
Diagnostic Accuracy and Reliability of Noncontrast Computed Tomography Markers for Acute Hematoma Expansion among Radiologists
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
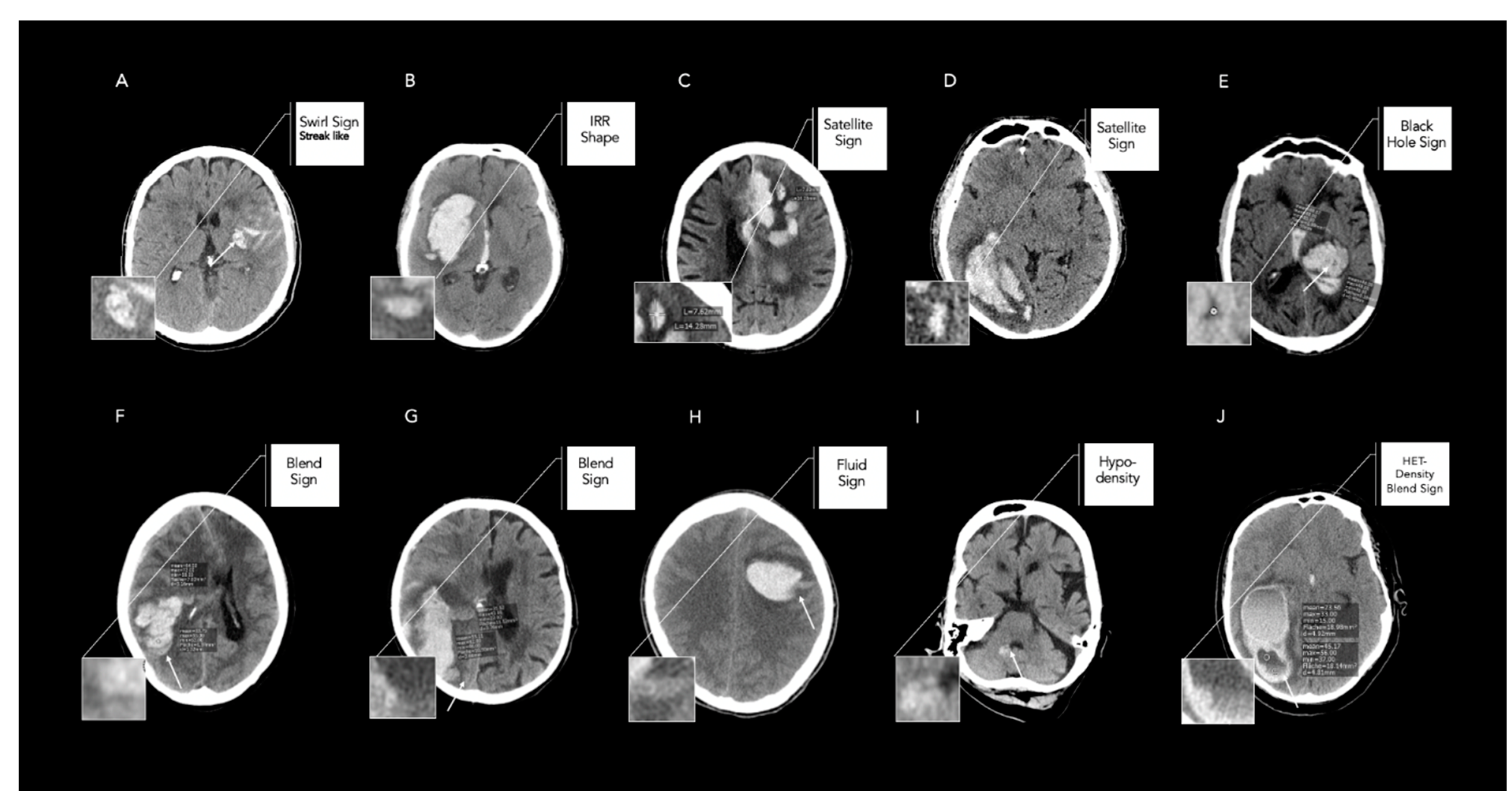
2.2. Image Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van Asch, C.J.; Luitse, M.J.; Rinkel, G.J.; van der Tweel, I.; Algra, A.; Klijn, C.J. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: A systematic review and meta-analysis. Lancet Neurol. 2010, 9, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Dowlatshahi, D.; Demchuk, A.M.; Flaherty, M.L.; Ali, M.; Lyden, P.L.; Smith, E.E.; On behalf of the VISTA Collaboration. Defining hematoma expansion in intracerebral hemorrhage: Relationship with patient outcomes. Neurology 2011, 76, 1238–1244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morotti, A.; Arba, F.; Boulouis, G.; Charidimou, A. Noncontrast CT markers of intracerebral hemorrhage expansion and poor outcome: A meta-analysis. Neurology 2020, 95, 632–643. [Google Scholar] [CrossRef] [PubMed]
- Morotti, A.; Dowlatshahi, D.; Boulouis, G.; Al-Ajlan, F.; Demchuk, A.M.; Aviv, R.I.; Yu, L.; Schwab, K.; Romero, J.M.; Gurol, M.E.; et al. Predicting Intracerebral Hemorrhage Expansion with Noncontrast Computed Tomography. Stroke 2018, 49, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Morotti, A.; Boulouis, G.; Dowlatshahi, D.; Li, Q.; Barras, C.D.; Delcourt, C.; Yu, Z.; Zheng, J.; Zhou, Z.; Aviv, R.I.; et al. Standards for Detecting, Interpreting, and Reporting Noncontrast Computed Tomographic Markers of Intracerebral Hemorrhage Expansion. Ann. Neurol. 2019, 86, 480–492. [Google Scholar] [CrossRef]
- Nawabi, J.; Elsayed, S.; Kniep, H.; Sporns, P.; Schlunk, F.; McDonough, R.; Broocks, G.; Dührsen, L.; Schön, G.; Götz, T.; et al. Inter- and Intrarater Agreement of Spot Sign and Noncontrast CT Markers for Early Intracerebral Hemorrhage Expansion. J. Clin. Med. 2020, 9, 1020. [Google Scholar] [CrossRef] [Green Version]
- Dowlatshahi, D.; Morotti, A.; Al-Ajlan, F.S.; Boulouis, G.; Warren, A.D.; Petrcich, W.; Aviv, R.I.; Demchuk, A.M.; Goldstein, J.N.; PREDICT Collaboration and the MGH Hemorrhagic Stroke Research Program. Interrater and Intrarater Measurement Reliability of Noncontrast Computed Tomography Predictors of Intracerebral Hemorrhage Expansion. Stroke 2019, 50, 1260–1262. [Google Scholar] [CrossRef]
- Falcone, G.J.; Biffi, A.; Brouwers, H.B.; Anderson, C.D.; Battey, T.W.K.; Ayres, A.; Vashkevich, A.; Schwab, K.; Rost, N.S.; Goldstein, J.N.; et al. Predictors of Hematoma Volume in Deep and Lobar Supratentorial Intracerebral Hemorrhage. JAMA Neurol. 2013, 70, 988. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Wang, X.; Anderson, C.S.; Robinson, T.; Lavados, P.M.; Lindley, R.I.; Chalmers, J.; Delcourt, C.; for the INTERACT Investigators. Infratentorial Intracerebral Hemorrhage. Stroke 2019, 50, 1257–1259. [Google Scholar] [CrossRef]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef]
- Mishra, M.; Shukla, P.; Bodhit, A.; Asaithambi, G.; Velez, A.; Rosado, C.; Mishra, M.; Saravanapavan, P.; Khan, S.; Reddy, V.; et al. Intracerebral Hematoma Volume Measurement Using ITK-SNAP Software: Initial Experience (P7.145). Neurology 2014, 82, P7.145. [Google Scholar]
- Yang, W.; Zhang, S.; Shen, Y.; Wei, X.; Zhao, L.; Xie, X.; Deng, L.; Li, X.; Lv, X.; Lv, F.; et al. Noncontrast Computed Tomography Markers as Predictors of Revised Hematoma Expansion in Acute Intracerebral Hemorrhage. J. Am. Heart Assoc. 2021, 10, e018248. [Google Scholar] [CrossRef]
- Barras, C.D.; Tress, B.M.; Christensen, S.; MacGregor, L.; Collins, M.; Desmond, P.M.; Skolnick, B.E.; Mayer, S.A.; Broderick, J.P.; Diringer, M.N.; et al. Density and Shape as CT Predictors of Intracerebral Hemorrhage Growth. Stroke 2009, 40, 1325–1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, Z.; Zheng, J.; Ali, H.; Guo, R.; Li, M.; Wang, X.; Ma, L.; Li, H.; You, C. Significance of satellite sign and spot sign in predicting hematoma expansion in spontaneous intracerebral hemorrhage. Clin. Neurol. Neurosurg. 2017, 162, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Liu, Q.J.; Yang, W.S.; Wang, X.C.; Zhao, L.B.; Xiong, X.; Li, R.; Cao, D.; Zhu, D.; Wei, X.; et al. Island sign: An imaging predictor for early hematoma expansion and poor outcome in patients with intracerebral hemorrhage. Stroke 2017, 48, 3019–3025. [Google Scholar] [CrossRef]
- Selariu, E.; Zia, E.; Brizzi, M.; Abul-Kasim, K. Swirl sign in intracerebral haemorrhage: Definition, prevalence, reliability and prognostic value. BMC Neurol. 2012, 12, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, X.; Li, Q.; Yang, W.-S.; Wei, X.; Hu, X.; Wang, X.-C.; Zhu, D.; Li, R.; Cao, D.; Xie, P. Comparison of Swirl Sign and Black Hole Sign in Predicting Early Hematoma Growth in Patients with Spontaneous Intracerebral Hemorrhage. Med. Sci. Monit. 2018, 24, 567–573. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Zhang, G.; Xiong, X.; Wang, X.C.; Yang, W.S.; Li, K.W.; Wei, X.; Xie, P. Black hole sign: Novel imaging marker that predicts hematoma growth in patients with intracerebral hemorrhage. Stroke 2016, 47, 1777–1781. [Google Scholar] [CrossRef] [Green Version]
- Sporns, P.B.; Schwake, M.; Kemmling, A.; Minnerup, J.; Schwindt, W.; Niederstadt, T.; Schmidt, R.; Hanning, U. Comparison of Spot Sign, Blend Sign and Black Hole Sign for Outcome Prediction in Patients with Intracerebral Hemorrhage. J. Stroke 2017, 19, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Zhang, G.; Huang, Y.-J.; Dong, M.-X.; Lv, F.-J.; Wei, X.; Chen, J.-J.; Zhang, L.-J.; Qin, X.-Y.; Xie, P. Blend Sign on Computed Tomography. Stroke 2015, 46, 2119–2123. [Google Scholar] [CrossRef] [Green Version]
- Seo, J.-S.; Nam, T.-K.; Kwon, J.-T.; Park, Y.-S. Multiple Spontaneous Simultaneous Intracerebral Hemorrhages. J. Cerebrovasc. Endovasc. Neurosurg. 2014, 16, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlunk, F.; Kuthe, J.; Harmel, P.; Audebert, H.; Hanning, U.; Bohner, G.; Scheel, M.; Kleine, J.; Nawabi, J. Volumetric accuracy of different imaging modalities in acute intracerebral hemorrhage. BMC Med. Imaging 2022, 22, 9. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- Delong, E.R.; Delong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Nehme, A.; Ducroux, C.; Panzini, M.-A.; Bard, C.; Bereznyakova, O.; Boisseau, W.; Deschaintre, Y.; Diestro, J.D.B.; Guilbert, F.; Jacquin, G.; et al. Non-contrast CT markers of intracerebral hematoma expansion: A reliability study. Eur. Radiol. 2022, 32, 6126–6135. [Google Scholar] [CrossRef]


{kind=link}
| Baseline Characteristics | All (n = 735) |
|---|---|
| Age [years], median (IQR) | 73 (62–80) |
| Female, n (%) | 410 (56.9) |
| Systolic RR [mmHg], median (IQR) | 165 (145–195) |
| Hypertension, n (%) | 581 (80.7) |
| Diabetes mellitus, n (%) | 121 (16.6) |
| Anticoagulation Treatment, n (%) | 201 (27.9) |
| Antiplatelet Treatment, n (%) | 324 (45.0) |
| GCS admission, median (IQR) | 13 (9–15) |
| Δ symptom onset to imaging [h], median (IQR) | 6.23 (1.65–17.55) |
| Craniotomy, n (%) | 116 (16.11) |
| Hemorrhage Characteristics | |
| ICH Volume on admission [mL], mean (SD) | 44.56 (5.99) |
| ICH Volume on follow-up [mL], mean (SD) | 60.86 (16.42) |
| Intraventricular hemorrhage on admission, n (%) | 327 (45.42) |
| Intraventricular hemorrhage on follow-up, n (%) | 363 (50.4) |
| HE [>6 mL; >33%], n (%) | 150 (20.8) |
| revised HE [HE; IVH growth], n (%) | 271 (37.7) |
| Location characteristics | |
| Supratentorial, n (%) | 615 (85.4) |
| Lobar, n (%) | 309 (43) |
| Basal ganglia, n (%) | 306 (42.6) |
| Thalamic, n (%) | 36 (5.7) |
| Brainstem/pons, n (%) | 69 (9.6) |
| Cerebellar, n (%) | 35 (4.9) |
| Clinical Outcome | |
| mRS 0–3, n (%) | 190 (26.39) |
| mRS 4–6, n (%) | 530 (73.61) |
| mRS 6 (mortality), n (%) | 188 (26.10) |
| NCCT Marker (n = 735) | Neuroradiology Fellow | Radiology Resident | Radiology Fellow | p-Value |
|---|---|---|---|---|
| Shape Markers | ||||
| IRR Shape, n (%) | 467 (63.54) | 466 (63.40) | 469 (63.81) | <0.001 |
| Satellite Sign, n (%) | 300 (40.82) | 285 (38.78) | 311 (42.31) | <0.001 |
| Island Sign, n (%) | 347 (47.21) | 328 (44.63) | 298 (40.54) | <0.001 |
| Density Markers | ||||
| HET Density, n (%) | 191 (25.99) | 162 (22.05) | 177 (24.08) | <0.001 |
| Swirl Sign, n (%) | 488 (66.39) | 475 (64.63) | 529 (71.97) | <0.001 |
| Black Hole Sign, n (%) | 192 (26.12) | 175 (23.81) | 148 (20.14) | <0.001 |
| Blend Sign, n (%) | 81 (11.02) | 79 (10.75) | 75 (10.220) | <0.001 |
| Fluid Sign, n (%) | 49 (6.67) | 46 (6.26) | 43 (5.85) | <0.001 |
| Hypodensities, n (%) | 325 (44.22) | 356 (48.44) | 296 (36.60) | <0.001 |
| NCCT Marker | Rater | Cohen’s Kappa (95% CI) | Rater | Fleiss Kappa (95% CI) |
|---|---|---|---|---|
| Shape Markers | ||||
| IRR Shape | Rad Resident and Neurorad Fellow | 0.88 (0.85–0.92) | Rad Resident, Rad Fellow, and Neurorad Fellow | 0.90 (0.86–0.94) |
| Rad Fellow and Neurorad Fellow | 0.94 (0.92–0.97) | |||
| Satellite Sign | Rad Resident and Neurorad Fellow | 0.94 (0.91–0.96) | Rad Resident, Rad Fellow, and Neurorad Fellow | 0.80 (0.76–0.84) |
| Rad Fellow and Neurorad Fellow | 0.86 (0.78–0.93) | |||
| Island Sign | Rad Resident and Neurorad Fellow | 0.95 (0.92–0.97) | Rad Resident, Rad Fellow, and Neurorad Fellow | 0.86 (0.82–0.91) |
| Rad Fellow and Neurorad Fellow | 0.78 (0.71–0.84) | |||
| Density Markers | ||||
| HET Density | Rad Resident and Neurorad Fellow | 0.85 (0.80–0.89) | Rad Resident, Rad Fellow, and Neurorad Fellow | 0.86 (0.82–0.9) |
| Rad Fellow and Neurorad Fellow | 0.94 (0.91–0.97) | |||
| Swirl Sign | Rad Resident and Neurorad Fellow | 0.96 (0.94–0.98) | Rad Resident, Rad Fellow, and Neurorad Fellow | 0.62 (0.57–0.66) |
| Rad Fellow and Neurorad Fellow | 0.58 (0.52–0.65) | |||
| Black Hole Sign | Rad Resident and Neurorad Fellow | 0.94 (0.91–0.97) | Rad Resident, Rad Fellow, and Neurorad Fellow | 0.79 (0.75–0.84) |
| Rad Fellow and Neurorad Fellow | 0.75 (0.66–0.84) | |||
| Blend Sign | Rad Resident and Neurorad Fellow | 0.70 (0.65–0.81) | Rad Resident, Rad Fellow, and Neurorad Fellow | 0.79 (0.75–0.83) |
| Rad Fellow and Neurorad Fellow | 0.77 (0.67–0.88) | |||
| Fluid Sign | Rad Resident and Neurorad Fellow | 0.96 (0.91–1.00) | Rad Resident, Rad Fellow, and Neurorad Fellow | 0.93 (0.89–0.97) |
| Rad Fellow and Neurorad Fellow | 0.92 (0.86–0.98) | |||
| Hypodensities | Rad Resident and Neurorad Fellow | 0.84 (0.80–0.88) | Rad Resident, Rad Fellow, and Neurorad Fellow | 0.83 (0.79–0.87) |
| Rad Fellow and Neurorad Fellow | 0.83 (0.78–0.87) | |||
| NCCT Marker | Intrarater | Cohen’s Kappa (95% CI) | p-Value |
|---|---|---|---|
| Shape Markers | |||
| IRR Shape | Neurorad Fellow | 0.87 (0.83–0.91) | <0.001 |
| Satellite Sign | Neurorad Fellow | 0.93 (0.88–0.97) | <0.001 |
| Island Sign | Neurorad Fellow | 0.95 (0.90–1.00) | <0.001 |
| Density Markers | |||
| HET Density | Neurorad Fellow | 0.79 (0.73–0.84) | <0.001 |
| Swirl Sign | Neurorad Fellow | 0.94 (0.91–0.98) | <0.001 |
| Black Hole Sign | Neurorad Fellow | 0.98 (0.95–1.00) | <0.001 |
| Blend Sign | Neurorad Fellow | 0.96 (0.90–1.00) | <0.001 |
| Fluid Sign | Neurorad Fellow | 0.95 (0.90–1.00) | <0.001 |
| Hypodensities | Neurorad Fellow | 0.81(0.78–0.86) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almubarak, H.; Elsayed, S.; Mazzacane, F.; Schlunk, F.; Cao, H.; Vu, L.H.; Vogt, E.; Dell Orco, A.; Desser, D.; Böhmer, M.F.H.; et al. Diagnostic Accuracy and Reliability of Noncontrast Computed Tomography Markers for Acute Hematoma Expansion among Radiologists. Tomography 2022, 8, 2893-2901. https://doi.org/10.3390/tomography8060242
Almubarak H, Elsayed S, Mazzacane F, Schlunk F, Cao H, Vu LH, Vogt E, Dell Orco A, Desser D, Böhmer MFH, et al. Diagnostic Accuracy and Reliability of Noncontrast Computed Tomography Markers for Acute Hematoma Expansion among Radiologists. Tomography. 2022; 8(6):2893-2901. https://doi.org/10.3390/tomography8060242
Chicago/Turabian StyleAlmubarak, Hawra, Sarah Elsayed, Federico Mazzacane, Frieder Schlunk, Haoyin Cao, Ly Huong Vu, Estelle Vogt, Andrea Dell Orco, Dmitriy Desser, Maik F. H. Böhmer, and et al. 2022. "Diagnostic Accuracy and Reliability of Noncontrast Computed Tomography Markers for Acute Hematoma Expansion among Radiologists" Tomography 8, no. 6: 2893-2901. https://doi.org/10.3390/tomography8060242