stress Distribution under the Oblique Load
3.2.1. Lithium Disilicate Restoration

3.2.2. Tooth Structure

3.2.3. Cement Layer
| Model Preparation Design | Endocrown Restoration | Cement Layer | Tooth Structure | |
|---|---|---|---|---|
| Enamel | Dentin | |||
| Model A | 77.6 | 17.8 | 56.7 | 40.8 |
| Model B | 79.4 | 17.3 | 59.1 | 40.6 |
| Model C | 80.2 | 34.7 | 57.1 | 46.2 |
| Model D | 73.1 | 42.2 | 52.8 | 37.9 |
| Model E | 76.7 | 32.3 | 56.2 | 41.5 |
| Model F | 79.3 | 30.0 | 56.5 | 44.7 |

4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dietschi, D.; Duc, O.; Krejci, I.; Sadan, A. Biomechanical considerations for the restoration of endodontically treated teeth: A systematic review of the literature, Part II (Evaluation of fatigue behavior, interfaces, and in vivo studies). Quintessence Int. 2008, 39, 117–129. [Google Scholar]
- Schestatsky, R.; Dartora, G.; Felberg, R.; Spazzin, A.O.; Sarkis-Onofre, R.; Bacchi, A.; Pereira, G.K.R. Do endodontic retreatment techniques influence the fracture strength of endodontically treated teeth? A systematic review and meta-analysis. J. Mech. Behav. Biomed. Mater. 2019, 90, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Souza, E.M.; do Nascimento, L.M.; Maia Filho, E.M.; Alves, C.M.C. The impact of post preparation on the residual dentin thickness of maxillary molars. J. Prosthet. Dent. 2011, 106, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Phang, Z.Y.; Quek, S.H.Q.; Teoh, K.H.; Tan, K.B.C.; Tan, K. A Retrospective Study on the Success, Survival, and Incidence of Complications of Post-Retained Restorations in Premolars Supporting Fixed Dental Prostheses with a Mean of 7 Years in Function. Int. J. Prosthodont. 2020, 33, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Dal Piva, A.; Campos, F.; Alves, M.; Sousa, R.S.; Lima, J.; Souza, R. Influence of alveolar bone level on the pull-out bond strength of fiber-reinforced composite posts to root dentin. Gen Dent. 2016, 64, e5–e8. [Google Scholar]
- Dal Piva, A.M.d.O.; Tribst, J.P.M.; E Souza, R.O.d.A.; Borges, A.L.S. Influence of alveolar bone loss and cement layer thickness on the biomechanical behavior of endodontically treated maxillary incisors: A 3-dimensional finite element analysis. J. Endod. 2017, 43, 791–795. [Google Scholar] [CrossRef]
- Dartora, N.R.; de Conto Ferreira, M.B.; Moris, I.C.M.; Brazão, E.H.; Spazin, A.O.; Sousa-Neto, M.D.; Silva-Sousa, Y.-T.; Gomes, E.A. Effect of intracoronal depth of teeth restored with endocrowns on fracture resistance: In vitro and 3-dimensional finite element analysis. J. Endod. 2018, 44, 1179–1185. [Google Scholar] [CrossRef]
- Sedrez-Porto, J.A.; da Rosa, W.L.d.O.; Da Silva, A.F.; Münchow, E.A.; Pereira-Cenci, T. Endocrown restorations: A systematic review and meta-analysis. J. Dent. 2016, 52, 8–14. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dal Piva, A.M.d.O.; Madruga, C.F.L.; Valera, M.C.; Borges, A.L.S.; Bresciani, E.; de Melo, R.M. Endocrown restorations: Influence of dental remnant and restorative material on stress distribution. Dent. Mater. 2018, 34, 1466–1473. [Google Scholar] [CrossRef]
- Zheng, Z.; Sun, J.; Jiang, L.; Wu, Y.; He, J.; Ruan, W.; Yan, W. Influence of margin design and restorative material on the stress distribution of endocrowns: A 3D finite element analysis. BMC Oral Health 2022, 22, 30. [Google Scholar] [CrossRef]
- Sedrez-Porto, J.A.; Münchow, E.A.; Cenci, M.S.; Pereira-Cenci, T. Which materials would account for a better mechanical behavior for direct endocrown restorations? J. Mech. Behav. Biomed. Mater. 2020, 103, 103592. [Google Scholar] [CrossRef] [PubMed]
- Shah, Y.R.; Shiraguppi, V.L.; Deosarkar, B.; Tayeeb, S.M.; Pandey, A.; Shelke, U.R. Endocrowns: A Review. J. Interdiscip. Dent. Sci. 2020, 9, 7–12. [Google Scholar]
- Zhu, J.; Wang, D.; Rong, Q.; Qian, J.; Wang, X. Effect of central retainer shape and abduction angle during preparation of teeth on dentin and cement layer stress distributions in endocrown-restored mandibular molars. Dent. Mater. J. 2020, 39, 464–470. [Google Scholar] [CrossRef]
- Lin, J.; Lin, Z.; Zheng, Z. Effect of different restorative crown design and materials on stress distribution in endodontically treated molars: A finite element analysis study. BMC Oral Health 2020, 20, 226. [Google Scholar] [CrossRef]
- Rocca, G.T.; Sedlakova, P.; Saratti, C.; Sedlacek, R.; Gregor, L.; Rizcalla, N.; Feilzer, A.J.; Krejci, I. Fatigue behavior of resin-modified monolithic CAD–CAM RNC crowns and endocrowns. Dent. Mater. 2016, 32, e338–e350. [Google Scholar] [CrossRef]
- Hayes, A.; Duvall, N.; Wajdowicz, M.; Roberts, H. Effect of endocrown pulp chamber extension depth on molar fracture resistance. Oper. Dent. 2017, 42, 327–334. [Google Scholar] [CrossRef]
- Gurpinar, B.; Tak, O. Effect of pulp chamber depth on the accuracy of endocrown scans made with different intraoral scanners versus an industrial scanner: An in vitro study. J. Prosthet. Dent. 2022, 127, 430–437. [Google Scholar] [CrossRef] [PubMed]
- de Kuijper, M.C.; Cune, M.S.; Tromp, Y.; Gresnigt, M.M. Cyclic loading and load to failure of lithium disilicate endocrowns: Influence of the restoration extension in the pulp chamber and the enamel outline. J. Mech. Behav. Biomed. Mater. 2020, 105, 103670. [Google Scholar] [CrossRef]
- Einhorn, M.; DuVall, N.; Wajdowicz, M.; Brewster, J.; Roberts, H. Preparation ferrule design effect on endocrown failure resistance. J. Prosthodont. 2019, 28, e237–e242. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lai, H.; Meng, Q.; Gong, Q.; Tong, Z. The synergetic effect of pulp chamber extension depth and occlusal thickness on stress distribution of molar endocrowns: A 3-dimensional finite element analysis. J. Mater. Sci. Mater. Med. 2022, 33, 56. [Google Scholar] [CrossRef] [PubMed]
- Haralur, S.B.; Alamrey, A.A.; Alshehri, S.A.; Alzahrani, D.S.; Alfarsi, M. Effect of different preparation designs and all ceramic materials on fracture strength of molar endocrowns. J. Appl. Biomater. Funct. Mater. 2020, 18, 2280800020947329. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; He, Y.; Ruan, W.; Ling, Z.; Zheng, C.; Gai, Y.; Yan, W. Biomechanical behavior of endocrown restorations with different CAD-CAM materials: A 3D finite element and in vitro analysis. J. Prosthet. Dent. 2021, 125, 890–899. [Google Scholar] [CrossRef] [PubMed]
- Bamajboor, A.; Dudley, J. The Influence of Ferrule on the Marginal Gap and Fracture Resistance of Zirconia Endocrowns. Int. J. Prosthodont. 2022, 35, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Vianna, A.L.S.d.V.; Prado, C.J.d.; Bicalho, A.A.; Pereira, R.A.d.S.; Neves, F.D.d.; Soares, C.J. Effect of cavity preparation design and ceramic type on the stress distribution, strain and fracture resistance of CAD/CAM onlays in molars. J. Appl. Oral Sci. 2018, 26. [Google Scholar] [CrossRef] [PubMed]
- Bakeman, E.; Rego, N.; Chaiyabutr, Y.; Kois, J. Influence of ceramic thickness and ceramic materials on fracture resistance of posterior partial coverage restorations. Oper. Dent. 2015, 40, 211–217. [Google Scholar] [CrossRef]
- Al-Dabbagh, R.A. Survival and success of endocrowns: A systematic review and meta-analysis. J. Prosthet. Dent. 2021, 125, 415.e1–415.e9. [Google Scholar] [CrossRef]
- Xiao, W.; Chen, C.; Yang, T.; Zhu, Z. Influence of Different Marginal Forms on Endodontically Treated Posterior Teeth Restored with Lithium Disilicate Glass-Ceramic Onlays: Two-Year Follow-up. Int. J. Prosthodont. 2020, 33, 22–28. [Google Scholar] [CrossRef]
- Albakry, M.; Guazzato, M.; Swain, M.V. Influence of hot pressing on the microstructure and fracture toughness of two pressable dental glass–ceramics. J. Biomed. Mater. Res. 2004, 71, 99–107. [Google Scholar] [CrossRef]
- Zarone, F.; Di Mauro, M.I.; Ausiello, P.; Ruggiero, G.; Sorrentino, R. Current status on lithium disilicate and zirconia: A narrative review. BMC Oral Health 2019, 19, 134. [Google Scholar] [CrossRef] [PubMed]
- Zarone, F.; Ferrari, M.; Mangano, F.G.; Leone, R.; Sorrentino, R. “Digitally oriented materials”: Focus on lithium disilicate ceramics. Int. J. Dent. 2016, 2016, 9840594. [Google Scholar] [CrossRef]
- Abo El Fadl, A.; Elsewify, T. Fracture Resistance of Endodontically Treated Mandibular Molars Restored with Two Endocrown Designs (An In-Vitro Study). Egypt. Dent. J. 2019, 65, 3745–3750. [Google Scholar] [CrossRef]
- Da Fonseca, G.F.; De Andrade, G.S.; Dal Piva, A.M.d.O.; Tribst, J.P.M.; Borges, A.L.S. Computer-aided design finite element modeling of different approaches to rehabilitate endodontically treated teeth. J. Indian Prosthodont. Soc. 2018, 18, 329. [Google Scholar] [PubMed]
- Ghoul, W.E.; Özcan, M.; Tribst, J.P.M.; Salameh, Z. Fracture resistance, failure mode and stress concentration in a modified endocrown design. Biomater. Investig. Dent. 2020, 7, 110–119. [Google Scholar] [CrossRef]
- Zhu, J.; Rong, Q.; Wang, X.; Gao, X. Influence of remaining tooth structure and restorative material type on stress distribution in endodontically treated maxillary premolars: A finite element analysis. J. Prosthet. Dent. 2017, 117, 646–655. [Google Scholar] [CrossRef] [PubMed]
- Cantó-Navés, O.; Marimon, X.; Ferrer, M.; Cabratosa-Termes, J. Comparison between experimental digital image processing and numerical methods for stress analysis in dental implants with different restorative materials. J. Mech. Behav. Biomed. Mater. 2021, 113, 104092. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dal Piva, A.M.d.O.; de Jager, N.; Bottino, M.A.; de Kok, P.; Kleverlaan, C.J. Full-Crown Versus Endocrown Approach: A 3D-Analysis of Both Restorations and the Effect of Ferrule and Restoration Material. J. Prosthodont. 2021, 30, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Gulec, L.; Ulusoy, N. Effect of endocrown restorations with different CAD/CAM materials: 3D finite element and weibull analyses. BioMed Res. Int. 2017, 2017, 5638683. [Google Scholar] [CrossRef]
- Dawood, S.N.; Al-Zahawi, A.R.; Sabri, L.A. Mechanical and thermal stress behavior of a conservative proposed veneer preparation design for restoring misaligned anterior teeth: A 3D finite element analysis. Appl. Sci. 2020, 10, 5814. [Google Scholar] [CrossRef]
- Ibrahim, R.O.; AL-Zahawi, A.R.; Sabri, L.A. Mechanical and thermal stress evaluation of PEEK prefabricated post with different head design in endodontically treated tooth: 3D-finite element analysis. Dent. Mater. J. 2021, 40, 508–518. [Google Scholar] [CrossRef]
- Dartora, G.; Pereira, G.K.R.; de Carvalho, R.V.; Zucuni, C.P.; Valandro, L.F.; Cesar, P.F.; Caldas, R.A.; Bacchi, A. Comparison of endocrowns made of lithium disilicate glass-ceramic or polymer-infiltrated ceramic networks and direct composite resin restorations: Fatigue performance and stress distribution. J. Mech. Behav. Biomed. Mater. 2019, 100, 103401. [Google Scholar] [CrossRef]
- Dejak, B.; Młotkowski, A. 3D-Finite element analysis of molars restored with endocrowns and posts during masticatory simulation. Dent. Mater. 2013, 29, e309–e317. [Google Scholar] [CrossRef] [PubMed]
- Ausiello, P.; Ciaramella, S.; Di Rienzo, A.; Lanzotti, A.; Ventre, M.; Watts, D.C. Adhesive class I restorations in sound molar teeth incorporating combined resin-composite and glass ionomer materials: CAD-FE modeling and analysis. Dent. Mater. 2019, 35, 1514–1522. [Google Scholar] [CrossRef]
- Ausiello, P.; Ciaramella, S.; Fabianelli, A.; Gloria, A.; Martorelli, M.; Lanzotti, A.; Watts, D.C. Mechanical behavior of bulk direct composite versus block composite and lithium disilicate indirect Class II restorations by CAD-FEM modeling. Dent. Mater. 2017, 33, 690–701. [Google Scholar] [CrossRef]
- Dal Piva, A.M.d.O.; Tribst, J.P.M.; Borges, A.L.S.; e Souza, R.O.d.A.; Bottino, M.A. CAD-FEA modeling and analysis of different full crown monolithic restorations. Dent. Mater. 2018, 34, 1342–1350. [Google Scholar] [CrossRef]
- Durand, L.B.; Guimarães, J.C.; Monteiro Junior, S.; Baratieri, L.N. Effect of ceramic thickness and composite bases on stress distribution of inlays-a finite element analysis. Braz. Dent. J. 2015, 26, 146–151. [Google Scholar] [CrossRef]
- Alharbi, F.A.; Nathanson, D.; Morgano, S.M.; Baba, N.Z. Fracture resistance and failure mode of fatigued endodontically treated teeth restored with fiber-reinforced resin posts and metallic posts in vitro. Dent. Traumatol. 2014, 30, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, M.; Saidi, A.; Nassab, S.A.G.; Hashemipour, M.A. A three-dimensional finite element analysis of the effects of restorative materials and post geometry on stress distribution in mandibular molar tooth restored with post-core crown. Dent. Mater. J. 2012, 31, 171–179. [Google Scholar] [CrossRef] [PubMed]

| Model | Description | Elements | Nodes |
|---|---|---|---|
| A | Complete butt joint | 3,157,093 | 4,526,045 |
| B | Complete anatomic margin | 2,991,456 | 4,312,502 |
| C | Partial butt joint | 2,700,180 | 3,900,583 |
| D | Partial anatomic margin | 2,857,399 | 4,116,555 |
| E | Partial butt joint and MO cavity | 2,880,944 | 4,146,766 |
| F | Partial anatomic margin and MO cavity | 2,859,467 | 4,116,028 |
| Material | Elastic Modulus (GPa) | Poisson’s Ratio | References |
|---|---|---|---|
| Lithium disilicate | 95 | 0.3 | [22] |
| Resin cement | 7.5 | 0.3 | [37] |
| Enamel | 84.1 | 0.33 | [22] |
| Dentin | 18.6 | 0.31 | [38] |
| Cementum | 15.5 | 0.31 | [20] |
| Gutta-percha | 0.14 | 0.45 | [20,39] |
| Polystyrene resin cylinder | 2.9 | 0.31 | [40] |
| Model Preparation Design | Adhesive Area (mm2) |
|---|---|
| Model A | 136.61 |
| Model B | 154.71 |
| Model C | 127.84 |
| Model D | 141.71 |
| Model E | 131.99 |
| Model F | 143.47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-naqshabandi, F.I.; Selivany, B.J.; Al-zahawi, A.R. Biomechanical Behavior of Lithium-Disilicate-Modified Endocrown Restorations: A Three-Dimensional Finite Element Analysis. Ceramics 2023, 6, 2162-2177. https://doi.org/10.3390/ceramics6040133
Al-naqshabandi FI, Selivany BJ, Al-zahawi AR. Biomechanical Behavior of Lithium-Disilicate-Modified Endocrown Restorations: A Three-Dimensional Finite Element Analysis. Ceramics. 2023; 6(4):2162-2177. https://doi.org/10.3390/ceramics6040133
Chicago/Turabian StyleAl-naqshabandi, Fatien I., Bahar Jaafar Selivany, and Abdulsalam Rasheed Al-zahawi. 2023. "Biomechanical Behavior of Lithium-Disilicate-Modified Endocrown Restorations: A Three-Dimensional Finite Element Analysis" Ceramics 6, no. 4: 2162-2177. https://doi.org/10.3390/ceramics6040133