
Genotypes of Hepatitis C Virus and Efficacy of Direct-Acting Antiviral Drugs among Chronic Hepatitis C Patients in a Tertiary Care Hospital

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
- A patient who met the following criteria was eligible for the study:
- Positive HCV-RNA;
- Age ≥ 18 years.
- Exclusion criteria: the following patients were excluded from the study:
- Pregnant or breastfeeding women;
- Decompensated cirrhosis (Child–Pugh C patients);
- Patient with hepatocellular carcinoma;
- Patient with systemic malignancy except after 2 years of disease-free interval;
- Patients with concurrent hepatitis B virus and/or HIV infection;
- Platelet count less than 500,000/mm3;
- Patients with significant illnesses such as congestive heart failure, renal failure, respiratory failure, or autoimmune diseases.
2.1. Screening for HCV Infection
2.2. Confirmation of HCV Infection and Quantification of HCV RNA
2.3. Determination of HCV Genotype
2.4. The Treatment Decision
- Sofosbuvir/Daclatasvir ± Ribavirin (SOF/DCV 400/60 mg once daily oral dose ± RBV) as a pangenomic regimen for 12 weeks for non-cirrhotic and compensated cirrhotic patients;
- Sofosbuvir/Ledipasvir ± Ribavirin (SOF/LDV 400/90 mg once daily dose ± RBV) for GT1 for 8 or 12 weeks according to the baseline HCV RNA and the cirrhosis state;
- Ombitasvir/Paritaprevir/Ritonavir/Dasabuvir ± Ribavirin (OBV/PTV/Rtv (25/150/100 mg once daily orally) plus DSV (250 mg twice daily orally) ± RBV) for 12 weeks for non-cirrhotic GT 1a patients;
- Elbasvir/Grazoprevir (EBR/GZR) 50/100 mg single oral daily dose for 12 weeks as a non-pangenomic regimen for patients with GT1b;
- Glecaprevir/Pibrentasvir/Ribavirin (GLE/PIB 300/120 mg single daily oral dose ± RBV) as a pangenotypic regimen for 8 weeks.
2.5. Assessment of Treatment Efficacy
2.6. Sample Size Calculation
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Studied Population
3.2. Prescribed Treatment Regimens
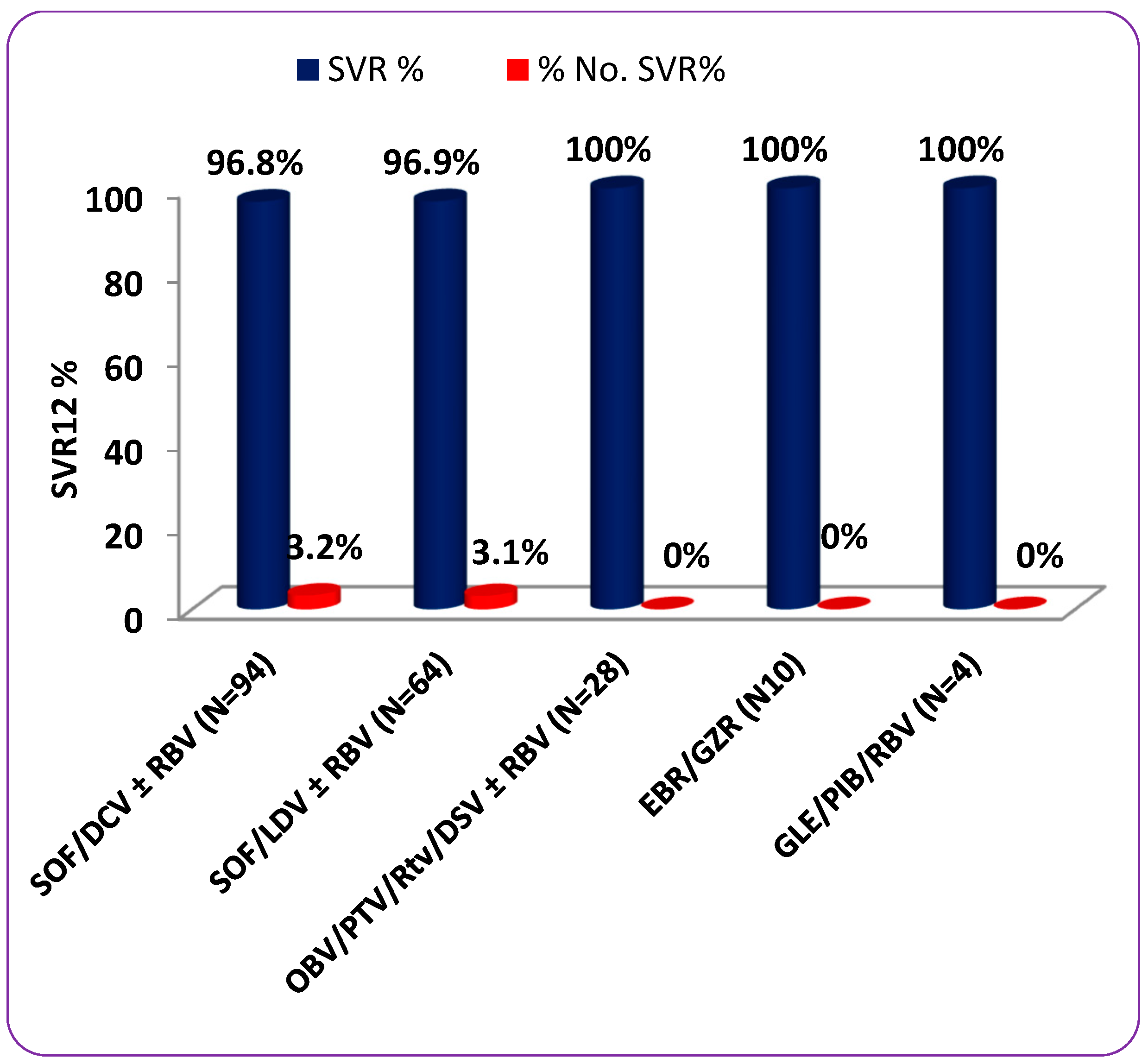
3.3. Treatment Efficacy
3.4. Predictors of SVR12
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Mohamoud, Y.A.; Riome, S.; Abu-Raddad, L.J. Epidemiology of hepatitis C virus in the Arabian Gulf countries: Systematic review and meta-analysis of prevalence. Int. J. Infect. Dis. 2016, 46, 116–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jadoul, M.; Berenguer, M.C.; Doss, W.; Fabrizi, F.; Izopet, J.; Jha, V.; Kamar, N.; Kasiske, B.L.; Lai, C.-L.; Morales, J.M.; et al. Executive summary of the 2018 KDIGO Hepatitis C in CKD Guideline: Welcoming advances in evaluation and management. Kidney Int. 2018, 94, 663–673. [Google Scholar] [CrossRef] [Green Version]
- Pol, S.; Parlati, L.; Jadoul, M. Hepatitis C virus and the kidney. Nat. Rev. Nephrol. 2018, 15, 73–86. [Google Scholar] [CrossRef]
- Jefferies, M.; Rauff, B.; Rashid, H.; Lam, T.; Rafiq, S. Update on global epidemiology of viral hepatitis and preventive strategies. World J. Clin. Cases 2018, 6, 589–599. [Google Scholar] [CrossRef]
- WHO. Global Hepatitis Report 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c (accessed on 10 September 2021).
- Al-Raddadi, R.M.; Dashash, N.A.; Alghamdi, H.A.; Alzahrani, H.S.; Alsahafi, A.J.; Algarni, A.M.; Alraddadi, Z.M.; Alghamdi, M.M.; Hakim, R.F.; Al-Zalabani, A.H. Prevalence and predictors of hepatitis B in Jeddah City, Saudi Arabia: A population-based seroprevalence study. J. Infect. Dev. Ctries. 2016, 10, 1116–1123. [Google Scholar] [CrossRef] [Green Version]
- Sanai, F.M.; Aljumah, A.A.; Babatin, M.; Hashim, A.; Abaalkhail, F.; Bassil, N.; Safwat, M. Hepatitis B care pathway in Saudi Arabia: Current situation, gaps and actions. Saudi J. Gastroenterol. 2019, 25, 73–80. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021. Towards Ending Viral Hepatitis. Available online: http://www.who.int/hepatitis/strategy2016-2021/ghss-hep/en/ (accessed on 10 September 2021).
- Kato, N. Genome of human hepatitis C virus (HCV): Gene organization, sequence diversity, and variation. Microb. Comp. Genom. 2000, 5, 129–151. [Google Scholar] [CrossRef] [PubMed]
- Op De Beeck, A.; Dubuisson, J. Topology of hepatitis C virus envelope glycopro-teins. Rev. Med. Virol. 2003, 13, 233–241. [Google Scholar] [CrossRef]
- Simmonds, P.; Bukh, J.; Combet, C.; Deléage, G.; Enomoto, N.; Feinstone, S.; Halfon, P.; Inchauspé, G.; Kuiken, C.; Maertens, G.; et al. Consensus proposals fora unified system of nomenclature of hepatitis C virusgenotypes. Hepatology 2005, 42, 962–973. [Google Scholar] [CrossRef] [PubMed]
- Tsukiyama-Kohara, K.; Kohara, M. Hepatitis C virus: Viralquasispecies and genotypes. Int. J. Mol. Sci. 2017, 19, 23. [Google Scholar] [CrossRef]
- Li, G.; De Clercq, E. Current therapy for chronic hepatitis C: The role of direct-acting antivirals. Antivir. Res. 2017, 142, 83–122. [Google Scholar] [CrossRef] [PubMed]
- Abdelhameed, R.F.A.; Ibrahim, A.K.; Elfaky, M.A.; Habib, E.S.; Mahamed, M.I.; Mehanna, E.T.; Darwish, K.M.; Khodeer, D.M.; Ahmed, S.A.; Elhady, S.S. Antioxidant and Anti-Inflammatory Activity of Cynanchum Acutum L. Isolated Flavonoids Using Experimentally Induced Type 2 Diabetes Mellitus: Biological and In Silico Investigation for NF-ΚB Pathway/MiR-146a Expression Modulation. Antioxidants 2021, 10, 1713. [Google Scholar] [CrossRef]
- Petruzziello, A.; Marigliano, S.; Loquercio, G.; Cozzolino, A.; Cacciapuoti, C. Globalepidemiology of hepatitis C virus infection: An up-date of thedistribution and circulation of hepatitis C virus genotypes. World J. Gastroenterol. 2016, 22, 7824–7840. [Google Scholar] [CrossRef] [PubMed]
- Blach, S.; Zeuzem, S.; Manns, M.; Altraif, I.; Duberg, A.S.; Muljono, D.H.; Waked, I.; Alavian, S.M.; Lee, M.H.; Negro, F.; et al. Global prevalence andgenotype distribution of hepatitis C virus infection in 2015, amodelling study. Lancet Gastroenterol. Hepatol. 2017, 2, 161–176. [Google Scholar] [CrossRef] [Green Version]
- Bawazir, A.; AlGusheri, F.; Jradi, H.; AlBalwi, M.; Abdel-Gader, A.-G. Hepatitis C virus genotypes in Saudi Arabia: A future prediction and laboratory profile. Virol. J. 2017, 14, 208. [Google Scholar] [CrossRef] [Green Version]
- Yu, M.-L.; Tsai, W.-L.; Chi-Jen Chu, C.-J.; Kao, J.-H. Characteristics of patients with hepatitis C virus infection and antiviral treatment initiation in Taiwan: The MOSAIC study. Kaohsiung J. Med. Sci. 2020, 37, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Gower, E.; Estes, C.; Blach, S.; Razavi-Shearer, K.; Razavi, H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J. Hepatol. 2014, 61, S45–S57. [Google Scholar] [CrossRef] [Green Version]
- Messina, J.P.; Humphreys, I.; Flaxman, A.; Brown, A.; Cooke, G.S.; Pybus, O.G.; Barnes, E. Global distribution and prevalence of hepatitis C virus genotypes. Hepatology 2015, 61, 77–87. [Google Scholar] [CrossRef] [Green Version]
- de Castroa, G.L.C.; Amoras, E.G.S.; de Araújo, M.S.M.; da Silva Conde, S.R.S.; Vallinoto, A.C.R. Hepatitis C virus genotypes and associated risk factors in the state of Pará, Northern Brazil. Braz. J. Infect. Dis. 2020, 24, 304–309. [Google Scholar] [CrossRef]
- Ellabban, M.A.; Fattah, I.O.A.; Kader, G.A.; Eldeen, O.S.; Mehana, A.E.; Khodeer, D.M.; Hosny, H.; Elbasiouny, M.S.; Masadeh, S. The Effects of Sildenafil and/or Nitroglycerin on Random-Pattern Skin Flaps After Nicotine Application in Rats. Sci. Rep. 2020, 10, 3212. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL 2017 clinical practice guidelines on the management of hepatitis C virus infection. J. Hepatol. 2017, 66, 153–194. [Google Scholar]
- Shaheen, M.A.; Idrees, M. Evidence-based consensus on the diagnosis, prevention and management of hepatitis C virus disease. World J. Hepatol. 2015, 7, 616–627. [Google Scholar] [CrossRef] [PubMed]
- Manns, M.P.; McHutchison, J.G.; Gordon, S.C.; Rustgi, V.K.; Shiffman, M.; Reindollar, R.; Goodman, Z.D.; Koury, K.; Ling, M.-H.; Albrecht, J.K. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: A randomised trial. Lancet 2001, 358, 958–965. [Google Scholar] [CrossRef] [PubMed]
- Bertino, G.; Ardiri, A.; Proiti, M.; Rigano, G.; Frazzetto, E.; Demma, S.; Ruggeri, M.I.; Scuderi, L.; Malaguarnera, G.; Bertino, N.; et al. Chronic hepatitis C: This and the new era of treatment. World J. Hepatol. 2016, 8, 92–106. [Google Scholar] [CrossRef]
- Hong, C.M.; Liu, C.H.; Su, T.H.; Yang, H.C.; Chen, P.J.; Chen, Y.W.; Kao, J.H.; Liu, C.J. Real-world effectiveness of direct-acting antiviral agents for chronic hepatitis C in Taiwan: Real-world data. J. Microbiol. Immunol. Infect. 2020, 53, 569–577. [Google Scholar] [CrossRef]
- Zeng, H.; Li, L.; Hou, Z.; Zhang, Y.; Tang, Z.; Liu, S. Direct-acting Antiviral in the Treatment of Chronic Hepatitis C: Bonuses and Challenges. Int. J. Med. Sci. 2020, 17, 892–902. [Google Scholar] [CrossRef] [Green Version]
- Abdulla, M.; Ali, H.; Nass, H.; Khamis, J.; Al Qamish, J. Efficacy of direct-acting antiviral therapy for hepatitis C viral infection. Real-life experience in Bahrain. Hepat. Med. 2019, 11, 69–78. [Google Scholar] [CrossRef] [Green Version]
- Cárdaba-García, M.E.; Abad-Lecha, E.; Calleja-Hernández, M.Á. Effectiveness of direct-acting antiviral drugs against hepatitis C virus: Predictive factors of response to the treatment. Libyan J. Med. 2021, 16, 1949797. [Google Scholar] [CrossRef]
- Chung, R.T.; Davis, G.L.; Jensen, D.M.; Masur, H.; Saag, M.S.; Thomas, D.L.; Aronsohn, A.I.; Charlton, M.R.; Feld, J.J.; Fontana, R.J.; et al. Hepatitis C guidance: AASLDIDSA recommendations for testing, managing, and treating adults infected with hepatitis C virus. Hepatology 2015, 62, 932–954. [Google Scholar] [CrossRef] [Green Version]
- Alghamdi, A.S.; Alghamdi, M.; Sanai, F.M.; Alghamdi, H.; Aba-Alkhail, F.; Alswat, K.; Babatin, M.; Alqutub, A.; Altraif, I.; Alfaleh, F. SASLT guidelines: Update in treatment of Hepatitis C virus infection. Saudi J. Gastroenterol. 2016, 22, S25–S27. [Google Scholar] [CrossRef]
- Axley, P.; Ahmed, Z.; Ravi, S.; Singal, A.K. Hepatitis C virus and hepatocellular carcinoma: A narrative review. J. Clin. Transl. Hepatol. 2018, 6, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Bhamidimarri, K.R.; Satapathy, S.K.; Martin, P. Hepatitis C virus and liver transplantation. Gastroenterol. Hepatol. 2017, 13, 214–220. [Google Scholar]
- Aljumah, A.; Abaalkhail, F.; Al-Ashgar, H.; Assiri, A.; Babatin, M.; Al-Faleh, F.; Alghamdi, A.; Al-Hakeem, R.; Hashim, A.; Alqutub, A.; et al. Epidemiology, disease burden, and treatment strategies of chronic hepatitis C virus infections in Saudi Arabia in the new treatment paradigm shift. Saudi J. Gastroenterol. 2016, 22, 269. [Google Scholar] [CrossRef]
- Ahmed, O.A.; Kaisar, H.H.; Hawash, N.; Samir, H.; Shabana, S.; Fouad, H.A.; Rizk, F.; Abd-Elsalam, S. Efficacy of sofosbuvir plus ribavirin with or without peginterferon- alfa interferon in treatment of a cohort of Egyptian patients with hepatitis C virus infection. Infect. Disord. Drug Targets 2017, 17, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Juanbeltz, R.; Castilla, J.; Martínez-Baz, I.; O’Leary, A.; Sarobe, M.; San Miguel, R. Health-related quality of life in hepatitis C patients who achieve sustained virological response to direct-acting antivirals: A comparison with the general population. Qual. Life Res. 2019, 28, 1477–1484. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Moneim, A.; Bamaga, M.; Shehab, G.; Abu Elsaad, A.; Farahat, F. HCV Infection among Saudi Population: High Prevalence of Genotype 4 and Increased Viral Clearance Rate. PLoS ONE 2012, 7, e29781. [Google Scholar] [CrossRef] [Green Version]
- Alarfaj, S.J.; Alzahrani, A.; Alotaibi, A.; Almutairi, M.; Hakami, M.; Alhomaid, N.; Alharthi, N.; Ghazwa, B.K.; Alghamdi, A. The effectiveness and safety of direct-acting antivirals for hepatitis C virus treatment: A single-center experience in Saudi Arabia. Saudi Pharm. J. 2022, 30, 1448–1453. [Google Scholar] [CrossRef]
- Ghaderi-Zefrehi, H.; Gholami-Fesharaki, M.; Sharafi, H.; Sadeghi, F.; Alavian, S. The Distribution of Hepatitis C Virus Genotypes in Middle Eastern Countries: A Systematic Review and Meta-Analysis. Hepat. Mon. 2016, 16, e40357. [Google Scholar] [CrossRef] [Green Version]
- Hashim, A.E.M.; Zaky, S.; Alghannam, M.Z.; Ibraheem, S.A.; El-Raey, F.M.; Abdelaziz, A. Efficacy and safety of daclatasvir-containing regimens in the treatment of chronic hepatitis C patients in Damietta. Al-Azhar Assiut Med. J. 2020, 18, 159. [Google Scholar]
- Ahmed, O.A.; Kaisar, H.H.; Badawi, R.; Hawash, N.; Samir, H.; Shabana, S.S.T.; Fouad, M.H.A.; Rizk, F.H.; Khodeir, S.A.; Abd-Elsalam, S. Efficacy and safety of sofosbuvir-ledipasvir for treatment of a cohort of Egyptian patients with chronic hepatitis C genotype 4 infection. Drug Resist. Infect. 2018, 11, 295–298. [Google Scholar] [CrossRef] [Green Version]
- El Kassas, M.; Alboraie, M.; Omar, H.; El Latif, Y.A.; Algaber, M.A.; El Tahan, A.; El Halwagy, H.; Afify, S.; Elserafy, M.; Elsaeed, K.; et al. High success rates for the use of ombitasvir/paritaprevir/ritonavir containing regimens in treatment of naïve and experienced chronic hepatitis C genotype 4: Real world results. J. Med. Virol. 2022, 94, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Wu, F.-P.; Wang, W.-J.; Shi, J.-J.; Li, Y.-P.; Zhang, X.; Dang, S.S. Real-life efficacy and safety of direct-acting antiviral therapy for treatment of patients infected with hepatitis C virus genotypes 1, 2 and 3 in northwest China. World J. Gastroenterol. 2019, 25, 6551. [Google Scholar] [CrossRef] [PubMed]
- Kamel, S.; Elessawy, H.; Ashraf, O.; Elbaz, A.; Dabbous, H.; El-Sayed, M.; Ali, S.; Kamel, H. Effectiveness of Direct-Acting Antivirals in Treatment of Elderly Egyptian Chronic Hepatitis C Patients. Gastroenterol. Insights 2021, 12, 336–346. [Google Scholar] [CrossRef]
- Iliescu, E.L.; Mercan-Stanciu, A.; Toma, L. Safety and efficacy of direct-acting antivirals for chronic hepatitis C in patients with chronic kidney disease. BMC Nephrol. 2020, 21, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tatar, B.; Kose, S.; Ergun, N.; Turken, M.; Onlen, Y.; Yilmaz, Y.; Akhan, S. Response to direct-acting antiviral agents in chronic hepatitis C patients with end-stage renal disease: A clinical experience. Rev. Assoc. Med. Bras. 2019, 65, 1470–1475. [Google Scholar] [CrossRef] [PubMed]
- Marciano, S.; Haddad, L.; Reggiardo, M.V.; Peralta, M.; Vistarini, C.; Marino, M.; Descalzi, V.I.; D’Amico, C.; Escuti, S.F.; Gaite, L.A.; et al. Effectiveness and safety of original and generic sofosbuvir for the treatment of chronic hepatitis C: A real-world study. J. Med. Virol. 2018, 90, 951–958. [Google Scholar] [CrossRef]
- Abd-Elsalam, S.; Sharaf-Eldin, M.; Soliman, S.; Elfert, A.; Badawi, R.; Ahmad, Y.K. Efficacy and safety of sofosbuvir plus ribavirin for treatment of cirrhotic patients with genotype 4 hepatitis C virus in real-life clinical practice. Arch. Virol. 2018, 163, 51–56. [Google Scholar] [CrossRef]
- Buti, M.; Riveiro-Barciela, M.; Esteban, R. Management of direct-acting antiviral agent failures. J. Hepatol. 2015, 63, 1511–1522. [Google Scholar] [CrossRef]
- Abdelsameea, E.; Alsebaey, A.; Abdel-Razek, W.; Ehsan, N.; Morad, W.; Salama, M.; Waked, I. Elastography and serum markers of fbrosis versus liver biopsy in 1270 Egyptian patients with hepatitis C. Eur. J. Gastroenterol. Hepatol. 2020, 32, 1553–1558. [Google Scholar] [CrossRef]
- Prosół, M.; Bladowskab, J.; Ejmaa, M.; Stepniewskac, K.; Rymer, W.; Sąsiadek, M.; Pawłowski, T.; Małyszczak, K.; Inglot, M.; Żelwetro, A.; et al. Visual and brainstem auditory evoked potentials in HCV-infected patients before and after interferon-free therapy—A pilot study. Int. J. Infect. Dis. 2019, 80, 122–128. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Study Patients (n = 200) |
|---|---|
| Age (years) | |
| Mean ± SD | 53.17 ± 15.71 |
| Gender | |
| Male | 119 (59.5) |
| Female | 81 (40.5) |
| Treatment history | |
| Naïve | 119 (60.0) |
| Experienced | 81 (41.54) |
| INF/RBV (48 weeks) | 26 (13) |
| INF/RBV (24 weeks) | 35 (17.5) |
| SOF/SIM (12 weeks) | 11 (5.5) |
| SOF/DAC (12 weeks) | 9 (4.5) |
| Baseline viral load IU/mL | 2,340,000 ± 2,150,000 |
| Body mass index (mean ± SD) | 28.8 ± 6.2 |
| FibroScan (mean ± SD) | 8.7 ± 4.1 |
| Fibrosis n, (%) | |
| F0–F3 | 130 (70.0) |
| F4 (Cirrhosis) | 70 (35.0) |
| Child–Pugh n, (%) | |
| A | 26 (13) |
| B | 44 (22) |
| Associated comorbidities (n/%) | |
| CKD | 23 (11.5) |
| HTN | 57 (28.5) |
| DM | 78 (39.5) |
| IHD | 20 (10.0) |
| None | 65 (32.5) |
| Baseline lab | |
| Albumin (g/dL) mean ± SD (range) | 3.47 ± 0.48 (2.9–4.7) |
| ALT (U/L) mean ± SD (range) | 35.48 ± 17.51 (11–71) |
| Total bilirubin (mg/dL) mean ± SD (range) | 1.67 ± 2.62 (0.9–2.7) |
| Creatinine (mg/dL) mean ± SD (range) | 1.07 ± 0.20 (0.5–2.4) |
| HCV genotype | |
| 1(a and b) | 64 (32.0) |
| 2 | 3 (1.5) |
| 3 | 14 (7.0) |
| 4 | 109 (54.5) |
| Mixed (1a+4) | 10 (5.0) |
| Antiviral drug combinations | |
| SOF/DCV ± RBV | 94 (47.0) |
| SOF/LDV ± RBV | 64 (32.0) |
| OBV/PTV/Rtv/DSV ± RBV | 28 (14.0) |
| EBR/GZR | 10 (5.0) |
| GLE/PIB/RBV | 4 (2.0) |
| RBV included in therapy | 67 (33.5) |
| Study Patients (N) | GT4 (N = 109) | GT1a (N = 42) | GT1b (N = 22) | GT3 (N = 14) | GT2 (N = 3) | Mixed Genotypes (N = 10) | p-Value |
|---|---|---|---|---|---|---|---|
| Age (years) | |||||||
| Mean ± SD | 47.43 ± 11.8 | 48.52 ± 11.9 | 54.62 ± 19.6 | 54.82 ± 16.7 | 55.66 ± 5.8 | 55.20 ± 15.7 | 0.220 |
| Gender | |||||||
| Male | 55 (50.5) | 35 (83.3) | 13 (59.1) | 12 (85.7) | 0 (0.0%) | 4 (40.0) | 0.001 * |
| Female | 54 (49.5) | 7 (16.7) | 9 (40.9) | 2 (14.3) | 3 (100.0) | 6 (60.0) | |
| Treatment history | |||||||
| Naïve | 62 (56.9) | 27 (64.3) | 13 (59.1) | 9 (64.3) | 2 (75) | 6 (60.0) | 0.869 |
| Experienced | 47 (43.1) | 15 (35.7) | 9 (40.9) | 5 (35.7) | 1 (25.0) | 4 (40.0) | |
| Cirrhosis status | |||||||
| Cirrhotic | 39 (35.8) | 13 (41.9) | 13 (59.1) | 2 (14.3) | 1 (25.0) | 2 (20.0) | 0.075 |
| Non-cirrhotic | 70 (64.2) | 29 (69.0) | 9 (40.9) | 12 (85.7) | 2 (75.0) | 8 (80.0) | |
| Chronic kidney disease | |||||||
| Yes | 11 (10.1) | 9 (21.42) | 0 | 1 (7.14) | 0 | 2 (20) | 0.195 |
| No | 98 (89.91) | 33 (78.57) | 22 (100) | 13 (92.86) | 3 (100) | 8 (80) | |
| Antiviral drugs combination | |||||||
| SOF/DCV ± RBV | 47 (43.1) | 20 (47.6) | 9 (40.9) | 11 (78.6) | 3 (100.0) | 4 (40.0) | 0.780 |
| SOF/LDV ± RBV | 38 (34.9) | 12 (28.6) | 8 (36.4) | 2 (14.3) | 0 | 4 (40.0) | |
| OBV/PTV/Rtv/DSV ± RBV | 16 (14.7) | 6 (14.3) | 5 (22.7) | 0 | 0 | 1 (10.0) | |
| EBR/GZR | 7 (6.4) | 2 (4.8) | 0 | 0 | 0 | 1 (10.0) | |
| GLE/PIB/RBV | 1 (0.9) | 2 (4.8) | 0 | 1 (7.1) | 0 | 0 | |
| Ribavirin included in therapy | |||||||
| Yes | 35 (32.1) | 14 (33.3) | 12 (54.5) | 4 (28.6) | 1 (33.3) | 1 (10.0) | 0.131 |
| No | 74 (67.9) | 28 (66.7) | 10 (45.5) | 10 (71.4) | 2 (66.7) | 9 (10) | |
| Variable | SVR12 Group (n = 195) | Non-SVR12 Group (n = 5) | p-Value |
|---|---|---|---|
| Age (years) | |||
| Mean ± SD | 52.94 ± 15.79 | 62 ± 9.03 | 0.204 |
| Gender | |||
| Male | 118 (60.5) | 1 (20.0%) | 0.068 |
| Female | 77 (39.5) | 4 (80.0%) | |
| Treatment history | |||
| Naïve | 114 (58.46) | 5 (100.0%) | 0.230 |
| Experienced | 81 (41.54) | 0 (0.0%) | |
| Liver cirrhosis | |||
| Cirrhotic | 66 (33.8%) | 4(80.0%) | 0.032 ** |
| Non-cirrhotic | 129 (66.2%) | 1 (20.0%) | |
| Child–Pugh n, (%) | |||
| A | 25 (12.8%) | 1 (20.0%) | 0.002 ** |
| B | 40 (20.5%) | 4 (80.0%) | |
| CKD | |||
| Yes | 23 (11.79%) | 0 | 0.716 |
| No | 172 (88.21%) | 5 (100%) | |
| HCV genotype | |||
| 1a (a and b) | 63 (32.3%) | 0 | 0.001 ** |
| 2 | 3 (1.54%) | 0 | |
| 3 | 14 (7.18%) | 0 | |
| 4 | 105 (53.85%) | 4 (80.0%) | |
| Mixed (1a+4) | 10 (5.13%) | 0 | |
| Antiviral drug combinations | |||
| SOF/DCV ± RBV | 91 (46.67%) | 3 (60.0%) | 0.348 |
| SOF/LDV ± RBV | 62 (31.79%) | 2 (40.0%) | |
| OBV/PTV/Rtv/DSV ± RBV | 28 (14.36) | 0 | |
| EBR/GZR | 10 (5.13%) | 0 | |
| GLE/PIB/RBV | 4 (2.05%) | 0 | |
| RBV included in therapy | |||
| Yes | 65 (33.33) | 2 (40.0) | 0.755 |
| No | 130 (66.6) | 3 (60.0) | |
| Variable | Overall Patients (N = 200) | SOF/DCV ± RBV (N = 94) | SOF/LDV ± RBV (N = 64) | OBV/PTV/Rtv/DSV ± RBV (N = 28) | EBR/GZR (N = 10) | GLE/PIB/RBV (N = 4) |
|---|---|---|---|---|---|---|
| Overall patients | 195/200 (97.5%) | 91/94 (96.8%) | 62/64 (96.9%) | 28/28 (100%) | 10/10 (100%) | 4/4 (100%) |
| Age (years) | p = 0.632 | p = 0.898 | p = 0.878 | |||
| <40 | 43/43 (100%) | 24/24 (100%) | 13/13 (100%) | 5/5 (100%) | 1/1 (100%) | - |
| 40–60 | 92/96 (95.8%) | 45/48 (93.8%) | 24/25 (96%) | 16/16 (100%) | 4/4 (100%) | 3/3 (100%) |
| >60 | 60/61 (98.4%) | 22/22 (100%) | 25/26 (96.2%) | 7/7 (100%) | 5/5 (100%) | 1/1 (100%) |
| Gender | p = 0.160 | p = 0.553 | p = 0.613 | |||
| Male | 118/119 (99.2%) | 58/59 (98.3%) | 32/32 (100%) | 18/18 (100%) | 8/8 (100%) | 2/2 (100%) |
| Female | 77/81 (95.1%) | 33/35 (94.3%) | 30/32 (93.8%) | 10/10 (100%) | 2/2 (100%) | 2/2 (100%) |
| Treatment history | p = 0.018 ** | p = 0.116 | p = 0.075 | |||
| Naïve | 114/119 (95.8%) | 53/56 (94.6%) | 38/40 (95%) | 12/12 (100%) | 8/8 (100%) | 3/3 (100%) |
| Experienced | 81/81 (100%) | 38/38 (100%) | 24/24 (100%) | 16/16 (100%) | 2/2 (100%) | 1/1 (100%) |
| Liver cirrhosis | p = 0.121 | p = 0.252 | p = 0.283 | |||
| Yes | 66/70 (94.3%) | 29/31 (93.5%) | 21/23 (91.3%) | 11/11 (100%) | 4/4 (100%) | 1/1 (100%) |
| No | 129/130 (99.2%) | 62/63 (98.4%) | 41/41 (100%) | 17/17 (100%) | 6/6 (100%) | 3/3 (100%) |
| Genotype | p = 0.847 | p = 0.660 | p = 0.448 | |||
| 1 (a and b) | 63/64 (98.4%) | 28/29 (96.6%) | 20/20 (100%) | 11/11 (100%) | 2/2 (100%) | 2/2 (100%) |
| 2 | 3/3 (100%) | 3/3 (100%) | - | - | - | - |
| 3 | 14/14 (100%) | 11/11 (100%) | 2/2 (100%) | - | - | 1/1 (100%) |
| 4 | 105/109 (96.3%) | 45/47 (95.7%) | 36/38 (94.7%) | 16/16 (100%) | 7/7 (100%) | 1/1 (100%) |
| Mixed (1a+4) | 10/10 (100%) | 4/4 (100%) | 4/4 (100%) | 1/1 (100%) | 1/1 (100%) | - |
| Predictor | Unadjusted | Adjusted | ||
|---|---|---|---|---|
| Univariate OR (95% CI) | p-Value | Multivariate OR (95% CI) | p-Value | |
| Age (continuous, years) | 0.962 (0.906–1.021) | 0.205 | ||
| Gender | ||||
| Female | Reference | Reference | ||
| Male | 6.13 (0.672–55.88) | 0.108 | 12.34 (1.056–144.36) | 0.045 ** |
| Treatment history | ||||
| Naïve | Reference | Reference | ||
| Experienced | - | 0.97 | Overestimate | |
| Cirrhosis status | ||||
| No | Reference | Reference | ||
| Yes | 0.128 (0.014–1.167) | 0.068 | 0.071 (0.006–0.843) | 0.036 ** |
| Antiviral drugs | ||||
| SOF/DCV ± RBV | Reference | Reference | ||
| SOF/LDV ± RBV | 0.44 (0.02–8.07) | 0.520 | Overestimate | - |
| OBV/PTV/Rtv/DSV ± RBV | 6.23 (0.358–107.31) | 0.240 | Overestimate | - |
| EBR/GZR | 9.10 (0.58–156.95) | 0.129 | Overestimate | - |
| GLE/PIB/RBV | 2.30 (0.160–49.11) | 0.521 | Overestimate | - |
| CKD | ||||
| No | Reference | Reference | ||
| Yes | Overestimate | - | Overestimate | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hawsawi, N.M.; Saber, T.; Salama, H.M.; Fouad, W.S.; Hagag, H.M.; Alhuthali, H.M.; Eed, E.M.; Saber, T.; Ismail, K.A.; Al Qurashi, H.H.; et al. Genotypes of Hepatitis C Virus and Efficacy of Direct-Acting Antiviral Drugs among Chronic Hepatitis C Patients in a Tertiary Care Hospital. Trop. Med. Infect. Dis. 2023, 8, 92. https://doi.org/10.3390/tropicalmed8020092
Hawsawi NM, Saber T, Salama HM, Fouad WS, Hagag HM, Alhuthali HM, Eed EM, Saber T, Ismail KA, Al Qurashi HH, et al. Genotypes of Hepatitis C Virus and Efficacy of Direct-Acting Antiviral Drugs among Chronic Hepatitis C Patients in a Tertiary Care Hospital. Tropical Medicine and Infectious Disease. 2023; 8(2):92. https://doi.org/10.3390/tropicalmed8020092
Chicago/Turabian StyleHawsawi, Nahed Mohammed, Tamer Saber, Hussein M. Salama, Walaa S. Fouad, Howaida M. Hagag, Hayaa M. Alhuthali, Emad M. Eed, Taisir Saber, Khadiga A. Ismail, Hesham H. Al Qurashi, and et al. 2023. "Genotypes of Hepatitis C Virus and Efficacy of Direct-Acting Antiviral Drugs among Chronic Hepatitis C Patients in a Tertiary Care Hospital" Tropical Medicine and Infectious Disease 8, no. 2: 92. https://doi.org/10.3390/tropicalmed8020092