
Missing Cases of Bacteriologically Confirmed TB/DR-TB from the National Treatment Registers in West and North Sumatra Provinces, Indonesia

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Study Setting
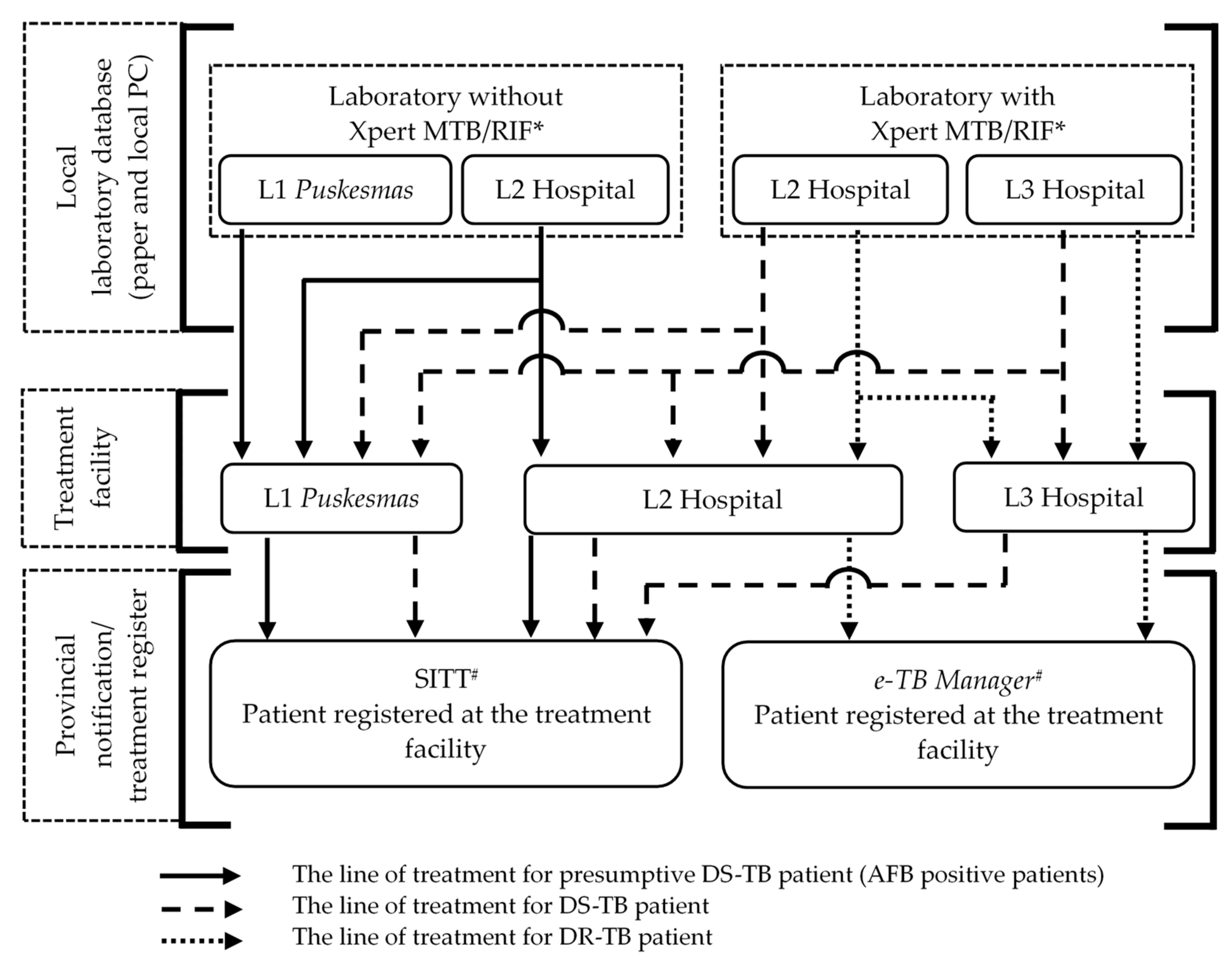
2.3. Health System for TB Diagnosis and Treatment
2.4. Study Population and Sampling Process
2.5. Data Source and Flow
2.6. Analysis of Matching Records
2.7. Soundex Analysis
2.8. The Jaro–Winkler String Distance
2.9. Cut Point and Accuracy of the Jaro–Winkler Distance
2.10. Linkage Laboratory to Treatment Register
2.11. Analysis of Predictors for Missing Cases
2.12. Ethical Consideration
3. Results
3.1. Data Sources
3.2. Cut Point for the Soundex String Distance
3.3. Cascade of Patients and Missing DS-TB/DR-TB Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Furin, J.; Cox, H.; Pai, M. Tuberculosis. Lancet 2019, 393, 1642–1656. [Google Scholar] [CrossRef] [PubMed]
- Tiemersma, E.W.; van der Werf, M.J.; Borgdorff, M.W.; Williams, B.G.; Nagelkerke, N.J. Natural History of Tuberculosis: Duration and Fatality of Untreated Pulmonary Tuberculosis in HIV Negative Patients: A Systematic Review. PLoS ONE 2011, 6, e17601. [Google Scholar] [CrossRef]
- World Health Organization. Global Tuberculosis Report 2022; World Health Organization: Geneva, Switzerland, 2022; ISBN 978-92-4-006172-9. [Google Scholar]
- Chin, D.P.; Hanson, C.L. Finding the Missing Tuberculosis Patients. J. Infect. Dis. 2017, 216, S675–S678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, S.; Mokaddas, E. Recent Advances in the Diagnosis and Treatment of Multidrug-Resistant Tuberculosis. Respir. Med. 2009, 103, 1777–1790. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The End TB Strategy; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Uplekar, M.; Atre, S.; Wells, W.A.; Weil, D.; Lopez, R.; Migliori, G.B.; Raviglione, M. Mandatory Tuberculosis Case Notification in High Tuberculosis-Incidence Countries: Policy and Practice. Eur. Respir. J. 2016, 48, 1571–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacPherson, P.; Houben, R.M.G.J.; Glynn, J.R.; Corbett, E.L.; Kranzer, K. Pre-Treatment Loss to Follow-up in Tuberculosis Patients in Low-and Lower-Middle-Income Countries and High-Burden Countries: A Systematic Review and Meta-Analysis. Bull. World Health Organ. 2013, 92, 126–138. [Google Scholar] [CrossRef]
- Tollefson, D.; Ngari, F.; Mwakala, M.; Gethi, D.; Kipruto, H.; Cain, K.; Bloss, E. Under-Reporting of Sputum Smear-Positive Tuberculosis Cases in Kenya. Int. J. Tuberc. Lung Dis. 2016, 20, 1334–1341. [Google Scholar] [CrossRef]
- Bassili, A.; Grant, A.D.; El-Mohgazy, E.; Galal, A.; Glaziou, P.; Seita, A.; Abubakar, I.; Bierrenbach, A.L.; Crofts, J.P.; van Hest, N.A. Estimating Tuberculosis Case Detection Rate in Resource-Limited Countries: A Capture-Recapture Study in Egypt. Int. J. Tuberc. Lung Dis. 2010, 14, 727–732. [Google Scholar]
- Masini, E.; Hanson, C.; Ogoro, J.; Brown, J.; Ngari, F.; Mingkwan, P.; Makayova, J.; Osberg, M. Using Patient-Pathway Analysis to Inform a Differentiated Program Response to Tuberculosis: The Case of Kenya. J. Infect. Dis. 2017, 216, S714–S723. [Google Scholar] [CrossRef]
- Hanson, C.; Osberg, M.; Brown, J.; Durham, G.; Chin, D.P. Finding the Missing Patients with Tuberculosis: Lessons Learned From Patient-Pathway Analyses in 5 Countries. J. Infect. Dis. 2017, 216, S686–S695. [Google Scholar] [CrossRef] [Green Version]
- Htwe, K.K.; Kyaw, N.T.T.; Kumar, A.M.V.; Kyaw, K.W.Y.; Oo, M.M.; Thwin, T.; Saw, S.; Aung, S.T. Pre-Treatment Loss to Follow-up and Treatment Delay among Bacteriologically-Confirmed Tuberculosis Patients Diagnosed in Mandalay Region, Myanmar. Trop. Med. Health 2019, 47, 30. [Google Scholar] [CrossRef]
- Nadjib, M.; Dewi, R.K.; Setiawan, E.; Miko, T.Y.; Putri, S.; Hadisoemarto, P.F.; Sari, E.R.; Pujiyanto; Martina, R.; Syamsi, L.N. Cost and Affordability of Scaling up Tuberculosis Diagnosis Using Xpert MTB/RIF Testing in West Java, Indonesia. PLoS ONE 2022, 17, e0264912. [Google Scholar] [CrossRef] [PubMed]
- Soeroto, A.Y.; Lestari, B.W.; Santoso, P.; Chaidir, L.; Andriyoko, B.; Alisjahbana, B.; van Crevel, R.; Hill, P.C. Evaluation of Xpert MTB-RIF Guided Diagnosis and Treatment of Rifampicin-Resistant Tuberculosis in Indonesia: A Retrospective Cohort Study. PLoS ONE 2019, 14, e0213017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusumawati, R.L.; Tania, T.; McNeil, E.; Chongsuvivatwong, V. Predictors of Multidrug Resistance among Pulmonary Tuberculosis Patients in a Tertiary Hospital in North Sumatera, Indonesia. Bali Med. J. 2018, 7, 68–73. [Google Scholar] [CrossRef]
- MOH Indonesia. Strategi Nasional Penanggulangan Tuberculosis Di Indonesia 2020-2024; MOH Indonesia: Jakarta, Indonesia, 2020. [Google Scholar]
- MOH Indonesia. Profil Kesehatan Indonesia 2021; MOH Indonesia: Jakarta, Indonesia, 2022. [Google Scholar]
- Soundex System | National Archives. Available online: https://www.archives.gov/research/census/soundex (accessed on 8 March 2022).
- Van der Loo, M.P.J. The Stringdist Package for Approximate String Matching. R J. 2014, 6, 111–122. [Google Scholar]
- Jaro, M.A. Advances in Record-Linkage Methodology as Applied to Matching the 1985 Census of Tampa, Florida. J. Am. Stat. Assoc. 1989, 84, 414–420. [Google Scholar] [CrossRef]
- Sadinle, M.; Fienberg, S.E. A Generalized Fellegi-Sunter Framework for Multiple Record Linkage with Application to Homicide Record Systems. J. Am. Stat. Assoc. 2013, 108, 385–397. [Google Scholar] [CrossRef] [Green Version]
- William, E.W.; Thibaudeau, Y. An Application of the Fellegi-Sunter Model of Record Linkage to the 1990 US Decennial Census; U.S. Bureau of the Census: Suitland, MD, USA, 1991. [Google Scholar]
- van der Loo, M.; van der Laan, J.; Team, R.C.; Logan, N.; Muir, C. Package ‘Stringdist’. Available online: https://cran.r-project.org/web/packages/stringdist/index.html (accessed on 20 September 2022).
- Cox, S.; Martin, R.; Somaia, P.; Smith, K. The Development of a Data-Matching Algorithm to Define the ‘Case Patient. ’ Aust. Health Rev. 2013, 37, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.M.F.; Porto Filho, C.H.; Cozin, L.F.; Pereyra, L.C.; De Azevedo Marques, P.M. Deterministic Record Linkage versus Similarity Functions: A Study in Health Databases from Brazil. In Studies in Health Technology and Informatics; IOS Press: Amsterdam, The Netherlands, 2013; Volume 192. [Google Scholar]
- Jain, A.K.; Jaggi, K.R.; Bhayana, H.; Saha, R. Drug-Resistant Spinal Tuberculosis. Indian J. Orthop. 2018, 52, 100–107. [Google Scholar] [CrossRef]
- Waruru, A.; Natukunda, A.; Nyagah, L.M.; Kellogg, T.A.; Zielinski-Gutierrez, E.; Waruiru, W.; Masamaro, K.; Harklerode, R.; Odhiambo, J.; Manders, E.J.; et al. Where No Universal Health Care Identifier Exists: Comparison and Determination of the Utility of Score-Based Persons Matching Algorithms Using Demographic Data. JMIR Public Health Surveill 2018, 4, e10436. [Google Scholar] [CrossRef] [PubMed]
- Helgertz, J.; Price, J.; Wellington, J.; Thompson, K.J.; Ruggles, S.; Fitch, C.A. A New Strategy for Linking U.S. Historical Censuses: A Case Study for the IPUMS Multigenerational Longitudinal Panel. Hist. Methods 2022, 55, 12–59. [Google Scholar] [CrossRef] [PubMed]
- MOH Indonesia. Technical Guidance for TB Examination Using Molecular Rapid Tests; Indonesia Ministri of Health: Jakarta, Indonesia, 2017. [Google Scholar]
- Nikolayevskyy, V.; Kontsevaya, I.; Nikolaevskaya, E.; Surkova, E.; Samchenko, S.; Esipenko, S. Diagnostic Performance and Impact of Routinely Implemented Xpert® MTB/RIF Assay in a Setting of High Incidence of Drug-Resistant TB in Odessa Oblast, Ukraine. Clin. Microbiol. Infect. 2019, 25, 1040.e1–1040.e6. [Google Scholar] [CrossRef] [PubMed]
- Subbaraman, R.; Jhaveri, T.; Nathavitharana, R.R. Closing Gaps in the Tuberculosis Care Cascade: An Action-Oriented Research Agenda. J. Clin. Tuberc. Other Mycobact. Dis. 2020, 19, 100144. [Google Scholar] [CrossRef] [PubMed]
- Yellappa, V.; Lefèvre, P.; Battaglioli, T.; Devadasan, N.; Van der Stuyft, P. Patients Pathways to Tuberculosis Diagnosis and Treatment in a Fragmented Health System: A Qualitative Study from a South Indian District. BMC Public Health 2017, 17, 635. [Google Scholar] [CrossRef] [Green Version]
- National TB Program; The Republic of Indonesia Joint External Monitoring Mission for Tuberculosis; MOH Indonesia: Jakarta, Indonesia, 2020; pp. 1–105.
- World Health Organization. Global Tuberculosis Report; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Numpong, S.; Toutchon, Y.; Sungkhabut, W. A Systematic Literature Review of the Diagnosis of Drug Resistant Tuberculosis Using Xpert MTB/RIF Assay and Its Potential Impacts on Treatment Outcomes. Dis. Control. J. 2020, 46, 303–312. [Google Scholar] [CrossRef]
- Thomas, B.E.; Subbaraman, R.; Sellappan, S.; Suresh, C.; Lavanya, J.; Lincy, S.; Raja, A.L.; Javeed, B.; Kokila, S.; Arumugam, S.; et al. Pretreatment Loss to Follow-up of Tuberculosis Patients in Chennai, India: A Cohort Study with Implications for Health Systems Strengthening. BMC Infect. Dis. 2018, 18, 142. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.M.; Naureen, F.; Noor, A.; Fatima, I.; Viney, K.; Ishaq, M.; Anjum, N.; Rashid, A.; Haider, G.R.; Khan, M.A.; et al. Loss-to-Follow-up and Delay to Treatment Initiation in Pakistan’s National Tuberculosis Control Programme. BMC Public Health 2018, 18, 335. [Google Scholar] [CrossRef] [PubMed]
- Kurd, S.A.; Wali, A.; Fatima, R.; Yaqoob, A.; Khan, D.; Lehri, S. Pre-Treatment Loss to Follow-up among Patients with Rifampicin-Resistant Tuberculosis in Baluchistan, Pakistan, 2012–2017: A Retrospective Cohort Study. F1000Research 2018, 7, 1905. [Google Scholar] [CrossRef] [Green Version]
- Evans, D.; Sineke, T.; Schnippel, K.; Berhanu, R.; Govathson, C.; Black, A.; Long, L.; Rosen, S. Impact of Xpert MTB/RIF and Decentralized Care on Linkage to Care and Drug-Resistant Tuberculosis Treatment Outcomes in Johannesburg, South Africa. BMC Health Serv. Res. 2018, 18, 973. [Google Scholar] [CrossRef] [Green Version]
- Gopi, P.; Chandrasekaran, V.; Subramani, R.; Narayanan, P. Failure to Initiate Treatment for Tuberculosis Patients Diagnosed in a Community Survey and at Health Facilities under a Dots Programme in a District of South India. Indian J. Tuberc. 2005, 52, 153–156. [Google Scholar]
- Bhanbhro, S.; Kamal, T.; Diyo, R.W.; Lipoeto, N.I.; Soltani, H. Factors Affecting Maternal Nutrition and Health: A Qualitative Study in a Matrilineal Community in Indonesia. PLoS ONE 2020, 15, e0234545. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Criteria | Laboratory Register (n) | Provincial Treatment Register | |
|---|---|---|---|
| SITT (n) | e-TB Manager (n) | ||
| Initial records | 9353 | 73,594 | 794 |
| Removed records | 3468 | 6494 | 95 |
| Non-residents of North and West Sumatra | 543 | 193 | 60 |
| Missing information on gender, age, name, or district address | 104 | 67 | 1 |
| Age less than 8 years | 22 | 3948 | - |
| Duplicated record | 1233 | 2286 | 34 |
| Previously treated or treatment delayed more than 182 days | 1566 | - | - |
| Eligible for linkage analysis | 5885 | 67,100 | 699 |
| DS-TB | 5353 | 67,100 | - |
| DR-TB | 532 | - | 699 |
| Jaro–Winkler Score | Matched (n = 128) | Unmatched (n = 128) |
|---|---|---|
| 0.000–0.050 | 126 | 0 |
| 0.051–0.134 | 2 | 1 |
| 0.135–0.200 | 0 | 2 |
| 0.201–0.250 | 0 | 4 |
| 0.251–0.300 | 0 | 3 |
| 0.301–0.400 | 0 | 17 |
| 0.401–0.500 | 0 | 72 |
| 0.501–0.750 | 0 | 22 |
| 0.751–1.000 | 0 | 7 |
| Diagnosed Facility Level | Total n | Treatment (Notified) Facility Levels | Missing Patients | |||
|---|---|---|---|---|---|---|
| L1 Puskesmas | L2 Hospital | L3 Hospital | Private | |||
| n (%) | n (%) | n (%) | n (%) | n (%) | ||
| DS-TB patients | ||||||
| All cases | 5353 | 3233 (60.4) | 424 (7.9) | 91 (1.7) | 181 (3.4) | 1424 (26.6) |
| L1 Puskesmas | 1052 | 960 (91.2) | 9 (0.9) | 0 (0.0) | 7 (0.7) | 76 (7.2) |
| L2 Hospital | 3292 | 1921 (58.4) | 360 (10.9) | 6 (0.2) | 65 (2.0) | 940 (28.6) |
| L3 Hospital | 1009 | 352 (34.9) | 55 (5.5) | 85 (8.4) | 109 (10.8) | 408 (40.4) |
| DR-TB patients | ||||||
| All cases | 532 | 0 (0.0) | 65 (12.2) | 334 (62.8) | 0 (0.0) | 133 (25.0) |
| L2 Hospital | 132 | 0 (0.0) | 65 (49.2) | 5 (3.8) | 0 (0.0) | 62 (47.0) |
| L3 Hospital | 400 | 0 (0.0) | 0 (0.0) | 329 (82.2) | 0 (0.0) | 71 (17.8) |
| Characteristics | Missing of DS-TB Patients n/Total (%) | Missing of DR-TB Patients n/Total (%) | MH Chi-Square p Value | Heterogeneity Test p Value | AOR (95% CI) from LR | |
|---|---|---|---|---|---|---|
| Gender | ||||||
| Female | 511/1722 (29.7%) | 47/167 (28.1%) | 0.434 | 0.959 | 1.3 (1.2, 1.5) | |
| Male | 913/3631 (25.1%) | 86/365 (23.6%) | 1 | |||
| Age (years) | ||||||
| 8–44 | 704/2709 (26.0%) | 59/264 (22.3%) | 0.665 | 0.364 | 1 | |
| 45–64 | 502/2032 (24.7%) | 64/243 (26.3%) | 0.9 (0.8, 1.1) | |||
| 65–100 | 218/612 (35.6%) | 10/25 (40.0%) | 1.6 (1.3, 1.9) | |||
| Patient residence | ||||||
| Rural | 980/3586 (27.3%) | 64/264 (24.2%) | 0.523 | 358 | 1 | |
| Urban | 444/1767 (25.1%) | 69/268 (25.7%) | 1.0 (0.9, 1.1) | |||
| Year of diagnosis | ||||||
| 2017 | 497/2219 (22.4%) | 38/219 (17.4%) | 0.416 | 0.116 | 1 | |
| 2018 | 927/3134 (29.6%) | 95/313 (30.4%) | 1.4 (1.2, 1.6) | |||
| Facility level | ||||||
| L1 Puskesmas | 76/1052 (7.2%) | - | 1 | |||
| L2 Hospital | 940/3292 (28.6%) | 62/132 (47%) | not computable | 4.9 (3.8, 6.4) | ||
| L3 Hospital | 408/1009 (40.4%) | 71/400 (17.8%) | 7.6 (5.9, 10.0) | |||
| Province facility level | DS-TB | DR-TB | ||||
| West Sumatra | 801/2977 (26.9%) | 24/58 (41.4%) | 0.628 | 0.005 * | 1 | 1 |
| North Sumatra | 623/2376 (26.2%) | 109/474 (23%) | 1.0 (0.9, 1.2) | 0.4 (0.2, 0.7) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Widoyo, R.; Djafri, D.; Putri, A.S.E.; Yani, F.F.; Kusumawati, R.L.; Wongsirichot, T.; Chongsuvivatwong, V. Missing Cases of Bacteriologically Confirmed TB/DR-TB from the National Treatment Registers in West and North Sumatra Provinces, Indonesia. Trop. Med. Infect. Dis. 2023, 8, 31. https://doi.org/10.3390/tropicalmed8010031
Widoyo R, Djafri D, Putri ASE, Yani FF, Kusumawati RL, Wongsirichot T, Chongsuvivatwong V. Missing Cases of Bacteriologically Confirmed TB/DR-TB from the National Treatment Registers in West and North Sumatra Provinces, Indonesia. Tropical Medicine and Infectious Disease. 2023; 8(1):31. https://doi.org/10.3390/tropicalmed8010031
Chicago/Turabian StyleWidoyo, Ratno, Defriman Djafri, Ade Suzana Eka Putri, Finny Fitry Yani, R Lia Kusumawati, Thakerng Wongsirichot, and Virasakdi Chongsuvivatwong. 2023. "Missing Cases of Bacteriologically Confirmed TB/DR-TB from the National Treatment Registers in West and North Sumatra Provinces, Indonesia" Tropical Medicine and Infectious Disease 8, no. 1: 31. https://doi.org/10.3390/tropicalmed8010031