
Connected Blockchain Federations for Sharing Electronic Health Records



Abstract
:1. Introduction
- Development of a novel healthcare blockchain integration model using transaction-based inter-blockchain communication for EHR sharing in a federation of independent blockchains.
- The use of local and global smart contracts to establish communication links and transaction flow in a blockchain federation.
- Implementation of independent blockchains in healthcare, which represent the first example where an inter-blockchain communication model is implemented for healthcare data sharing. Two Hyperledger Fabric networks are used that operate independently, with each running different business logic. Both networks are integrated for inter-blockchain communication to enable EHR sharing among them.
- Defining a set of metrics used to evaluate the performance of independent blockchains and the derived inter-blockchain communication model while demonstrating improvements in performance results compared with previous work.
2. Literature Review
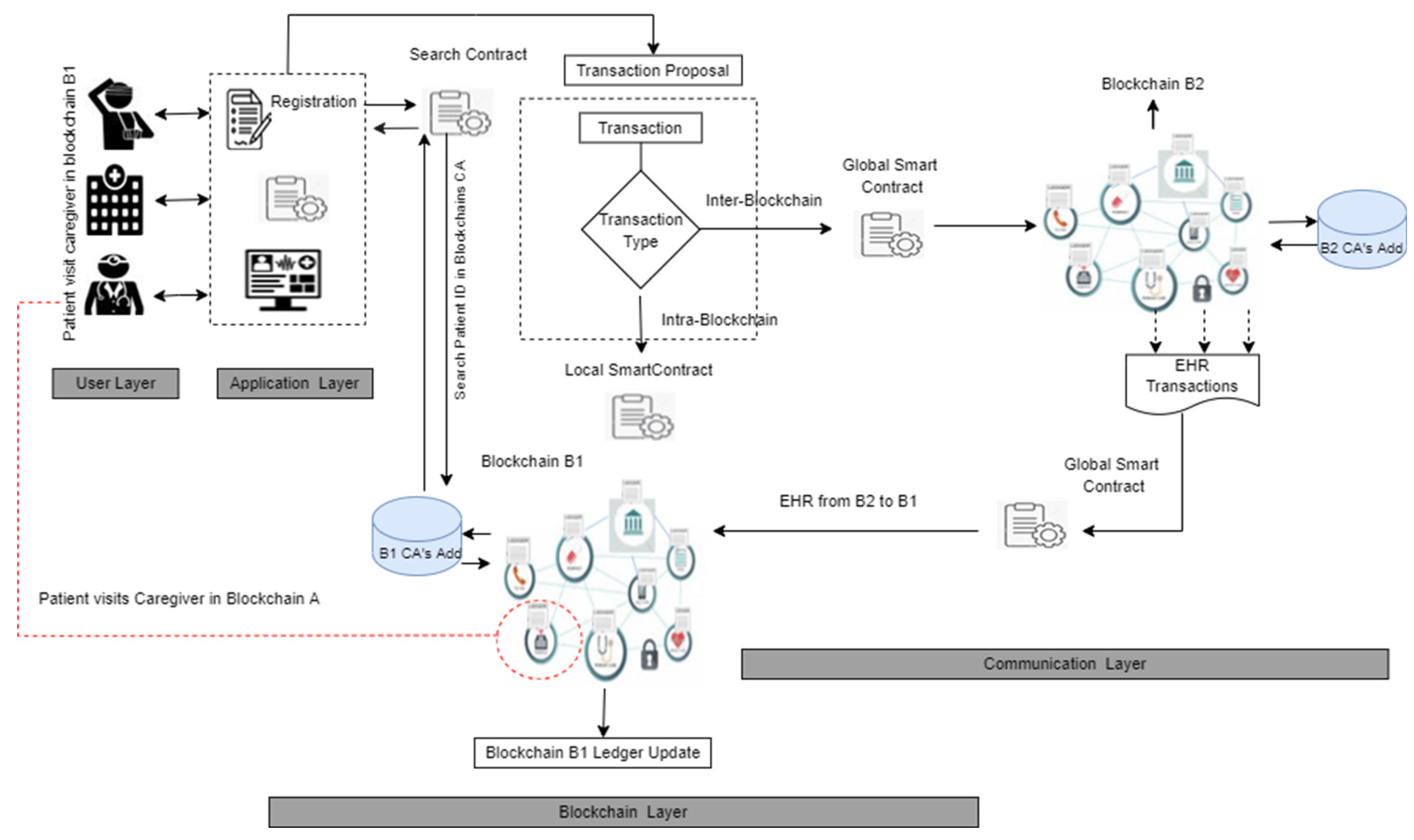
3. Methods
3.1. User Layer
3.2. Application Layer
3.3. Blockchain Layer
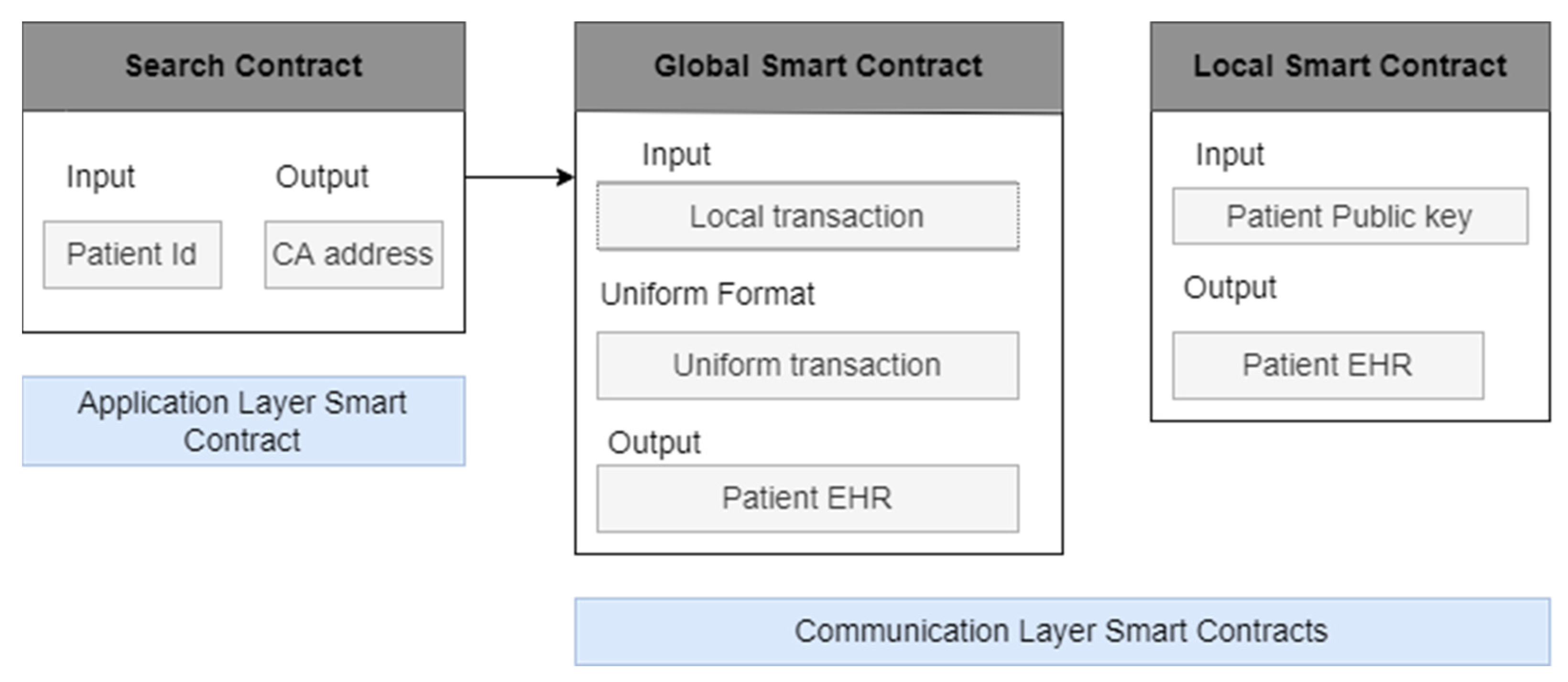
3.3.1. Smart Contracts
3.3.2. Decentralized Off-Chain Storage
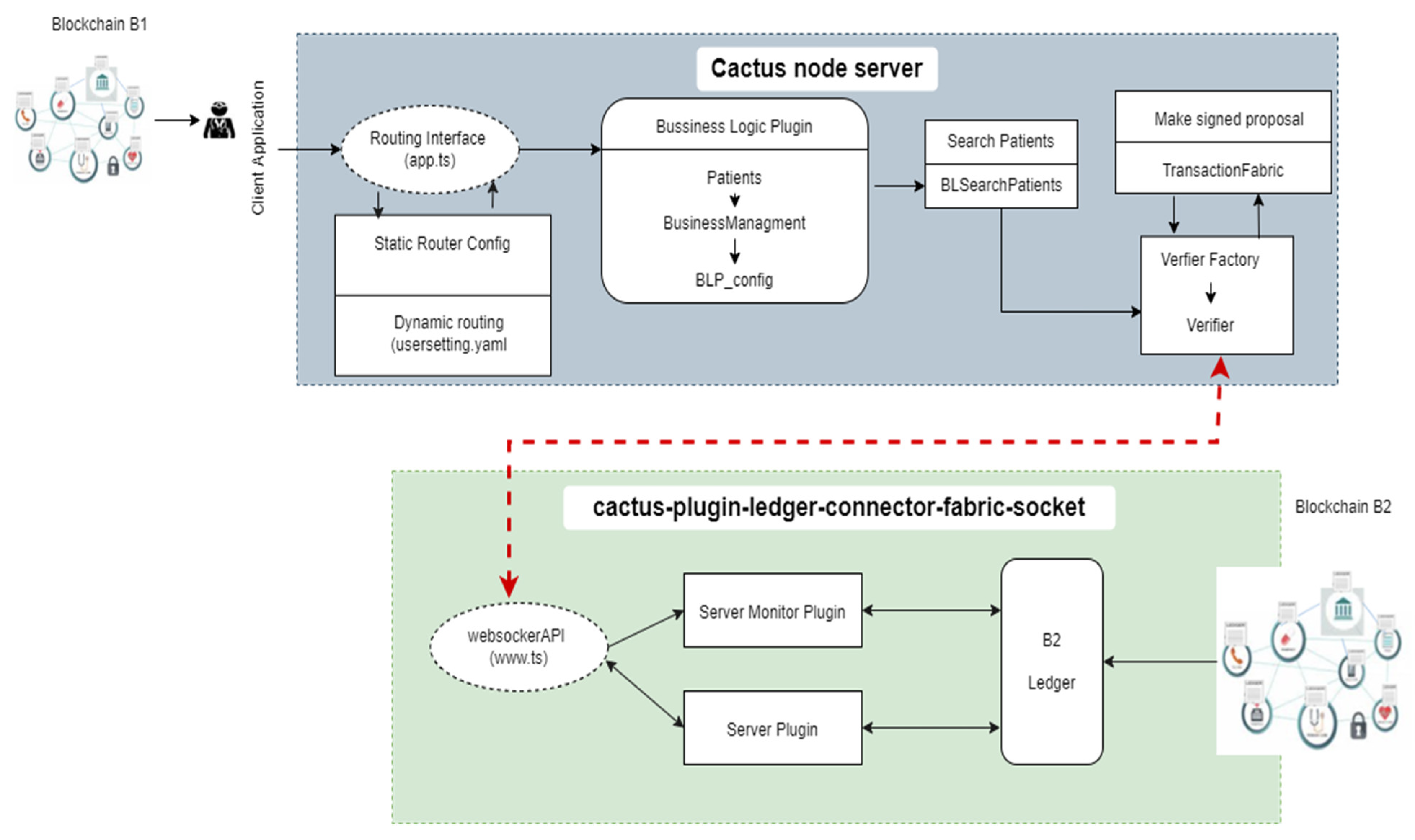
3.4. Communication Layer
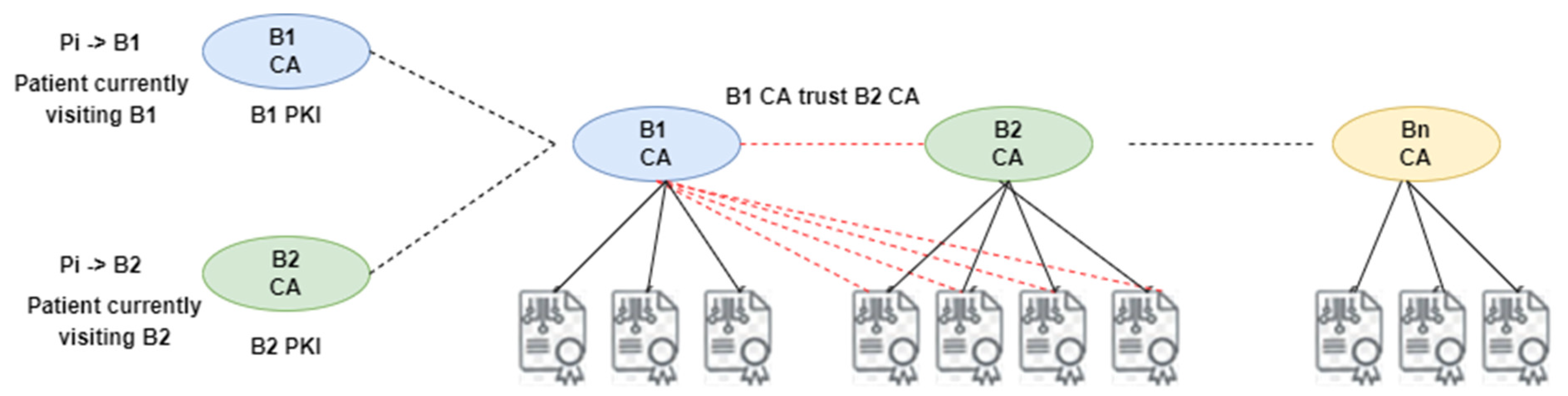
3.4.1. CA Chain
3.4.2. Patient Record Retrieval
| Algorithm 1. Patient Electronic Health Record Retrieval |
| 1. Smartcontract: DataRequest (Pid) |
| 2. DataRequest (Pid) # Pid = Patient id |
| 3. if (msg.sender = Authorized BN) then |
| 4. Ppk ← Pid |
| 5. Search (Ppk) |
| 6. if Ppk == found then |
| 7. return (PR) #PR = Patient Record |
| 8. else |
| 9. AbbortSession |
| 10. end if |
| 11. end if |
| 12. PR → CGpk.Encrypt |
| 13. E(PR) → IPFS |
| 14. IPFS → H(E < PR >) |
| 15. H(E < PR >) → Trans |
| 16. Trans → broadcast |
| Algorithm 2. Inter-Blockchain Communication |
| Patient Pi visits Healthcare Professional Di in blockchain Bi having EHR in blockchain Bj |
| 1. Di issue transaction ⟨Tran type, PID, DPK, C_form, S_CAADD, R_CAADD, TS, DS ⟩ inBi |
| 2. Bi nodes validate Tran |
| 3. Wait for {Tran} from Bj |
| 4. if (Tran type == inter blockchain) then |
| 5. Trigger GS # Global Smart Contract |
| 6. Procedure Request _Connection (S_CAADD, R_CAADD) |
| 7. Create connection S_CAADD → R_CAADD |
| 8. Procedure Request Transaction (Tran, S_CAADD, R_CAADD) |
| 9. Procedure Request Transaction (Tran, S_CAADD, R_CAADD) |
| 10 end if |
| 11. CA_Bj Validate Tran |
| 12. if (Tran ==TRUE) then |
| 13. Tran → < Tran + query> |
| 14. end if |
| 15. CA_Bj ⟨ Tran ⟩ →Bj Nodes |
| 16. Procedure Searchrecord (Tran, Bj Nodes) |
| 17. Each node in Bj search (PID in PR) |
| 18. if (PID found) then |
| 19. Issue Tran ⟨Tran type, PID, S_CAADD, R_CAADD, Hash(EHR), TS, DS, Ack> |
| 20. end if |
| 21. Bj Nodes validate Tran |
| 22. if (Tran type == inter blockchain) then |
| 23. Trigger GS |
| 24. if (Query == Ack) then |
| 25. Procedure Transfer Tran (Tran, R_CAADD) |
| 26. end if |
| 27. end if |
| 28. ∀Tran →Tran pool of Bi |
| 29. Wait = NULL |
| 30. Di adds Tran to block |
| 31. Procedure Consensus (block, Bi nodes) |
| 32. Consensus protocol |
| 33. Update ledger Bi |
| 34. Appointment = NULL |
4. Performance Evaluation
4.1. Evaluation Metrics
4.2. Experimental Environment (The Source Code of the Implementation Used in this Paper Will Be Provided by the First Author upon Request)
4.2.1. Hardware Environment
- 2 Core CPU (Intel (R) Core ™ i5-4570 CPU @ 3.20 GHz);
- 8 GB RAM;
- Ubuntu OS (version 20.04.1 (TS)).
4.2.2. Software Environment
- Hyperledger Fabric V2.x;
- Git 2.9+;
- Python 2.7.x;
- Npm V 5.x;
- Docker Engine 17.037;
- Docker Compose 1.8+;
- VS code;
- Hyperledger Caliper;
- Hyperledger Cactus.
5. Experimental Results and Discussion
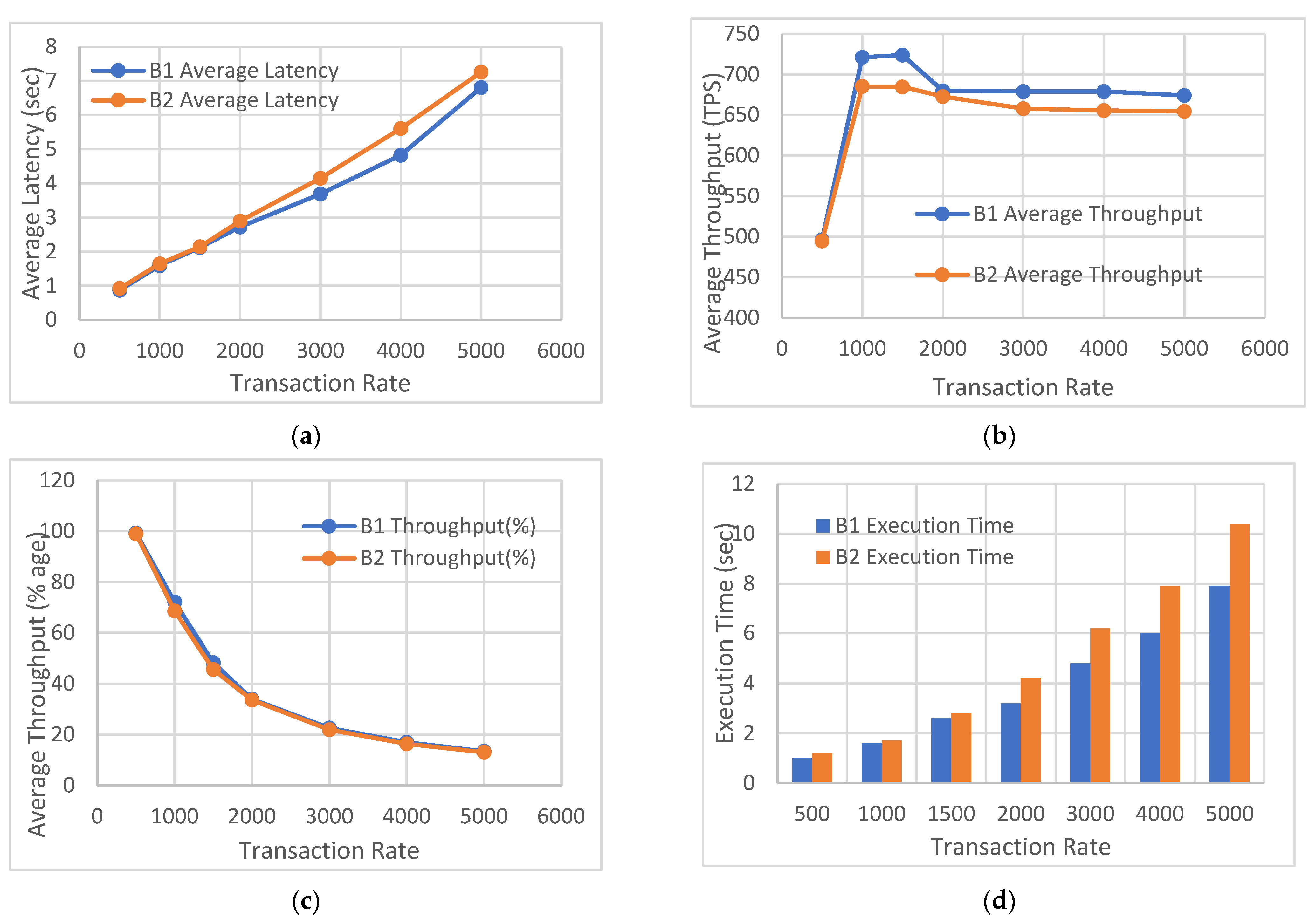
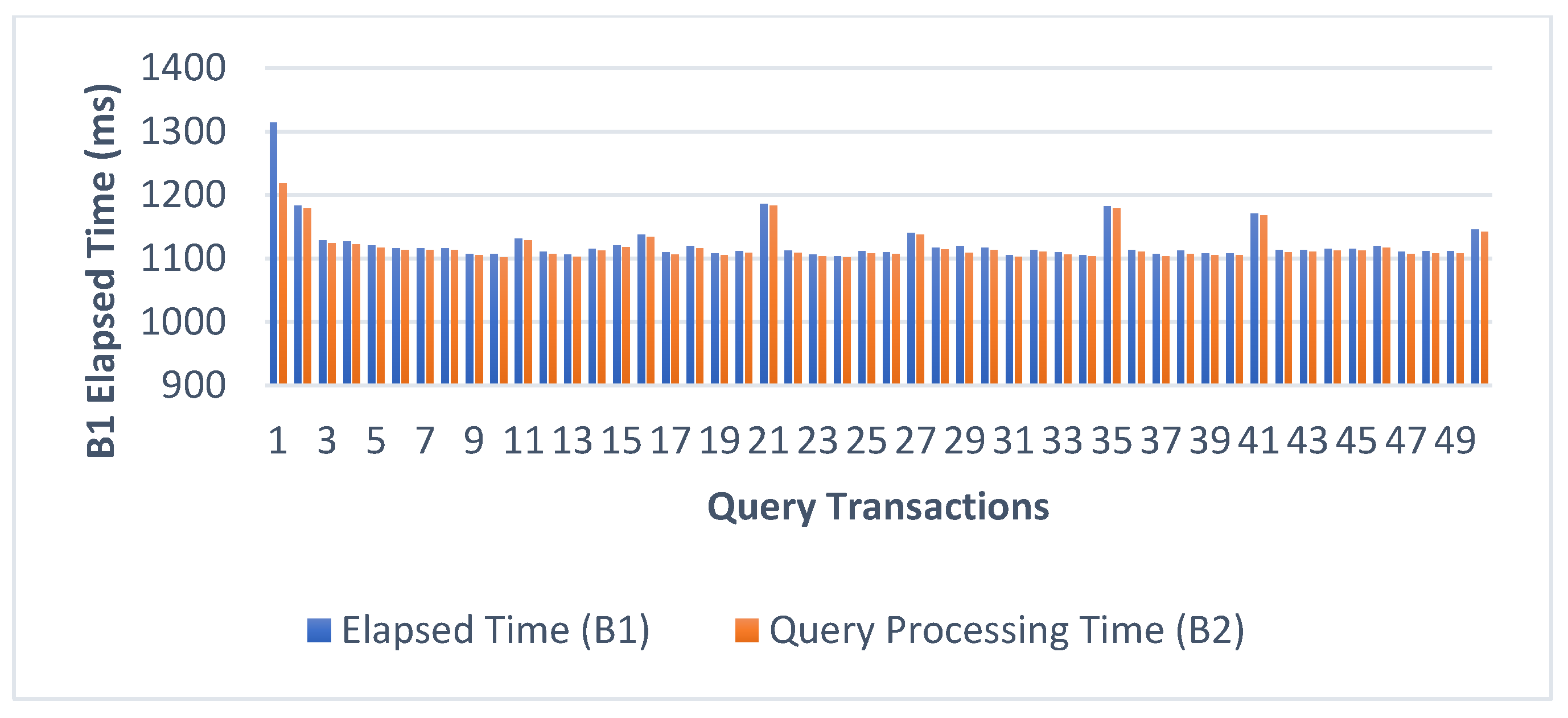
5.1. Peak Performance
5.2. Scalability Performance
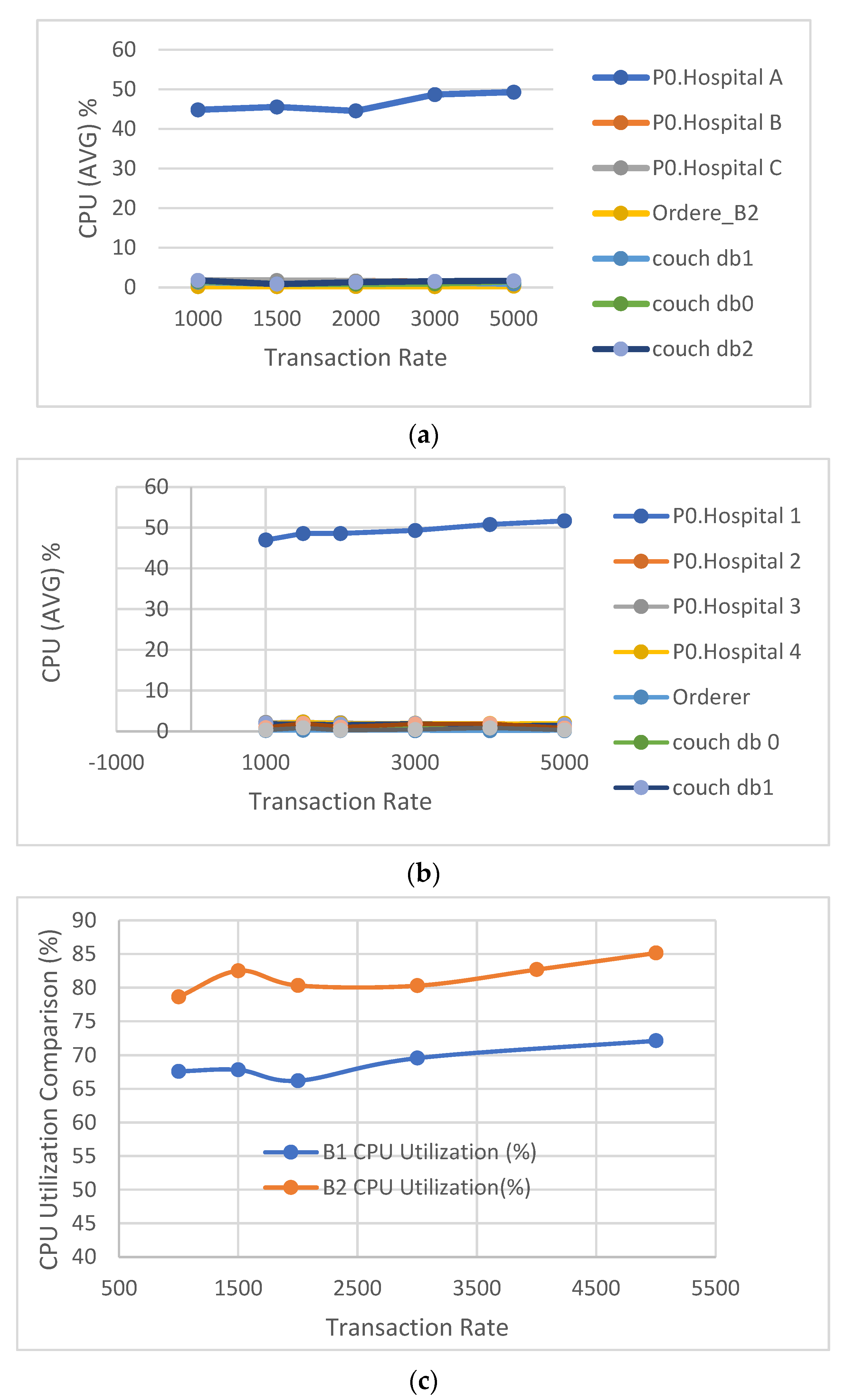
5.3. CPU Utilization
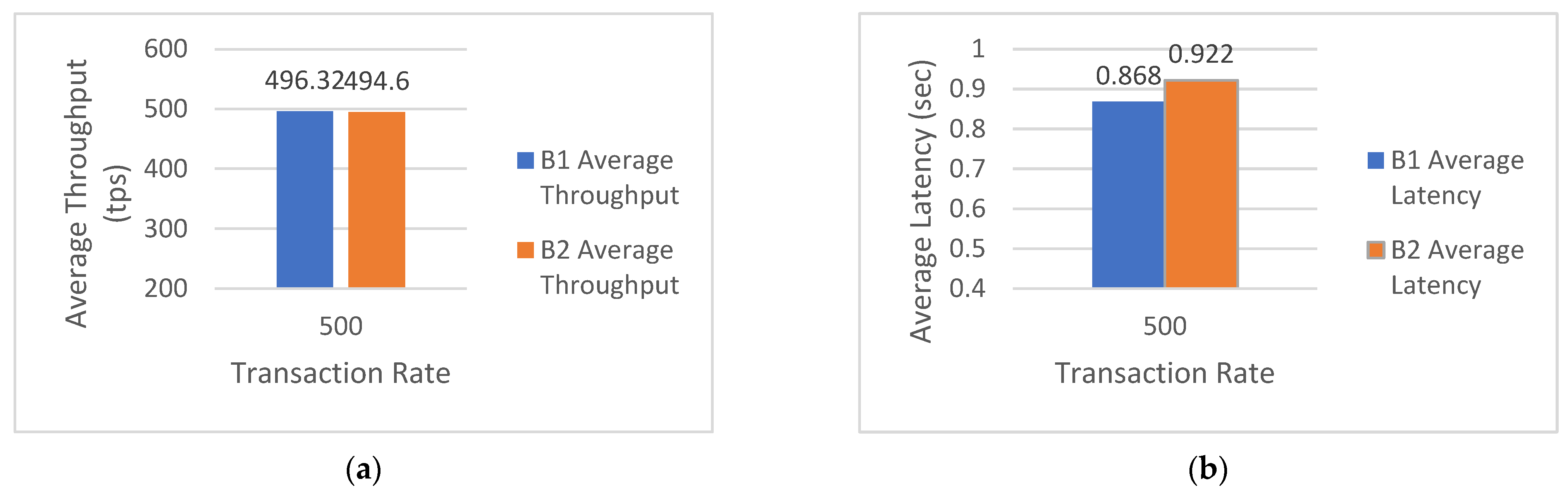
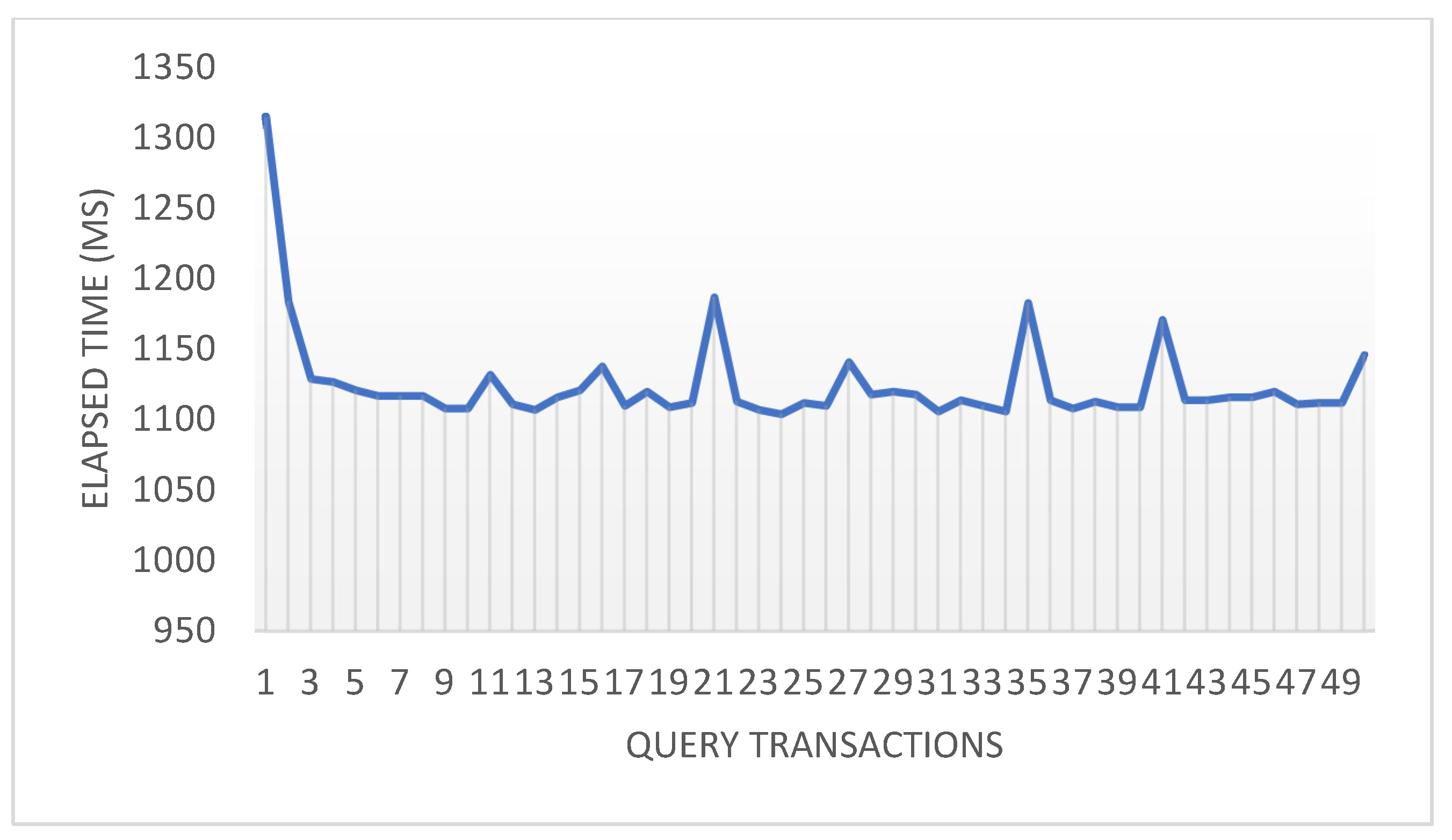
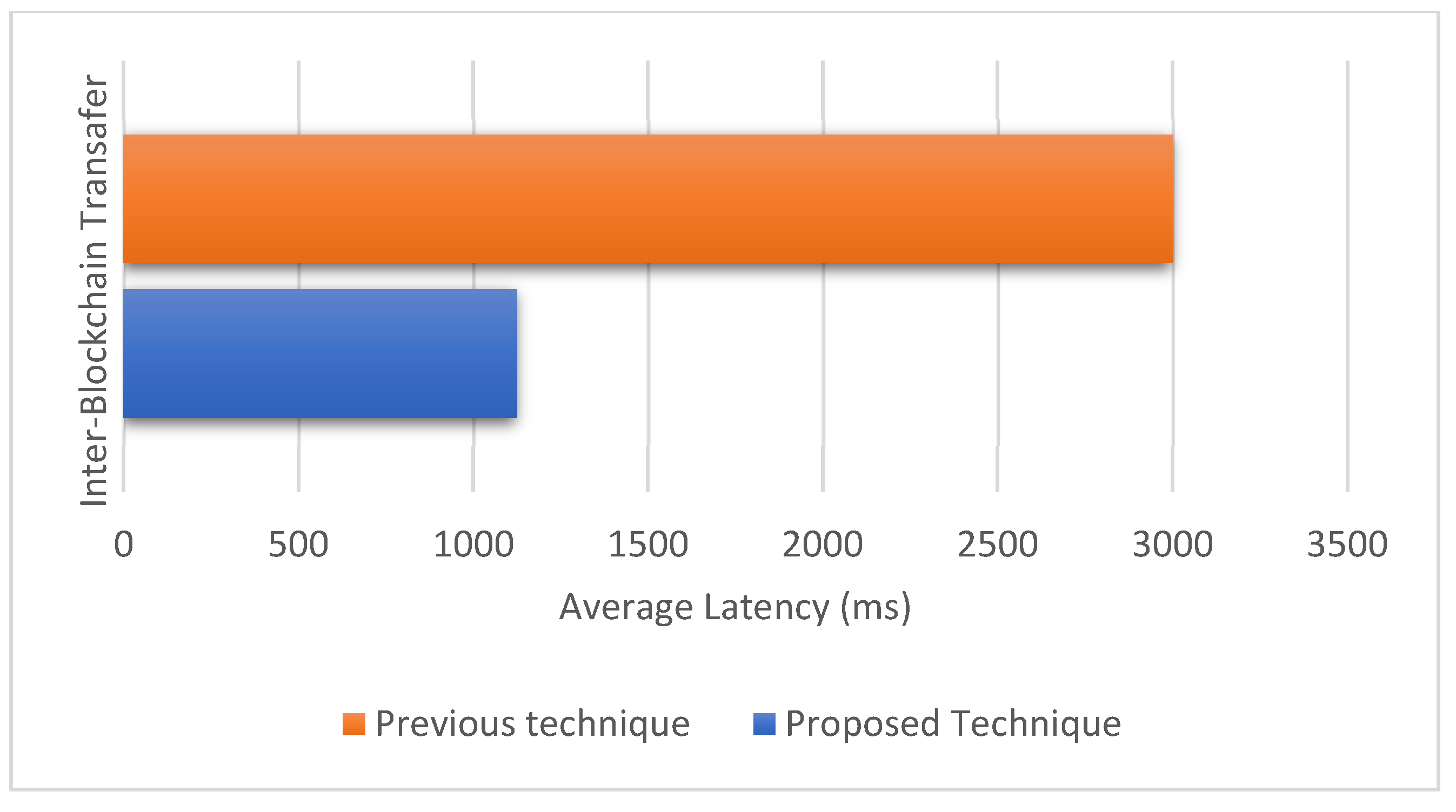
5.4. Inter-Blockchain Communication Performance
Average Latency Comparison
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Jamoom, E.W.; Yang, N.; Hin, E. Adoption of Certified Electronic Health Record Systems and Electronic Information Sharing in Physician Offices: United States, 2013 and 2014. NCHS Data Brief 2016, 236, 1–8. [Google Scholar]
- Uddin, M.; Memon, M.S.; Memon, I.; Ali, I.; Memon, J.; Abdelhaq, M.; Alsaqour, R. Hyperledger Fabric Blockchain: Secure and Efficient Solution for Electronic Health Records. Comput. Mater. Contin. 2021, 68, 2377–2397. [Google Scholar] [CrossRef]
- Rouhani, S. MediChain TM: A Secure Decentralized Medical Data Asset Management System. In Proceedings of the 2018 IEEE International Conference on Internet of Things (iThings) and IEEE Green Computing and Communications (GreenCom) and IEEE Cyber, Physical and Social Computing (CPSCom) and IEEE Smart Data (SmartData), Halifax, NS, Canada, 30 July–3 August 2018; No. Section II. pp. 1533–1538. [Google Scholar]
- Tanwar, S.; Parekh, K.; Evans, R. Blockchain-based electronic healthcare record system for healthcare 4.0 applications. J. Inf. Secur. Appl. 2019, 50, 102407. [Google Scholar] [CrossRef]
- Al-Karaki, J.N.; Gawanmeh, A.; Ayache, M.; Mashaleh, A. DASS-CARE: A decentralized, accessible, scalable, and secure healthcare framework using blockchain. In Proceedings of the 2019 15th International Wireless Communications & Mobile Computing Conference (IWCMC), Tangier, Morocco, 24–28 June 2019; pp. 330–335. [Google Scholar] [CrossRef]
- McGhin, T.; Choo, K.-K.R.; Liu, C.Z.; He, D. Blockchain in healthcare applications: Research challenges and opportunities. J. Netw. Comput. Appl. 2019, 135, 62–75. [Google Scholar] [CrossRef]
- Shuaib, K.; Abdella, J.; Sallabi, F.; Serhani, M.A. Secure decentralized electronic health records sharing system based on blockchains. J. King Saud Univ. Comput. Inf. Sci. 2022, 34, 5045–5058. [Google Scholar] [CrossRef]
- Fan, K.; Wang, S.; Ren, Y.; Li, H.; Yang, Y. MedBlock: Efficient and Secure Medical Data Sharing Via Blockchain. J. Med. Syst. 2018, 42, 136. [Google Scholar] [CrossRef]
- Azaria, A.; Ekblaw, A.; Vieira, T.; Lippman, A. MedRec: Using Blockchain for Medical Data Access and Permission Management. In Proceedings of the 2016 2nd International Conference on Open and Big Data (OBD), Vienna, Austria, 22–24 August 2016; pp. 25–30. [Google Scholar] [CrossRef]
- Li, H.; Zhu, L.; Shen, M.; Gao, F.; Tao, X.; Liu, S. Blockchain-Based Data Preservation System for Medical Data. J. Med. Syst. 2018, 42, 141. [Google Scholar] [CrossRef]
- Zghaibeh, M.; Farooq, U.; Hassan, N.U.; Baig, I. SHealth: A Blockchain-Based Health System With Smart Contracts Capabilities. IEEE Access 2020, 8, 70030–70043. [Google Scholar] [CrossRef]
- Hashim, F.; Shuaib, K.; Sallabi, F. MedShard: Electronic Health Record Sharing Using Blockchain Sharding. Sustainability 2021, 13, 5889. [Google Scholar] [CrossRef]
- Milojkovic, M. Privacy-Preserving Framework for Access Control and Interoperability of Electronic Health Records Using Blockchain Technology. Showcase of Undergraduate Research and Creative Endeavors, April 2018, United States, [Online]. Available online: https://digitalcommons.winthrop.edu/source/SOURCE_2018/posterpresentations/64 (accessed on 15 June 2022).
- Fatokun, T.; Nag, A.; Sharma, S. Towards a Blockchain Assisted Patient Owned System for Electronic Health Records. Electronics 2021, 10, 580. [Google Scholar] [CrossRef]
- Fallis, A. Rootstock Platform: Bitcoin Powered Smart Contracts—White Paper. J. Chem. Inf. Model. 2015, 53, 1689–1699. [Google Scholar]
- Back, A.; Corallo, M.; Dashjr, L.; Friedenbach, M.; Maxwell, G.; Miller, A.; Poelstra, A.; Timón, J.; Wuille, P. Enabling Blockchain Innovations with Pegged Sidechains. 2014. Volume 72, pp. 201–224. Available online: http://www.opensciencereview.com/papers/123/enablingblockchain-innovations-with-pegged-sidechains (accessed on 21 May 2022).
- Poon, J.; Buterin, V. Plasma: Scalable Autonomous Smart Contracts. White Paper, 2017, pp. 1–47. [Online]. Available online: https://plasma.io/ (accessed on 15 June 2022).
- Wang, H.; Cen, Y.; Li, X. Blockchain router: A cross-chain communication protocol. In Proceedings of the 6th International Conference on Informatics, Environment, Energy and Applications, Jeju Island, Korea, 29–31 March 2017; pp. 94–97. [Google Scholar] [CrossRef]
- Chen, Z.D.; Zhuo, Y.; Duan, Z.B.; Kai, H. Inter-Blockchain Communication. DEStech Trans. Comput. Sci. Eng. 2017, 448–454. [Google Scholar] [CrossRef]
- Kan, L.; Wei, Y.; Muhammad, A.H.; Siyuan, W.; Linchao, G.; Kai, H. A Multiple Blockchains Architecture on Inter-Blockchain Communication. In Proceedings of the 2018 IEEE International Conference on Software Quality, Reliability and Security Companion (QRS-C), Lisbon, Portugal, 16–20 July 2018; pp. 139–145. [Google Scholar] [CrossRef]
- Fynn, E.; Bessani, A.; Pedone, F. Smart Contracts on the Move. In Proceedings of the 50th Annual IEEE/IFIP International Conference on Dependable Syst Networks, Valencia, Spain, 1 June 2020; pp. 233–244. [Google Scholar]
- Dagher, G.G.; Adhikari, C.L.; Enderson, T. Towards Secure Interoperability between Heterogeneous Blockchains using Smart Contracts. In Proceedings of the Future Technologies Conference (FTC), Vancouver, BC, Canada, 29–30 November 2017; pp. 73–81. [Google Scholar]
- Bennink, P.; Gijtenbeek, L.V.; Deventer, O.V.; Everts, M. An Analysis of Atomic Swaps on and between Ethereum Blockchains Using Smart Contracts; Technical Report; 11 Feb 2018. Available online: https://rp.os3.nl/2017-2018/p42/report.pdf (accessed on 19 April 2022).
- Nakamoto, S. Bitcoin: A Peer-to-Peer Electronic Cash System, Decentralized Bussines Review 2009, p. 21260. [Online]. Available online: www.bitcoin.org (accessed on 6 July 2022).
- Sumathi, M.; Sangeetha, S. Blockchain Based Sensitive Attribute Storage and Access Monitoring in Banking System. Int. J. Cloud Appl. Comput. 2020, 10, 77–92. [Google Scholar] [CrossRef]
- Osmani, M.; El-Haddadeh, R.; Hindi, N.; Janssen, M.; Weerakkody, V. Blockchain for next generation services in banking and finance: Cost, benefit, risk and opportunity analysis. J. Enterp. Inf. Manag 2021, 34, 884–899. [Google Scholar] [CrossRef]
- Ravi, D.; Ramachandran, S.; Vignesh, R.; Falmari, V.R.; Brindha, M. Privacy preserving transparent supply chain management through Hyperledger Fabric. Blockchain Res. Appl. 2022, 3, 100072. [Google Scholar] [CrossRef]
- Queiroz, M.M.; Telles, R.; Bonilla, S.H. Blockchain and supply chain management integration: A systematic review of the literature. Supply Chain Manag. Int. J. 2019, 25, 241–254. [Google Scholar] [CrossRef]
- Panarello, A.; Tapas, N.; Merlino, G.; Longo, F.; Puliafito, A. Blockchain and IoT Integration: A Systematic Survey. Sensors 2018, 18, 2575. [Google Scholar] [CrossRef]
- Yetis, R.; Sahingoz, O.K. Blockchain based secure communication for IoT devices in smart cities. In Proceedings of the 7th International Istanbul Smart Grids and Cities Cong. and Fair (ICSG), Istanbul, Turkey, 25–26 April 2019; Available online: https://ieeexplore.ieee.org/abstract/document/8782285/ (accessed on 6 July 2022).
- Hashim, F.; Shuaib, K.; Sallabi, F. Performance Evaluation of Blockchain Consensus Algorithms for Electronic Health Record Sharing. In Proceedings of the 2021 Global Congress on Electrical Engineering (GC-ElecEng), Valencia, Spain, 10–12 December 2021; pp. 136–143. [Google Scholar] [CrossRef]
- Hölbl, M.; Kompara, M.; Kamišalić, A.; Nemec Zlatolas, L. A Systematic Review of the Use of Blockchain in Healthcare. Symmetry 2018, 10, 470. [Google Scholar] [CrossRef]
- Hasselgren, A.; Kralevska, K.; Gligoroski, D.; Pedersen, S.A.; Faxvaag, A. Blockchain in healthcare and health sciences—A scoping review. Int. J. Med. Inform. 2019, 134, 104040. [Google Scholar] [CrossRef]
- Mohan, A.P.; Gladston, A. Merkle Tree and Blockchain-Based Cloud Data Auditing. Int. J. Cloud Appl. Comput. 2020, 10, 54–66. [Google Scholar] [CrossRef]
- Gai, K.; Guo, J.; Zhu, L.; Yu, S. Blockchain Meets Cloud Computing: A Survey. IEEE Commun. Surv. Tutor. 2020, 22, 2009–2030. [Google Scholar] [CrossRef]
- Qasse, I.A.; Talib, M.A.; Nasir, Q. Inter blockchain communication: A survey. In Proceedings of the ArabiWIC 6th Annual International Conference Research Track, Rabat, Morocco, 7–9 March 2019. [Google Scholar] [CrossRef]
- Singh, A.; Click, K.; Parizi, R.M.; Zhang, Q.; Dehghantanha, A.; Choo, K.-K.R. Sidechain technologies in blockchain networks: An examination and state-of-the-art review. J. Netw. Comput. Appl. 2019, 149, 102471. [Google Scholar] [CrossRef]
- Li, W.; Sforzin, A.; Fedorov, S.; Karame, G.O. Towards Scalable and Private Industrial Blockchains. In Proceedings of the ACM Workshop on Blockchain, Cryptocurrencies and Contracts, Abu Dhabi, United Arab Emirates, 2–6 April 2017; ACM: New York, NY, USA, 2017; pp. 9–14. [Google Scholar] [CrossRef]
- Deng, L.; Chen, H.; Zeng, J.; Zhang, L.J. Research on cross-chain technology based on sidechain and hash-locking. Lect. Notes Comput. Sci. 2018, 10973, 144–151. [Google Scholar] [CrossRef]
- Donawa, A.; Orukari, I.; Baker, C.E. Scaling Blockchains to Support Electronic Health Records for Hospital Systems. In Proceedings of the 2019 IEEE 10th Annual Ubiquitous Computing, Electronics & Mobile Communication Conference (UEMCON), New York, NY, USA, 10–12 October 2019; pp. 0550–0556. [Google Scholar] [CrossRef]
- Belchior, R.; Vasconcelos, A.; Guerreiro, S.; Correia, M. A Survey on Blockchain Interoperability: Past, Present, and Future Trends. ACM Comput. Surv. 2021, 54, 168. [Google Scholar] [CrossRef]
- Ding, D.; Duan, T.; Jia, L.; Li, K.; Li, Z.; Sun, Y. InterChain: A Framework to Support Blockchain Interoperability. Second Asia Pacific Work. Netw. 2018, [Online]. Available online: https://icowhitepapers.co/wp-content/uploads/ (accessed on 15 June 2022).
- Borkowski, M.; Sigwart, M.; Frauenthaler, P.; Hukkinen, T.; Schulte, S. Dextt: Deterministic Cross-Blockchain Token Transfers. IEEE Access 2019, 7, 111030–111042. [Google Scholar] [CrossRef]
- Polk, W.T.; Hastings, N.E.; Polk, W.T. Bridge Certification Authorities: Connecting B2B Public Key Infrastructures. In PKI Forum Meeting Proceedings; 2000; pp. 27–79. Available online: https://csrc.nist.rip/groups/ST/crypto_apps_infra/documents/B2B-article.pdf (accessed on 25 April 2022).
- De Angelis, S.; Aniello, L.; Baldoni, R.; Lombardi, F.; Margheri, A.; Sassone, V. PBFT vs Proof-of-Authority: Applying the CAP Theorem to Permissioned Blockchain. In Proceedings of the 2018 Italian Conference on Cyber Security, Milan, Italy, 6–9 February 2018. [Google Scholar]
- Tseng, L. Recent results on fault-tolerant consensus in message-passing networks. Lect. Notes Comput. Sci. 2016, 9988, 92–108. [Google Scholar] [CrossRef]
- Castro, M.; Liskov, B. Practical byzantine fault tolerance and proactive recovery. ACM Trans. Comput. Syst. 2002, 20, 398–461. [Google Scholar] [CrossRef]
- Al Asad, N.; Elahi, M.T.; al Hasan, A.; Yousuf, M.A. Permission-based blockchain with proof of authority for secured healthcare data sharing. In Proceedings of the 2020 2nd International Conference on Advanced Information and Communication Technology (ICAICT), Dhaka, Bangladesh, 28–29 November 2020; pp. 35–40. [Google Scholar] [CrossRef]
- A Blockchain Platform for the Enterprise—Hyperledger-Fabricdocs Main Documentation. Available online: https://hyperledger-fabric.readthedocs.io/en/release-2.2/ (accessed on 15 January 2022).
- Antwi, M.; Adnane, A.; Ahmad, F.; Hussain, R.; Rehman, M.H.U.; Kerrache, C.A. The case of HyperLedger Fabric as a blockchain solution for healthcare applications. Blockchain Res. Appl. 2021, 2, 100012. [Google Scholar] [CrossRef]
- Pajooh, H.H.; Rashid, M.; Alam, F.; Demidenko, S. Hyperledger Fabric Blockchain for Securing the Edge Internet of Things. Sensors 2021, 21, 359. [Google Scholar] [CrossRef]
- Figueroa-Lorenzo, S.; Benito, J.A.; Arrizabalaga, S. Modbus Access Control System Based on SSI over Hyperledger Fabric Blockchain. Sensors 2021, 21, 5438. [Google Scholar] [CrossRef]
- Podda, A.S.; Pompianu, L. An overview of blockchain-based systems and smart contracts for digital coupons. In Proceedings of the 2020 IEEE/ACM 42nd International Conference on Software Engineering Work ICSEW, Seoul, Korea, 27 June–19 July 2020; Volume 20, pp. 770–778. [Google Scholar] [CrossRef]
- Getting Started | Hyperledger Caliper. Available online: https://hyperledger.github.io/caliper/v0.4.2/getting-started/ (accessed on 20 February 2022).
- Hyperledger Cactus: On the Road to General Blockchain Integration—Hyperledger Foundation. Available online: https://www.hyperledger.org/blog/2021/03/31/hyperledger-cactus-on-the-road-to-general-blockchain-integration (accessed on 15 March 2022).
- Bellavista, P.; Esposito, C.; Foschini, L.; Giannelli, C.; Mazzocca, N.; Montanari, R. Interoperable Blockchains for Highly-Integrated Supply Chains in Collaborative Manufacturing. Sensors 2021, 21, 4955. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index | Consensus | Features (+/−) | Solution Type | Shortcomings of the Solution |
|---|---|---|---|---|
| [15] | PoW | (+) Works as sidechain pegged to bitcoin. Faster transaction validation, lower transaction fee. (−) Mining is performed on the main chain, completely dependent on the main chain for the mining process. | Side chain solution | Supports 1–1 communication among sidechains and main chain. Focus on homogenous blockchains. Higher computational cost and complex Sidechain blockchains cannot operate independently. |
| [17] | PoS | (+) Each sidechain has its own independent rules and constraints. (−) Mining is performed on the main chain, completely dependent on the main chain for the mining process. | ||
| [38] | Heterogeneous consensus algorithms | (+) Sidechains use independent consensus algorithms. Maintains private ledger, which provides faster block generation. (−) The private ledger is not shared with all participants. | ||
| [39] | (+) Uses a federated two-way peg mechanism, provides increased security to the funds transferred among sidechains and main chain. (−) The federated two-way peg mechanism increases the transaction validation time. | |||
| [18] | Delegated Stake-PBFT | (+) Provides communication among heterogeneous blockchains. Can dynamically add blockchain routers. (−) Communication via blockchain router only. One-point failure issue can compromise communication. | Blockchain router solution | Design and frameworks available but are not yet implemented. The configuration of blockchain node needs to be changed to function as router node. One-point failure issue. Communication is affected as the router node fails or compromised. |
| [19] | PBFT | (+) Different blockchain systems communicate without any intermediaries. Using ANN-router-based network architecture, a part of the blockchain can function as router, however, configuration details of such setup are required. (−) The connection mechanism is not provided. Based on each blockchain topology, throughput is affected. Implementation details are missing. | ||
| [20] | (+) Created a dynamic blockchain network called router blockchain, which includes router nodes from each blockchain. (−) One-point failure issue due to communication via a single node. The configuration setting of router node is not provided. | |||
| [22] | PoS | (+) Smart contract-based interoperability solution between independent blockchains (public and private) without intermediaries. (−) The authors did not apply their solution between two hybrid networks. | Smart contract solutions | Available solutions operate in homogeneous blockchains. Smart contract solutions in infancy and implementations not available. Smart contract sharing not available. |
| [43] | (+) Cross-blockchain data transfer, smart contract interaction, currency transfer. Transfer same kind of token any number of blockchain simultaneously. (−) Proposed protocol operates in same environment only among homogeneous blockchains. | |||
| [23] | (+) A cross-chain atomic swap is used for assets transfer across multiple participants between multiple Ethereum blockchains. (−) Need to implement atomic swaps on and with other blockchains. |
| Parameters | Configuration |
|---|---|
| Workers | 5 |
| Test Duration | 50 sec |
| Rounds | 5 |
| Transaction Load per Round | 500, 1000, 1500, 2000, 3000, 4000, 5000 |
| Transactions Mode | Read |
| Network Size | 3 Healthcare entities, 6 peers/4 Healthcare entities, 8 peers |
| Varied Factor | Block time |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hashim, F.; Shuaib, K.; Sallabi, F. Connected Blockchain Federations for Sharing Electronic Health Records. Cryptography 2022, 6, 47. https://doi.org/10.3390/cryptography6030047
Hashim F, Shuaib K, Sallabi F. Connected Blockchain Federations for Sharing Electronic Health Records. Cryptography. 2022; 6(3):47. https://doi.org/10.3390/cryptography6030047
Chicago/Turabian StyleHashim, Faiza, Khaled Shuaib, and Farag Sallabi. 2022. "Connected Blockchain Federations for Sharing Electronic Health Records" Cryptography 6, no. 3: 47. https://doi.org/10.3390/cryptography6030047