
Non-Oxide Ceramics for Bone Implant Application: State-of-the-Art Overview with an Emphasis on the Acetabular Cup of Hip Joint Prosthesis

Abstract
:1. Introduction
2. Evolution of Bone Implant Materials and Ceramics for Osseous Applications
3. Design and Challenges Associated with the Acetabular Cup
4. Silicon Carbide
4.1. Major Properties and Production Methods
4.2. Biomedical Applications
4.2.1. Porous Silicon Carbide for Bone Implant Applications
4.2.2. Silicon Carbide Thin Films
5. Silicon Nitride
5.1. Major Properties and Production Methods
5.2. Biomedical Applications
5.2.1. Robocasting of Silicon Nitride and Bone Scaffold Applications
5.2.2. Silicon Nitride for Biomedical Bearing Applications
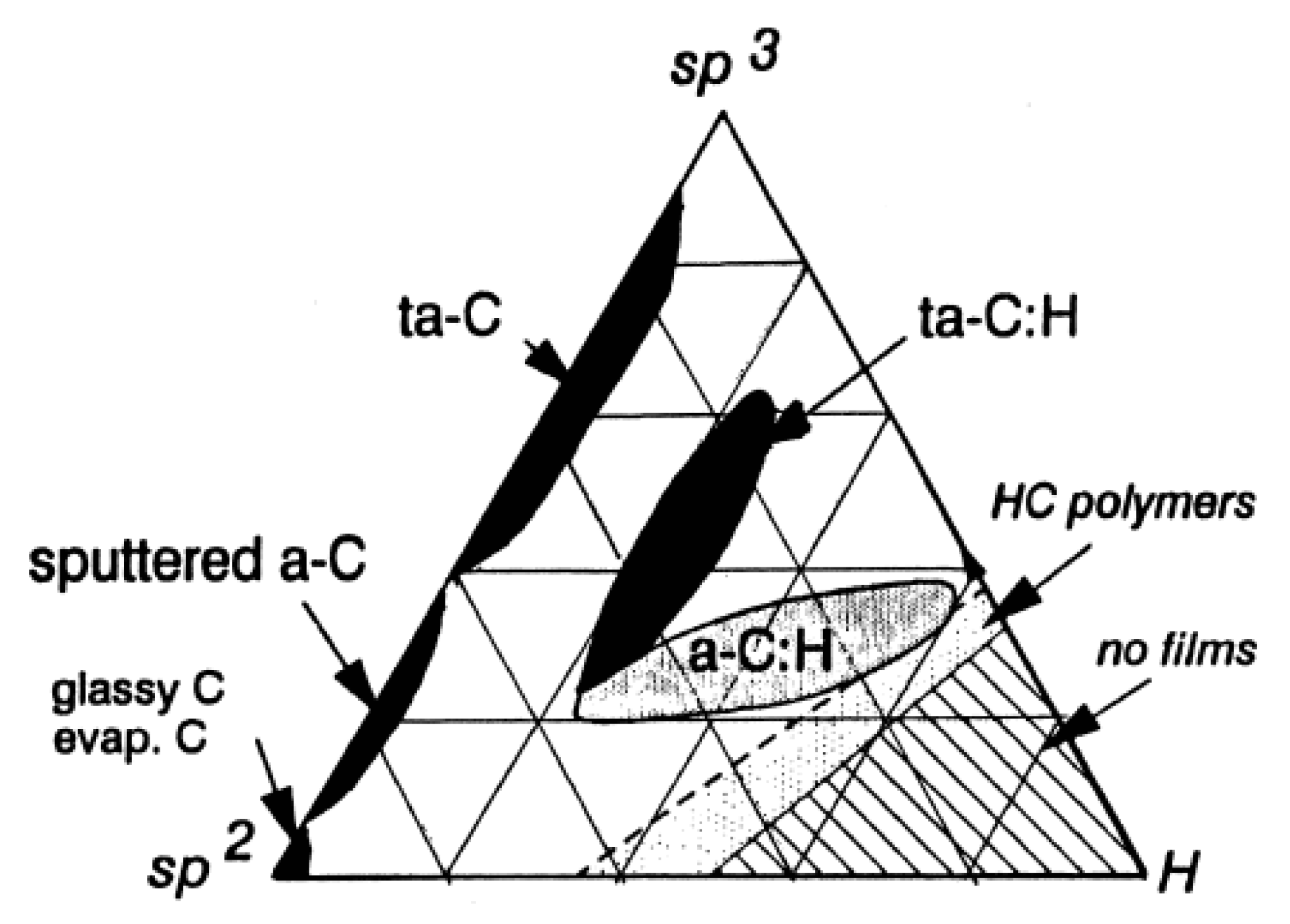
6. Diamond-like Carbon
6.1. Major Properties and Production Methods
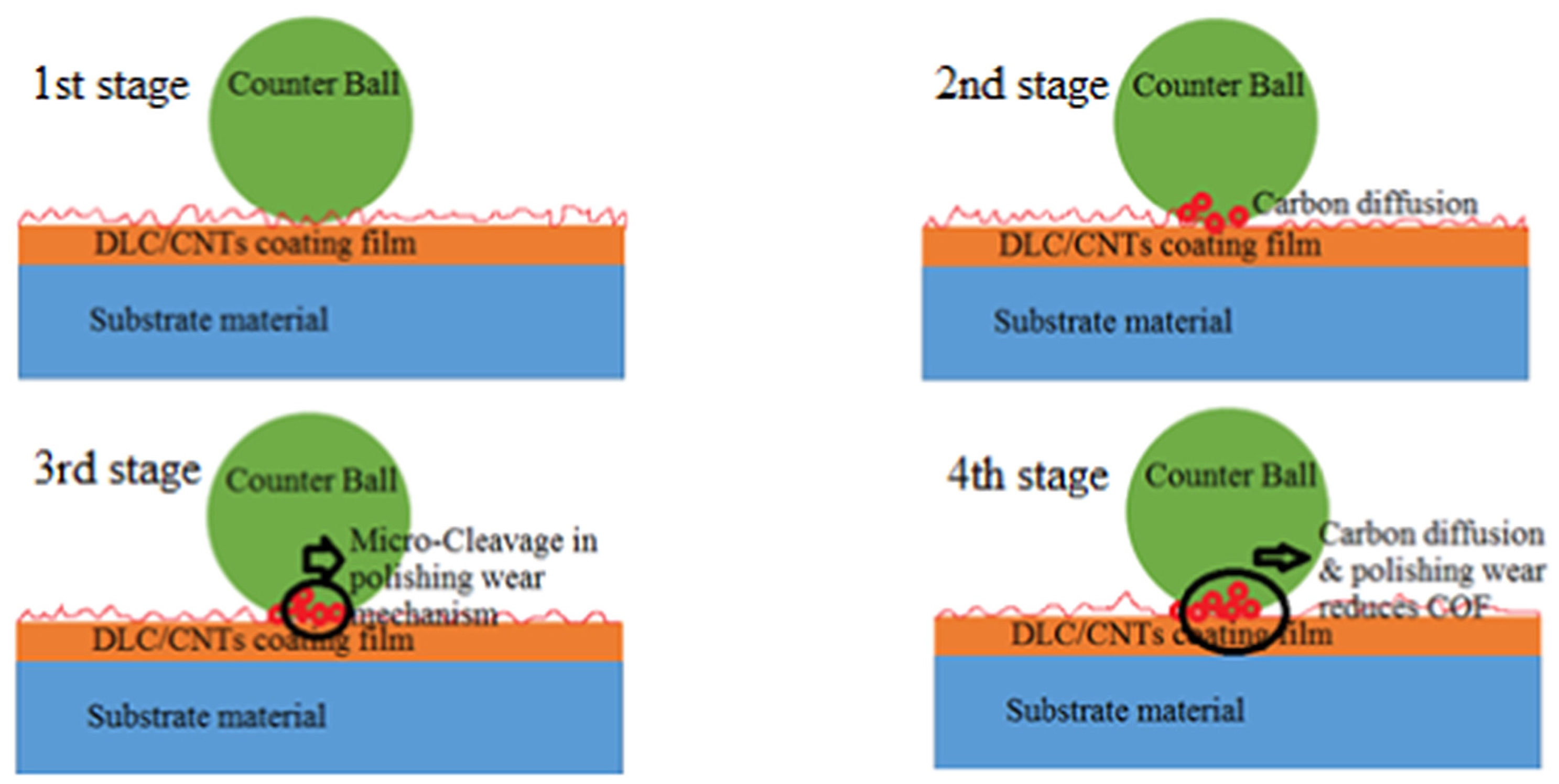
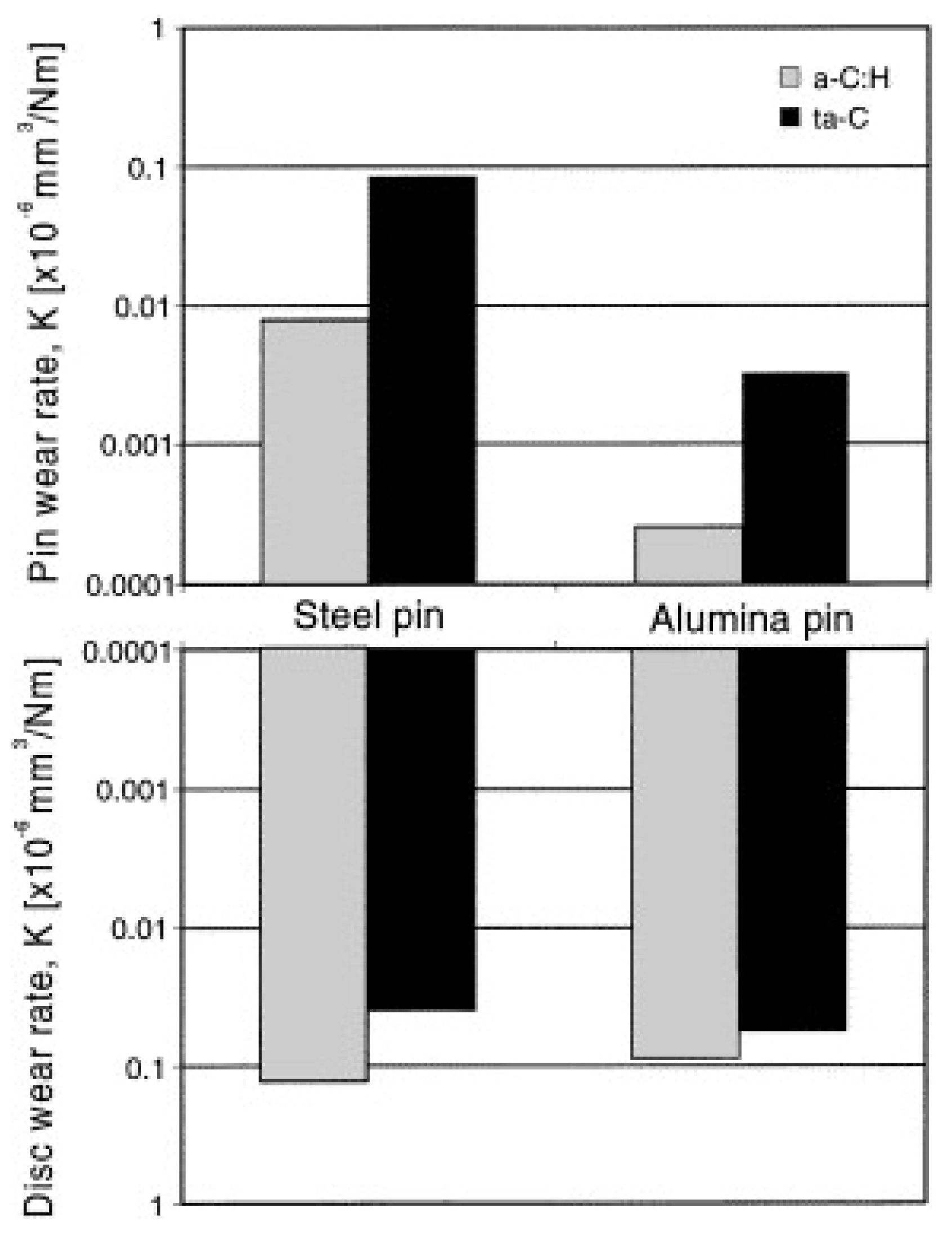
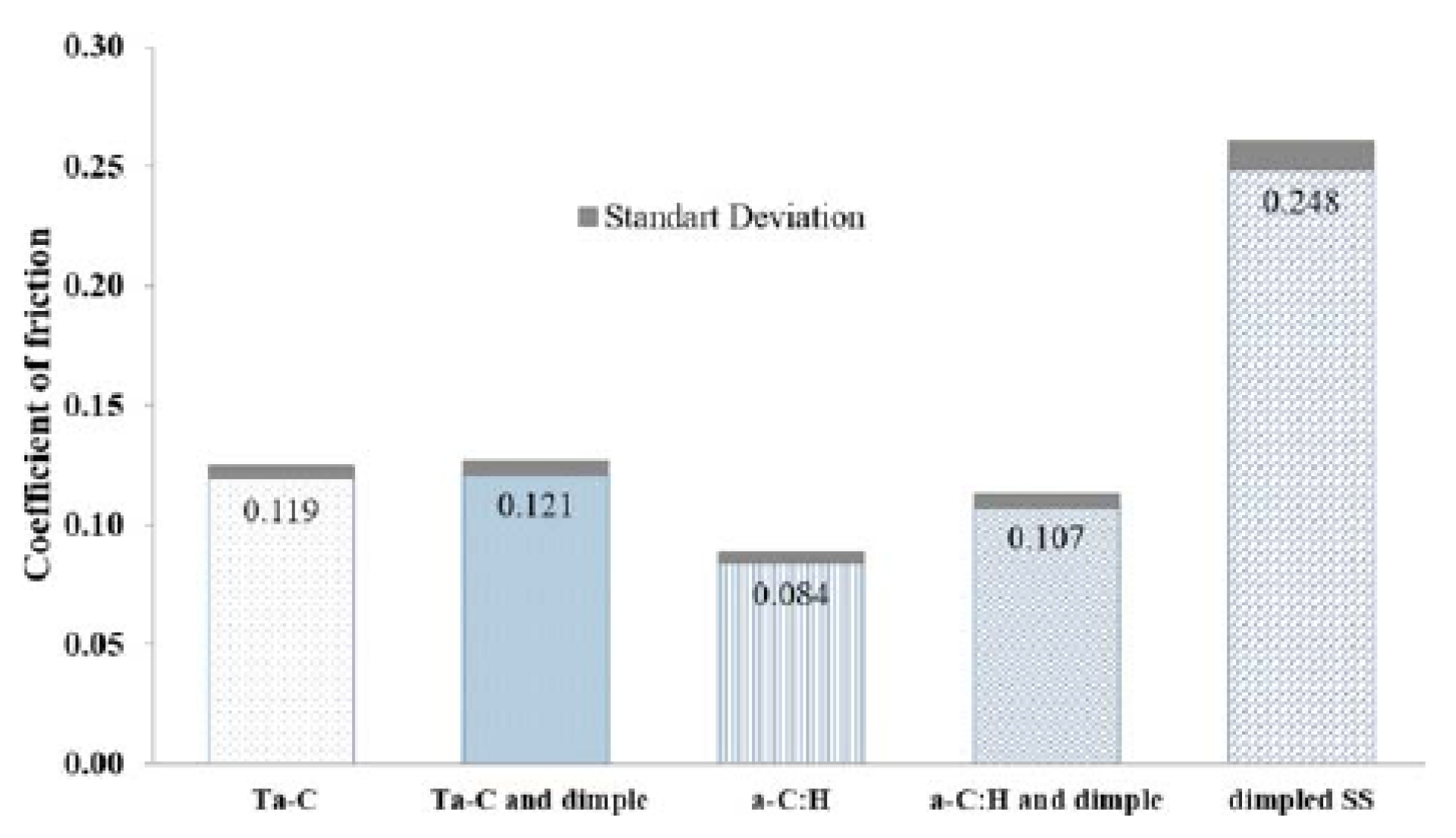
6.2. DLC for Biomedical Bearing Applications
7. Composites
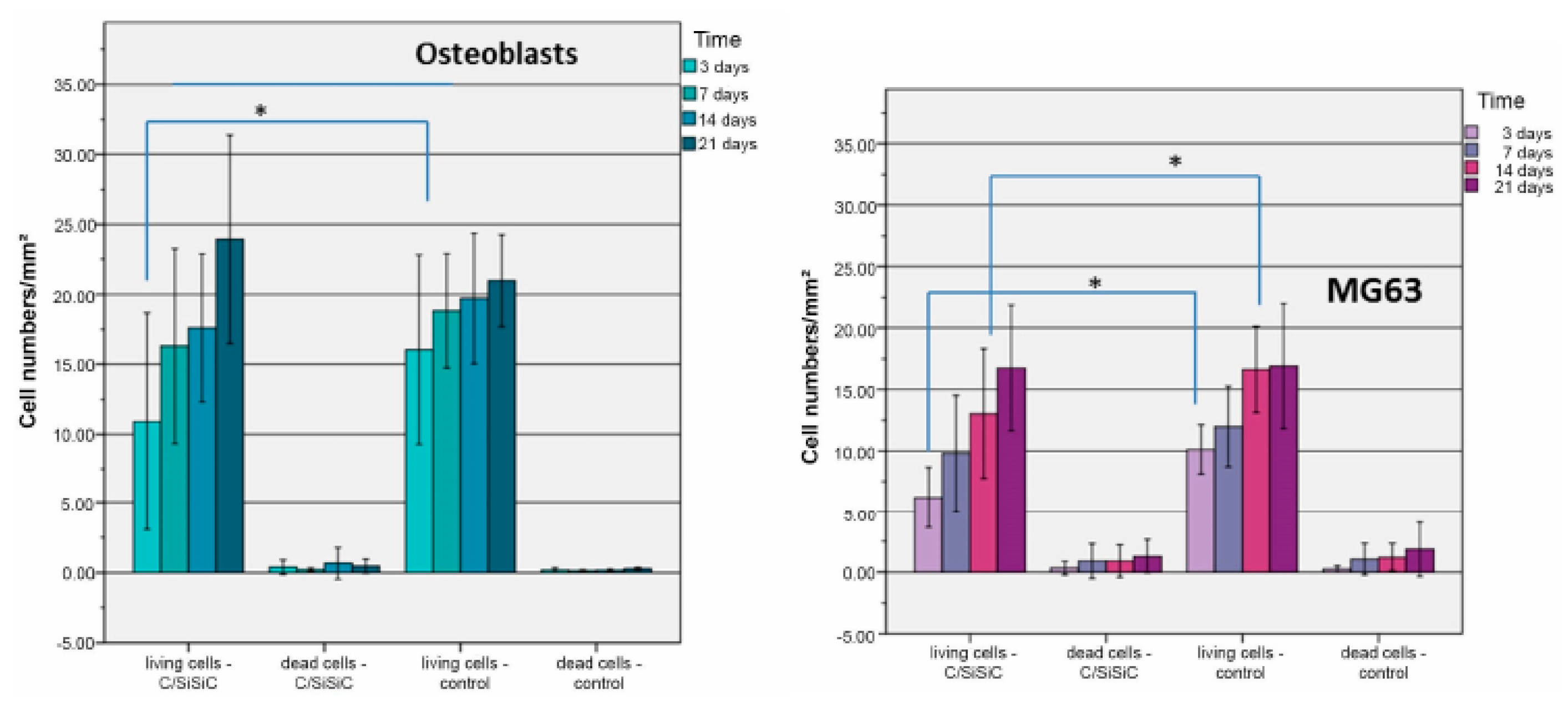
7.1. C/SiC Composites
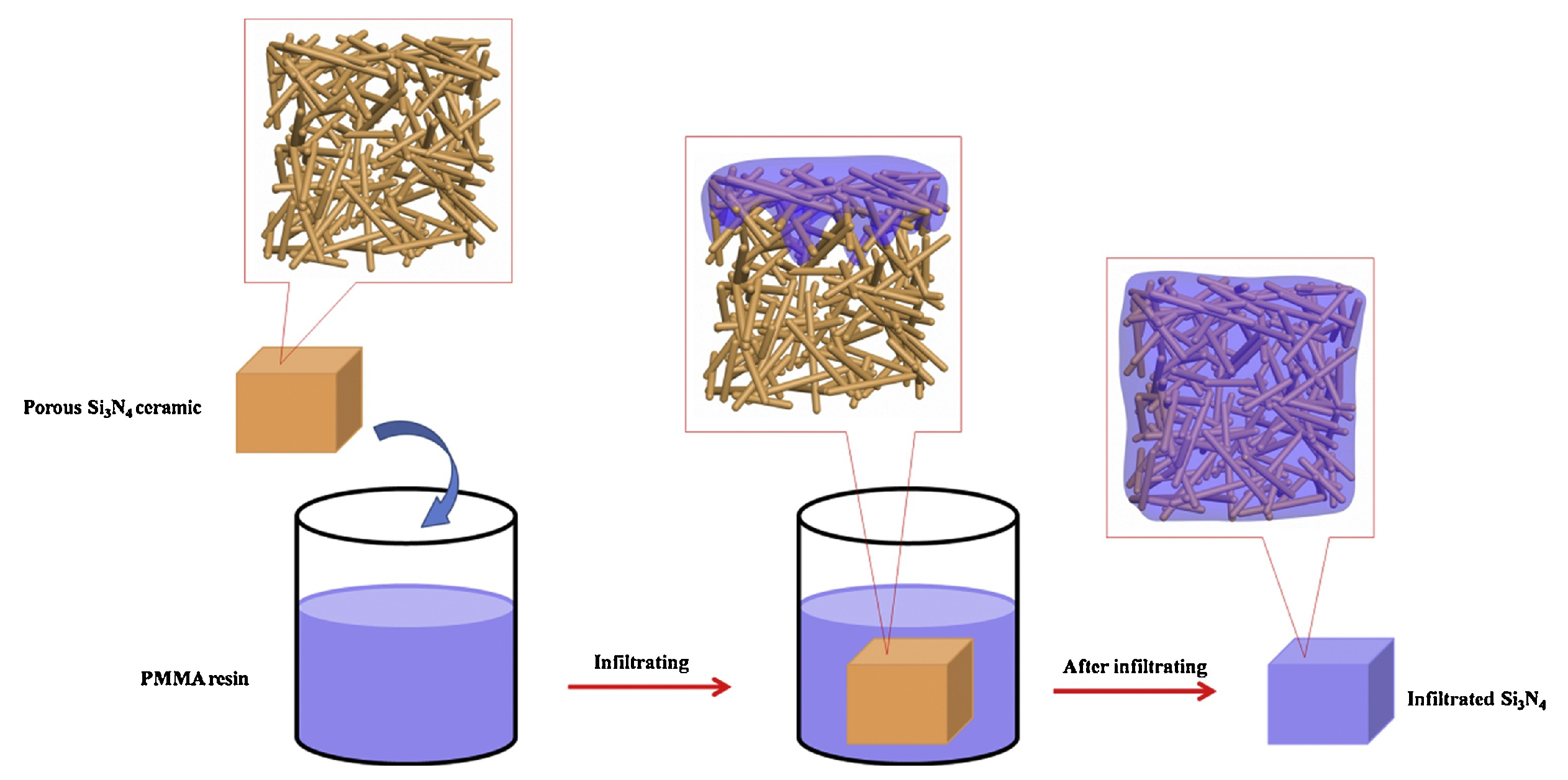
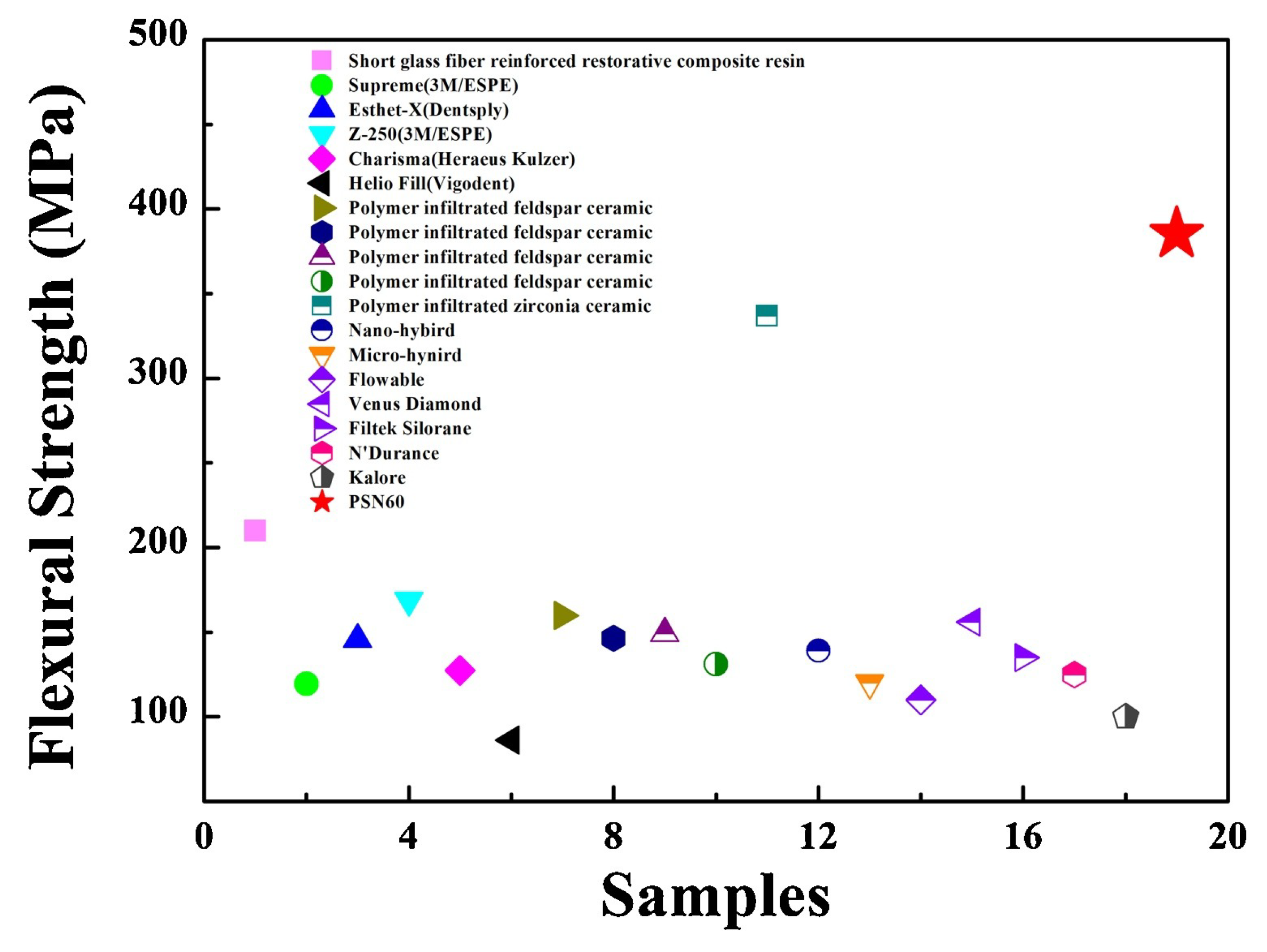
7.2. Polymer-Infiltrated Silicon Nitride Composites
7.3. Alumina-SiC
7.4. SiC/Si3N4
8. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferrand, H.L.; Athanasiou, C.E. A materials perspective on the design of damage-resilient artificial bones and bone implants through additive/advanced manufacturing. J. Miner. Met. Mater. Soc. 2020, 72, 1195–1210. [Google Scholar] [CrossRef]
- Deere, K.; Whitehouse, M.R.; Kunutsor, S.K.; Sayers, A.; Mason, J.; Blom, A.W. How long do revised and multiply revised hip replacements last? A retrospective observational study of the National Joint Registry. Lancet Rheumatol. 2022, 4, e468–e479. [Google Scholar] [CrossRef] [PubMed]
- Duman, S.; Çamurcu, İ.Y.; Uçpunar, H.; Sevencan, A.; Akıncı, Ş.; Şahin, V. Comparison of clinical characteristics and 10-year survival rates of revision hip arthroplasties among revision time groups. Arch. Med. Sci. 2021, 17, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Bronzino, J.D.; Peterson, D.R. The Biomedical Engineering Handbook, 4th ed.; CRC Press: Boca Raton, FL, USA, 2015. [Google Scholar]
- Eliaz, N. Corrosion of Metallic Biomaterials: A Review. Materials 2019, 12, 407. [Google Scholar] [CrossRef]
- Kurtz, S.M. The UHMWPE Handbook: Ultra-High Molecular Weight Polyethylene in Total Joint Replacement; Elsevier Academic Press: San Diego, CL, USA, 2004. [Google Scholar]
- Jackson, J. Father of the modern hip replacement: Professor Sir John Charnley (1911–1982). J. Med. Biogr. 2011, 19, 151–156. [Google Scholar] [CrossRef]
- Sukur, E.; Akman, Y.E.; Ozturkmen, Y.; Kucukdurmaz, F. Particle Disease: A.Current Review of the Biological Mechanisms in Periprosthetic Osteolysis After Hip Arthroplasty. Open Orthop. J. 2016, 10, 241–251. [Google Scholar] [CrossRef]
- Piconi, C. Oxide Ceramics for Biomedical Applications. In Encyclopedia of Materials: Technical Ceramics and Glasses; Elsevier: Amsterdam, The Netherlands, 2021; Volume 3, pp. 511–525. [Google Scholar]
- Hannouche, D.; Zaoui, A.; Zadegan, F.; Sedel, L.; Nizard, R. Thirty years of experience with alumina-on-alumina bearings in total hip arthroplasty. Int. Orthop. 2011, 35, 207–213. [Google Scholar] [CrossRef]
- Montazerian, M.; Hosseinzadeh, F.; Migneco, C.; Fook, M.V.L.; Baino, F. Bioceramic coatings on metallic implants: An overview. Ceram. Int. 2022, 48, 8987–9005. [Google Scholar] [CrossRef]
- Jones, J.R.; Gentleman, E.; Polak, J. Bioactive glass scaffolds for bone regeneration. Elements 2007, 3, 393–399. [Google Scholar] [CrossRef]
- Baino, F.; Fiume, E.; Barberi, J.; Kargozar, S.; Marchi, J.; Massera, J.; Verné, E. Processing methods for making porous bioactive glass-based scaffolds—A state-of-the-art review. Int. J. Appl. Ceram. Technol. 2019, 16, 1762–1796. [Google Scholar] [CrossRef]
- Rezwan, K.; Chen, Q.Z.; Blaker, J.J.; Boccaccini, A.R. Biodegradable and bioactive porous polymer/inorganic composite scaffolds for bone tissue engineering. Biomaterials 2006, 27, 3413–3431. [Google Scholar] [CrossRef] [PubMed]
- Bal, B.S.; Rahaman, M.N. Orthopedic applications of silicon nitride ceramics. Acta Biomater. 2012, 8, 2889–2898. [Google Scholar] [CrossRef] [PubMed]
- Maximilien, E.; Launey, M.J.B.; Ritchie, R.O. On the mechanistic origins of toughness in bone. Annu. Rev. Mater. Res. 2010, 40, 25–53. [Google Scholar]
- OECD. Health at a Glance: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Pezzotti, G.; Yamamoto, K. Artificial hip joints: The biomaterials challenge. J. Mech. Behav. Biomed. Mater. 2014, 31, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Knight, S.R.; Aujla, R.; Biswas, S.P. Total Hip Arthroplasty—Over 100 years of operative history. Orthop. Rev. 2011, 3, 2. [Google Scholar]
- Latham, B.; Goswami, T. Effect of geometric parameters in the design of hip implants-paper IV. Mater. Des. 2006, 25, 287–307. [Google Scholar] [CrossRef]
- Sargeant, A.; Goswami, T. Hip Implants: Paper V. Physiological Effects. Mater. Des. 2006, 25, 287–307. [Google Scholar] [CrossRef]
- Kircher, J.; Bader, R.; Schroeder, B.; Mittelmeier, W. Extremely high fracture rate of a modular acetabular component with a sandwich polyethylene ceramic insertion for THA: A preliminary report. Arch. Orthop. Trauma Surg. 2009, 129, 1145–1150. [Google Scholar] [CrossRef]
- Baino, F.; Minguella, J.; Kirk, N.; Montealegre, M.A.; Fiaschi, C.; Korkusuz, F.; Orlygsson, G.; Vitale-Brovarone, C. Novel full-ceramic monoblock acetabular cup with a bioactive trabecular coating: Design, fabrication and characterization. Ceram. Int. 2016, 42, 6833–6845. [Google Scholar] [CrossRef]
- Clarke, I.C.; Manaka, M.; Green, D.D. Current status of zirconia used in total hip implants. J. Bone Joint Surg. Am. 2003, 85, 73–84. [Google Scholar] [CrossRef]
- Rahman, M.N.; Yao, A.; Bal, B.S.; Garino, J.P.; Ries, N.D. Ceramics for prosthetic hip and knee joint replacement. J. Am. Ceram. Soc. 2007, 90, 1965–1988. [Google Scholar] [CrossRef]
- Bistolfi, A.; Ferracini, R.; Lee, G.C.; Mellano, D.; Guidotti, C.; Baino, F.; Verné, E. Ceramic-on-ceramic catastrophic liner failure in total hip arthroplasty: Morphological and compositional analysis of fractured ceramic components. Ceram. Int. 2021, 47, 11029–11036. [Google Scholar] [CrossRef]
- Saddow, S.E. Silicon Carbide Technology for Advanced Human Healthcare Applications. Micromachines 2022, 13, 346. [Google Scholar] [CrossRef] [PubMed]
- Harris, G.L. Properties of Silicon Carbide; INSPEC: Manchester, UK, 1995; Volume 1, pp. 3–9. [Google Scholar]
- Guichelaar, P.J. Acheson Process. In Carbide, Nitride and Boride Materials Synthesis and Processing; Chapman and Hall: London, UK, 1997; pp. 115–129. [Google Scholar]
- Surek, T. Crystal growth and materials research in photovoltaics: Progress and challenges. J. Cryst. Growth 2005, 275, 292–304. [Google Scholar] [CrossRef]
- Li, H.C.; Chen, W.-S. Recovery of silicon carbide from waste silicon slurry by using flotation. Energy Procedia 2017, 136, 53–59. [Google Scholar] [CrossRef]
- Yalcin, N.; Sevinc, V. Studies on silica obtained from rice husk. Ceram. Int. 2001, 27, 219–224. [Google Scholar] [CrossRef]
- Miller, R.B. Wood Handbook—Wood as an Engineering Material; USDA: Washington, DC, USA, 1999; Volume 2, pp. 2–6. [Google Scholar]
- Greil, P.; Lifka, T.; Kaindl, A. Biomorphic Cellular Silicon Carbide Ceramics from Wood: II Mechanical Properties. J. Eur. Ceram. Soc. 1998, 18, 1975–1983. [Google Scholar] [CrossRef]
- Singh, M.; Salem, J.A. Mechanical properties and microstructure of biomorphic silicon carbide ceramics fabricated from wood precursors. J. Eur. Ceram. Soc. 2002, 22, 2709–2717. [Google Scholar] [CrossRef]
- Kaur, G.; Kumar, V.; Baino, F. Mechanical properties of bioactive glasses, ceramics, glass-ceramics and composites: State of the art review and future challenges. Mater. Sci. Eng. C 2019, 104, 109895. [Google Scholar] [CrossRef]
- Cameron, J.R.; James, G.; Skofronick, R.M.G. Physics of the Body, 2nd ed.; Medical Physics Publishing: Madison, WI, USA, 1999; Volume 96. [Google Scholar]
- Rade, K.; Martinčič, A.; Novak, S.; Kobe, S. Feasibility study of SiC-ceramics as a potential material for bone implants. J. Mater. Sci. 2013, 48, 5295–5301. [Google Scholar] [CrossRef]
- Miguel, B.S.; Kriauciunas, R.; Tosatti, S.; Ehrbar, M.; Ghayor, C.; Textor, M.; Weber, F.E. Enhanced osteoblastic activity and bone regeneration using surface-modified porous bioactive glass scaffolds. J. Biomed. Mater. Res. Part A 2010, 94, 1023. [Google Scholar] [CrossRef] [PubMed]
- Bal, B.S.; Rahaman, M.N.; Jayabalan, P.; Kuroki, K.; Cockrell, M.K.; Yao, J.Q.; Cook, J.L. In vivo outcomes of tissue-engineered osteochondral grafts. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 93, 164–174. [Google Scholar]
- Nordsletten, L.; Høgåsen, A.K.M.; Konttinen, Y.; Santavirta, S.; Aspenberg, P.; Aasen, A.O. Human monocytes stimulation by particles of hydroxyapatite, silicon carbide and diamond: In vitro studies of new prosthesis coatings. Biomaterials 1996, 17, 1521–1527. [Google Scholar] [CrossRef]
- Gryshkov, O.; Klyui, N.I.; Temchenko, V.P.; Kyselov, V.S.; Chatterjee, A.; Belyaev, A.E.; Lauterboeck, L.; Iarmolenko, D.; Glasmacher, B. Porous biomorphic silicon carbide ceramics coated with hydroxyapatite as prospective materials for bone implants. Mater. Sci. Eng. 2016, 68 C, 143–152. [Google Scholar] [CrossRef]
- Hatty, V.; Kahn, H. Fracture toughness of low-pressure chemical-vapor-deposited polycrystalline silicon carbide thin films. J. Appl. Phys. 2006, 99, 013517. [Google Scholar] [CrossRef]
- Oujja, M.; Tabakkouht, K.; Sanz, M.; Rebollar, E.; Sánchez-Arenillas, M.; Marco, J.F.; Castillejo, M.; de Nalda, R. Synthesis of smooth amorphous thin films of silicon carbide with controlled properties through pulsed laser deposition. Appl. Phys. A 2022, 128, 375. [Google Scholar] [CrossRef]
- Wang, W.-X.; Niu, L.-S.; Zhang, Y.-Y.; Lin, E.-Q. Tensile mechanical behaviors of cubic silicon carbide thin films. Comput. Mater. Sci. 2012, 62, 195–202. [Google Scholar] [CrossRef]
- Zhao, L.; Zhang, J.; Pfetzing, J.; Alam, M.; Hartmaier, A. Depth-sensing ductile and brittle deformation in 3C-SiC under Berkovich nanoindentation. Mater. Des. 2021, 197, 109223. [Google Scholar] [CrossRef]
- Heimann, R.B.; Nitride, S. A Close to Ideal Ceramic Material for Medical Application. Ceramics 2021, 4, 208–223. [Google Scholar] [CrossRef]
- Riley, F.L. Silicon Nitride and Related Materials. J. Am. Ceram. Soc. 2000, 83, 245–265. [Google Scholar] [CrossRef]
- Lange, F. The sophistication of ceramic science through silicon nitride studies. J. Ceram. Soc. Jpn. 2006, 114, 873–879. [Google Scholar] [CrossRef]
- Lange, F.F. Relation Between Strength, Fracture Energy, and Microstructure of Hot-Pressed Si3N4. J. Am. Ceram 1973, 56, 518–522. [Google Scholar] [CrossRef]
- Aguirre, T.G.; Cramer, C.L.; Mitchell, D.J. Review of additive manufacturing and densification techniques for the net- and near net-shaping of geometrically complex silicon nitride components. J. Eur. Ceram. Soc. 2022, 42, 735–743. [Google Scholar] [CrossRef]
- Wang, K.J.; Bao, C.G.; Zhang, C.; Li, Y.; Liu, R.; Xu, H.; Song, S. Preparation of high-strength Si3N4 antenna window using selective laser sintering. Ceram. Int. 2021, 47, 28218–28225. [Google Scholar] [CrossRef]
- Zanocco, M.; Boschetto, F.; Zhu, W.; Marin, E.; McEntire, B.J.; Bal, B.S.; Pezzotti, G. 3D-additive deposition of an antibacterial and osteogenic silicon nitride coating on orthopaedic titanium sub-strate. J. Mech. Behav. Biomed. 2020, 103, 103557. [Google Scholar] [CrossRef]
- Xing, H.Y.; Zou, B.; Liu, X. Fabrication strategy of complicated Al2O3 -Si3N4 functionally graded materials by stereolithography 3D printing. J. Eur. Ceram. Soc. 2020, 40, 5797–5809. [Google Scholar] [CrossRef]
- Altun, A.A.; Prochaska, T.; Konegger, T.; Schwentenwein, M. Dense, strong, and precise silicon nitride-based ceramic parts by lithography-based ceramic manufacturing. Appl. Sci. 2020, 10, 996. [Google Scholar] [CrossRef]
- Chen, R.F.; Duan, W.Y.; Wang, G.; Liu, B.; Zhao, Y.; Li, S. Preparation of broadband transparent Si3N4 -SiO2 ceramics by digital light processing (DLP) 3D printing technology. J. Eur. Ceram. Soc. 2021, 41, 5495–5504. [Google Scholar] [CrossRef]
- Xiao, S.S.; Mei, H.; Han, D.; Yuan, W.; Cheng, L. Porous(SiCw-Si3N4w )/(Si3N4-SiC) composite with enhanced mechanical performance fabricated by 3D printing. Ceram. Int. 2018, 44, 14122–14127. [Google Scholar] [CrossRef]
- Peng, E.; Zhang, D.; Ding, J. Ceramic robocasting: Recent achievements, potential, and future developments. Adv. Mater. 2018, 30, 1802404. [Google Scholar] [CrossRef]
- Sainz, M.A.; Serena, S.; Belmonte, M.; Miranzo, P.; Osendi, M.I. Protein adsorption and in vitro behavior of additively manufactured 3D-silicon nitride scaffolds intended for bone tissue engineering. Mater. Sci. Eng. C 2020, 115, 110734. [Google Scholar] [CrossRef]
- Zhao, S.; Xiao, W.; Rahaman, M.N.; O’Brien, D.; Seitz-Sampson, J.W.; Bal, B.S. Robocasting of silicon nitride with controllable shape and architecture for biomedical applications. Appl. Ceram. Technol. 2017, 14, 117–127. [Google Scholar] [CrossRef]
- Baino, F.; Novajra, G.; Vitale-Brovarone, C. Bioceramics and scaffolds, a winning combination for tissue engineering. Front. Bioeng. Biotechnol. 2015, 3, 202. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Titze, M.; Cappi, B.; Wirtz, D.C.; Telle, R.; Fischer, H. Improved mechanical long-term reliability of hip resurfacing prostheses by using silicon nitride. J. Mater. Sci. Mater. Med. 2010, 21, 3049–3057. [Google Scholar] [CrossRef] [PubMed]
- Bal, B.S.; Khandkar, A.; Lakshminarayanan, R.; Clarke, I.; Hoffman, A.A.; Rahaman, M.N. Testing of silicon nitride ceramic bearings for total hip arthroplasty. J. Biomed. Mater. Res. B 2008, 87, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Park, D.S.; Danyluk, S.; McNallan, M.J. Influence of tribochemical reaction products on friction and wear of silicon nitride at elevated temperatures in reactive environments. J. Am. Ceram. Soc. 1992, 75, 3033–3039. [Google Scholar] [CrossRef]
- Tomizawa, H.; Fischer, T.E.; Trans, A. Friction and Wear of Silicon Nitride and Silicon Carbide in Water: Hydrodynamic Lubrication at Low Sliding Speed Obtained by Tribochemical Wear. ASLE Trans. 1988, 30, 41–46. [Google Scholar]
- Zhou, Y.S.; Ohashi, M.; Tomita, N.; Ikeuchi, K.; Takashima, K. Study on the possibility of silicon nitride-silicon nitride as a material for hip prostheses. Mater. Sci. Eng. 1997, 5 C, 125–129. [Google Scholar] [CrossRef]
- Neumann, A.; Jahnke, K.; Maier, H.R.; Ragoß, C. Biocompatibility of silicon nitride ceramic in vitro. A comparative fluorescence-microscopic and scanning. Laryngorhinootologie 2004, 83, 845–851. [Google Scholar] [CrossRef]
- Neumann, A.; Reske, T.; Held, M.; Jahnke, K.; Ragoss, C.; Maier, H.R. Comparative investigation of the biocompatibility of various silicon nitride ceramic qualities in vitro. J. Mater. Sci. Mater. Med. 2004, 15, 1135–1140. [Google Scholar] [CrossRef]
- Kue, R.; Sohrabi, A.; Nagle, D.; Frondoza, C.; Hungerford, D. Enhanced proliferation and osteocalcin production by human osteoblast-like MG63 cells on silicon nitride ceramic discs. Biomaterials 1999, 20, 1195–1201. [Google Scholar] [CrossRef]
- Kong, X.; Hu, X.; Chai, W. In Vitro & In Vivo investigation of the silicon nitride ceramic hip implant’s safety and effectiveness evaluation. J. Orthop. Surg. Res. 2022, 17, 87. [Google Scholar] [PubMed]
- Grill, A. Diamond-like carbon: State of the art. Diam. Relat. Mater. 1999, 8, 428–434. [Google Scholar] [CrossRef]
- Aisenberg, S.; Chabot, R. Ion-Beam Deposition of Thin Films of Diamondlike Carbon. J. Appl. Phys. 1971, 42, 2953–2958. [Google Scholar] [CrossRef]
- Hahn, S.S.-H.; Madeira, J.; Chou, C.P.; Brooks, L.E. Razor Blade Technology. US Patent 5669144, 7 November 1995. [Google Scholar]
- Angus, J.C.; Jansen, F. Dense “diamondlike” hydrocarbons as random covalent networks. J. Vac. Sci. Technol. 1988, 6, 1778–1782. [Google Scholar] [CrossRef]
- Robertson, J.; O’Reilly, E.P. Electronic and atomic structure of amorphous carbon. Phys Rev. B 1987, 35, 2946–2957. [Google Scholar] [CrossRef]
- Tyagi, A.; Walia, R.S.; Murtaza, Q.; Pandey, S.M.; Tyagi, P.K.; Bajaj, B. A critical review of diamond like carbon coating for wear resistance applications. Int. J. Refract. Met. Hard Mater. 2019, 78, 107–122. [Google Scholar] [CrossRef]
- Ronkainen, H.; Varjus, S.; Koskinen, J.; Holmberg, K. Differentiating the tribological performance of hydrogenated and hydrogen-free DLC coatings. Wear 2001, 249, 260–266. [Google Scholar] [CrossRef]
- Kunze, T.; Posselt, M.; Gemming, S.; Seifert, G.; Konicek, A.R.; Carpick, R.W.; Pastewka, L.; Moseler, M. Wear, Plasticity and Rehybridization in Tetrahedral Amorphous Carbon. Tribol. Lett. 2014, 53, 119–126. [Google Scholar] [CrossRef]
- Liu, Y.; Erdemir, A.; Meletis, E.I. Influence of environmental parameters on the frictional behavior of DLC coatings. Surf. Coat. Technol. 1997, 94–95, 463–468. [Google Scholar] [CrossRef]
- Choudhury, D.; Ching, H.A.; Mamat, A.B.; Cizek, J.; Osman, N.A.A.; Vrbka, M.; Hartl, M.; Krupka, I. Fabrication and characterization of DLC coated microdimples on hip prosthesis heads. J. Biomed. Mater. Res. Part B 2015, 103, 1002–1012. [Google Scholar] [CrossRef]
- Rubstein, A.P.; Makarova, E.B.; Trakhtenberg, I.S.; Kudryavtseva, I.P.; Bliznets, D.G.; Philippov, Y.I.; Shlykov, I.L. Osseointegration of porous titanium modified by diamond-like carbon and carbon nitride. Diam. Relat. Mater. 2012, 22, 128–135. [Google Scholar] [CrossRef]
- Liao, T.T. Biological responses of diamond-like carbon (DLC) films with different structures in biomedical application. Mater. Sci. Eng. 2016, C 69, 751–759. [Google Scholar] [CrossRef]
- Taeger, G.; Podleska, L.E.; Schmidt, B.; Ziegler, M.; Nast-Kolb, D. Comparison of diamond-like carbon and alumina oxide articulating with polyethylene in total hip anthroplasty. Matwiss. Werkst. 2003, 34, 1094–1100. [Google Scholar] [CrossRef]
- Berndt, W.K.F. C/C–SiC composites for space applications and advanced friction systems. Mater. Sci. Eng. 2005, A 412, 177–181. [Google Scholar]
- Reichert, A.; Seidenstuecker, M.; Gadow, R.; Mayr, H.O.; Suedkamp, N.P.; Latorre, S.H.; Weichand, P.; Bernstein, A. Carbon-Fibre-Reinforced SiC Composite (C/SiSiC) as an Alternative Material for Endoprosthesis: Fabrication, Mechanical and In-Vitro Biological Properties. Materials 2018, 11, 316. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Guo, J.; Li, K.; Sun, J.; Zeng, Y.; Ning, C. High strength polymer/silicon nitride composites for dental restorations. Dent. Mater. 2019, 35, 1254–1263. [Google Scholar] [CrossRef] [PubMed]
- Reilly, D.T.; Burstein, A.H.; Frankel, V.H. The elastic modulus for bone. J. Biomech. 1974, 7, 271–275. [Google Scholar] [CrossRef]
- Crispim da Silveira, O.; Rodrigues, A.M.; Montazerian, M.; de Lucena Lira, H.; Baino, F.; Menezes, R.R. Al2O3 preforms infiltated with polymethyl methacrilate for dental prosthesis manufacturing. Appl. Sci. 2021, 11, 7583. [Google Scholar] [CrossRef]
- Niihara, K. New Design Concept of Structural Ceramics–Ceramic Nanocomposites. J. Ceram. Soc. Jpn. 1991, 99, 974–982. [Google Scholar] [CrossRef]
- Niihara, K.; Nakahira, A. Strengthening and toughening mechanisms in nanocomposite ceramics. Ann. Chim. 1991, 16, 479–486. [Google Scholar]
- Zhao, J.; Stearns, L.C.; Harmer, M.P.; Chan, H.M.; Miller, G.A.; Cook, R.F. Mechanical Behavior of Alumina–Silicon Carbide Nanocomposites. J. Am. Ceram Soc. 1993, 76, 503–510. [Google Scholar] [CrossRef]
- Davidge, R.W.; Twigg, P.C.; Riley, F.L. Effects of Silicon Carbide Nano-phase on the Wet Erosive Wear of Polycrystalline Alumina. J. Eur. Ceram. Soc. 1996, 16, 799–802. [Google Scholar] [CrossRef]
- Davidge, R.W.; Riley, F.L. Grain-Size Dependence of the Wear of Alumina. Wear 1995, 45, 186–187. [Google Scholar] [CrossRef]
- O’Sullivan, D.; Hampshire, S.; Kennedy, T. Fabrication, Properties, and Modeling of Engineering Ceramics Reinforced with Nanoparticles of Silicon Carbide. Br. Ceram. Trans. 1996, 96, 121–127. [Google Scholar]
- Sternitzke, M.; Dupas, E.; Twigg, P.; Derby, B. Surface Mechanical Properties of Alumina Matrix Nanocomposites. Acta Mater. 1997, 45, 3963–3973. [Google Scholar] [CrossRef]
- Rodríguez, J.; Martín, A.; Pastor, J.Y.; Llorca, J.; Bartolomé, J.F.; Moya, J.S. Sliding Wear of Alumina/Silicon Carbide Nanocomposites. J. Am.Ceram. Soc. 1999, 82, 2252–2254. [Google Scholar] [CrossRef]
- Greskovich, C.; Palm, J.A. Observations on the Fracture Toughness of b-Si3N4–b-SiC Composites. J. Am. Ceram. Soc. 1980, 63, 597–599. [Google Scholar] [CrossRef]
- Sasaki, G.; Nakase, H.; Suganuma, K.; Fujita, T.; Niihara, K. Mechanical Properties and Microstructure of Si3N4 Matrix Composite with Nanometer Scale SiC Particles. J. Ceram. Soc. Jpn. 1992, 100, 536–540. [Google Scholar] [CrossRef]
- Hirano, T.; Niihara, K. Microstructure and Mechanical Properties of Si3N4/SiC Composites. Mater. Lett. 1995, 22, 249–254. [Google Scholar] [CrossRef]
- Sawaguchi, K.T.; Niihara, K. Mechanical and Electrical Properties of Silicon Nitride–Silicon Carbide Nanocomposite Material. Mater. Lett. 1991, 74, 1142–1144. [Google Scholar] [CrossRef]
- El-Desouky, I.I. Ten-year survival of ceramic-on-ceramic total hip arthroplasty in patients younger than 60 years: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2021, 16, 679. [Google Scholar] [CrossRef] [PubMed]
- Ely, K.S.; Khandkar, A.C.; Lakshminarayanan, R.; Hofmann, A.A. Hip Prosthesis with Monoblock Ceramic Acetabular Cup. U.S. Patent No. 7695521, 13 April 2010. [Google Scholar]
- Padture, N.P. In Situ-Toughened Silicon Carbide. J. Am. Ceram. Soc. 1994, 77, 519–523. [Google Scholar] [CrossRef]
- Kusaka, J.; Takashima, K.; Yamane, D.; Ikeuchi, K. Fundamental study for all-ceramic artificial hip joint. Wear 1999, 225–229, 734–742. [Google Scholar] [CrossRef]
- Grossin, D.; Montón, A.; Navarrete-Segado, P.; Özmen, E.; Urruth, G.; Maury, F.; Maury, D.; Frances, C.; Tourbin, M.; Lenormand, P.; et al. A review of additive manufacturing of ceramics by powder bed selective laser processing (sintering/melting): Calcium phosphate, silicon carbide, zirconia, alumina, and their composites. Open Ceram. 2021, 5, 100073. [Google Scholar] [CrossRef]
- Love, C.A.; Cook, R.B.; Harvey, T.J.; Dearnley, P.A.; Wood, R.J.K. Diamond like carbon coatings for potential application in biological implants—A review. Tribol. Int. 2013, 63, 141–150. [Google Scholar] [CrossRef]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Elastic Modulus [GPa] | Tensile Strength [MPa] | Compressive Strength [MPa] | Fracture Toughness [MPa · m] | Biological Behaviour |
|---|---|---|---|---|---|
| Alumina | 400–450 | 250–300 | 2000–3000 | 4–5 | inert |
| Zirconia | 210 | 700 | 2000 | 8 | inert |
| Hydroxyapatite | 100 | 40 | 400 | 1 | bioactive (osteoconductive) |
| 45S5 Bioglass | 35 | 45 | 500 | 0.5–1 | bioactive (osteoinductive) |
| Materials | Density [kg/m3] | Elastic Modulus [GPa] | Tensile Strength [MPa] | Compressive Strength [MPa] | Flexural Strength [MPa] | Fracture Toughness [MPa · m] |
|---|---|---|---|---|---|---|
| Si3N4 | 3150–3260 | 300–320 | 350–400 | 2500–3000 | 800–1100 | 8–11 |
| SiC | 3050 | 420 | - | 3900 | 280–428 | 4.6 |
| Al2O3 | 3986 | 400–450 | 250–300 | 2000–3000 | 300–500 | 4–5 |
| ZTA | 4370 | 350 | - | 4300 | 1000 | 5.7 |
| CoCr | 8500 | 210–250 | - | 600–1800 | - | 50–100 |
| PEEK | 1290 | 4.2 | 100–110 | 130–140 | 160–180 | - |
| Ti-alloy | 4430 | 105–115 | 920–980 | 950–990 | - | 75 |
| Bone | 1900 | 8–12 | 50–130 | 130–190 | - | 1.7–5 |
| Ceramic Type | Pros | Cons |
|---|---|---|
| Si3N4 | Higher toughness than SiC, alumina, ZTA, DLC | Relatively higher friction coefficient compared with alumina, SiC |
| Higher osteoconductivity than alumina, SiC, DLC | Relatively higher wear rate compared to SiC, alumina, DLC | |
| SiC | Similar friction coefficient to alumina | Not osteoconductive, requires HA coating like alumina |
| Can also be toughened to ZTA levels | More expensive than alumina, Si3N4 | |
| DLC | Lowest friction coefficient | Requires high hardness counter-surfaces, like alumina or Si3N4 |
| Lowest wear rate | Conflicting clinical evidence |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paione, C.M.; Baino, F. Non-Oxide Ceramics for Bone Implant Application: State-of-the-Art Overview with an Emphasis on the Acetabular Cup of Hip Joint Prosthesis. Ceramics 2023, 6, 994-1016. https://doi.org/10.3390/ceramics6020059
Paione CM, Baino F. Non-Oxide Ceramics for Bone Implant Application: State-of-the-Art Overview with an Emphasis on the Acetabular Cup of Hip Joint Prosthesis. Ceramics. 2023; 6(2):994-1016. https://doi.org/10.3390/ceramics6020059
Chicago/Turabian StylePaione, Consiglio M., and Francesco Baino. 2023. "Non-Oxide Ceramics for Bone Implant Application: State-of-the-Art Overview with an Emphasis on the Acetabular Cup of Hip Joint Prosthesis" Ceramics 6, no. 2: 994-1016. https://doi.org/10.3390/ceramics6020059