
Hepatitis C Virus Infection in Eastern Libya: Efforts Needed to Improve HCV Testing and Linkage to Care in the Resource-Limited Setting



{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Design
2.2. Study Setting and Population
2.3. Laboratory Assays
2.4. Statistical Analysis
3. Results
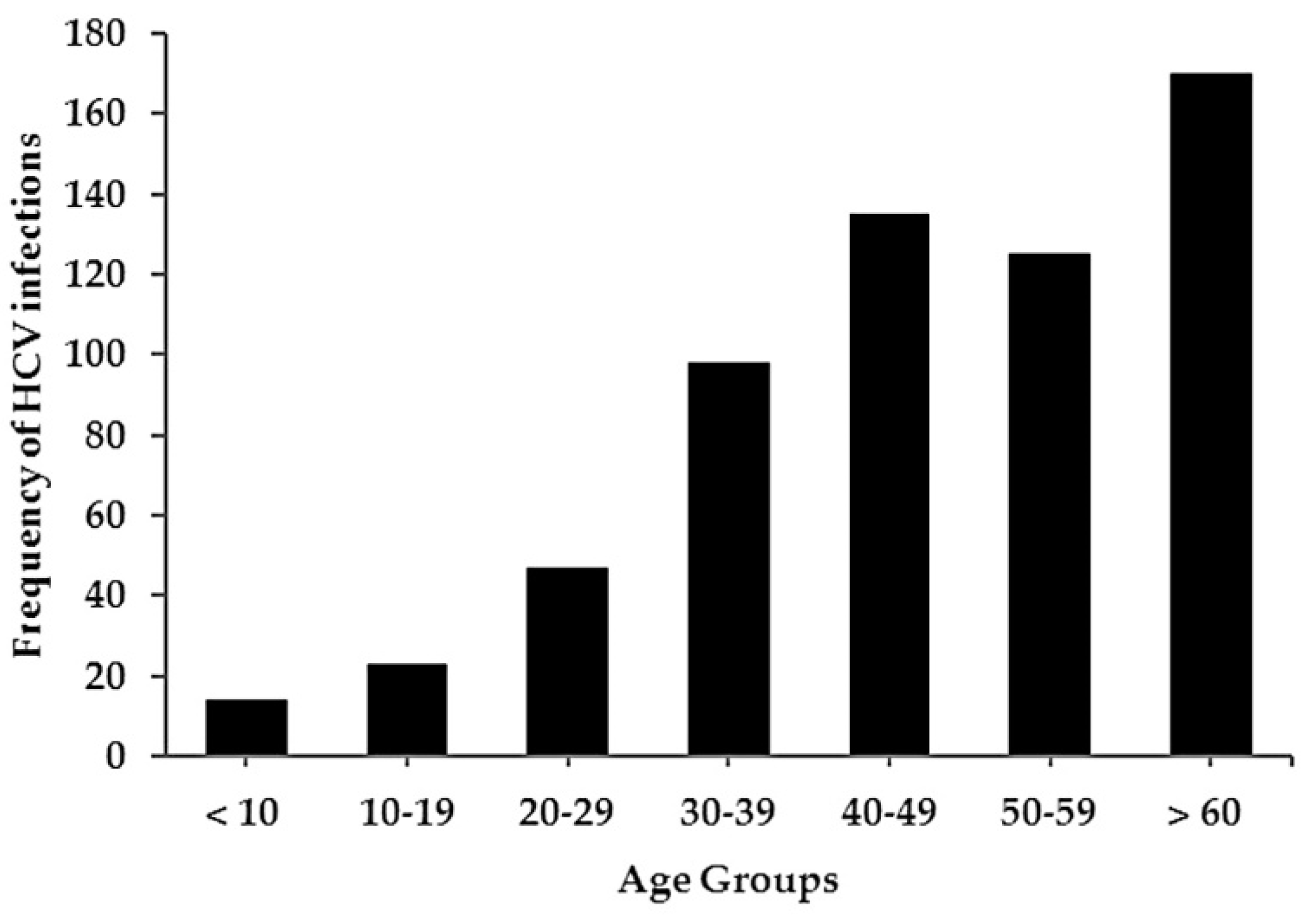
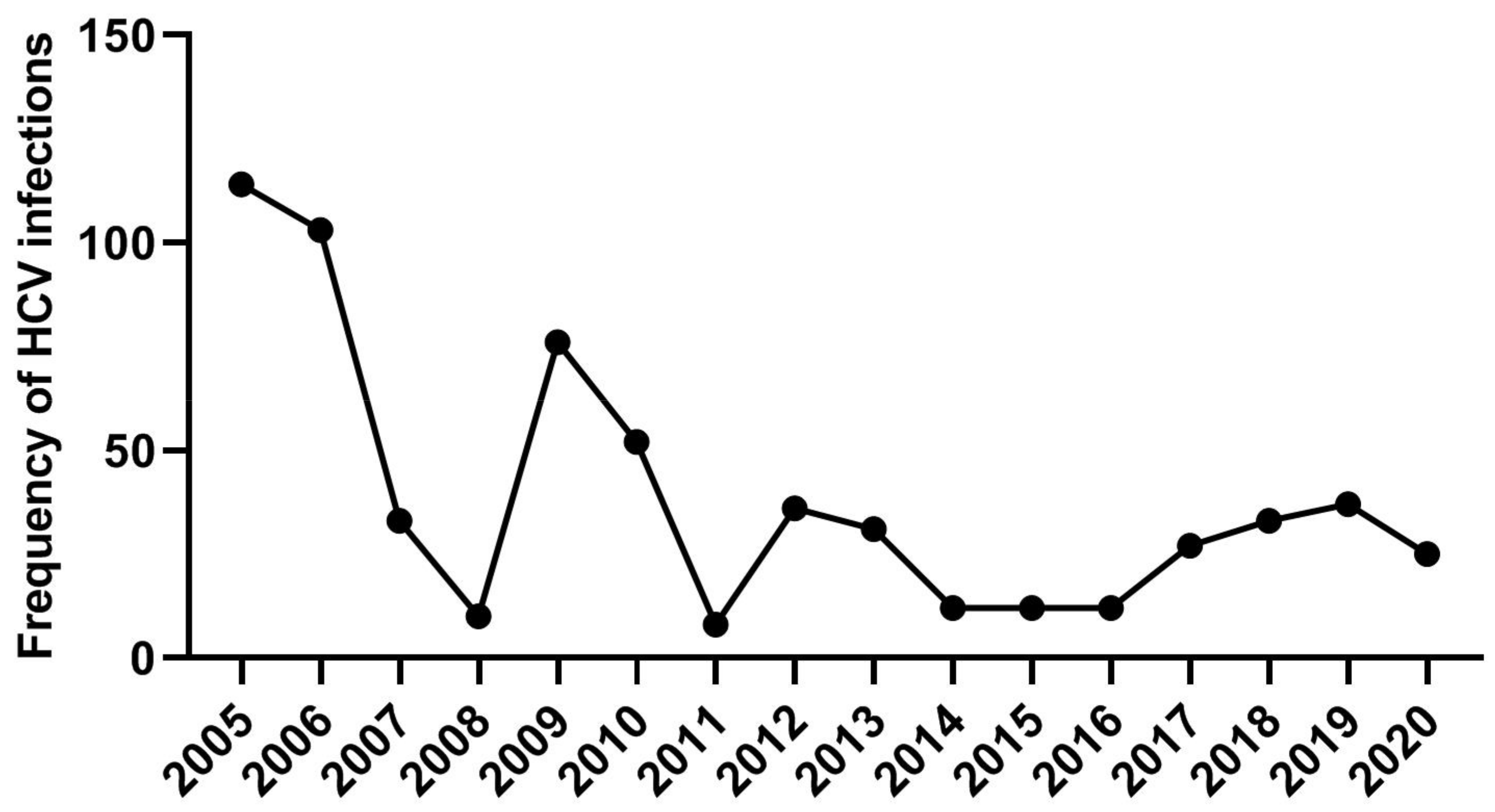
3.1. Incidence of Anti-HCV Antibodies in Tested Individuals
3.2. Follow Up Detection of HCV-RNA and Linkage to Care and Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petruzziello, A.; Marigliano, S.; Loquercio, G.; Cozzolino, A.; Cacciapuoti, C. Global epidemiology of hepatitis C virus infection: An up-date of the distribution and circulation of hepatitis C virus genotypes. World J. Gastroenterol. 2016, 22, 7824–7840. [Google Scholar] [CrossRef] [PubMed]
- Spada, E.; Mele, A.; Ciccozzi, M.; Tosti, M.E.; Bianco, E.; Szklo, A.; Ragni, P.; Gallo, G.; Balocchini, E.; Sangalli, M.; et al. Changing epidemiology of parenterally transmitted viral hepatitis: Results from the hepatitis surveillance system in Italy. Dig. Liver Dis. 2001, 33, 778–784. [Google Scholar] [CrossRef]
- Hashem, M.; Zaghla, H.; Zakaria, Z.; Allam, W.R.; Sameea, E.A.; Mikhail, N.N.; Sobhy, M.; Galal, I.F.; Mokhtar, Y.; Hamdy, S.; et al. High spontaneous clearance of symptomatic iatrogenic acute hepatitis C genotype 4 infection. J. Med. Virol. 2018, 90, 1841–1847. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Hepatitis C Key Fact. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c (accessed on 3 July 2021).
- Daw, M.A.; El-Bouzedi, A. Prevalence of hepatitis B and hepatitis C infection in Libya: Results from a national population based survey. BMC Infect. Dis. 2014, 14, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Averhoff, F.M.; Glass, N.; Holtzman, D. Global Burden of Hepatitis C: Considerations for Healthcare Providers in the United States. Clin. Infect. Dis. 2012, 55, S10–S15. [Google Scholar] [CrossRef] [PubMed]
- Elzouki, A.-N. Hepatitis B infection in Libya: The magnitude of the problem. Libyan J. Infect. Dis. 2008, 2, 20–25. [Google Scholar]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021. Towards Ending Viral Hepatitis. World Health Organization. 2016. Available online: https://apps.who.int/iris/handle/10665/246177 (accessed on 3 July 2021).
- Encyclopædia Britannica. Available online: https://www.britannica.com/place/Libya#/media/1/339574/61572 (accessed on 14 January 2022).
- Jin, J. Screening for Hepatitis C Virus Infection. JAMA 2020, 323, 1008. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Zhou, Y.; Lin, X.; Jiang, Y.; Tian, R.; Zhang, Y.; Wu, J.; Zhang, F.; Zhang, Y.; Wang, Y.; et al. General epidemiological parameters of viral hepatitis A, B, C, and E in six regions of China: A cross-sectional study in 2007. PLoS ONE 2009, 4, e8467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.Y.; Kim, I.H.; Jeong, S.H.; Cho, Y.K.; Lee, J.H.; Jin, Y.J.; Lee, D.; Suh, D.J.; Han, K.H.; Park, N.H.; et al. A nationwide seroepidemiology of hepatitis C virus infection in South Korea. Liver Int. 2013, 33, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Li, H.; Ji, Y.; Ma, Y.; Hou, F.; Yuan, P. Hepatitis C virus infection in the general population: A large community-based study in Mianyang, West China. Biosci. Trends 2015, 9, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Q.; Qi, W.; Wang, X.; Zhang, Y.; Xu, Y.; Qin, S.; Zhao, P.; Guo, H.; Jiao, J.; Zhou, C.; et al. Epidemiology of Hepatitis B and Hepatitis C Infections and Benefits of Programs for Hepatitis Prevention in Northeastern China: A Cross-Sectional Study. Clin. Infect. Dis. 2016, 62, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, R.; McQuinn, B.; Purushotham, A. How are we going to rebuild public health in Libya? J. R. Soc. Med. 2011, 104, 490–492. [Google Scholar] [CrossRef]
- Force UPST. Screening for Hepatitis C Virus Infection in Adolescents and Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2020, 323, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Yehia, B.R.; Schranz, A.J.; Umscheid, C.A.; Lo Re, V., 3rd. The treatment cascade for chronic hepatitis C virus infection in the United States: A systematic review and meta-analysis. PLoS ONE 2014, 9, e101554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maier, M.M.; Ross, D.B.; Chartier, M.; Belperio, P.S.; Backus, L.I. Cascade of Care for Hepatitis C Virus Infection within the US Veterans Health Administration. Am. J. Public Health 2016, 106, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Linas, B.P.; Barter, D.M.; Leff, J.A.; Assoumou, S.A.; Salomon, J.A.; Weinstein, M.C.; Kim, A.Y.; Schackman, B.R. The hepatitis C cascade of care: Identifying priorities to improve clinical outcomes. PLoS ONE 2014, 9, e97317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waked, I.; Esmat, G.; Elsharkawy, A.; El-Serafy, M.; Abdel-Razek, W.; Ghalab, R.; Elshishiney, G.; Salah, A.; Abdel Megid, S.; Kabil, K.; et al. Screening and Treatment Program to Eliminate Hepatitis C in Egypt. New Engl. J. Med. 2020, 382, 1166–1174. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ismail, F.; Haq, S.; El-Garawani, I.; Abdelsameea, E. Hepatitis C Virus Infection in Eastern Libya: Efforts Needed to Improve HCV Testing and Linkage to Care in the Resource-Limited Setting. Trop. Med. Infect. Dis. 2022, 7, 14. https://doi.org/10.3390/tropicalmed7020014
Ismail F, Haq S, El-Garawani I, Abdelsameea E. Hepatitis C Virus Infection in Eastern Libya: Efforts Needed to Improve HCV Testing and Linkage to Care in the Resource-Limited Setting. Tropical Medicine and Infectious Disease. 2022; 7(2):14. https://doi.org/10.3390/tropicalmed7020014
Chicago/Turabian StyleIsmail, Faisal, Soghra Haq, Islam El-Garawani, and Eman Abdelsameea. 2022. "Hepatitis C Virus Infection in Eastern Libya: Efforts Needed to Improve HCV Testing and Linkage to Care in the Resource-Limited Setting" Tropical Medicine and Infectious Disease 7, no. 2: 14. https://doi.org/10.3390/tropicalmed7020014