
Myocarditis in a Pediatric Patient with Campylobacter Enteritis: A Case Report and Literature Review

 , , and
, , and
Abstract
:1. Introduction
2. Case Report
3. Discussion and Literature Review
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Law, Y.M.; Lal, A.K.; Chen, S.; Čiháková, D.; Cooper, L.T.; Deshpande, S.; Godown, J.; Grosse-Wortmann, L.; Robinson, J.D.; Towbin, J.A.; et al. Diagnosis and Management of Myocarditis in Children: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e123–e135. [Google Scholar] [CrossRef] [PubMed]
- Hessulf, F.; Ljungberg, J.; Johansson, P.-A.; Lindgren, M.; Engdahl, J. Campylobacter jejuni-associated perimyocarditis: Two case reports and review of the literature. BMC Infect. Dis. 2016, 16, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Putschoegl, A.; Auerbach, S. Diagnosis, Evaluation, and Treatment of Myocarditis in Children. Pediatric Clin. N. Am. 2020, 67, 855–874. [Google Scholar] [CrossRef] [PubMed]
- Dind, A.; Whalley, D. Recurrence of myopericarditis triggered by Campylobacter jejuni. Intern. Med. J. 2019, 49, 409–411. [Google Scholar] [CrossRef] [PubMed]
- Heinzl, B.; Köstenberger, M.; Nagel, B.; Sorantin, E.; Beitzke, A.; Gamillscheg, A. Campylobacter jejuni infection associated with myopericarditis in adolescents: Report of two cases. Eur. J. Pediatr. 2010, 169, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Fica, A.; Seelmann, D.; Porte, L.; Eugenin, D.; Gallardo, R. A case of myopericarditis associated to Campylobacter jejuni infection in the southern hemisphere. Braz. J. Infect. Dis. 2012, 16, 294–296. [Google Scholar] [CrossRef] [Green Version]
- Pena, L.A.; Fishbein, M.C. Fatal myocarditis related to Campylobacter jejuni infection: A case report. Cardiovasc. Pathol. 2007, 16, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Yaita, S.; Tago, M.; Hisata, Y.; Fujiwara, M.; Yamashita, S. Relapse of acute myocarditis associated with Campylobacter jejuni enterocolitis. Clin. Case Rep. 2020, 8, 2605–2609. [Google Scholar] [CrossRef] [PubMed]
- Kanj, S.S.; Araj, G.F.; Taher, A.; Reller, L.B. Campylobacter fetus pericarditis in a patient with β-thalassemia: Case report and review of the literature. Clin. Microbiol. Infect. 2001, 7, 510–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzgerald, C. Campylobacter. Clin. Lab. Med. 2015, 35, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Same, R.G.; Tamma, P.D. Campylobacter Infections in Children. Pediatrics Rev. 2018, 39, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Vaughan-Shaw, P.G.; Rees, J.R.; White, D.; Burgess, P. Campylobacter jejuni cholecystitis: A rare but significant clinical entity. Case Rep. 2010, 2010, bcr1020092365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pope, J.E.; Krizova, A.; Garg, A.X.; Thiessen-Philbrook, H.; Ouimet, J.M. Campylobacter Reactive Arthritis: A Systematic Review. Semin. Arthritis Rheum. 2007, 37, 48–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nachamkin, I.; Allos, B.M.; Ho, T. Campylobacter Species and Guillain-Barré Syndrome. Clin. Microbiol. Rev. 1998, 11, 555–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veerasamy, M.; Alguire, C.T. Food finds its way to a woman’s heart: Campylobacter jejuni-associated myopericarditis. Glob. Cardiol. Sci. Pract. 2017, 2017, e201708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, J.; Fernandes, N.; Alvarez, D.; Khanna, S. Acute Myopericarditis in an Adolescent Mimicking Acute Myocardial Infarction. Pediatric Emerg. Care 2015, 31, 427–430. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reference Values | Emergency Department | Day 2 | Day 3 | Day 6 | Day 8 | ||
|---|---|---|---|---|---|---|---|
| Complete Blood Count | WBC (/μL) | 11,220 | 9750 | 9150 | 9830 | 12,790 | |
| Neu/Lymph/Mono (%) | 80.6/10.8/7 | 78.6/12.5/8 | 74.6/13.5/8 | 51.6/32/9 | 67.2/22.6/6 | ||
| Hgb (mg/dL)/Hct (%) | 12/37.2 | 11.8/35.9 | 11.3/33.9 | 12.3/39 | 12.2/38 | ||
| PLT (/μL) | 226,000 | 205,000 | 185,000 | 306,000 | 298,000 | ||
| Blood Metabolic Panel | U/Cr (mg/dL) | 9–35/0.2–1 | 24/0.84 | 18/0.75 | 15/0.72 | 30/0.7 | 24/0.7 |
| AST/ALT (IU/L) | 10–60/5–45 | 13/12 | 31/17 | 64/23 | 23/34 | 15/25 | |
| LDH (IU/L) | 120–300 | 168 | 285 | 268 | 190 | ||
| CK (IU/L) | <140 | 307 | 643 | 35 | 35 | ||
| Cardiac Biomarkers | CK-MB (ng/mL) | <3 | 25.3 | 51.6 | 0.7 | 0.9 | |
| Troponin T (pg/mL) | <14 | 456.4 | 872.2 | 24.4 | 8.2 | ||
| NT-proBNP (pg/mL) | <300 | 715 | 369 | 185 | |||
| Inflammatory markers | ESR 1sth (mm) | 55 | 45 | ||||
| CRP (mg/L) | <10 | 25.2 | 40.1 | 48.4 | 8.2 | 3.0 | |
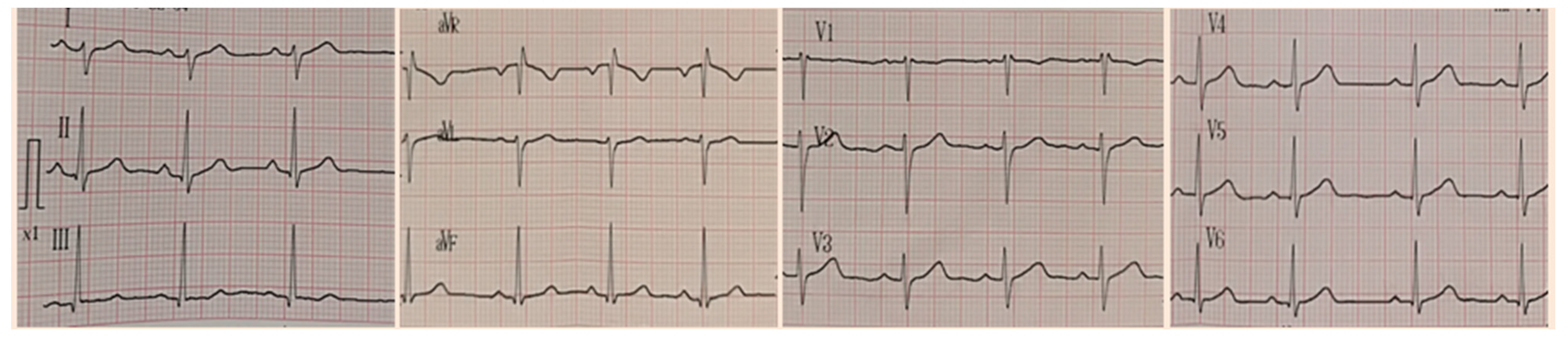
| Cardiology | Electrocardiography | Normal | Normal | Normal | Normal | ||
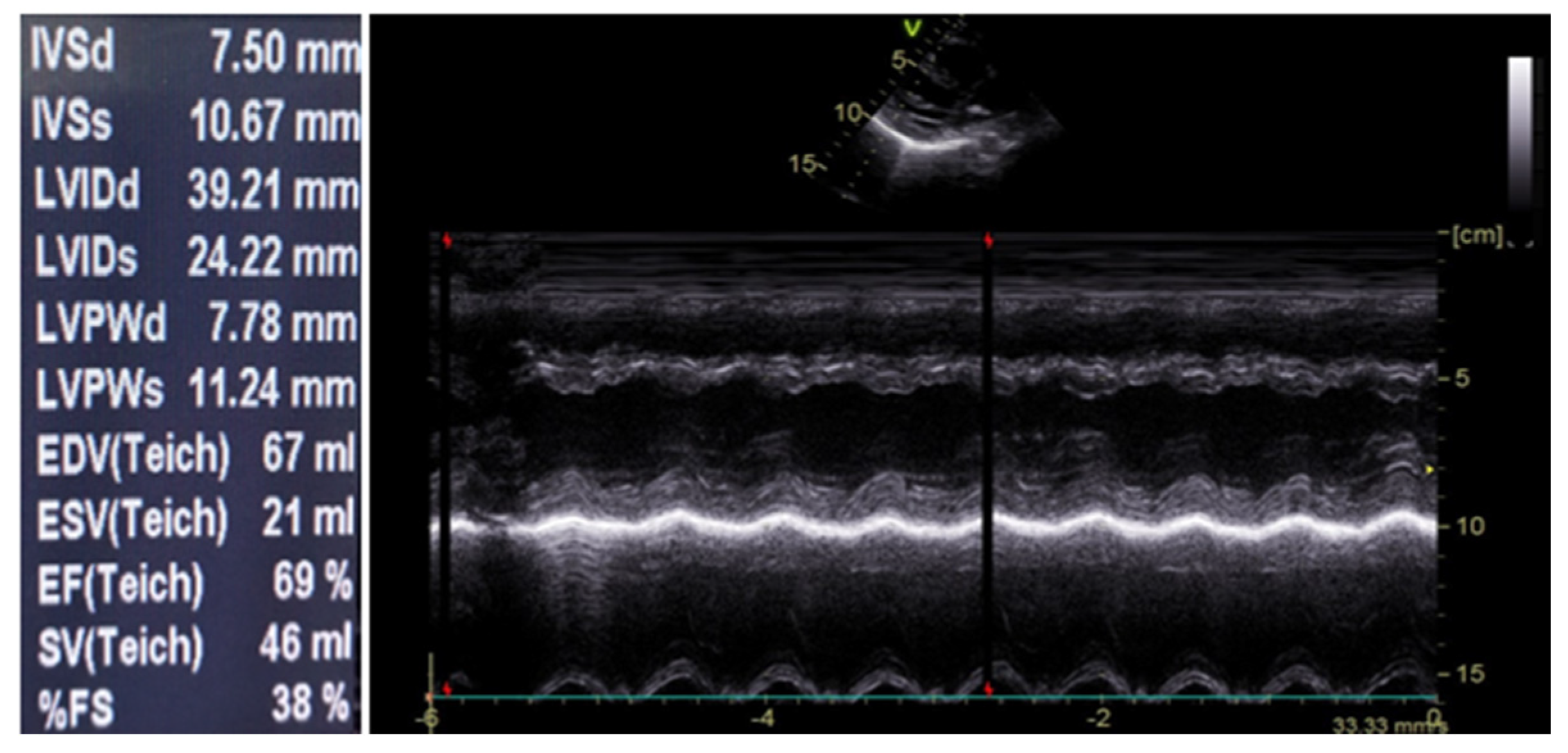
| Echocardiography | Normal | Normal | Normal | Normal | |||
| 24 h Holter monitoring | Normal |
| Test | Day 1 | Day 2 | |||||
|---|---|---|---|---|---|---|---|
| Urinalysis | PH = 6.5 SG = 1016 RBC = 0–2/cfu WBC = 0–2/cfu | ||||||
| Stool culture | Campylobacter jejuni | ||||||
| Blood culture | Negative | ||||||
| Rapid multiplex PCR stool analysis | Campylobacter spp. | ||||||
| Serological testing | EBV | IgM IgG | − | Parvovirus | IgM IgG | − − | |
| + | |||||||
| CMV | IgM IgG | − − | SARS-CoV-2 | IgG | − | ||
| HSV | IgM IgG | − − | Mycoplasma | IgM IgG | − | ||
| + | |||||||
| HHV-6 | IgM IgG | − − | HBV | HBsAg | − | ||
| HIV | Ag Ab | − − | HCV | Anti-HCV | − | ||
| Nasopharyngeal samples | Ag | Influenza A &B | − | ||||
| Adenovirus | − | ||||||
| PCR | Coxsackie A | − | |||||
| Coxsackie B | − | ||||||
| Author Year Country | G/ACardiac Involvement | GIS | CS (GIS-CS Interval) | ECG Changes | Echocardiographic Changes | Elevation of Cardiac Enzymes | Fecal Culture | Treatment (Outcome) |
|---|---|---|---|---|---|---|---|---|
| Yaita [8] 2020 Japan | M/16Myocarditis | Non hemorrhagic watery diarrhea, headache, fever, abdominal pain | Persistent chest pain at rest exacerbated by deep inspiration (4 days) | ST elevation in leads II, aVf, V3, V4, V5, and V6 | No asynergy of ventricular movement or pericardial effusion | Troponin TCKNT-proBNP | C. jejuni | No antibiotics (Recovery) |
| Dind [4] 2019 Australia | M/17Myopericarditis | Diarrhea | Severe central chest pain (7 days) | Widespread concave-up ST elevation | Globally impaired left ventricle LVEF 40% | Troponin I | C. jejuni | AzithromycinColchicineIbuprofenParacetamol (Recovery) |
| Fica [6] 2010 Chile | M/17Myopericarditis | Upper abdominal pain, fever up to 38.5 °C, dysentery | Severe anteriorchest pain relieved by sitting (2 days) | ST-segment elevation on V1-V6 leads, and a negative T wave | Normal | Troponin ICKCK-MB | C. jejuni | Azithromycin (Recovery) |
| Heinzl [5] 2009 Austria | M/16Myopericarditis | Bloody diarrhea, fever up to 40 °C, headache, abdominal pain | Constant chest pain associated with dyspnea (5 days) | Sinus rhythm and significant ST elevation in leads I, II, V4, V5, and V6. | Reduced leftLVEF 45%,shortening fraction 22% | Troponin TCKCK-MB | C. jejuni | Clarithromycin (Recovery) |
| M/17Myopericarditis | Fever up to 38 °C, diarrhea | Recurrent chest pain radiating to left arm (2 days) | Sinus rhythm and significant ST elevation in leads I, AVL, V4, and V5 | Normal left ventricular function without localized areas of hypokinesis, no significant pericardial effusion | Troponin TCKCK-MB | C. jejuni | ClarithromycinMefenamic acid (Recovery) | |
| Pena [7] 2007 USA | M/16Myocarditis | Fever, chills, myalgias, abdominal cramps, body stiffness, diarrhea, vomiting, decreasedappetite, sweats, abdominal tightness, restlessness | Chest tightness on inspiration, difficulty in breathing (4 days) | NR | NR | CK | C. jejuni | No antibiotics (Death) |
| Kanj [9] 2001 Lebanon | F/14Pericarditis | Fever, chills, vomiting, diarrhea | Severe dyspnea, dry cough (4 days) | Diffuse ST segment elevation | Large pericardial effusion, mild mitral regurgitation with significant respiratory variation across the mitral and the tricuspid valves, indicating tamponade | NR | C. fetus | Ampicillin (Recovery) |
| Present case 2021 Grreece | F/13Myocarditis | Fever, headache, abdominal pain, diarrhea | Stabbing pain of the anterior chest | Normal | Normal | Troponin TCKCK-MBNT-proBNP | C. jejuni | Azithromycin Carvedilol Captopril |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chantzaras, A.-P.; Karageorgos, S.; Panagiotou, P.; Georgiadou, E.; Chousou, T.; Spyridopoulou, K.; Paradeisis, G.; Kanaka-Gantenbein, C.; Botsa, E. Myocarditis in a Pediatric Patient with Campylobacter Enteritis: A Case Report and Literature Review. Trop. Med. Infect. Dis. 2021, 6, 212. https://doi.org/10.3390/tropicalmed6040212
Chantzaras A-P, Karageorgos S, Panagiotou P, Georgiadou E, Chousou T, Spyridopoulou K, Paradeisis G, Kanaka-Gantenbein C, Botsa E. Myocarditis in a Pediatric Patient with Campylobacter Enteritis: A Case Report and Literature Review. Tropical Medicine and Infectious Disease. 2021; 6(4):212. https://doi.org/10.3390/tropicalmed6040212
Chicago/Turabian StyleChantzaras, Anastasios-Panagiotis, Spyridon Karageorgos, Panagiota Panagiotou, Elissavet Georgiadou, Theodora Chousou, Kalliopi Spyridopoulou, Georgios Paradeisis, Christina Kanaka-Gantenbein, and Evanthia Botsa. 2021. "Myocarditis in a Pediatric Patient with Campylobacter Enteritis: A Case Report and Literature Review" Tropical Medicine and Infectious Disease 6, no. 4: 212. https://doi.org/10.3390/tropicalmed6040212