1. Introduction
In December 2019, in the city of Wuhan, China, there was human transmission of a new coronavirus, SARS-CoV-2. A few months later, the World Health Organization (WHO) declared the COVID-19 pandemic, which lasted more than three years with more than 700 million confirmed cases, including more than 6 million deaths, according to data available on the WHO Coronavirus Dashboard [
1]. Despite the WHO officially having declared the end of the COVID-19 pandemic health emergency in May 2023, the virus continues circulating, as happened with the influenza virus. The emergence of new pathogens that cause epidemics and pandemics is recurrent in humanity. In this way, experts suggest that the world should be better prepared to face a new pandemic in the future.
In this context, hospital units deserve great attention due to the pressure exerted on them during pandemic events, as occurred in the case of COVID-19. In order to contain disease spread in these units, numerous internal protocols were created—the use of Personal Protective Equipment (PPE), physical barriers, case mapping, quarantine, and return to work protocols, among others. However, the implementation of these measures was not able to prevent the collapse of the health system in many countries, pointing to a gap.
The rationale behind the present study is represented by the COVID-19 pandemic and its impact on the environmental safety of hospital facilities. The development of new risk assessment tools allowing the prioritization of specific actions is essential for allowing hospital units to cope effectively with pandemic requirements, assuming both the proper care of patients and the health and safety of patients, teams, and surrounding communities.
The main objective of this study is to propose a practical and objective method for assessing the risks of spreading SARS-CoV-2 pathogens in a hospital environment. At this point, it is emphasized that, due to the complexity of the hospital environment, it was necessary to delimit the study area of this research. Thus, a toilet located inside a hospital unit was selected, given its unhealthy and opportunistic aspect for pathogen spread, and because it is a restricted internal space and, in general, poorly ventilated and with a high circulation of people.
The proposed methodology was based on the selection of specific indicators for the studied environment, a toilet, and for the pathogen in question, SARS-CoV-2. Known risk assessment techniques were applied, such as Failure Modes and Effects Analysis (FMEA), Fault Tree Analysis (FTA), Ergonomic Work Analysis (EWA), and Analytic Hierarchy Process (AHP).
3. Materials and Methods
This research adopts a mixed methodological approach, consisting of a qualitative study regarding the identification of environmental, human, and transmission factors related to the spread of SARS-CoV-2. It is also characterized as quantitative because in addition to being identified, these factors are quantified, allowing the creation of the proposed Risk Score. Finally, the research can be classified as diagnostic since a building is analyzed, so that the methodology obtained can be applied in a case study, aiming for validation.
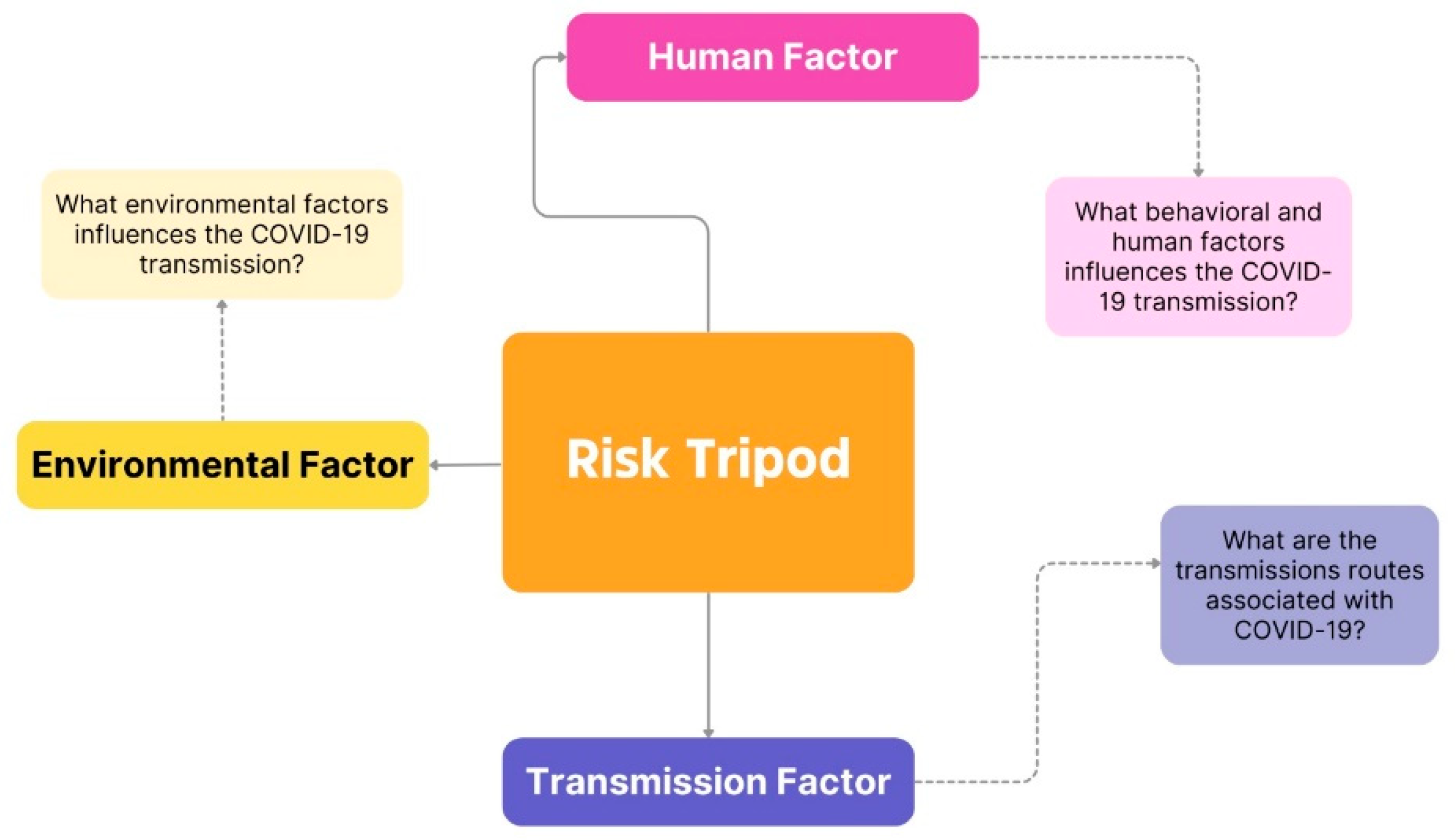
The literature review on SARS-CoV-2 transmission culminated in the identification of the three main influencing factors in the risk analysis, whose interaction can result in the main event of transmission. They are environmental, human, and transmission factors. This association of factors was named the Risk Tripod, as shown in
Figure 1.
Thus, to unravel each of the tripod components, a widely known technique in the health and safety area was selected, as follows:
Environmental factor: Failure Modes and Effects Analysis (FMEA);
Human factor: Ergonomic Work Analysis (EWA);
Transmission factor: Fault Tree Analysis (FTA).
The subsequent sections present the theoretical basis of these techniques and their application in the present study, conducted from September 2022 through to May 2023, for each of the indicated tripod components.
3.1. Environmental Factor: FMEA
For this study, as it is a robust methodology, a simplified FMEA application was chosen, extracting from it only what was considered relevant for the present research, that is, the failure modes related to the environmental factor of the risk tripod and its causes, concerning a hypothetical single toilet located in a hospital facility. The results of the developed FMEA can be explored in
Appendix A. Based on these results, it was possible to identify the risk factors related to the environmental component of the risk tripod. These factors will be classified and each of them will be assigned a score from 1 (one) to 3 (three), from the lowest to the highest risk, respectively, to calculate the risk score.
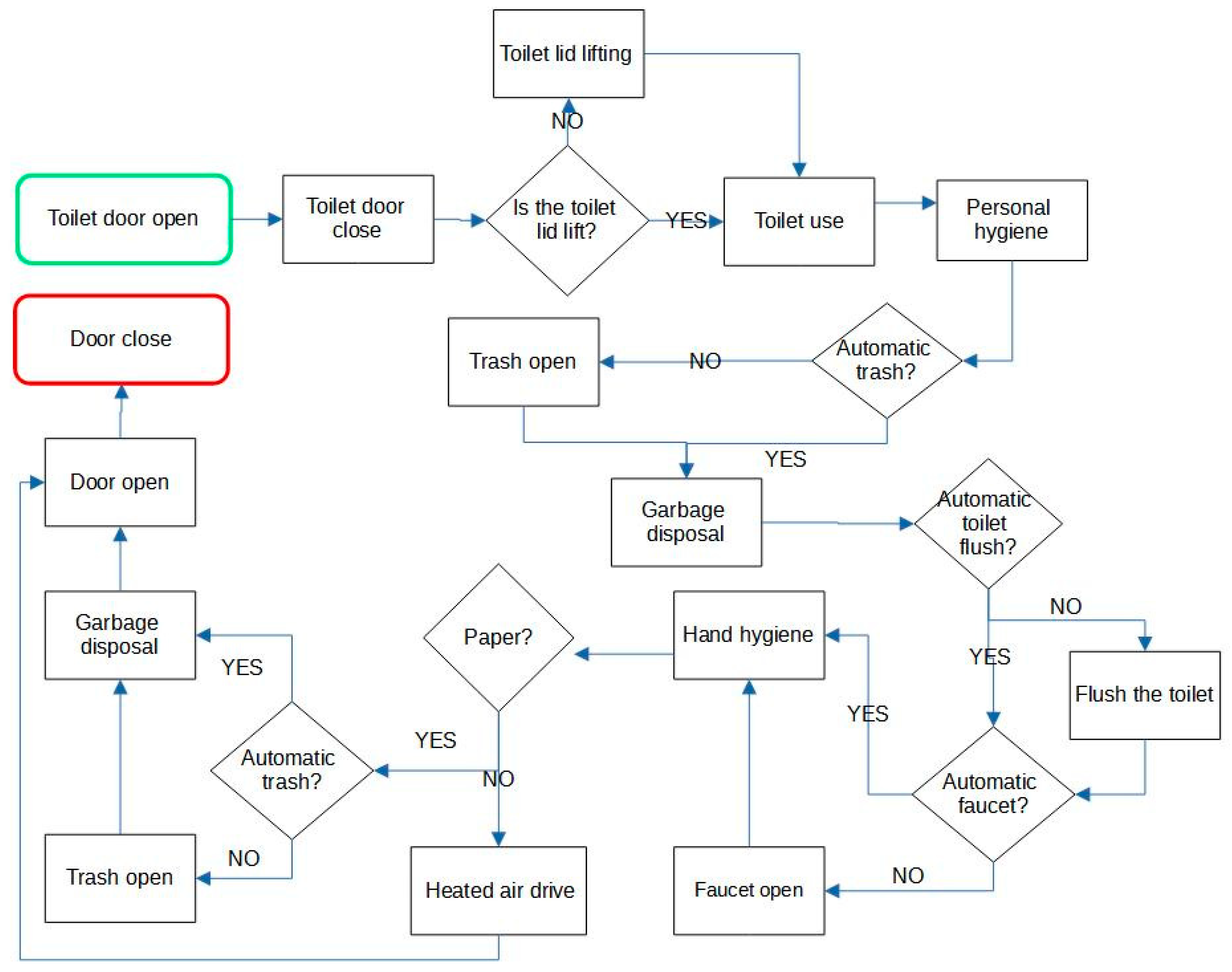
3.2. Human Factor: EWA
The first step for the EWA application in this study was to map the process of using the toilet, as seen in
Figure 2. To assess the human factor, in turn, it was decided to develop a questionnaire with which it was possible to identify risk factors related to human behavior. The questionnaire was prepared based on the process steps previously mapped, and can be accessed in
Appendix B. It is recommended to apply the instrument to different user groups involved in the analyzed environment. Finally, regarding the evaluation of the environment, for the most part, this evaluation was based on the application of the FMEA methodology, as previously seen. However, the EWA application allowed the identification of new environmental indicators that will be considered in the evaluation.
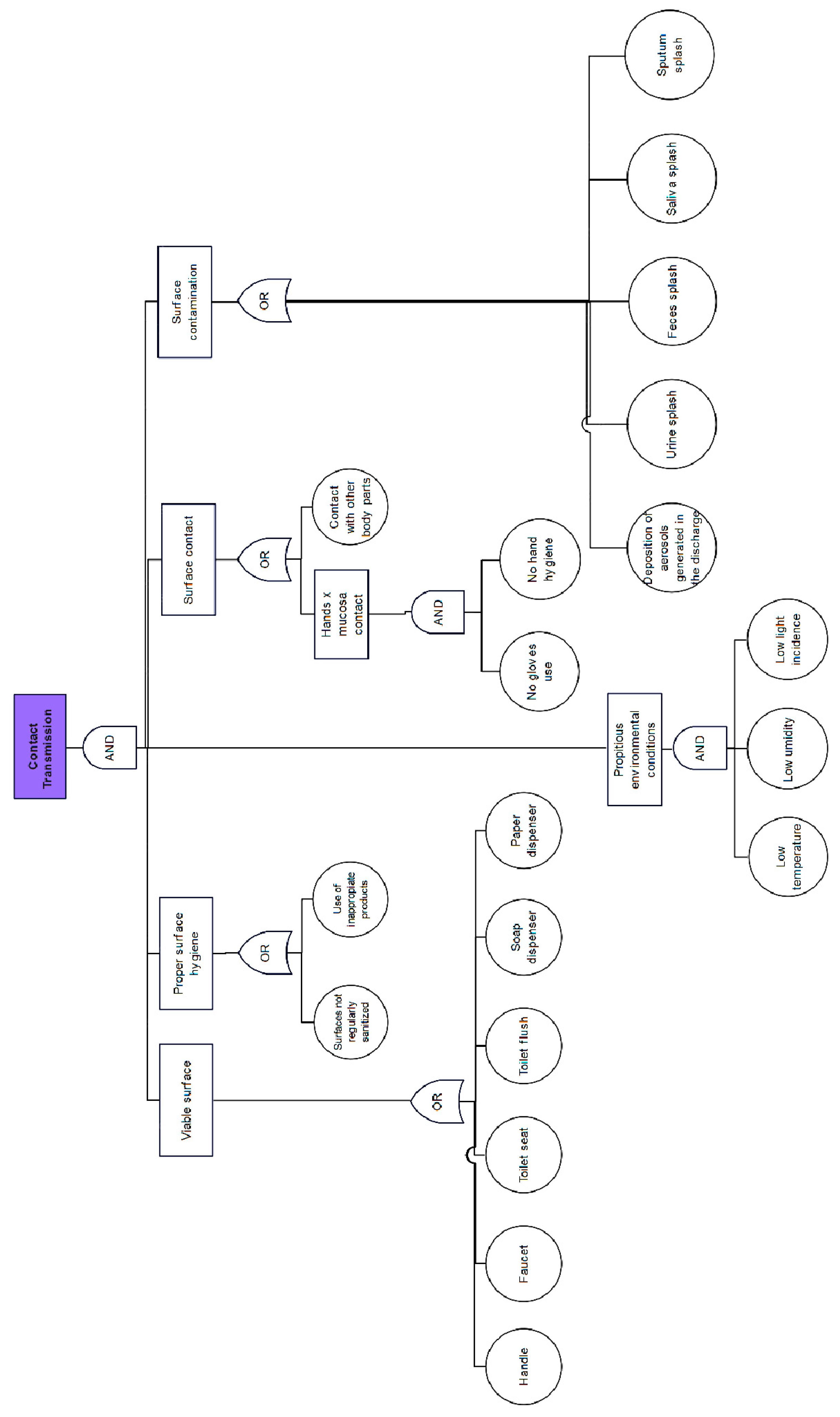
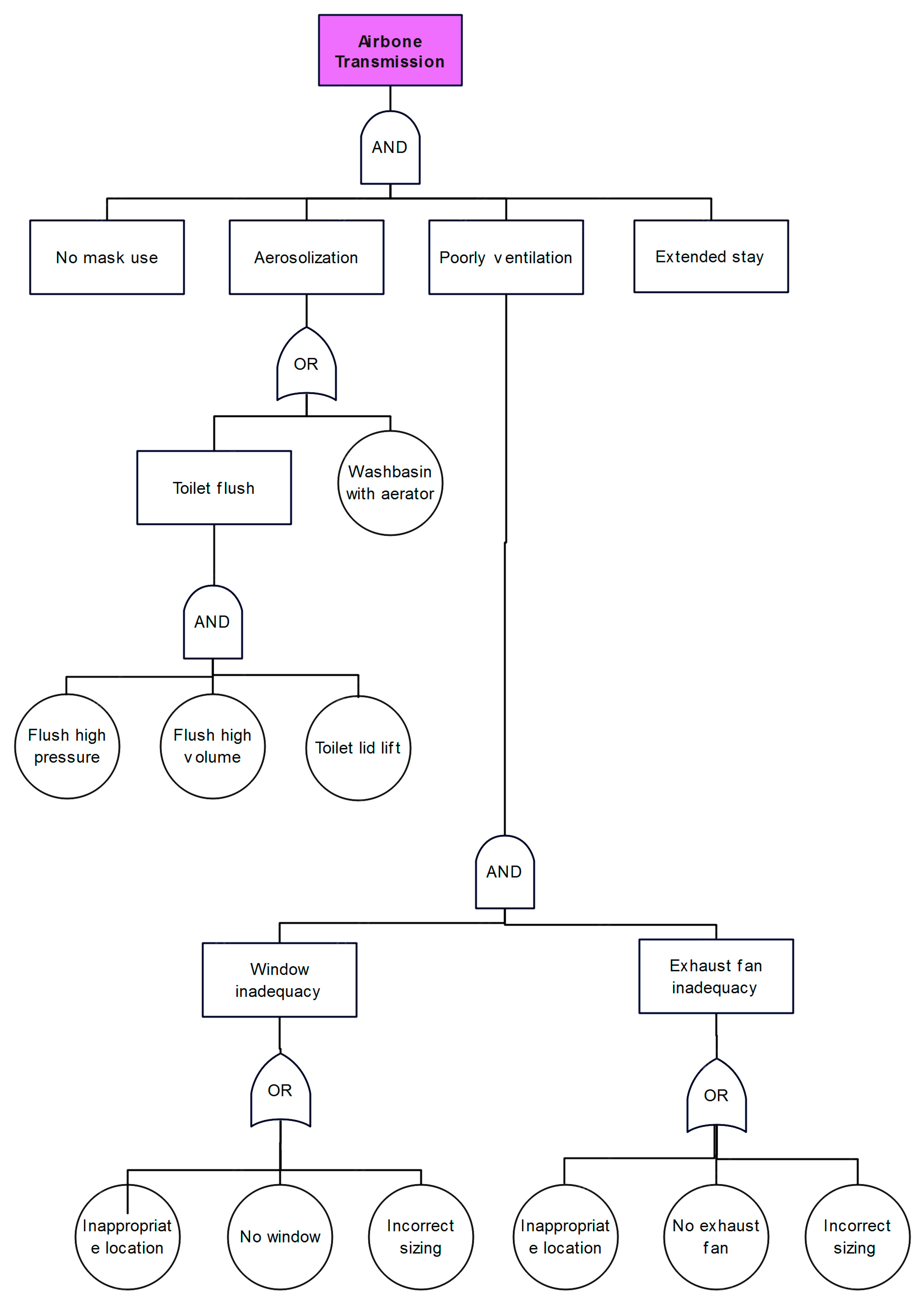
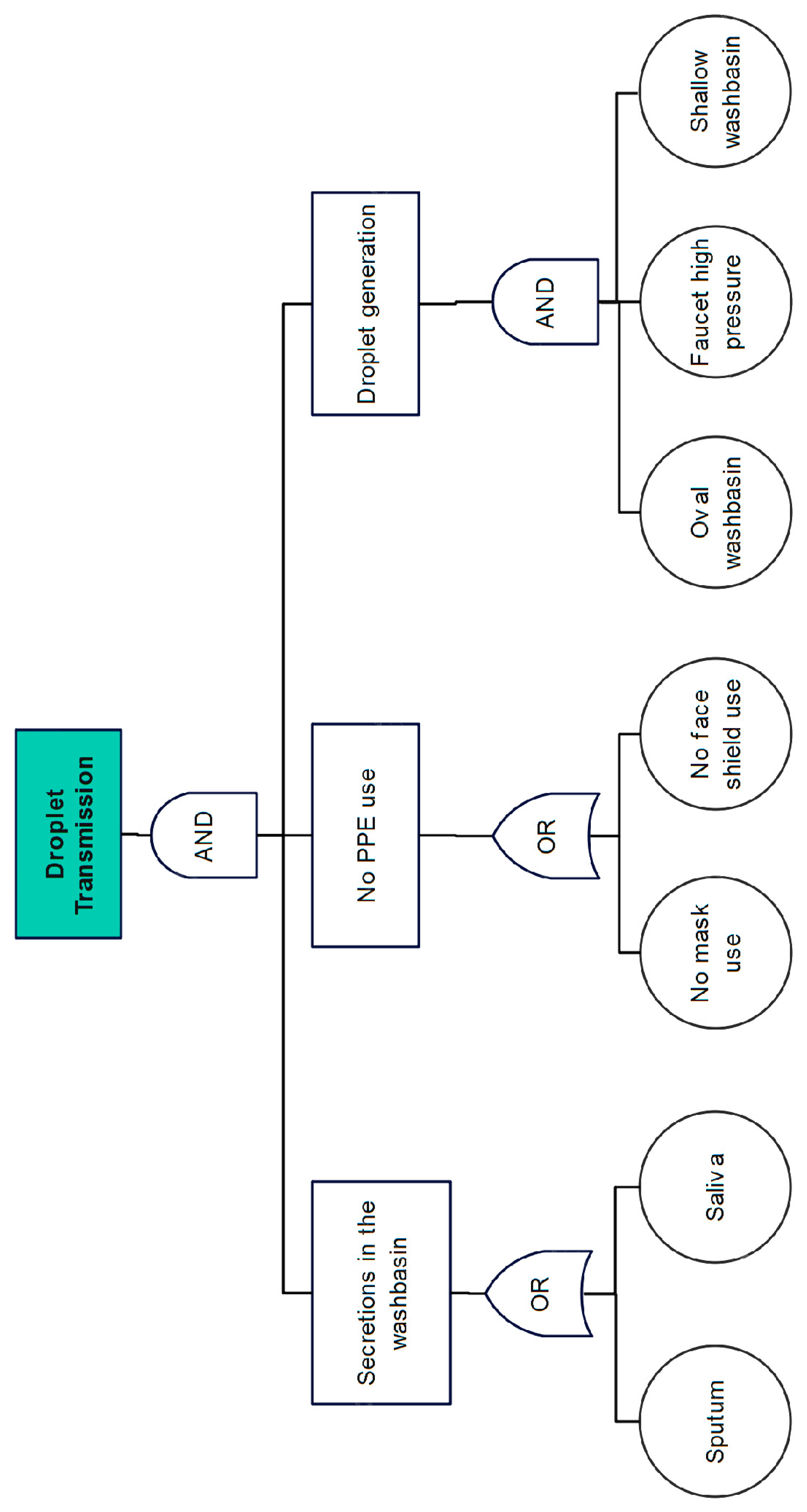
3.3. Transmission Factor: FTA
As previously mentioned, the FTA was applied to the “transmission routes” component of the risk tripod that underlines the methodology of the present study. The bibliographic review on SARS-CoV-2 allowed the identification of the main transmission routes related to the environment of a toilet. In this way, an FTA contemplating all these transmission routes was elaborated, as can be seen in
Appendix C. From the FTA results and fluid dynamics computational simulations, the study concluded that the direct transmission route is the main route of transmission of the virus.
3.4. Indicators for Assessing the Risk of SARS-CoV-2 Transmission in a Toilet
The methodologies used to assess the environmental, human, and transmission factors that constitute the Risk Tripod suggested by the present study provided the identification of relevant indicators for assessing the risk of transmission of SARS-CoV-2 in an individual toilet for common use located in a health unit by FMEA and EWA application, and the main routes acting on these indicators by FTA application.
Table 1 presents all the identified indicators, as well as their possible gradations and the risk score attributed to each gradation. The environmental indicators must be classified through site inspections, while the classification of human indicators must occur through observations and the application of the developed questionnaire. In addition, the transmission routes associated with each indicator are Airborne Transmission (AT); Contact Transmission (CT); Droplet or Airborne Transmission (DAT); Droplet Transmission (DT); Contact or Airborne Transmission (CAT); and Transmission by Droplets, Air, and Contact (DACT), as obtained in the FTA.
Analyzing
Table 1, the number of indicators per transmission route is observed as follows:
AT: 6 environmental and 2 human indicators;
CT: 12 environmental and 4 human indicators;
DAT: 7 environmental and no human indicators;
CAT: 4 environmental and no human indicators;
DACT: 2 human indicators and no environmental indicators.
A weighted average should be calculated, according to Equation (1). The calculated value will define the risk score.
where:
xi = score assigned to indicator i, which can be 1, 2, or 3;
pi = weight of indicator i related to the transmission route.
Finally, the Risk Score (RS) found should be classified as follows:
3.5. Analytic Hierarchy Process (AHP) for Prioritizing Transmission Routes
In order to be able to assess the risks, it was necessary to choose a methodology that would allow the weight of indicator i to be obtained related to the transmission route (pi) in Equation (1). Thus, the AHP method was adopted, a very widespread multicriteria analysis technique that has a range of applications.
AHP introduces a scale of numbers that indicates how many times more important or dominant an element is over another element, concerning the criterion or property for which they are compared—The Fundamental Judgment Scale [
43], as seen in
Table 2.
To evaluate consistency in a pairwise comparison matrix, Equation (2) is applied [
43]:
where:
CI is the matrix consistency index;
n is the array order;
λmax is the largest eigenvalue of the matrix or Eigen principal number.
Using Equation (3), it is possible evaluate the inconsistency according to the order of the matrix of judgments [
43], called the Consistency Ratio (
CR). Judgments are considered consistent when
CR ≤ 0.1.
where:
CI is the matrix consistency index;
RI is the consistency index for a reciprocal matrix, obtained from
Table 3 [
43]:
AHP Application for Prioritizing COVID-19 Transmission Routes in Toilets
As previously mentioned, there are six COVID-19 transmission routes associated with the indicators identified in
Table 1, obtained in the FTA. Thus, the AHP will be derived from a 6 × 6 pairwise comparison matrix. This matrix should be completed using the indices of the Fundamental Scale of Judgments, as seen in
Table 2. Therefore, some considerations were necessary. First, based on the bibliographical review, it was considered that the main SARS-CoV-2 transmission route was DT, followed by AT, and CT was the least relevant one. Thus, it was assumed that DT is 3 times more important than AT which, in turn, is 3 times more important than CT. So, by simple algebra, DT is nine times more important than CT. The relationships between the other matrix attributes were developed in the same way. The DAT is mutually associated with the DT and AT components:
Replacing Equation (4) with the previously established relations, it can be found that DAT is 4 times and 12 times more important than AT and CT, respectively. Concerning DT, after necessary replacements, it can be established that DAT is 1.33 times more important than DT. As this value does not exist in the Fundamental Judgments Scale, as seen in
Table 2, the value was rounded to 2, i.e., DAT was considered to be 2 times more important than DT. Likewise, in the DAT case, CAT is mutually associated with the CT and AT components; that is:
Then, replacing Equation (5) with the previously established relations, it can be found that CAT is 1.33 times more important than AT. However, as in the previous case, the value was rounded to 2. Then, as CAT was considered 2 times more important than AT and AT was 3 times more important than CT, so, by replacement, CAT can be considered 6 times more important than CT. Regarding DT, it is known that DT is 9 times more important than CT. So, after necessary replacements, it can be established that CAT is equal to half of DT. Likewise, the DACT is mutually associated with the DT, AT, and CT components; that is:
It is known that DT is 3 times more important than AT, and AT is 3 times more important than CT. So, after necessary replacements, it can be established that DACT is 4.33 times more important than AT, 1.66 times more important than DT, and 18 times more important than CT. As these values do not exist in the Fundamental Judgments Scale, as seen in
Table 2, they were rounded to 5, 2, and 9, respectively, i.e., DACT was considered 5 times more important than AT, 2 times more important than DT, and 9 times more important than CT. Finally, it is necessary to establish the relations between the attributes of the matrix that involve two or more routes. As DAT is 4 times more important than AT, and CAT is 2 times more important than AT, so, by replacement, it can be established that DAT is 2 times more important than CAT.
On the other hand, as DACT is 5 times more important than AT, it was considered that DACT is 1.25 more important than DAT and 2.5 more important than CAT, which was rounded to 2 and 3, respectively. Thus,
Table 4 presents the completed judgments matrix.
Then, we proceeded with the normalization of the original matrix and obtained the eigenvectors of the normalized matrix, also called criteria weights, obtained by calculating the arithmetic mean of each row. Next, the components of the original non-normalized matrix were multiplied by the column’s respective criteria weight, obtaining the result shown in
Table 5.
The quotient of dividing the sum of each row in
Table 5 by the respective prioritization index was then calculated. The average of the values obtained was equal to 6.1155 and is equivalent to the highest eigenvalue of the matrix (λ
max). Thus, for a 6 × 6 order matrix, applying Equation (2), CI = 0.0231.
Finally, considering that RI is equal to 1.24 for a 6 × 6 order matrix, according to
Table 3, to evaluate the inconsistency of the matrix, Equation (3) was applied and a CR equal to 0.0186 was obtained; that is, CR ≤ 0.1. Therefore, the judgments assumed for the transmission routes were considered consistent. In this way, the prioritization indexes obtained can be applied to the case of COVID-19 and are listed in
Table 6.
Therefore, calculating the sum of the products of the criteria weights and the number of associated indicators as presented in
Table 1, 2.9279 was obtained for the Environmental Indicators and 0.93 for the Human Indicators, totaling 3.8579, which will be the divisor of Equation (3).
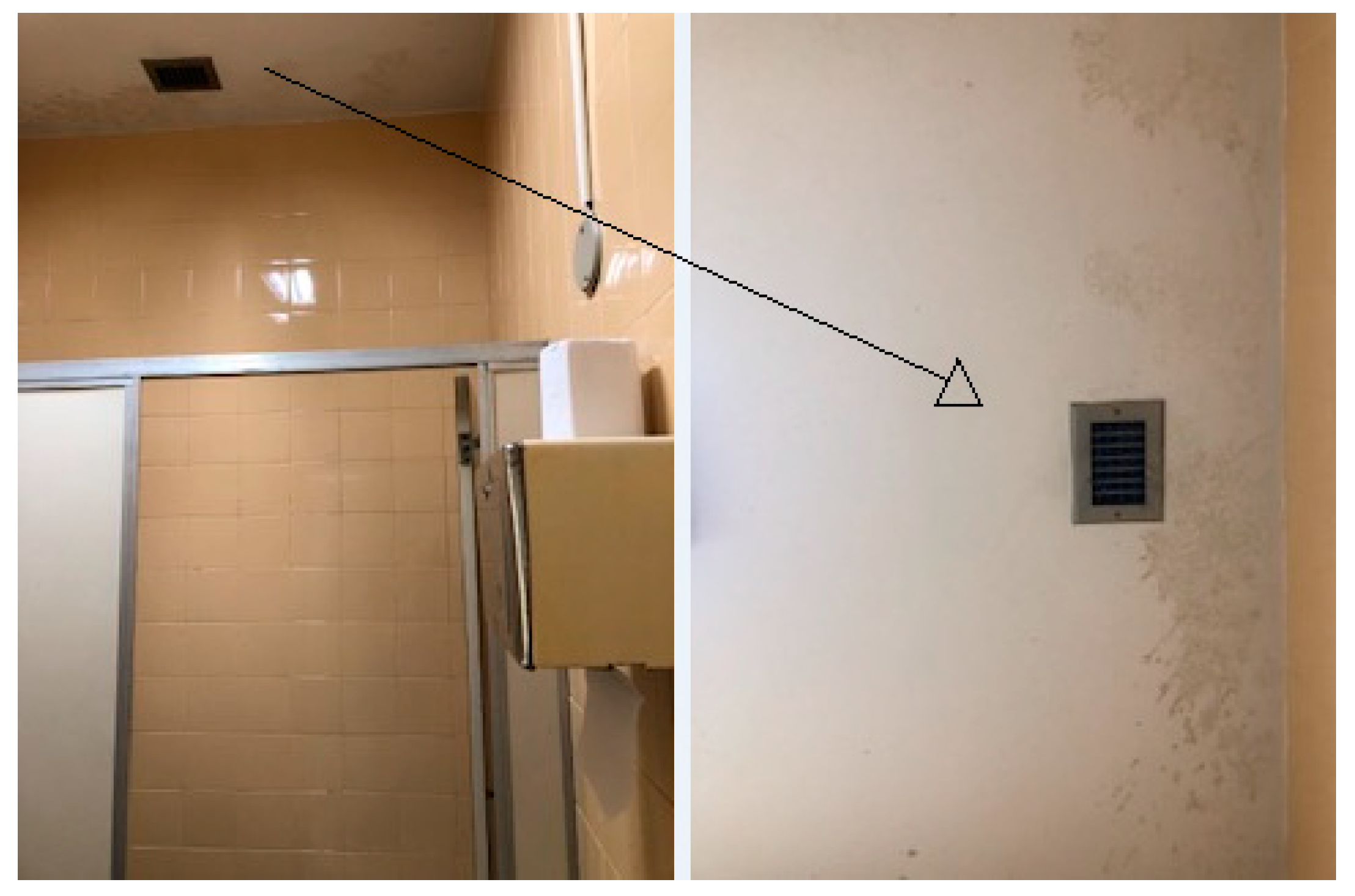
3.6. Risk Assessment: Case Study in a University Hospital
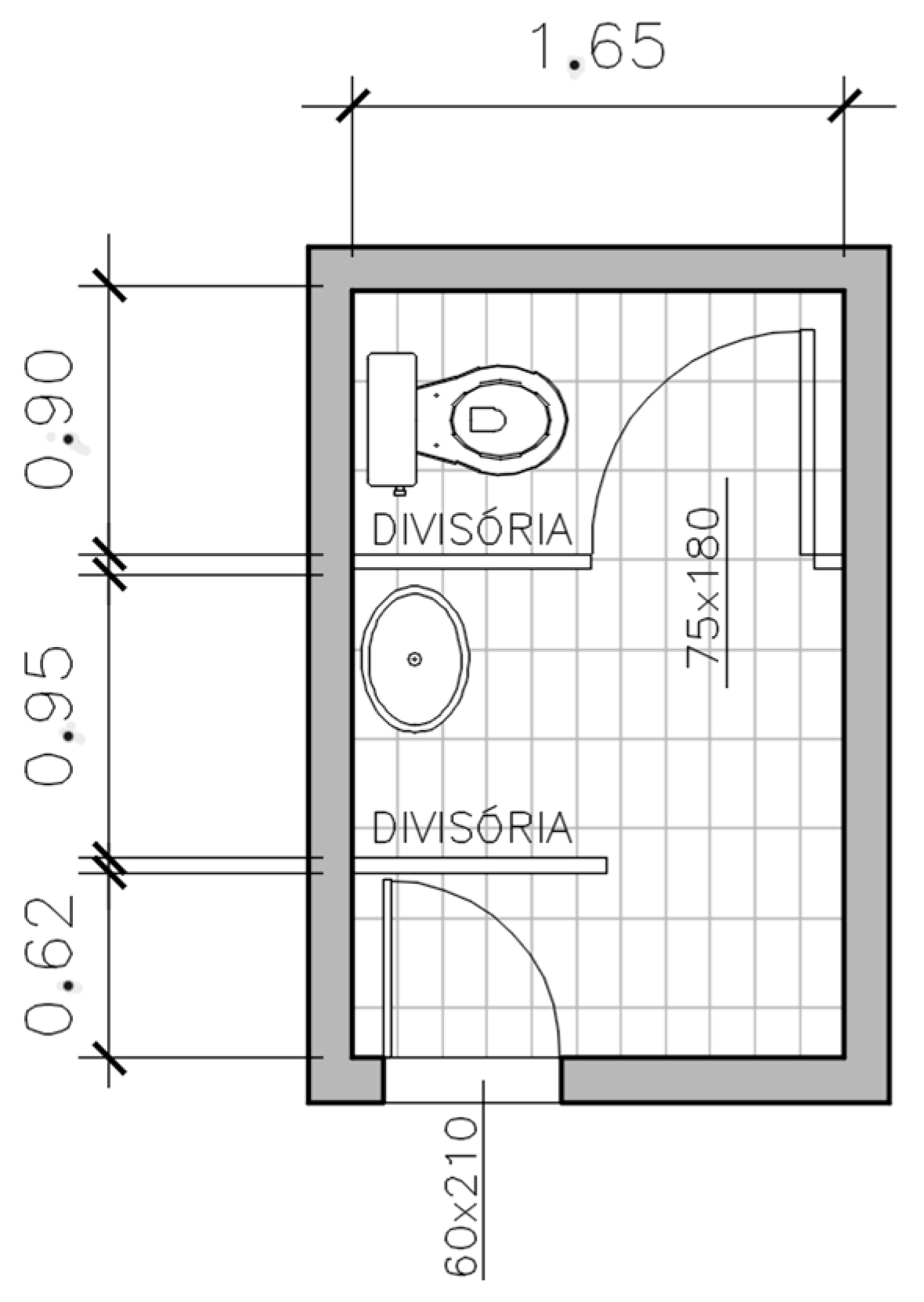
Finally, the indicators presented in
Table 1 will be evaluated for a 4.1 m
2 individual compartmentalized toilet, located in a university hospital and equipped with a washbasin and toilet, as can be seen in the sketch shown in
Figure 3. The results are presented in the next section.
5. Discussion
The objective of this research was to develop a risk assessment methodology for SARS-CoV-2 virus dissemination in toilets. To this end, this study applied widely employed safety engineering techniques—FMEA, FTA, and EWA. The application of these techniques made it possible to identify environmental, human, and transmission routes indicators related to the disease—the three main aspects of the study, which were called the “Risk Tripod”. Subsequently, the AHP methodology was applied to obtain the transmission route prioritization indexes identified for a toilet environment.
The risk score found for the restroom was classified as medium. Analyzing the used indicators, this result was consistent, considering that the studied environment had some deficiencies, as diagnosed in the inspection performed. Analyzing
Table 9, it is noted that the environmental indicators made a greater contribution to the final result, considering that the sum of the indicator scores in this group was 130% higher than the sum of the human indicator scores; that is, greater than twice. This is because 29 environmental indicators were evaluated, to the detriment of only 8 human indicators.
However, when looking at the obtained results separately for the environmental and human risk scores, it is noted that the latter resulted in a higher risk score—1.5842 versus 2.1685. This occurred because of the eight human-analyzed indicators, only one had a minimum risk score. In the case of environmental indicators, in turn, 12 of the 29 indicators had a minimum risk score, that is, 41%, which led to a result of lower risk related to these indicators.
The most important indicators in the study were those related to the DAT, CAT, and DACT routes, which had the highest Prioritization Index. Thus, it can be concluded that the project, design, and maintenance of sanitary parts have greater relevance in controlling the spread of pathogens in a sanitary environment. However, indicators such as materials and mechanisms for activating sanitary parts, associated with transmission by contact, as well as hand hygiene and the use of gloves, could be overrated regarding the transmission of the SARS-CoV-2 virus.
The risk score recalculation after simulating the implementation of corrective measures indicated a 9.9% drop in the risk score compared to the first simulation with real toilet conditions. However, despite this reduction, the risk continued to be classified as medium. Therefore, it was concluded that the selected measures—related to the mechanism for activating the faucet and the soap dispenser, the depth of the sink, and the general cleaning conditions—were not sufficient for a considerable risk reduction. This result suggests the need to implement more structural measures such as the installation of an exhaust fan, for example—it was seen that, in the case of the analyzed environment, despite the existence of an exhaust fan, it was inoperative. Regarding the sanitary part materials, there are currently no options on the market that offer less stability to pathogens, so the materials that constitute the sanitary parts of the studied environment are those commonly found in toilets and bathrooms—the adoption of futuristic surfaces such as copper and silver is still far from being a reality for the market.
It is important to highlight that the study stood out for its unprecedented method, considering that the literature review pointed out that most risk assessment tools focus on clinical practices rather than focusing on design in the area of architecture and civil construction. A study developed in Southern Switzerland, for example, conducted a prospective, SARS-CoV-2 seroprevalence study in healthcare workers. Participants were hospital personnel with varying COVID-19 exposure risk depending on job function and working site. They provided personal information (including age, sex, occupation, and medical history) and self-reported COVID-19 symptoms. The odds ratio (OR) of seropositivity to IgG antibodies was estimated by univariate and multivariate logistic regressions [
44]. Another study conducted in India introduced an innovative Risk Assessment Tool which goes beyond symptom detection and patient tracking. It includes four factors in assessment of risk: Health, Behavior, Exposure and Social Policy. Behavior covered subfactors like the use of masks, handwashing, sanitizing before touching the face, social distancing, and others [
45]. A cross-sectional online survey based on the World Health Organization (WHO) COVID-19 risk assessment tool involving physicians, pharmacists, and nurses was conducted from Pakistan to evaluate their knowledge, attitudes, and practices (KAP) and the ability to assess the risks associated with the outbreak [
46]. Finally, in a cross-sectional study that investigated the level of exposure to and risk of COVID-19 virus infection among healthcare workers in COVID-19 treatment centers in Ghana, adherence to infection prevention and control (IPC) measures were used to categorized them as at low or high risk of COVID-19 virus infection. The WHO COVID-19 risk assessment tool was also used to collect quantitative data from the study participants. The study measures were demographic characteristics, community and occupational exposure, and compliance with IPC measures [
47]. However, in all studies cited there were no subfactors related to environmental or project variables.
Regarding the limitations of the present study, it is important to discuss, firstly, the selected environment and the pathogen type. The indicators determined were specific to the environment of a toilet and the identified transmission routes were limited to the case of COVID-19. Second, three risk assessment methodologies were selected—FMEA, FTA, and EWA. These techniques were applied without multidisciplinary team participation. Thus, the identification of indicators and transmission routes was limited to the author’s knowledge and perceptions, requiring a deeper analysis. The evaluation of the human factor, for example, included a limited number of indicators and took place through observation and assumptions, without the direct application of the questionnaire.
Another limitation concerns the AHP application, which involved some assumptions that overestimated the contribution of some transmission modes. At this point, it is important to highlight the CT, for which was assumed, by simple algebra, an approximate importance of 11% DT (DT/9), although the Centers for Disease Control and Prevention (CDC) estimate the probability of contact transmission as less than 1 in 10,000 [
2]. However, it can be stated that the estimate of the real-life transmission potential of SARS-CoV-2 via fomites is still uncertain as some studies, as mentioned, found extensive virus contamination on surfaces, while others did not [
48].
For future work, a methodology application to other types of toilets or bathrooms (collective, male with urinals, equipped with a hygienic shower, shower, etc.) is recommended, encouraging the inclusion of new indicators and the identification of new transmission routes. It is even proposed to apply the methodology to non-sanitary environments, expanding the scope of the techniques used, thus enabling the identification of new risk assessment indicators that meet the specificities of other environments. It is also suggested to study other viral and bacterial infections and their transmission routes, with the application of the FTA and, subsequently, the AHP, to weigh them according to their importance in the disease spread. This will enable a more complete and robust risk assessment, covering other types of infections.
Finally, it is recommended to advance research on the design of the sanitary parts of bathrooms, with an emphasis on washbasins and flush toilets. Inspections and preventive maintenance are also essential. The adoption of safe habits and the use of PPE must be continuously encouraged, but greater attention is needed for technical and engineering issues.



 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}









