
Postural Evaluation in Young Healthy Adults through a Digital and Reproducible Method


 ,
,  , and
, and 
Abstract
:
1. Introduction
2. Materials and Methods
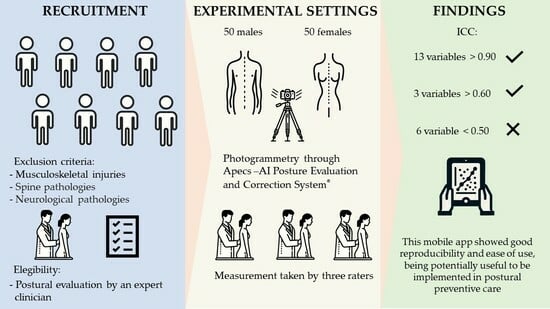
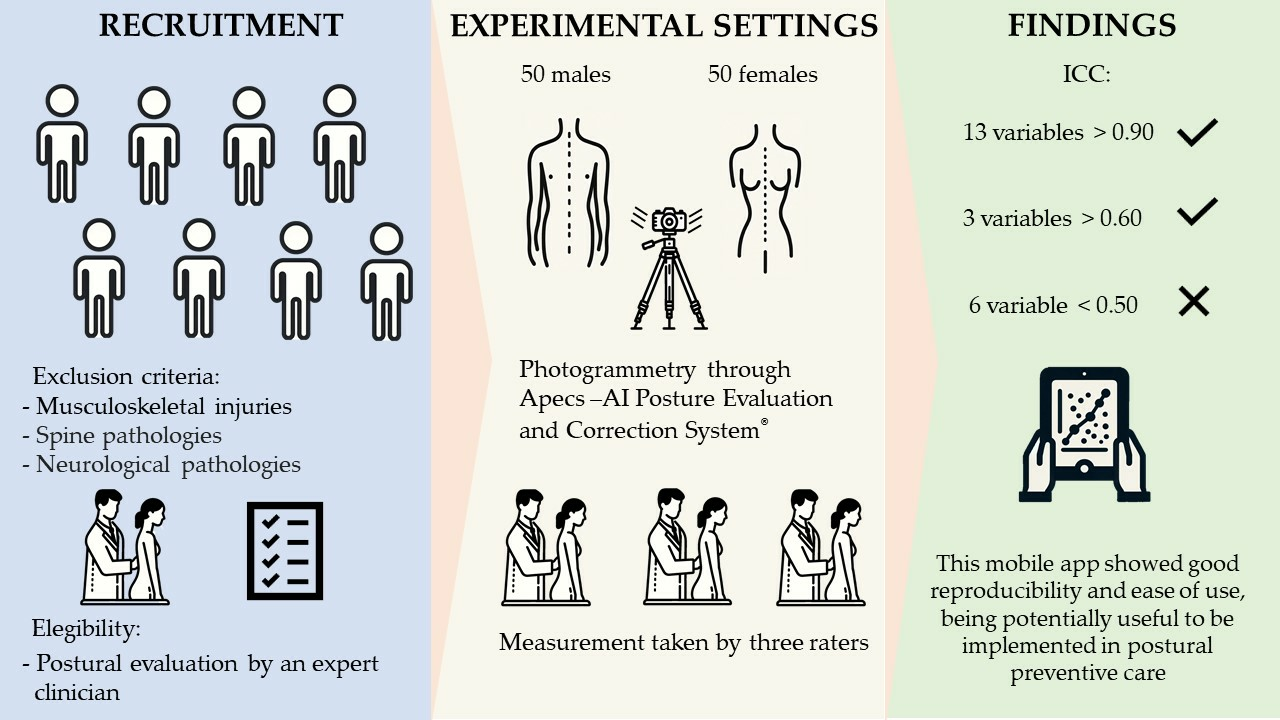
2.1. Participants
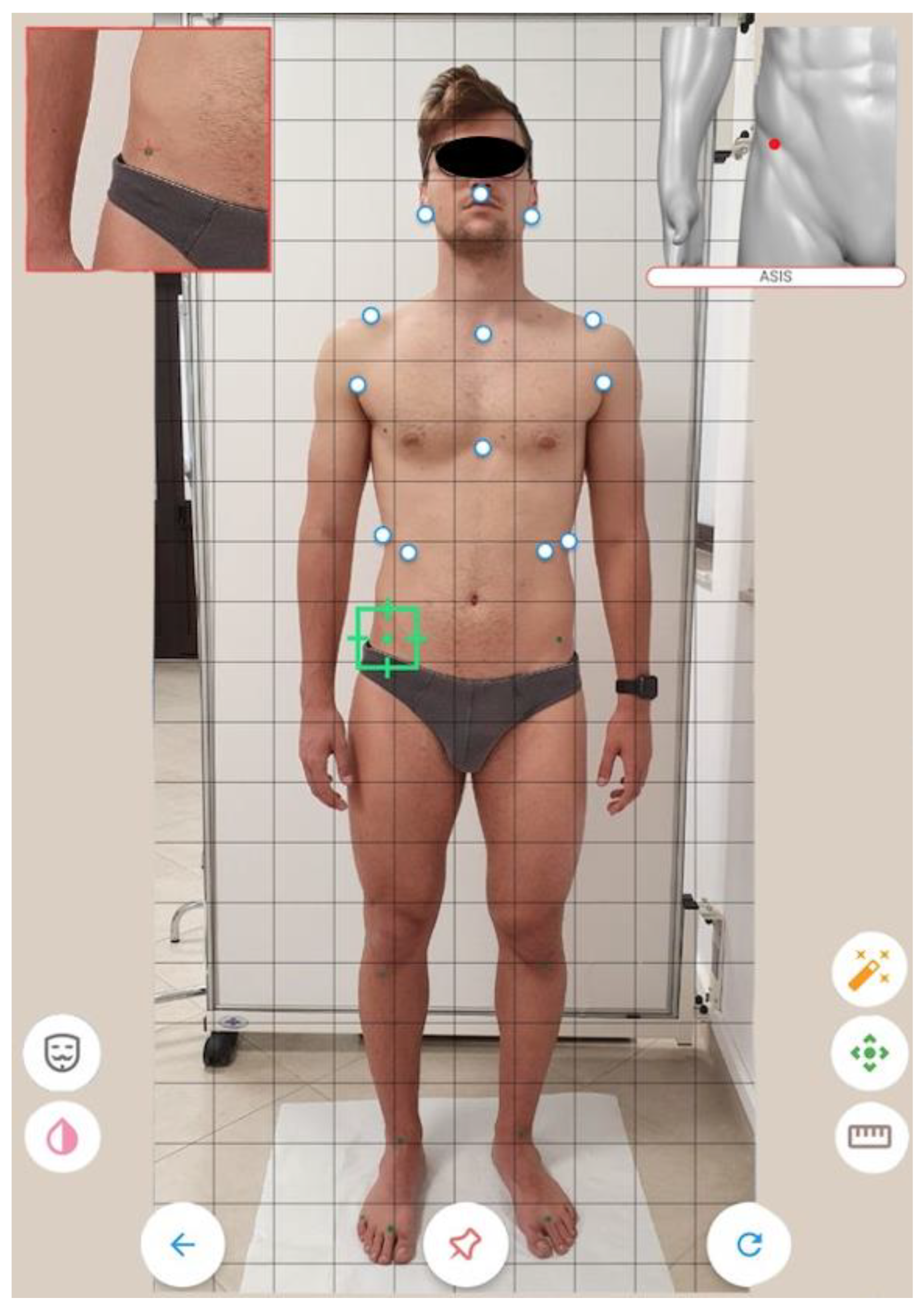
2.2. Study Design
2.3. Statistical Analysis
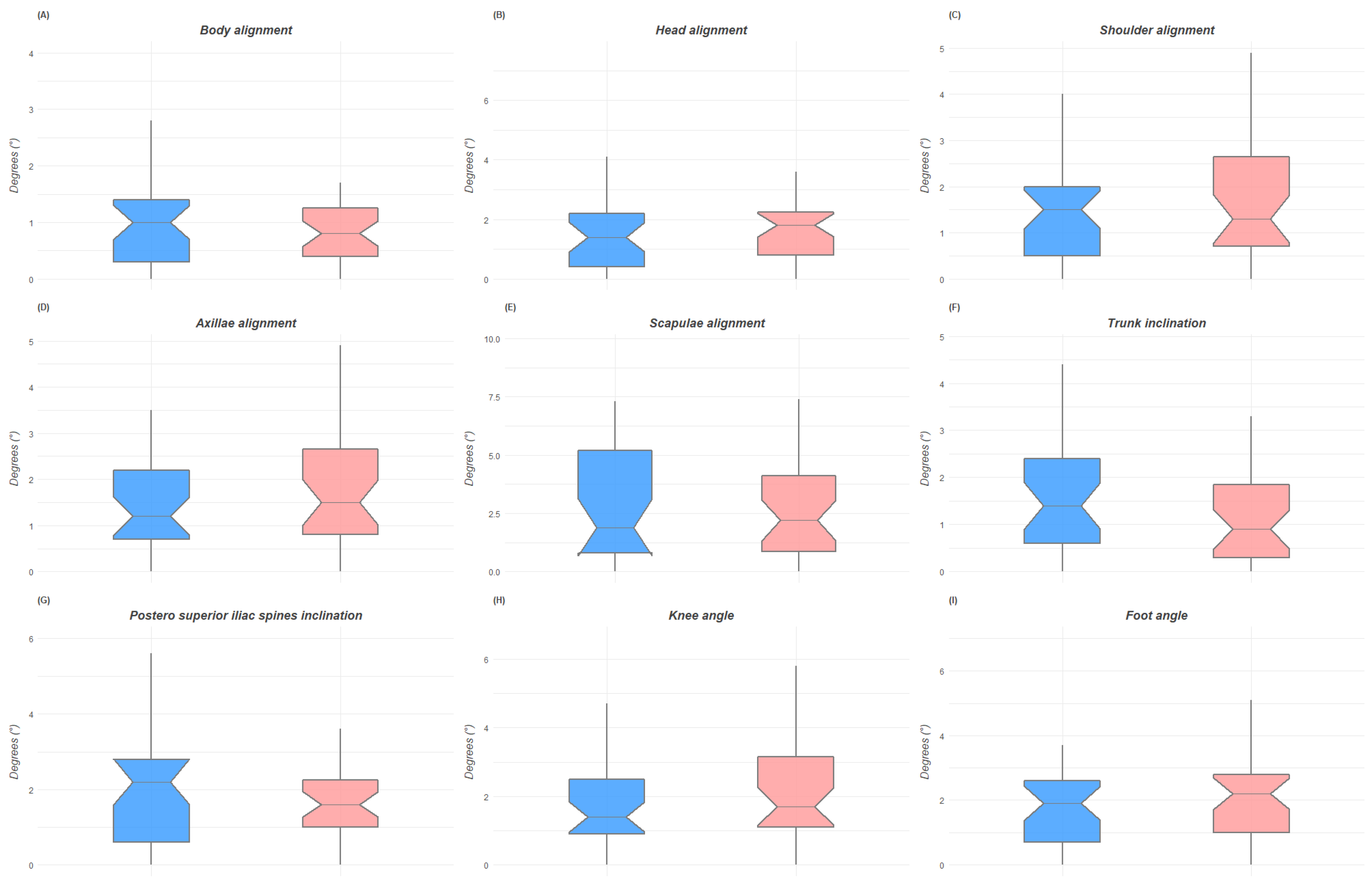
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carini, F.; Mazzola, M.; Fici, C.; Palmeri, S.; Messina, M.; Damiani, P.; Tomasello, G. Posture and posturology, anatomical and physiological profiles: Overview and current state of art. Acta Biomed. 2017, 88, 11–16. [Google Scholar] [CrossRef]
- Rodrigues, M.S.; Leite, R.D.V.; Lelis, C.M.; Chaves, T.C. Differences in ergonomic and workstation factors between computer office workers with and without reported musculoskeletal pain. Work 2017, 57, 563–572. [Google Scholar] [CrossRef] [Green Version]
- Harvey, R.H.; Peper, E.; Mason, L.; Joy, M. Effect of Posture Feedback Training on Health. Appl. Psychophysiol. Biofeedback 2020, 45, 59–65. [Google Scholar] [CrossRef]
- Hopkins, B.B.; Vehrs, P.R.; Fellingham, G.W.; George, J.D.; Hager, R.; Ridge, S.T. Validity and Reliability of Standing Posture Measurements Using a Mobile Application. J. Manip. Physiol. Ther. 2019, 42, 132–140. [Google Scholar] [CrossRef]
- Fortin, C.; Feldman, D.E.; Cheriet, F.; Labelle, H. Clinical methods for quantifying body segment posture: A literature review. Disabil. Rehabil. 2011, 33, 367–383. [Google Scholar] [CrossRef] [Green Version]
- Roggio, F.; Ravalli, S.; Maugeri, G.; Bianco, A.; Palma, A.; Di Rosa, M.; Musumeci, G. Technological advancements in the analysis of human motion and posture management through digital devices. World J. Orthop. 2021, 12, 467–484. [Google Scholar] [CrossRef]
- Betsch, M.; Wild, M.; Jungbluth, P.; Hakimi, M.; Windolf, J.; Haex, B.; Horstmann, T.; Rapp, W. Reliability and validity of 4D rasterstereography under dynamic conditions. Comput. Biol. Med. 2011, 41, 308–312. [Google Scholar] [CrossRef]
- Molinaro, L.; Russo, L.; Cubelli, F.; Taborri, J.; Rossi, S. Reliability analysis of an innovative technology for the assessment of spinal abnormalities. In Proceedings of the 2022 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Messina, Italy, 22–24 June 2022; pp. 1–6. [Google Scholar]
- Paloschi, D.; Bravi, M.; Schena, E.; Miccinilli, S.; Morrone, M.; Sterzi, S.; Saccomandi, P.; Massaroni, C. Validation and Assessment of a Posture Measurement System with Magneto-Inertial Measurement Units. Sensors 2021, 21, 6610. [Google Scholar] [CrossRef]
- Leirós-Rodríguez, R.; Romo-Pérez, V.; García-Soidán, J.L.; Soto-Rodríguez, A. Identification of Body Balance Deterioration of Gait in Women Using Accelerometers. Sustainability 2020, 12, 1222. [Google Scholar] [CrossRef] [Green Version]
- Tyson, S.F.; DeSouza, L.H. A clinical model for the assessment of posture and balance in people with stroke. Disabil. Rehabil. 2003, 25, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Youdas, J.W.; Carey, J.R.; Garrett, T.R. Reliability of measurements of cervical spine range of motion--comparison of three methods. Phys. Ther. 1991, 71, 98–104; discussion 105–106. [Google Scholar] [CrossRef] [PubMed]
- Timurtaş, E.; Avcı, E.E.; Mate, K.; Karabacak, N.; Polat, M.G.; Demirbüken, İ. A mobile application tool for standing posture analysis: Development, validity, and reliability. Ir. J. Med. Sci. 2021, 191, 2123–2131. [Google Scholar] [CrossRef] [PubMed]
- Szucs, K.A.; Brown, E.V.D. Rater reliability and construct validity of a mobile application for posture analysis. J. Phys. Ther. Sci. 2018, 30, 31–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreira, R.; Fialho, R.; Teles, A.S.; Bordalo, V.; Vasconcelos, S.S.; Gouveia, G.P.M.; Bastos, V.H.; Teixeira, S. A computer vision-based mobile tool for assessing human posture: A validation study. Comput. Methods Programs Biomed. 2022, 214, 106565. [Google Scholar] [CrossRef]
- Heyward, V.H. Advanced fitness assessment and exercise prescription. Med. Sci. Sport. Exerc. 1992, 24, 278. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Belli, G.; Toselli, S.; Latessa, P.M.; Mauro, M. Evaluation of Self-Perceived Body Image in Adolescents with Mild Idiopathic Scoliosis. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 319–333. [Google Scholar] [CrossRef]
- Boguszewski, D.V.; Cheung, E.C.; Joshi, N.B.; Markolf, K.L.; McAllister, D.R. Male-Female Differences in Knee Laxity and Stiffness: A Cadaveric Study. Am. J. Sports Med. 2015, 43, 2982–2987. [Google Scholar] [CrossRef]
- Raine, S.; Twomey, L.T. Head and shoulder posture variations in 160 asymptomatic women and men. Arch. Phys. Med. Rehabil. 1997, 78, 1215–1223. [Google Scholar] [CrossRef]
- Iacob, S.M.P.; Chisnoiu, A.M.P.; Lascu, L.M.P.; Berar, A.M.P.; Studnicska, D.M.; Fluerasu, M.I.P. Is PostureScreen® Mobile app an accurate tool for dentists to evaluate the correlation between malocclusion and posture? Cranio 2020, 38, 233–239. [Google Scholar] [CrossRef]
- Zhao, X.; Tsujimoto, T.; Kim, B.; Katayama, Y.; Tanaka, K. Characteristics of foot morphology and their relationship to gender, age, body mass index and bilateral asymmetry in Japanese adults. J. Back Musculoskelet Rehabil. 2017, 30, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Redmond, A.C.; Crane, Y.Z.; Menz, H.B. Normative values for the Foot Posture Index. J. Foot Ankle Res. 2008, 1, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gimunová, M.; Válková, H.; Kalina, T.; Vodička, T. The relationship between body composition and foot posture index in Special Olympics athletes. Acta Bioeng. Biomech. 2019, 21, 47–52. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Plane of the Space | Anatomical Landmarks | Postural Variables |
|---|---|---|
| Anterior coronal | Acromion Anterior axillary folds Anterior superior iliac spine Jugular notch Lobulus auriculae Lowest point of costal margin Midpoint between malleoli Most intended point of the trunk Philtrum Second metatarsophalangeal joint Tibial tuberosity Xiphoid process | Body alignment Head alignment Acromion alignment Axillae alignment Trunk inclination Ribcage tilt Antero superior iliac spine inclination Knee angle |
| Posterior coronal | Lobulus auriculae C-7 vertebrae Acromion Anterior axillary folds Inferior angle of the scapula T-6 vertebrae Most intended point of the trunk Posterior superior iliac spine Superior end of intergluteal cleft Popliteal fossa Calcaneal tuberosity | Body alignment Head alignment Shoulder alignment Axillae alignment Scapulae alignment Trunk inclination Postero superior iliac spines Knee angle Foot angle |
| Sagittal | Tragus C-7 vertebrae Acromion Posterior superior iliac spine Greater trochanter Lateral joint line Lateral malleolus Head of the fifth metatarsal bone | Body alignment Head alignment Acromion alignment Pelvic tilt Tibia shift Fibula alignment Foot angle |
| Postural Variables | Total | Males | Females | t-Test | ICC | Cohen d | |
|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |||||
| Anterior coronal | Body alignment | 0.9° ± 0.5 | 0.7° ± 0.4 | 1° ± 0.5 | 0.430 | 0.95 | −0.54 |
| Head alignment | 2° ± 1.4 | 2.2° ± 1.8 | 1.8° ± 1.4 | 0.989 | 0.51 | 0.25 | |
| Acromion alignment | 1.3° ± 1 | 1.4° ± 0.9 | 1.2° ± 1.1 | 0.423 | 0.91 | 0.17 | |
| Axillae alignment | 1.3° ± 1 | 1.4° ± 1.4 | 1.2° ± 0.8 | 0.044 * | 0.25 | 0.16 | |
| Trunk inclination | 1.6° ± 1.2 | 1.4° ± 1.3 | 1.8° ± 1.1 | 0.462 | 0.44 | −0.29 | |
| Ribcage tilt | 1.9° ± 1.6 | 1.7° ± 1.2 | 2.2° ± 1.8 | 0.039 * | 0.93 | −0.35 | |
| ASIS inclination | 2.3° ± 1.6 | 2.5° ± 1.7 | 1.5° ± 0.3 | 0.321 | 0.94 | 0.24 | |
| Knee angle | 6.2° ± 3.3 | 4.8° ± 2.9 | 7.5° ± 3.1 | 0.001 *** | 0.93 | −0.89 | |
| Posterior coronal | Body alignment | 1° ± 0.8 | 1° ± 0.8 | 0.9° ± 0.8 | 0.717 | 0.84 | 0.07 |
| Head alignment | 2.7° ± 1.5 | 1.6° ± 1.4 | 1.8° ± 1.5 | 0.652 | 0.30 | −0.14 | |
| Shoulder alignment | 1.5° ± 1.2 | 1.4° ± 1.1 | 1.7° ± 1.4 | 0.444 | 0.93 | −0.19 | |
| Axillae alignment | 1.6° ± 1.2 | 1.4° ± 1 | 1.7° ± 1.2 | 0.348 | 0.43 | −0.26 | |
| Scapulae alignment | 2.7° ± 2.2 | 2.8° ± 2.3 | 2.7° ± 2.2 | 0.879 | 0.92 | 0.05 | |
| Trunk inclination | 1.4° ± 1.2 | 1.6° ± 1.2 | 1.3° ± 1.2 | 0.925 | 0.26 | 0.23 | |
| PSIS inclination | 1.9° ± 1.4 | 2° ± 1.6 | 1.8° ± 1.3 | 0.247 | 0.66 | 0.15 | |
| Knee angle | 1.9° ± 1.4 | 1.8° ± 1.2 | 2.1° ± 1.6 | 0.172 | 0.94 | −0.23 | |
| Foot angle | 2.1° ± 1.6 | 1.9° ± 1.4 | 2.3° ± 1.8 | 0.151 | 0.75 | −0.24 | |
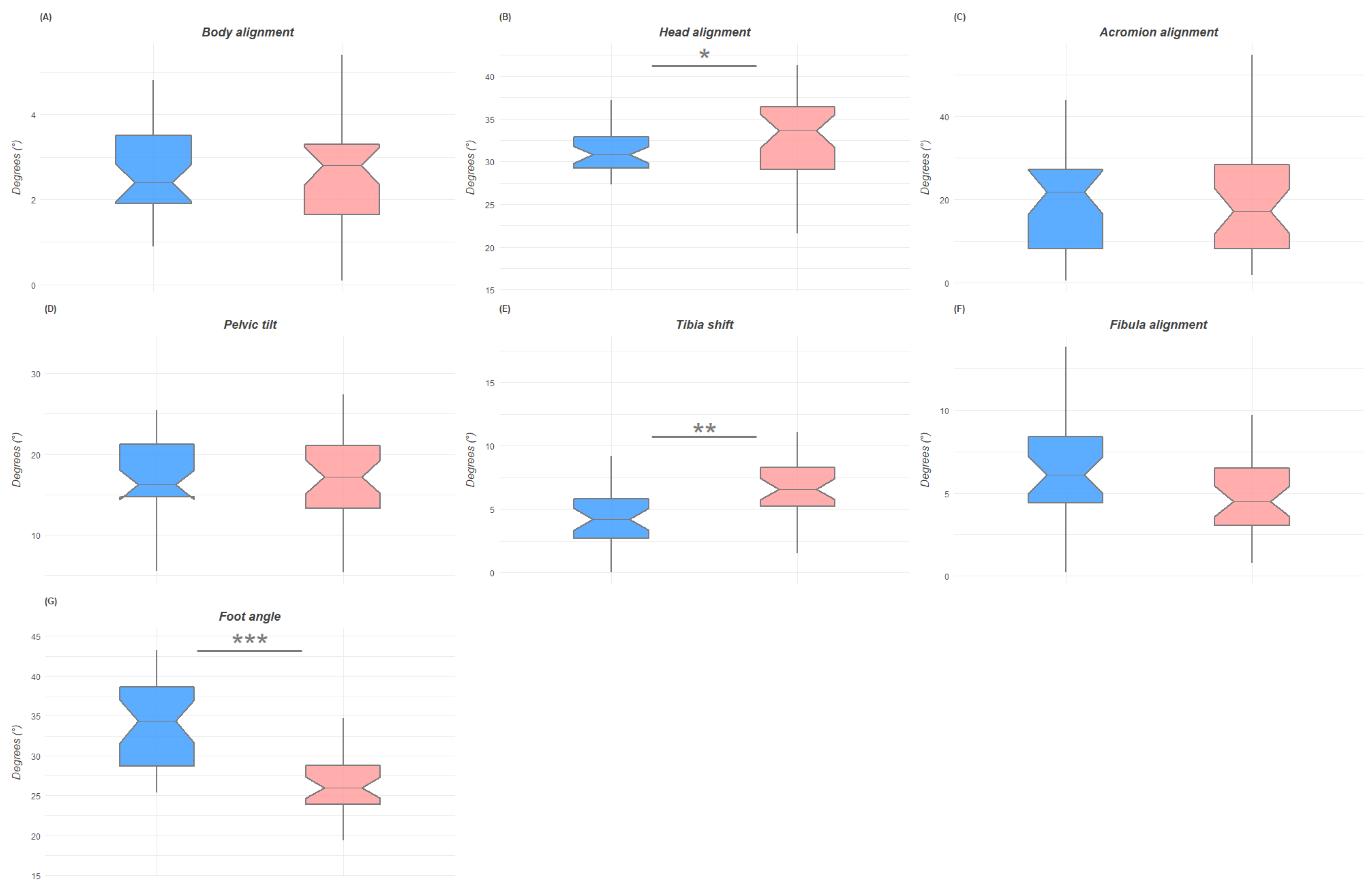
| Sagittal | Body alignment | 2.6° ± 1.2 | 2.6° ± 1.1 | 2.5° ± 1.3 | 0.691 | 0.94 | 0.1 |
| Head alignment | 31.4° ± 5.4 | 30.3° ± 4.3 | 32.4° ± 6.2 | 0.047 * | 0.91 | −0.38 | |
| Acromion alignment | 19.6° ± 12.3 | 19.9° ± 12.1 | 19.4° ± 12.8 | 0.866 | 0.24 | 0.04 | |
| Pelvic tilt | 16.9° ± 5.7 | 16.6° ± 5.3 | 17.1° ± 6.1 | 0.763 | 0.94 | −0.07 | |
| Tibia shift | 5.7° ± 3.3 | 4.2° ± 2.2 | 7.1° ± 3.5 | 0.017 ** | 0.91 | −0.95 | |
| Fibula alignment | 5.5° ± 3 | 6.3° ± 3.1 | 4.8° ± 2.7 | 0.491 | 0.94 | 0.49 | |
| Foot angle | 29.8° ± 6 | 33.7° ± 26.2 | 26.2° ± 4.2 | 0.001 *** | 0.93 | 1.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trovato, B.; Roggio, F.; Sortino, M.; Zanghì, M.; Petrigna, L.; Giuffrida, R.; Musumeci, G. Postural Evaluation in Young Healthy Adults through a Digital and Reproducible Method. J. Funct. Morphol. Kinesiol. 2022, 7, 98. https://doi.org/10.3390/jfmk7040098
Trovato B, Roggio F, Sortino M, Zanghì M, Petrigna L, Giuffrida R, Musumeci G. Postural Evaluation in Young Healthy Adults through a Digital and Reproducible Method. Journal of Functional Morphology and Kinesiology. 2022; 7(4):98. https://doi.org/10.3390/jfmk7040098
Chicago/Turabian StyleTrovato, Bruno, Federico Roggio, Martina Sortino, Marta Zanghì, Luca Petrigna, Rosario Giuffrida, and Giuseppe Musumeci. 2022. "Postural Evaluation in Young Healthy Adults through a Digital and Reproducible Method" Journal of Functional Morphology and Kinesiology 7, no. 4: 98. https://doi.org/10.3390/jfmk7040098