
A Qualitative Study on the Implementation of the Workplace TB Program in the Philippines: Challenges and Way Forward
 , and
, and
Abstract
:1. Introduction
Philippine Health System and TB in the Workplace Policy
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Data Processing and Analysis
2.4. Ethical Considerations
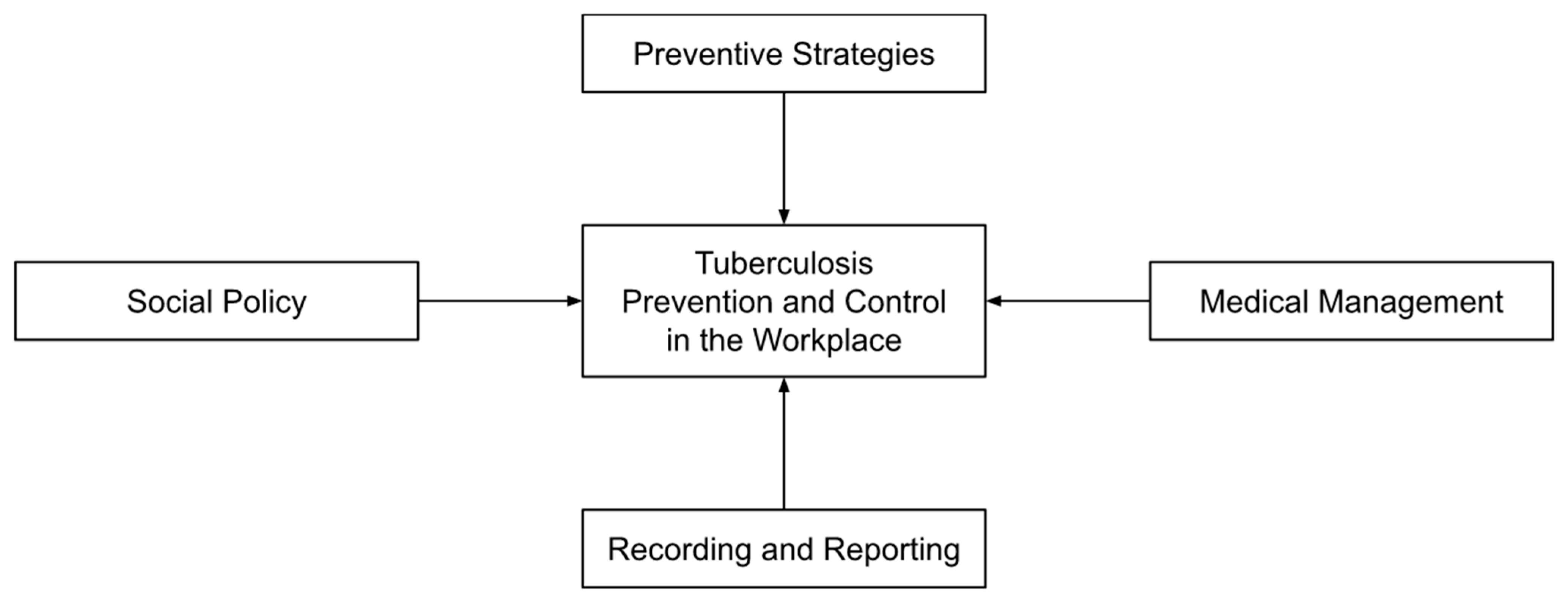
3. Results
3.1. Preventive Strategies
3.1.1. Inconsistencies in TB Guidelines
“That’s another challenge—the private [companies] involvement in the TB [in the workplace] Program because they have other—they have separate guidelines that they follow. Although we try to meet with them so that we can include them in trainings.”(DOH Program Personnel, Regional Office)
3.1.2. Importance of Company Support
“Due to the COVID prevention, we intensified the provision of proper ventilation of work areas, because there are some areas that we discovered are not properly ventilate[d]…I think it helped us install additional [TB] control measures for proper ventilation…We also have these Pi tags being given to our control room and power plant personnel…It is a social distancing device. If you get within one meter of each other, it will be recorded [alarm], so it is a reminder for them to keep [a] distance [of] at least one meter for COVID prevention.”(Health and Safety Officer, Company 4)
“We have annual WEM, or work environment monitoring. After the results, we analyze those parameters that fail and make corrective actions…We also monitor the area for ventilation if it’s adequate or not.”(Health and Safety Officer, Company 1)
3.1.3. Limited Conduct and Participation in Meetings and Capacity-Building Initiatives
“That’s also a slight frustration of mine. At the national level, DOH calls for regular meetings so national government agencies meet from time to time—at least at a minimum of four meetings—convene four times a year, so required once per quarter. But once you get to the regional level, it’s not like that. The enthusiasm at the national level is not mirrored at the regional level but that’s my impression. If only we could mirror the CUP (Comprehensive and Unified Policy) [on TB control] at the national level, we could translate and bring our discussions at the central office, [at the] national level, [with] national government agencies, to the grassroots, perhaps the implementation of the program from the regional office to the local government units will be more seamless.”(DOLE Program Personnel, National Office)
“So far, there isn’t [any training]. I suddenly got embarrassed. There’s none because—there isn’t anyone conducting training [for TB]. [It’s an] overall [training], not specifically for TB. So last time there was a training by [mentions office] on emerging health condition…it was like overall, not specific for TB only…In fairness, this is a good point—there’s like a gap. It’s good that DOH together with LGU has [a training] but for us [in DOLE], there’s no forever because we’re really lacking in interagency connection.”(DOLE Program Personnel, Regional Office)
“Sometimes for example, there is no budget, so we conduct the training but with our resource persons or we usually do the training per province, then the resource persons for that [companies] are the provincial coordinators”(DOH Program Personnel, Regional Office)
“Also the big ones [companies], like [company name], they can’t just attend anytime.”(Program Personnel, Provincial Health Office)
“Yes, that’s why it [communication with companies] is a problem, their personnel gets replaced to the point that we do not know [anyone]...because we do not know to whom we will address the letter since it’s different personnel…it would be better that they inform us who the new head is so that we can [write to them], so it would not be difficult for us, we do not usually know whom we would address in the letter that’s why our [program] stopped.”(Program Personnel, Provincial Health Office)
“Pre-COVID time, we partnered with the City Health Office. So in the City Health Office, they really are personnel in charge of IEC…We conducted annual lecture[s] to all workers.”(Health and Safety Officer, Company 4).
“They [Rural Health Unit] used to have a team for education, everything… campaigns against TB, prevention methods… But it [RHU TB Service] has not been functioning lately because there has not been follow-up training from DOTS [center].”(Security, Safety, and Health Officer, Company 2)
3.1.4. Missed Establishments for Inspection
“Let’s say our target is 76,000 [establishments] and let’s say we’ve surpassed that [and were] able to inspect 80,000+ establishments. But versus the universe of establishments that were given to us by the DTI (Department of Trade and Industry) of 900,000+, we’ve only roughly inspected around 10%. That’s what I was saying that most of what we haven’t been able to inspect were those that are called micro establishments because DTI said that around 94–96% are SMEs (small and mid-size enterprises). Only a few were large and medium establishments which are that we are able to cover since they have a lot of workers.”(DOLE Program Personnel, National Office)
“Apart from these, another challenge were those that are not listed under DOLE…which is the basis of our inspection since that is the database [for inspection] by our field offices and regional offices…These micro establishments are missed not only for TB but also for other programs under the DOLE. Even until now, we are perplexed on how we will reach them. It’s very hard to find them.”(DOLE Program Personnel, National Office)
3.2. Medical Management
3.2.1. Limited Personnel
“The thing is, the CHD level is like the overall monitoring of the program… usually the CHD NTP coordinator, they still have other programs to handle…yes it’s the personnel/people that would help or would focus on the initiatives because they could no longer focus or look into the other health programs, especially now that we have the COVID-19 pandemic. That’s why the other programs are neglected, not only with TB.”(DOH Program Personnel—01, National Office)
“For example, he’s a skilled worker. He is really needed. So how are we going to balance? He cannot report to work first. We inform his immediate supervisor that he should not report to work… We talk to the management to always consider the employee first… Health and safety first over productivity.”(Health and Safety Officer, Company 4)
3.2.2. Resource Availability
“The availability of the medicine, [that’s a challenge] because for instance, there’s someone diagnosed but [it falls to] the availability of free medicine. We have TB DOTS facilities wherein they cater for free. The tendency for others is that they don’t have [medicines] available.”(DOLE Program Personnel, Regional Office)
“Funding for PTB (pulmonary tuberculosis), for treatment…We are lacking in medicines… [If that happens, these will be] out of pocket.”(Program Nurse Coordinator, Municipality 2)
3.2.3. Issues with High Pill Burden
“They don’t like that—15 capsules. ‘There should be 3-in-1 like that.’ So others, they’re very choosy.”(DOLE Program Personnel, Regional Office)
3.2.4. Service Delivery Challenges in the Pandemic
“…the treatment partners were able to adjust. If before they gave [tablets] every day, in the pandemic they gave weekly as to limit [patients] going out [of their homes].”(DOLE Program Personnel, National Office)
“Last year we were not able to participate [in TB active case finding activities], because the mayor did not permit…They [active case finding activities] can cause crowding.”(NTP Nurse Coordinator, Municipality 1)
3.3. Recording and Reporting
3.3.1. Limited Programmatic Coordination and Data Integration
“The information system, how we get the data from DOLE, from workplaces… the data for TB… which is supposed to be integrated, which has a component for integration. We also have [a] connection with SSS, GSIS. That is what is still being fixed in the information system.”(DOH Program Personnel—01, National Office)
“Even us, we cannot figure out because the implementation of the program in DOH is very vertical. So when I say vertical, it is disease-specific. So in the infectious disease division, they have these diseases of public health significance that they focus on, like for example here we are talking about TB. And also, the strategy of DOH, it is community-based. Every service and strategy would be implemented starting at the community level, that’s why we have the rural health units, our government hospitals who provide services for these. So that is the slight gray area with us, our interface when it comes to the occupational health and TB program, because they are disease-specific while OH (occupational health) [is not]…”(DOH Program Personnel—02, National Office)
“Of course, DOH is advocating for coordination at all levels, so the workplace should have coordination with—they should have a partnership with a health facility, coordination with the LGU, because when it comes to the permits—health permits, you get it from the LGU, and then, with the CHD technical assistance, so there. We really need partnerships from all levels. But with DOH, in the LGU, there is no direct [connection] with them, it is with the CHD that we are connected with.”(DOH Program Personnel—01, National Office)
“What they are saying is there are no more cases there are none, so I said, why don’t we, we coordinate with these companies, because sometimes, that’s the thing, they are not… what do you call it, they are not that involved.”(DOH Program Personnel, Regional Office)
“We have direct communication with the local government unit because we know that they also have TB DOTS. That would be first [we contact]. Then usually with the provincial health office since our physician is connected with them… Not much coordination with DOH…With DOLE, we submit reports like the annual medical report.”(Health and Safety Officer, Company 2)
“Here in DOH, they are part of the RCC—Regional Coordinating Committee along with DOLE. They have a meeting every quarter. That’s where they have coordination for the program and between agencies…[However,] the last meeting of the RCC was still in February 2020. Maybe they need to re-activate it and push the TB in the workplace program.”(DOH Program Personnel—03, National Office)
3.3.2. Limited Jurisdiction by DOH on Establishments
“The information gathered from private entities were limited. If DOLE were to spearhead a program with strict monitoring on medical checkups of companies for employees, there is limited power of DOH over those facilities. Maybe [it would be good] if DOH would be given linkage or authority by DOLE.”(DOH Program Personnel—03, National Office)
3.3.3. Limited Compliance
“For instance, when there are findings in the [chest] x-ray, they [companies] refer [to physicians] but they do not have a referral form. Official referral forms are distributed to them, but they remain unused.”(Program Nurse Coordinator, Municipality 2)
3.3.4. Incomplete Data Reported
“It’s either the name of the facility, or the source of the TB case. But the thing is, there are facilities that don’t include the name of the facility, so you don’t really get the complete picture of it is from the workplace or not.”(DOH Program Personnel—01, National Office)
“It’s not [accurate] anymore…[It] could be underreporting.”(DOH Program Personnel—01, National Office)
“The private sector is a different thing, because while this is institutionalized in the private sector, the problem is with micro enterprises, they are required to have OSH established in their workplace or establishment. Although it will entail resources that the medium, small, and micro enterprises don’t have.”(DOH Program Personnel—02, National Office)
“The challenge with that I think is…the public sector since it’s not yet established and with the medium, small and micro enterprises, how or where will they go for these services…So with the surveillance part, I don’t know how you would implement it for those that don’t have the established system, for example in the private medium, small or micro, [and] in the informal sector...”(DOH Program Personnel—02, National Office)
“I’m also not sure if they are also issuing notices of violation, if they don’t submit will they issue something…Our policies should have fangs, because so what if we will follow or not. If you would say that it’s for your own good, it’s for your employees’ health, welfare, and things like that, but those are just, so to speak, additional burden, except maybe for the big companies, it’s quite manageable, but that’s the thing, who will monitor…There are already templated policies…there is just a need for it to have claws, for someone to enforce them.”(DOH Program Personnel, Regional Office)
“Age is also not there [in the reporting system]. We have no means to identify and that is still a challenge for us. I keep telling DOH whenever they say that there is missing [data] from us that if they improve their reporting system—put if the patient is working or not, what industry they’re in—then we could identify which industries we need to give attention.”(DOLE Program Personnel, National Office)
3.4. Social Policy
3.4.1. Importance of Social Policy Provisions
“Of course, it’s not only a health issue. It also includes rights issues—that you won’t be suddenly terminated from work just because you have TB, which is curable—so it also includes issues against discrimination and of course work accommodation for days that you will need to submit sputum, do follow-up check-ups with a DOTS physician. Flexibility will be given by the workplace either flexi-time or earlier work shifts so that the patient could complete the eight work hours and go to the DOTS facility or it could also be in between [work hours].”(DOLE Program Personnel, Regional Office)
“For example, if the employee is in a graveyard shift, we have to take care of that and take into consideration all the environmental factors that will speed up his healing. We assign him to a work shift that is most convenient to him while recovering.”(Health and Safety Officer, Company 1)
3.4.2. Stigma against TB-Positive Individuals
“The stigma of having TB is still there. When they get infected with TB, they are ashamed to let their community know that they have the TB disease.”(City health program personnel, LGU 4)
“Actually we have infectious disease guidelines in our head office. There’s the “no discrimination” policy among HIV and TB. So we have these guidelines installed... As long as they are properly treated and have obtained clearance, they can go back to work.”(Health and Safety Officer, Company 4)
3.4.3. Limited Knowledge on TB Benefits
“There are instances that they [employees] are not fully aware that once you’re a TB patient, you can file it under SSS [Social Security System]. So, for instance, they don’t—all they focus on is the negative—the negative aspect, ‘Oh no, another expense, oh no, I cannot work,’ but the positive [aspect] is that medications are free, then they also have compensation from SSS. So yes, it’s more on awareness, proper… information dissemination is what’s needed.”(DOLE Program Personnel, Regional Office)
3.4.4. Consultation with Experts
“We also have templates on posters and IEC materials but of course we work with other partners on these types of things since this is their specialty—how to work within sociocultural norms, behavioral change communication. They’re more experienced in that.”(DOLE Program Personnel, National Office)
“We also invite somebody from external agencies to lecture in the seminar. We invite everybody… We also invite the LGUs to lecture. For the contractors, they also have their separate lecture if they want. But we invite everyone for the lectures… Sometimes the DOH invites us whenever they have seminars”(Health and Safety Officer, Company 4)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramirez-Lapausa, M.; Menendez-Saldana, A.; Noguerado-Asensio, A. Extrapulmonary Tuberculosis: An Overview. Am. Fam. Physician 2015, 17, 1761–1768. [Google Scholar]
- World Health Organization. Global Tuberculosis Report. 2022. Available online: http://apps.who.int/bookorders (accessed on 21 March 2020).
- Maher, D.; Boldrini, F.; Pathania, V.; Alli, B.O. Guidelines for Workplace TB Control Activities: The Contribution of Workplace TB Control Activities to TB Control in the Community; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- World Health Organization. TB Control in the Workplace: Report of an Intercountry Consultation; WHO: New Delhi, India, 2004. [Google Scholar]
- Republic of the Philippines. Republic Act No. 7160: The Local Government Code of 1991; Republic of the Philippines: Manila, Philippines, 1991; pp. 1–281. [Google Scholar]
- Department of Health. National Tuberculosis Control Program. Available online: https://ntp.doh.gov.ph/about-ntp/ (accessed on 28 December 2022).
- Department of Labor and Employment. Department Order No. 131-B: Revised Rules on Labor Laws Compliance System; Department of Labor and Employment: Manila, Philippines, 2016; pp. 1–35. [Google Scholar]
- Republic of the Philippines. Executive Order No. 187: Instituting a Comprehensive and Unified Policy for the Tuberculosis Control in the Philippines; Republic of the Philippines: Manila, Philippines, 2003; pp. 1–2. [Google Scholar]
- Department of Health; Philippine Coalition Against Tuberculosis. Comprehensive and Unified Policy for TB Control in the Philippines; Department of Health: Manila, Philippines, 2004. [Google Scholar]
- Department of Labor and Employment. Department Order No. 73-05: Guidelines for the Implementation of Policy and Program on Tuberculosis (TB) Prevention and Control in the Workplace; Department of Labor and Employment: Manila, Philippines, 2005; pp. 1–10. [Google Scholar]
- Department of Health. National Tuberculosis Control Program: Manual of Procedures, 6th ed.; Department of Health: Manila, Philippines, 2021. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Zinatsa, F.; Engelbrecht, M.; Van Rensburg, A.J.; Kigozi, G. Voices from the frontline: Barriers and strategies to improve tuberculosis infection control in primary health care facilities in South Africa. BMC Health Serv. Res. 2018, 18, 269. [Google Scholar] [CrossRef] [PubMed]
- Philippine Statistics Authority. Occupational Safety and Health Practices in Establishments: CY 2015; Philippine Statistics Authority: Quezon City, Philippines, 2018. [Google Scholar]
- Philippine Statistics Authority. Highlights of the 2019/2020 Integrated Survey on Labor and Employment (ISLE)—Module on Occupational Safety and Health Practices (OSHP): 2019; Philippine Statistics Authority: Quezon City, Philippines, 2022. [Google Scholar]
- Mwenya, S.; Stapley, S. An exploration of health workers risks of contracting tuberculosis in the workplace: A qualitative study. BMC Health Serv. Res. 2020, 20, 1037. [Google Scholar] [CrossRef] [PubMed]
- Lota, M.M.M.; Chua, A.Q.; Azupardo, K.; Lumangaya, C.; Reyes, K.A.V.; Villanueva, S.Y.A.M.; Legido-Quigley, H.; Roxas, E.A. A Qualitative Study on the Design and Implementation of the National Action Plan on Antimicrobial Resistance in the Philippines. Antibiotics 2022, 11, 820. [Google Scholar] [CrossRef]
- World Health Organization. The Philippines Health System Review; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Endo, Y.; Jaramillo, J.; Yadav, R.P.H. Patient- and Health-System-Related Barriers to Treatment Adherence for Patients with Drug-Resistant Tuberculosis in the Philippines: A Mixed-Methods Study. Tuberc. Res. Treat. 2022, 2022, 6466960. [Google Scholar] [CrossRef] [PubMed]
- Guevarra, J.P.; Castillo, E.C.; Antonio, C.A.T.; Ting, M.A.L.; Cavinta, L.L.; Lara, A.B.; Eugenio, K.P.Y.; Tomanan, K.J.L.; Diez, M.V.V.; Garfin, A.M.C.G.; et al. Tuberculosis Case Finding and Case Holding Practices in Selected Drug Abuse Treatment and Rehabilitation Centers (DATRCS) In Luzon, Philippines. Acta Medica Philipp. 2021, 56, 56–63. [Google Scholar] [CrossRef]
- Department of Health. DOH Reports 18% Increase in TB Treatment Amid Pandemic; Seeks More Funds to End TB. Available online: https://doh.gov.ph/Press-release/DOH-REPORTS-18%25-INCREASE-IN-TB-TREATMENT-AMID-PANDEMIC-SEEKS-MORE-FUNDS-TO-END-TB (accessed on 28 February 2022).
- World Health Organization. Impact of the COVID-19 Pandemic on TB Detection and Mortality in 2020; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar] [CrossRef]
- Portero, J.L.; Rubio, M. Private practitioners and tuberculosis control in the Philippines: Strangers when they meet? Trop. Med. Int. Health 2003, 8, 329–335. [Google Scholar] [CrossRef] [PubMed]
- International Labor Organization. Improving Safety and Health in Micro-, Small and Medium-Sized Enterprises: An Overview of Initiatives and Delivery Mechanisms; International Labor Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Hernandez, P.M.R.; Quizon, R.R.; Lacsamana, G.C.; Remaneses, J.I. Occupational Health Systems across Selected Public Healthcare Facilities in the Philippines. Acta Med. Philipp. 2014, 48, 43–51. [Google Scholar] [CrossRef]
- Carter, D.J.; Glaziou, P.; Lönnroth, K.; Siroka, A.; Floyd, K.; Weil, D.; Raviglione, M.; Houben, R.M.G.J.; Boccia, D. The impact of social protection and poverty elimination on global tuberculosis incidence: A statistical modelling analysis of Sustainable Development Goal 1. Lancet Glob. Health 2018, 6, e514–e522. [Google Scholar] [CrossRef] [Green Version]
- Cotton, A.; Sohail, M.; Scott, R. Towards improved labour standards for construction of minor works in low income countries. Eng. Constr. Arch. Manag. 2005, 12, 617–632. [Google Scholar] [CrossRef] [Green Version]
- Anti-Red Tape Authority. ARTA, FDA to Deputize LGUs to Conduct MSME Inspections—Anti-Red Tape Authority. Available online: https://arta.gov.ph/press-releases/arta-fda-to-deputize-lgus-to-conduct-msme-inspections/ (accessed on 4 December 2022).
- Pan American Health Organization. Why Data Disaggregation Is Key during a Pandemic; Pan American Health Organization: Washington, DC, USA, 2020; Available online: https://iris.paho.org/handle/10665.2/52002 (accessed on 26 January 2023).
- World Health Organization. Implementing the End TB Strategy—The Essentials; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- International Labour Organization. Making Universal Social Protection a Reality for People Living with, at the Risk of, and Affected by HIV or Tuberculosis; International Labour Organization: Geneva, Switzerland, 2021; Available online: www.ilo.org/publns (accessed on 4 December 2022).
- World Health Organization. Tuberculosis and COVID-19: Considerations for Tuberculosis (TB) Care; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Kindig, D.; Isham, G.; Siemering, K.Q. The Business Role in Improving Health: Beyond Social Responsibility. NAM Perspect. 2013, 3. [Google Scholar] [CrossRef]
- Ruhwald, M.; Hannay, E.; Sarin, S.; Kao, K.; Sen, R.; Chadha, S. Considerations for simultaneous testing of COVID-19 and tuberculosis in high-burden countries. Lancet Glob. Health 2022, 10, e465–e466. [Google Scholar] [CrossRef] [PubMed]
- MacLean, E.L.; Villa-Castillo, L.; Ruhwald, M.; Ugarte-Gil, C.; Pai, M. Integrated testing for TB and COVID-19. Med 2022, 3, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Echeverría, G.; Espinoza, W.; De Waard, J. How TB and COVID-19 compare: An opportunity to integrate both control programmes. Int. J. Tuberc. Lung Dis. 2020, 24, 971–974. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Health | Labor * | Other | |
|---|---|---|---|
| National | 3 | 1 | n/a |
| Regional | 1 | 1 | n/a |
| Provincial | 2 | n/a | n/a |
| City/Municipality | 5 | n/a | n/a |
| Company | n/a | n/a | 5 |
| Theme | Subthemes |
|---|---|
| Preventive Strategies |
|
| Medical Management |
|
| Recording and Reporting |
|
| Social Policy |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roxas, E.A.; Fadrilan-Camacho, V.F.F.; Lota, M.M.M.; Hernandez, P.M.R.; Agravante, A.P.M.; Loterio, L.M.M.; Arevalo, M.J.; Maglalang, R.L.F.; Lumangaya, C.R.; Belizario, V.Y., Jr. A Qualitative Study on the Implementation of the Workplace TB Program in the Philippines: Challenges and Way Forward. Trop. Med. Infect. Dis. 2023, 8, 93. https://doi.org/10.3390/tropicalmed8020093
Roxas EA, Fadrilan-Camacho VFF, Lota MMM, Hernandez PMR, Agravante APM, Loterio LMM, Arevalo MJ, Maglalang RLF, Lumangaya CR, Belizario VY Jr. A Qualitative Study on the Implementation of the Workplace TB Program in the Philippines: Challenges and Way Forward. Tropical Medicine and Infectious Disease. 2023; 8(2):93. https://doi.org/10.3390/tropicalmed8020093
Chicago/Turabian StyleRoxas, Evalyn A., Vivien Fe F. Fadrilan-Camacho, Maria Margarita M. Lota, Paul Michael R. Hernandez, Adrian Paul M. Agravante, Loisse Mikaela M. Loterio, Micaela J. Arevalo, Richelle Liza F. Maglalang, Carlo R. Lumangaya, and Vicente Y. Belizario, Jr. 2023. "A Qualitative Study on the Implementation of the Workplace TB Program in the Philippines: Challenges and Way Forward" Tropical Medicine and Infectious Disease 8, no. 2: 93. https://doi.org/10.3390/tropicalmed8020093