
Evaluating the Quality of Latent Tuberculosis Infection Screening in Ireland: A Single-Centre Retrospective Cohort Study


 ,
,
Abstract
:1. Introduction
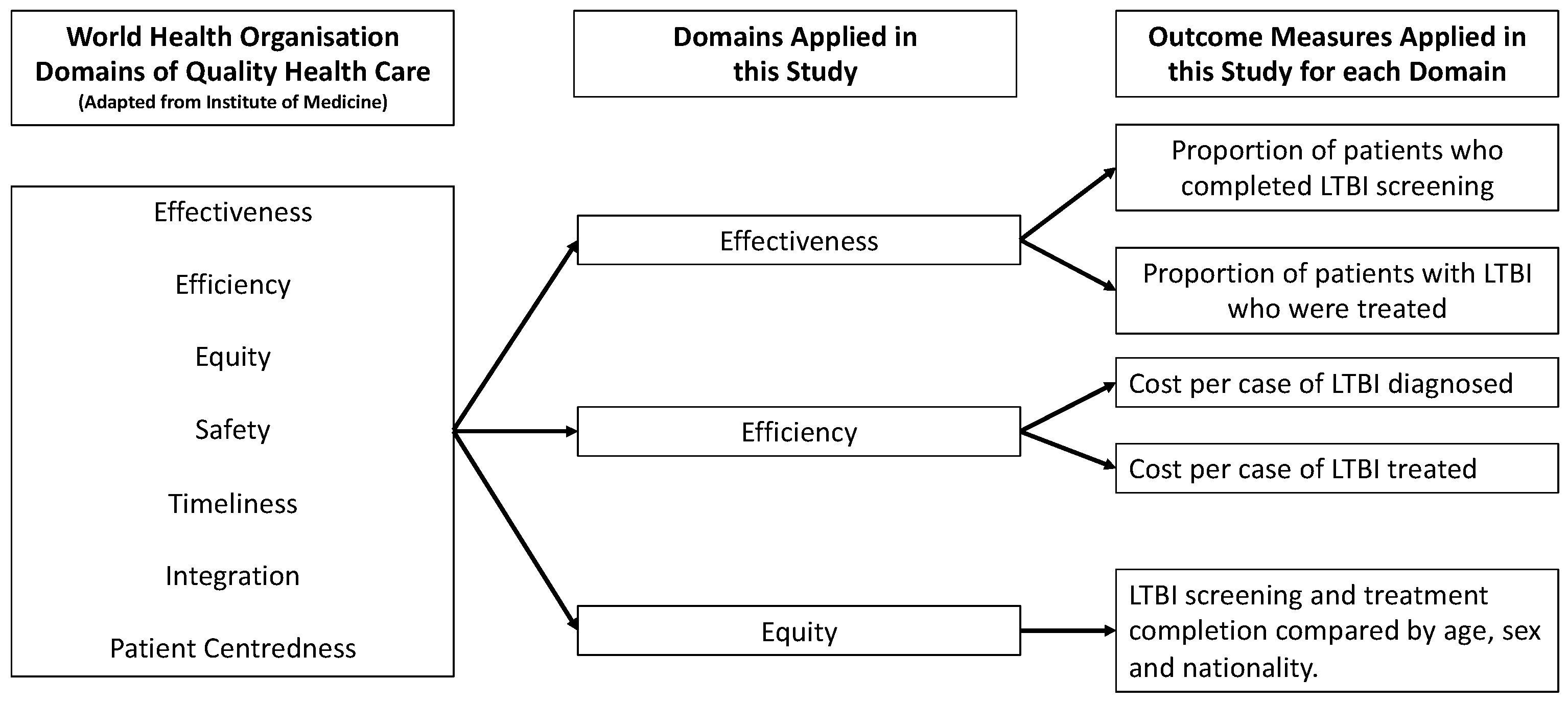
Framework to Measure the Quality of Latent Tuberculosis Infection Screening
2. Methods
2.1. Research Design, Setting, and Sample
2.2. Data Sources
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Description of Cohort Screened
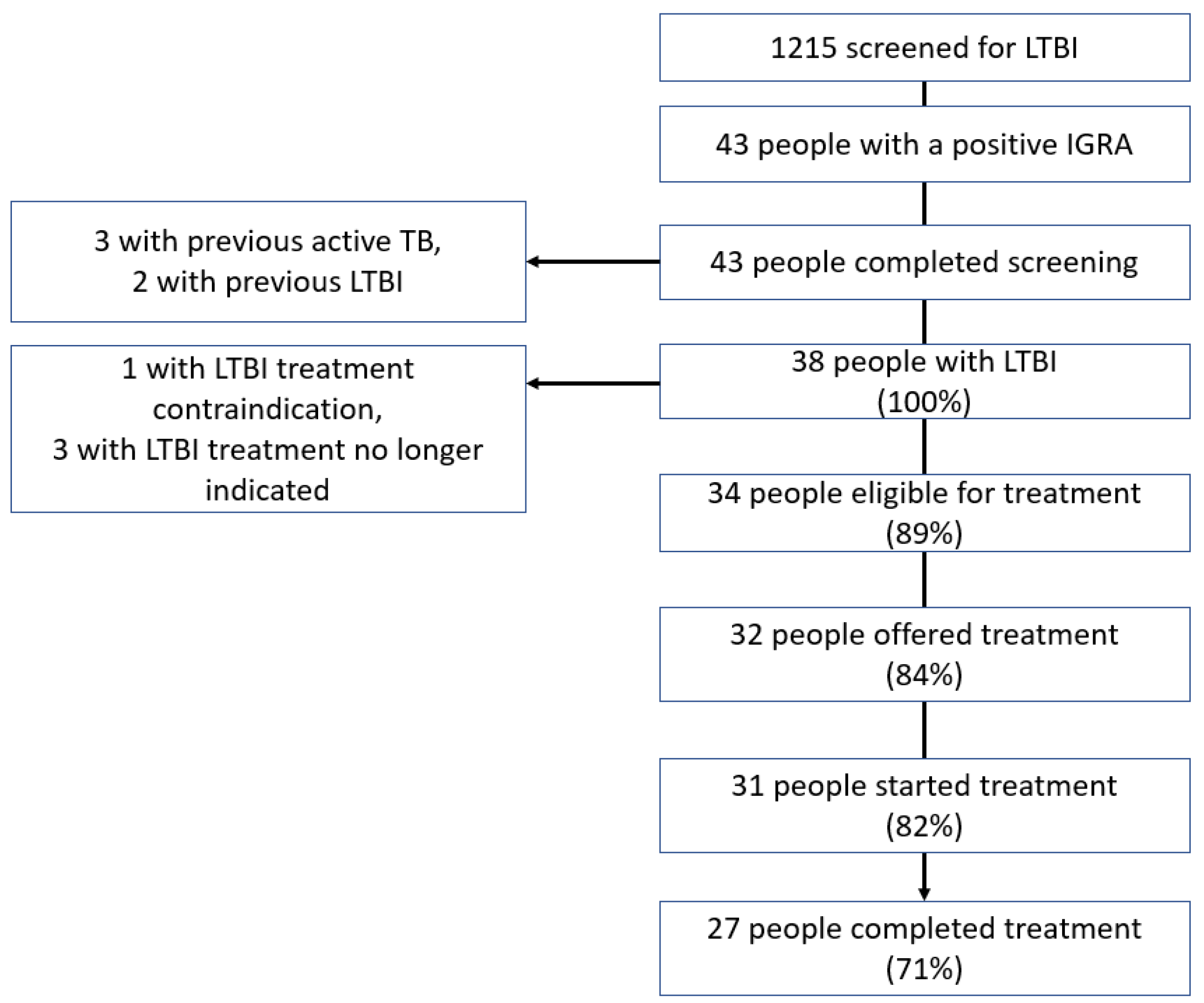
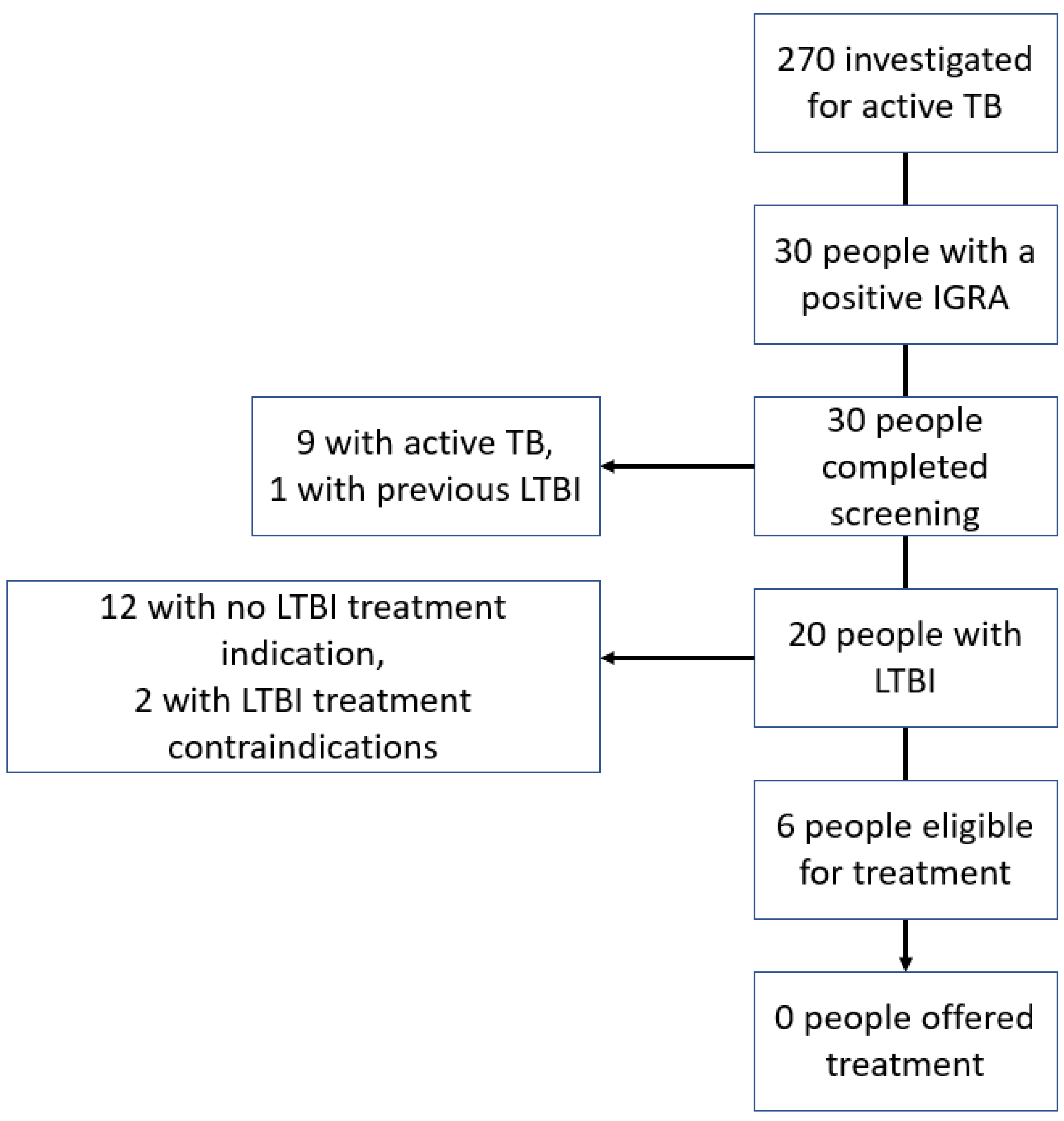
3.2. Screening Effectiveness
3.3. Screening Efficiency
3.4. Equity of Care
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. Global Tuberculosis Report 2020. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/336069/9789240013131-eng.pdf (accessed on 5 August 2021).
- Uplekar, M.; Weil, D.; Lonnroth, K.; Jaramillo, E.; Lienhardt, C.; Dias, H.M.; Falzon, D.; Floyd, K.; Gargioni, G.; Getahun, H.; et al. WHO’s new end TB strategy. Lancet 2015, 385, 1799–1801. [Google Scholar] [CrossRef]
- Lönnroth, K.; Migliori, G.B.; Abubakar, I.; D’Ambrosio, L.; De Vries, G.; Diel, R.; Douglas, P.; Falzon, D.; Gaudreau, M.-A.; Goletti, D.; et al. Towards tuberculosis elimination: An action framework for low-incidence countries. Eur. Respir. J. 2015, 45, 928–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, T.M.; Lalor, M.K.; Broda, A.; Ortega, L.S.; Morgan, M.; Parker, L.; Churchill, S.; Bennett, K.; Golubchik, T.; Giess, A.; et al. Assessment of Mycobacterium tuberculosis transmission in Oxfordshire, UK, 2007–2012, with whole pathogen genome sequences: An observational study. Lancet Respir. Med. 2014, 2, 285–292. [Google Scholar] [CrossRef] [Green Version]
- Shea, K.M.; Kammerer, J.S.; Winston, C.A.; Navin, T.R.; Horsburgh, C.R., Jr. Estimated rate of reactivation of latent tuberculosis infection in the United States, overall and by population subgroup. Am. J. Epidemiol. 2014, 179, 216–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosales-Klintz, S.; Bruchfeld, J.; Haas, W.; Heldal, E.; Houben, R.M.; van Kessel, F.; Mandelbaum, M.; Matteelli, A.; Migliori, G.B.; Oordt-Speets, A.; et al. Guidance for programmatic management of latent tuberculosis infection in the European Union/European Economic Area. Eur Respir. J. 2019, 53, 1802077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferebee, S.H.; Mount, F.W.; Comstock, G.W. The use of chemotherapy as a prophylactic measure in tuberculosis. Ann. N. Y. Acad. Sci. 1963, 106, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Ferebee, S.H.; Mount, F.W. Tuberculosis morbidity in a controlled trial of the prophylactic use of isoniazid among household contacts. American Review of Respiratory Disease. Am. Rev. Respir. Dis. 1962, 85, 490–510. [Google Scholar] [PubMed]
- Health Protection Surveillance Centre. National TB Surveillance 2019. Available online: https://www.hpsc.ie/a-z/vaccinepreventable/tuberculosistb/tbdataandreports/2019_Q1-4_TB_v1.0.pdf (accessed on 6 August 2021).
- Alsdurf, H.; Menzies, D. Identifying gaps in the quality of latent tuberculosis infection care. J. Clin. Tuberc. Other Mycobact. Dis. 2020, 18, 100142. [Google Scholar]
- O’Connell, J.; de Barra, E.; McConkey, S. Systematic review of latent tuberculosis infection research to inform programmatic management in Ireland. Ir. J. Med. Sci. 2021, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Baker, A. Crossing the Quality Chasm: A New Health System for the 21st Century; British Medical Journal Publishing Group: London, UK, 2001. [Google Scholar]
- World Health Organization. Delivering Quality Health Services: A Global Imperative for Universal Health Coverage. 2018. Available online: https://apps.who.int/iris/handle/10665/272465 (accessed on 5 August 2021).
- Alsdurf, H.; Hill, P.C.; Matteelli, A.; Getahun, H.; Menzies, D. The cascade of care in diagnosis and treatment of latent tuberculosis infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2016, 16, 1269–1278. [Google Scholar] [CrossRef]
- National Health Service. National Latent TB Infection Testing and Treatment Programme England. Available online: https://www.england.nhs.uk/tuberculosis-programme/area-for-action-8-national-latent-tb-infection-testing-and-treatment-programme/ (accessed on 11 July 2021).
- Assumpta, K.; Mater Misericordiae University Hospital, Dublin, Ireland; O’Connell, J.; Royal College of Surgeons in Ireland, Dublin, Ireland. Personal Communication, 6 June 2019.
- Bernardrine Luttrell; QIAGEN, Hilden, Germany; O’Connell, J.; Royal College of Surgeons in Ireland, Dublin, Ireland. Personal Communication, 24 June 2019.
- Public Spending Code E.01 Calculation of Staff Costs. 2019. Available online: https://govacc.per.gov.ie/wp-content/uploads/Public-Spending-Code-Consolidated-Document.pdf (accessed on 7 March 2021).
- Knottnerus, A.; Tugwell, P. STROBE-A checklist to Strengthen the Reporting of Observational Studies in Epidemiology. J. Clin. Epidemiol. 2008, 61, 323. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Tuberculosis Profiles. 2022. Available online: https://worldhealthorg.shinyapps.io/tb_profiles/?_inputs_&entity_type=%22country%22&lan=%22EN%22&iso2=%22AF%22 (accessed on 21 January 2022).
- StataCorp. Stata Statistical Software; Release 16; StataCorp LLC.: College Station, TX, USA, 2019. [Google Scholar]
- Erkens, C.G.; Slump, E.; Verhagen, M.; Schimmel, H.; de Vries, G.; Cobelens, F.; Hof, S.V.D. Monitoring latent tuberculosis infection diagnosis and management in the Netherlands. Eur. Respir. J. 2016, 47, 1492–1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jong, M.J.; Roosen, D.; van Tubergen, A. The prevalence of latent tuberculosis and hepatitis B after systematic screening of patients prescribed biological therapy in a low-endemic area. J. Crohns Colitis 2018, 12, 124–125. [Google Scholar] [CrossRef] [PubMed]
- Thi, A.A.; Abbara, A.; Bouri, S.; Collin, S.M.; Wolfson, P.; Owen, L.; Buell, K.; John, L.; Hart, A.L. Challenges in screening for latent tuberculosis in inflammatory bowel disease prior to biologic treatment: A UK cohort study. Frontline Gastroenterol. 2018, 9, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Dobler, C.C.; Marks, G.B. Completion of treatment for latent tuberculosis infection with monthly drug dispensation directly through the tuberculosis clinic. PLoS ONE 2012, 7, e48900. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.; de Barra, E.; McNally, C.; McConkey, S. A Survey of Latent Tuberculosis Screening and Treatment Practices in a Tertiary Centre. Ir. Med. J. 2021, 114, 406. [Google Scholar] [PubMed]
- O’Meara, M. An Evaluation of TB Service Delivery in the Northern Area Health Board. Ph.D. Thesis, Faculty of Public Health Medicine, Royal College of Physicians of Ireland, Dublin, Ireland, 2007. [Google Scholar]
- Grant, C.; McHugh, J.; Ryan, C.; Scarry, M.; O’Regan, A.; Tuite, H.; Fleming, C. Symptoms to script: Delays in tuberculosis treatment in the west of Ireland. Ir. J. Med. Sci. 2022, 191, 295–300. [Google Scholar] [CrossRef]
- Price, M.A. A Qualitative Study to Explore the Lived Experiences of Patients with Tuberculosis in the Community. Ph.D. Thesis, Royal College of Surgeons in Ireland, Dublin, Ireland, 2008. [Google Scholar]
- Roycroft, E.; Fitzgibbon, M.; Kelly, D.; Scully, M.; McLaughlin, A.; Flanagan, P.; Gordon, S.V.; Rogers, T.R.; Keane, J.; O´meara, M. The largest prison outbreak of TB in Western Europe investigated using whole-genome sequencing. Int. J. Tuberc. Lung Dis. 2021, 25, 491–497. [Google Scholar] [CrossRef]
- Conroy, O.; Wurie, F.; Collin, S.M.; Edmunds, M.; de Vries, G.; Lönnroth, K.; Abubakar, I.; Anderson, S.R.; Zenner, D. Barriers and enablers to implementing tuberculosis control strategies in EU and European Economic Area countries: A systematic review. Lancet Infect. Dis. 2021, 21, e272–e280. [Google Scholar] [CrossRef]
- O’Brien, K.; Ikram, S.; Burman, M.; Kunst, H. Barriers and facilitators of a latent tuberculosis screening and treatment programme of recent migrants. Eur Respir. J. 2020, 56, 508. [Google Scholar]
- Healthatlas Ireland NQAIS Clinical. Available online: https://www.healthatlasireland.ie/ (accessed on 31 May 2020).
- Health Protection Surveillance Centre. Guidelines on the Prevention and Control of Tuberculosis in Ireland 2010. Available online: https://www.hpsc.ie/a-z/vaccinepreventable/tuberculosistb/guidance/tbguidelines2010amended2014/File,4349,en.pdf (accessed on 5 August 2021).




{kind=link}
{kind=link}
{kind=link}
| Indication Group | Number of Tests (Proportion of Total Tests) | Positive IGRA (Proportion of Tests in Indication Group) | Number of Individuals (Proportion of Total Individuals) | Individuals Testing Positive (Proportion of Individuals in Indication Group) |
|---|---|---|---|---|
| Immunosuppression therapy | 1312 (78%) | 44 (3.3%) | 1164 (77.2%) | 40 (2.7%) |
| Investigation for active TB | 281 (16.7%) | 32 (11.4%) | 270 (17.9%) | 30 (11.4%) |
| Recent TB case contact | 28 (1.7%) | 2 (7.1%) | 25 (1.7%) | 2 (8%) |
| HIV | 9 (<1%) | 0 | 9 (<1%) | 0 |
| Pre-organ transplantation | 9 (<1%) | 1 (11.1%) | 8 (<1%) | 1 (12.5%) |
| Person from high incidence TB country | 2 (<1%) | 0 | 2 (<1%) | 0 |
| Radiological finding of LTBI | 3 (<1%) | 0 | 3 (<1%) | 0 |
| Unknown | 37 (2.2%) | 0 | 36 (2.4%) | 0 |
| Total | 1681 | 79 | 1507 * | 73 |
| Variable | Not Treated for LTBI (n = 13) | Treated for LBTI (n = 27) | Odds Ratio (Not Treated for LTBI vs. Treated for LTBI) |
|---|---|---|---|
| Age (years, mean ± SD) | 53.5 ± 12.1 | 55.7 ± 14.8 | 0.98 (95% CI 0.94–1.03, p = 0.64) |
| Sex | |||
| Men | 26% (6/23) | 74% (17/23) | 0.50 (95% CI 0.13–1.92, p = 0.317) |
| Women | 41% (7/17) | 59% (10/17) | |
| Nationality | |||
| Non-Irish | 67% (6/9) | 33% (3/9) | 6.86 (95% CI 1.35–34.70, p < 0.05) |
| Irish | 23% (7/31) | 77% (24/31) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Connell, J.; Oguntuase, J.; Li, B.; McNally, C.; Stanistreet, D.; McConkey, S.; de Barra, E. Evaluating the Quality of Latent Tuberculosis Infection Screening in Ireland: A Single-Centre Retrospective Cohort Study. Trop. Med. Infect. Dis. 2022, 7, 19. https://doi.org/10.3390/tropicalmed7020019
O’Connell J, Oguntuase J, Li B, McNally C, Stanistreet D, McConkey S, de Barra E. Evaluating the Quality of Latent Tuberculosis Infection Screening in Ireland: A Single-Centre Retrospective Cohort Study. Tropical Medicine and Infectious Disease. 2022; 7(2):19. https://doi.org/10.3390/tropicalmed7020019
Chicago/Turabian StyleO’Connell, James, Joy Oguntuase, Brian Li, Cora McNally, Debbi Stanistreet, Samuel McConkey, and Eoghan de Barra. 2022. "Evaluating the Quality of Latent Tuberculosis Infection Screening in Ireland: A Single-Centre Retrospective Cohort Study" Tropical Medicine and Infectious Disease 7, no. 2: 19. https://doi.org/10.3390/tropicalmed7020019