
Hemodynamic Assessment of the Pathological Left Ventricle Function under Rest and Exercise Conditions
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient-Specific Ultrasound Data and Medical Image Segmentation
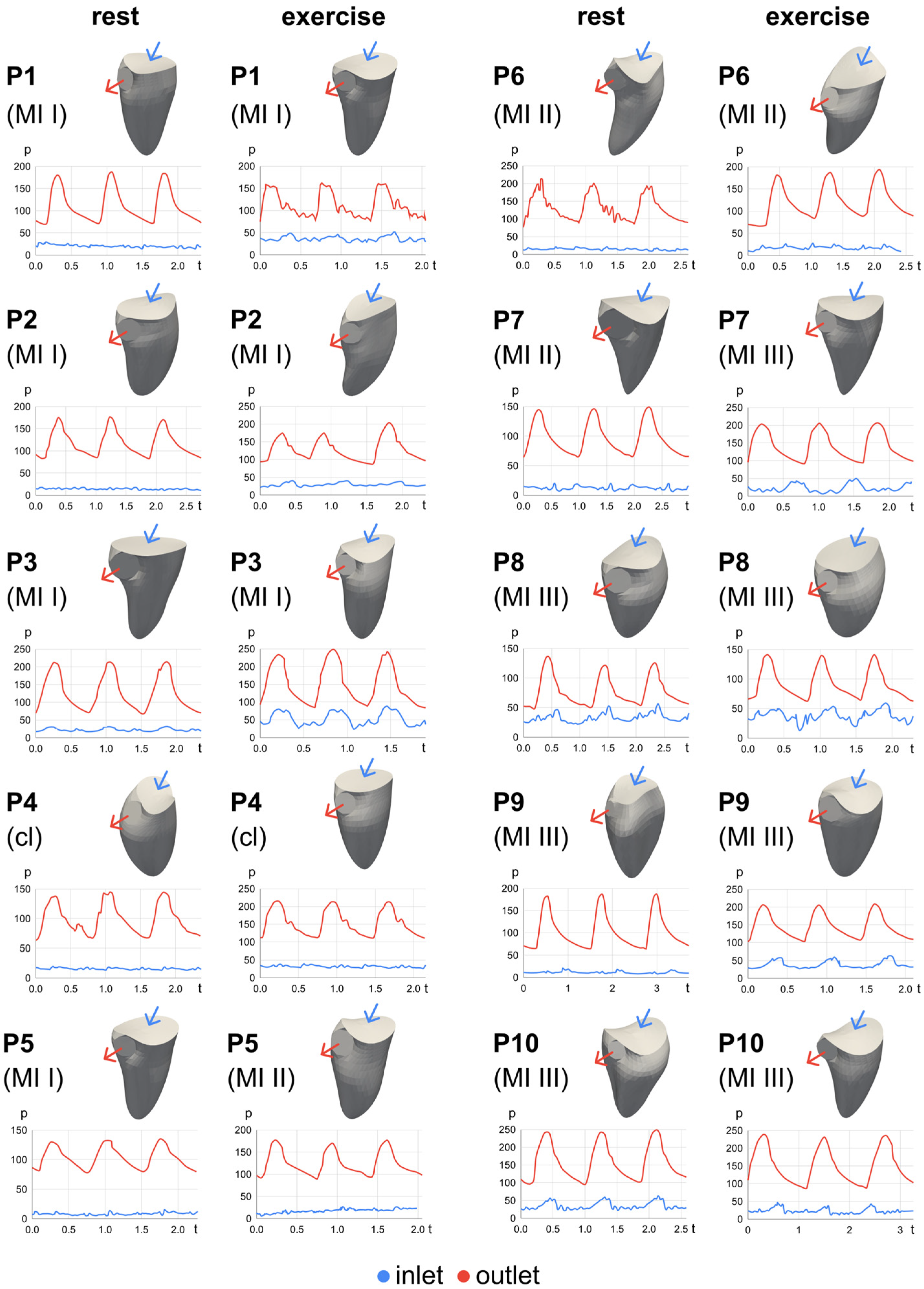
2.2. Boundary Conditions: Ventricular Wall Movement and Pressure Curves
2.3. Hemodynamic Moving Mesh Simulation
2.4. Hemodynamic Analysis
3. Results
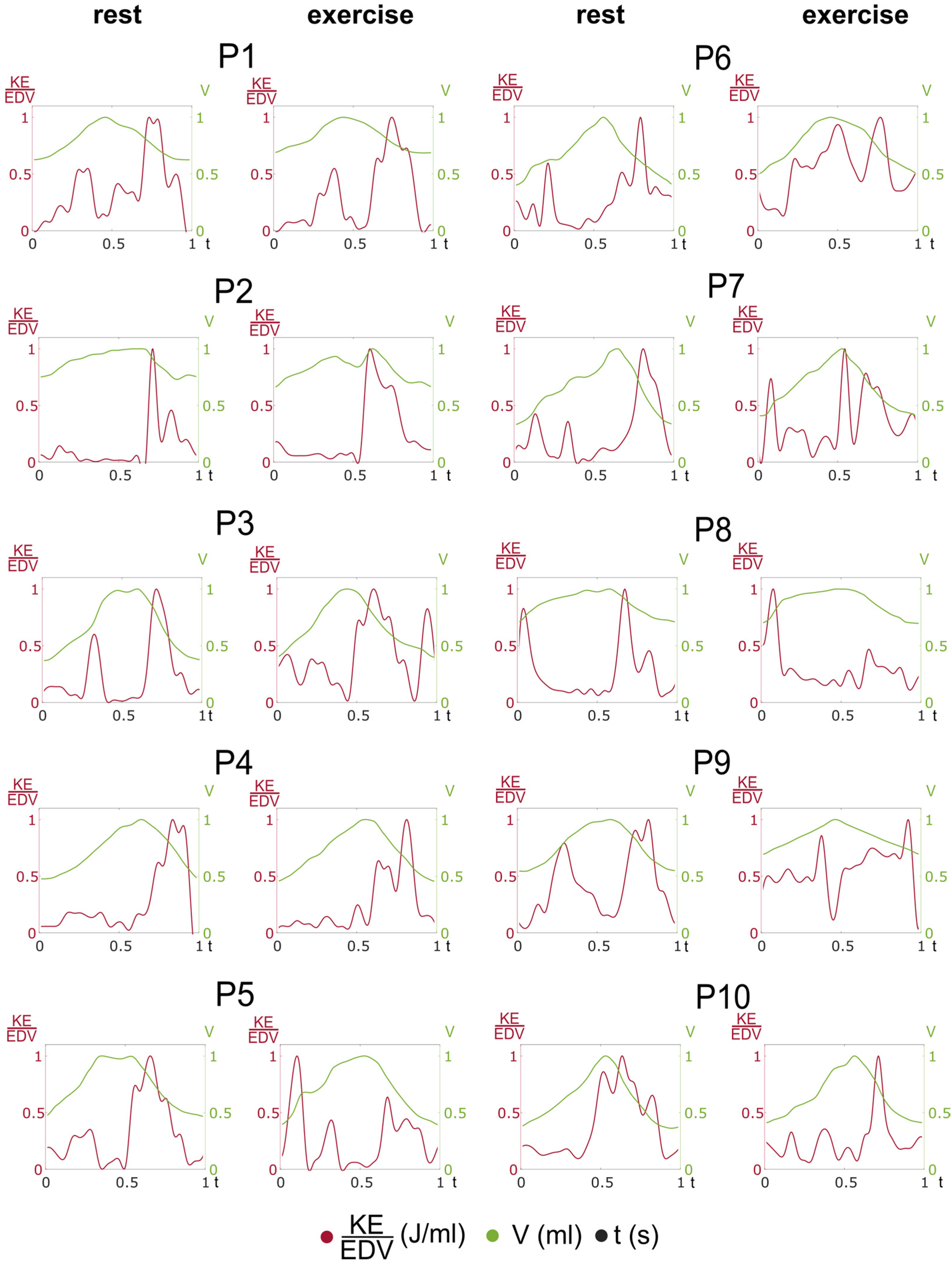
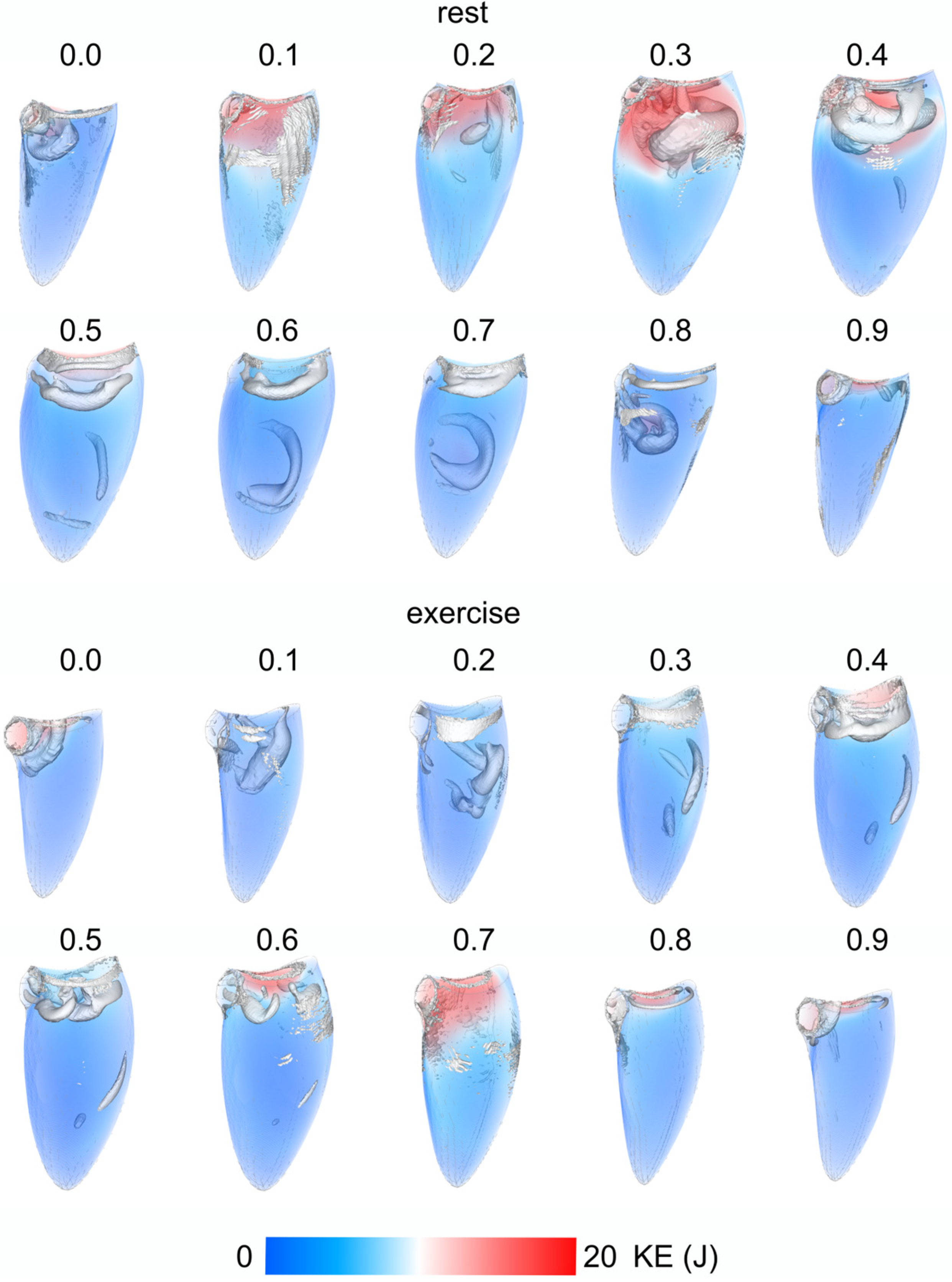
3.1. Intraventricular Kinetic Energy and Volume Curves
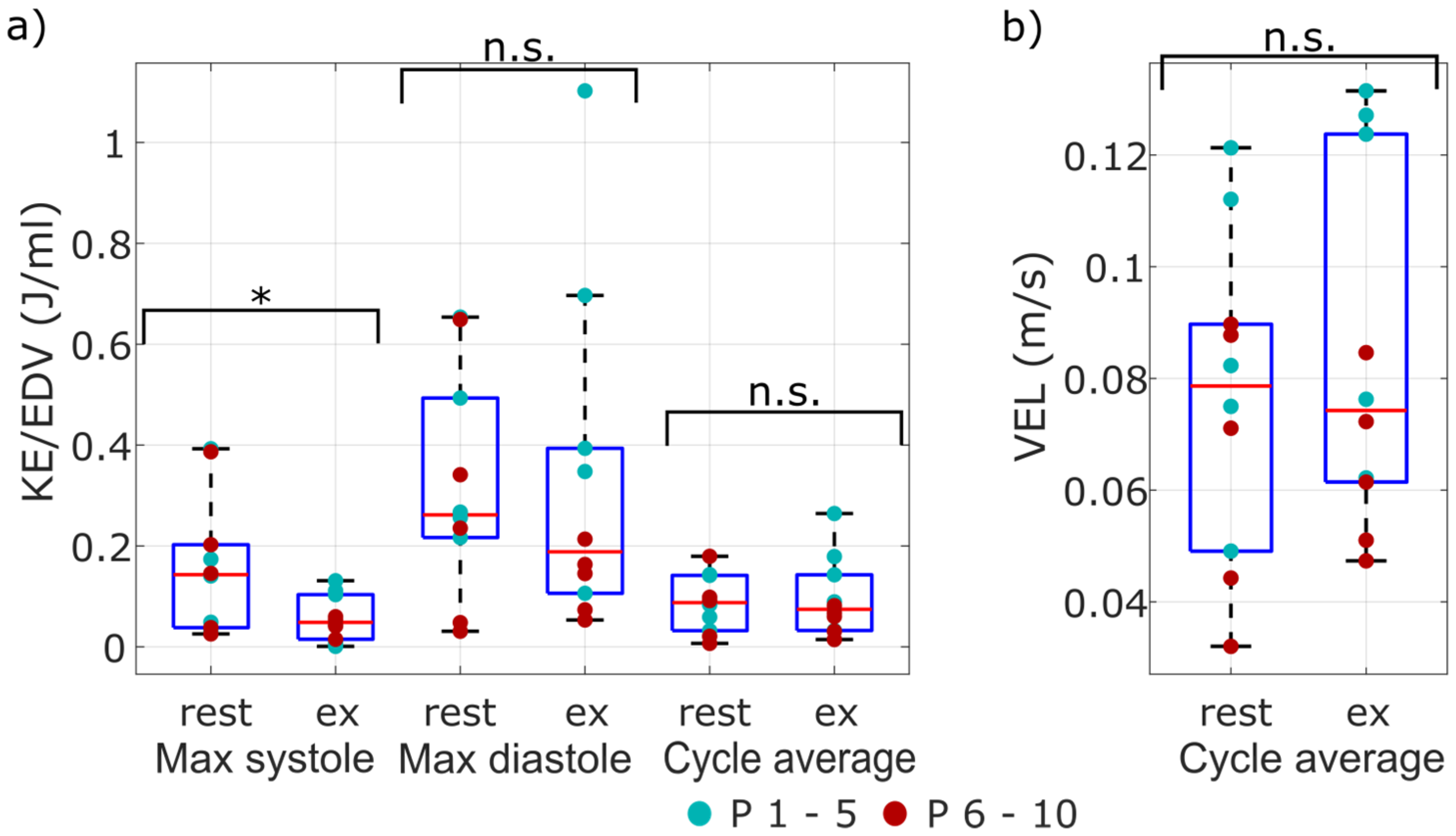
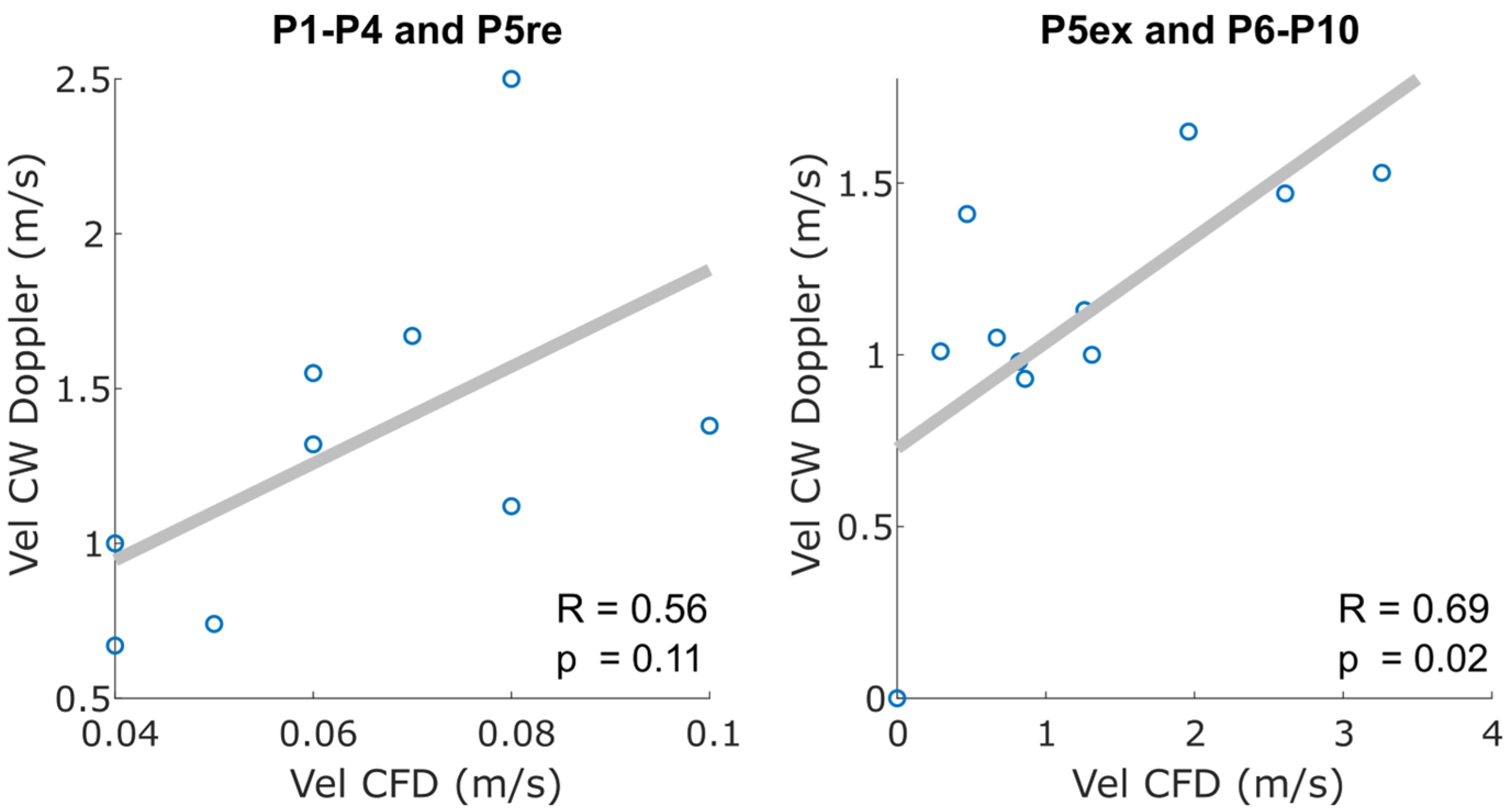
3.2. Hemodynamic Intraventricular Average and Peak Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | VCL (m) | Mean Vorticity (1/s) | Mean KE (J) | Mean VEL (m/s) | ||||
|---|---|---|---|---|---|---|---|---|
| re | ex | re | ex | re | ex | re | ex | |
| 1 | 0.01 | 0.39 | 13.46 | 9.57 | 11.07 | 4.39 | 0.11 | 0.06 |
| 2 | 0.46 | 0.69 | 10.23 | 35.23 | 3.41 | 16.34 | 0.05 | 0.12 |
| 3 | 0 | 0.07 | 22.61 | 24.04 | 15.45 | 14.86 | 0.12 | 0.13 |
| 4 | 0.17 | 0.18 | 10.74 | 15.02 | 6.30 | 6.79 | 0.07 | 0.08 |
| 5 | 0.27 | 0.26 | 21.70 | 28.69 | 8.04 | 16.56 | 0.08 | 0.13 |
| Mean | 0.18 | 0.32 | 15.75 | 22.51 | 8.85 | 11.79 | 0.09 | 0.10 |
| Std | 0.17 | 0.21 | 5.35 | 9.23 | 4.13 | 5.14 | 0.03 | 0.03 |
| 6 | 0.10 | 0.18 | 29.34 | 22.09 | 7.34 | 5.93 | 0.09 | 0.08 |
| 7 | 0.16 | 0.21 | 17.70 | 16.65 | 4.64 | 4.27 | 0.07 | 0.07 |
| 8 | 0.28 | 0.23 | 6.81 | 10.34 | 0.96 | 1.92 | 0.03 | 0.05 |
| 9 | 0.29 | 0.19 | 8.50 | 7.58 | 1.96 | 1.94 | 0.04 | 0.05 |
| 10 | 0.30 | 0.27 | 23.82 | 17.40 | 7.81 | 3.51 | 0.09 | 0.06 |
| Mean | 0.23 | 0.22 | 17.23 | 14.81 | 4.54 | 3.51 | 0.06 | 0.06 |
| Std | 0.08 | 0.03 | 8.66 | 5.20 | 2.76 | 1.51 | 0.02 | 0.01 |
References
- Faletra, F.; La Marchesina, U.; Bragato, R.; Grimaldi, A. Insufficienza mitralica. Ital. Heart J. Suppl. 2002, 3, 486–494. [Google Scholar] [PubMed]
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: A population-based study. Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Nagai, T.; Anzai, T. NYHA functional classification and AHA/ACC Stages for heart failure management. Nihon rinsho. Jpn. J. Clin. Med. 2016, 74 (Suppl. 6), 340–344. [Google Scholar]
- Sugimoto, T.; Bandera, F.; Generati, G.; Alfonzetti, E.; Barletta, M.; Losito, M.; Labate, V.; Rovida, M.; Caracciolo, M.; Pappone, C.; et al. Left Atrial Dynamics During Exercise in Mitral Regurgitation of Primary and Secondary Origin: Pathophysiological Insights by Exercise Echocardiography Combined With Gas Exchange Analysis. JACC Cardiovasc. Imaging 2020, 13, 25–40. [Google Scholar] [CrossRef]
- Izem, O.; Maufrais, C.; Obert, P.; Rupp, T.; Schuster, I.; Nottin, S. Kinetics of Left Ventricular Mechanics during Transition from Rest to Exercise. Med. Sci. Sports Exerc. 2019, 51, 1838–1844. [Google Scholar] [CrossRef] [PubMed]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef] [PubMed]
- Vakil, K.; Roukoz, H.; Sarraf, M.; Krishnan, B.; Reisman, M.; Levy, W.C.; Adabag, S. Safety and efficacy of the MitraClip® system for severe mitral regurgitation: A systematic review. Catheter. Cardiovasc. Interv. 2014, 84, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Borazjani, I.; Westerdale, J.; McMahon, E.M.; Rajaraman, P.K.; Heys, J.J.; Belohlavek, M. Left Ventricular Flow Analysis: Recent Advances in Numerical Methods and Applications in Cardiac Ultrasound. Comput. Math. Methods Med. 2013, 2013, 395081. [Google Scholar] [CrossRef] [Green Version]
- Collia, D.; Zovatto, L.; Tonti, G.; Pedrizzetti, G. Comparative Analysis of Right Ventricle Fluid Dynamics. Front. Bioeng. Biotechnol. 2021, 9, 667408. [Google Scholar] [CrossRef]
- Larsson, D.; Spuhler, J.H.; Petersson, S.; Nordenfur, T.; Colarieti-Tosti, M.; Hoffman, J.; Winter, R.; Larsson, M. Patient-Specific Left Ventricular Flow Simulations From Transthoracic Echocardiography: Robustness Evaluation and Validation Against Ultrasound Doppler and Magnetic Resonance Imaging. IEEE Trans. Med. Imaging 2017, 36, 2261–2275. [Google Scholar] [CrossRef]
- Nguyen, V.-T.; Wibowo, S.N.; Leow, Y.A.; Nguyen, H.-H.; Liang, Z.; Leo, H.L. A Patient-Specific Computational Fluid Dynamic Model for Hemodynamic Analysis of Left Ventricle Diastolic Dysfunctions. Cardiovasc. Eng. Technol. 2015, 6, 412–429. [Google Scholar] [CrossRef]
- Goubergrits, L.; Vellguth, K.; Obermeier, L.; Schlief, A.; Tautz, L.; Bruening, J.; Lamecker, H.; Szengel, A.; Nemchyna, O.; Knosalla, C.; et al. CT-Based Analysis of Left Ventricular Hemodynamics Using Statistical Shape Modeling and Computational Fluid Dynamics. Front. Cardiovasc. Med. 2022, 9, 901902. [Google Scholar] [CrossRef] [PubMed]
- Obermeier, L.; Vellguth, K.; Schlief, A.; Tautz, L.; Bruening, J.; Knosalla, C.; Kuehne, T.; Solowjowa, N.; Goubergrits, L. CT-Based Simulation of Left Ventricular Hemodynamics: A Pilot Study in Mitral Regurgitation and Left Ventricle Aneurysm Patients. Front. Cardiovasc. Med. 2022, 9, 828556. [Google Scholar] [CrossRef] [PubMed]
- Bavo, A.; Pouch, A.; Degroote, J.; Vierendeels, J.; Gorman, J.; Gorman, R.; Segers, P. Patient-specific CFD models for intraventricular flow analysis from 3D ultrasound imaging: Comparison of three clinical cases. J. Biomech. 2017, 50, 144–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilberath, J.N.; Oakes, D.A.; Shernan, S.K.; Bulwer, B.E.; D’Ambra, M.N.; Eltzschig, H.K. Safety of Transesophageal Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 1115–1127. [Google Scholar] [CrossRef] [PubMed]
- Matulevicius, S.A.; Rohatgi, A.; Das, S.R.; Price, A.L.; DeLuna, A.; Reimold, S.C. Appropriate Use and Clinical Impact of Transthoracic Echocardiography. JAMA Intern. Med. 2013, 173, 1600–1607. [Google Scholar] [CrossRef]
- Marino, P.N.; Zanaboni, J.; Degiovanni, A.; Sartori, C.; Patti, G.; Fraser, A.G. Left atrial conduit flow rate at baseline and during exercise: An index of impaired relaxation in HFpEF patients. ESC Hear. Fail. 2021, 8, 4334–4342. [Google Scholar] [CrossRef]
- Bakkestrøm, R.; Banke, A.; Christensen, N.L.; Pecini, R.; Irmukhamedov, A.; Andersen, M.; Borlaug, B.A.; Møller, J.E. Hemodynamic Characteristics in Significant Symptomatic and Asymptomatic Primary Mitral Valve Regurgitation at Rest and During Exercise. Circ. Cardiovasc. Imaging 2018, 11, e007171. [Google Scholar] [CrossRef] [Green Version]
- Grünwald, A.; Korte, J.; Wilmanns, N.; Winkler, C.; Linden, K.; Herberg, U.; Groß-Hardt, S.; Steinseifer, U.; Neidlin, M. Intraventricular Flow Simulations in Singular Right Ventricles Reveal Deteriorated Washout and Low Vortex Formation. Cardiovasc. Eng. Technol. 2021, 13, 495–503. [Google Scholar] [CrossRef]
- Qin, R.; Duan, C. The principle and applications of Bernoulli equation. J. Physics: Conf. Ser. 2017, 916, 012038. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, P.; Fraser, K.; Griffith, B.P.; Wu, Z.J. Comparison and Experimental Validation of Fluid Dynamic Numerical Models for a Clinical Ventricular Assist Device. Artif. Organs 2013, 37, 380–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghodrati, M.; Khienwad, T.; Maurer, A.; Moscato, F.; Zonta, F.; Schima, H.; Aigner, P. Validation of numerically simulated ventricular flow patterns during left ventricular assist device support. Int. J. Artif. Organs 2021, 44, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Mut, F.; Löhner, R.; Chien, A.; Tateshima, S.; Viñuela, F.; Putman, C.; Cebral, J.R. Computational hemodynamics framework for the analysis of cerebral aneurysms. Int. J. Numer. Methods Biomed. Eng. 2011, 27, 822–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheitlin, M.D.; Armstrong, W.F.; Aurigemma, G.P.; A Beller, G.; Bierman, F.Z.; Davis, J.L.; Douglas, P.S.; Faxon, D.P.; Gillam, L.D.; Kimball, T.R.; et al. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: Summary article: A report of the American college of cardiology/American heart association task force on practice guidelines (ACC/AHA/ASE committee to update the 1997 guidelines for the clinical application of echocardiography). J. Am. Coll. Cardiol. 2003, 42, 954–970. [Google Scholar]
- Voilliot, D.; Lancellotti, P. Exercise Testing and Stress Imaging in Mitral Valve Disease. Curr. Treat. Options Cardiovasc. Med. 2017, 19, 17. [Google Scholar] [CrossRef]
- Marwick, T.H.; Anderson, T.; Williams, M.; Haluska, B.; Melin, J.A.; Pashkow, F.; Thomas, J.D. Exercise echocardiography is an accurate and cost-efficient technique for detection of coronary artery disease in women. J. Am. Coll. Cardiol. 1995, 26, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Pearlman, A.S.; Ryan, T.; Picard, M.H.; Douglas, P.S. Evolving Trends in the Use of Echocardiography: A Study of Medicare Beneficiaries. J. Am. Coll. Cardiol. 2007, 49, 2283–2291. [Google Scholar] [CrossRef] [Green Version]
- Al-Wakeel, N.; Ms, J.F.F.; Amiri, A.; Siniawski, H.; Goubergrits, L.; Berger, F.; Kuehne, T. Hemodynamic and energetic aspects of the left ventricle in patients with mitral regurgitation before and after mitral valve surgery. J. Magn. Reson. Imaging 2015, 42, 1705–1712. [Google Scholar] [CrossRef]
- Grewal, J.; McCully, R.B.; Kane, G.C.; Lam, C.; Pellikka, P.A. Left ventricular function and exercise capacity. JAMA 2009, 301, 286–294. [Google Scholar] [CrossRef] [Green Version]
- Stöhr, E.J.; González-Alonso, J.; Bezodis, I.N.; Shave, R. Left ventricular energetics: New insight into the plasticity of regional contributions at rest and during exercise. Am. J. Physiol. Circ. Physiol. 2014, 306, H225–H232. [Google Scholar] [CrossRef] [Green Version]
- Vahanian, A.; Iung, B. Mitral regurgitation. Timing of surgery or interventional treatment. Herz 2016, 41, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Kenjereš, S. Numerical simulations of flow patterns in the human left ventricle model with a novel dynamic mesh morphing approach based on radial basis function. Comput. Biol. Med. 2021, 130, 104184. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, J.; Carlhäll, C.-J.; Dyverfeldt, P.; Engvall, J.; Bolger, A.F.; Ebbers, T. Semi-automatic quantification of 4D left ventricular blood flow. J. Cardiovasc. Magn. Reson. 2010, 12, 9. [Google Scholar] [CrossRef] [Green Version]



| Case | MI | Sex | Age | Weight | Height | ESV (mL) | ||
|---|---|---|---|---|---|---|---|---|
| rest | exercise | (kg) | (cm) | rest | exercise | |||
| 1 | MI I | MI I | m | 75 | 89 | 178 | 82.96 | 93.18 |
| 2 | MI I | MI I | m | 76 | 93 | 175 | 80.43 | 64.93 |
| 3 | MI I | MI I | m | 76 | 76 | 188 | 41.18 | 42.28 |
| 4 | clipped | clipped | f | 78 | 86 | 160 | 51.15 | 37.13 |
| 5 | MI I | MI II | f | 78 | 84 | 180 | 26.52 | 25.06 |
| 6 | MI II | MI II | f | 73 | 79 | 168 | 16.46 | 38.13 |
| 7 | MI II | MI III | f | 67 | 57 | 170 | 15.72 | 26.14 |
| 8 | MI III | MI III | m | 81 | 76 | 176 | 100.63 | 93.17 |
| 9 | MI III | MI III | f | 86 | 65 | 154 | 50.98 | 43.20 |
| 10 | MI III | MI III | f | 78 | 75 | 163 | 30.81 | 23.92 |
| Case | EDV (mL) | EF (-) | HR (bpm) | Timesteps n | ||||
| rest | exercise | rest | exercise | rest | exercise | rest | exercise | |
| 1 | 132.67 | 135.50 | 37.47 | 31.23 | 89 | 110 | 12 | 10 |
| 2 | 106.14 | 91.29 | 24.22 | 28.87 | 71 | 133 | 16 | 14 |
| 3 | 109.02 | 104.01 | 62.23 | 59.35 | 68 | 120 | 14 | 11 |
| 4 | 106.76 | 76.12 | 52.08 | 51.22 | 60 | 89 | 15 | 16 |
| 5 | 56.16 | 62.64 | 52.78 | 59.98 | 77 | 114 | 16 | 16 |
| 6 | 40.90 | 72.57 | 59.76 | 47.46 | 60 | 116 | 19 | 15 |
| 7 | 47.12 | 63.57 | 66.63 | 58.89 | 47 | 124 | 21 | 20 |
| 8 | 140.12 | 132.76 | 28.19 | 29.82 | 67 | 110 | 15 | 23 |
| 9 | 93.65 | 62.33 | 45.56 | 30.69 | 58 | 111 | 20 | 14 |
| 10 | 85.00 | 58.30 | 63.75 | 58.97 | 66 | 117 | 18 | 17 |
| Mean Rest | Std Rest | Mean Ex | Std Ex | p-Value | |
|---|---|---|---|---|---|
| VCL (m) | 0.20 | 0.14 | 0.27 | 0.16 | 0.36 |
| ω (1/s) | 16.49 | 7.24 | 18.66 | 8.42 | 0.56 |
| KE/EDV (J/mL) | 0.09 | 0.06 | 0.10 | 0.08 | 0.73 |
| VEL (m/s) | 0.08 | 0.03 | 0.08 | 0.03 | 0.60 |
| max dias KE/EDV (J/mL) | 0.32 | 0.22 | 0.33 | 0.34 | 0.94 |
| max sys KE/EDV (J/mL) | 0.16 | 0.14 | 0.06 | 0.05 | 0.04 |
| Mean P1–5 | Std P1–5 | Mean P6–10 | Std P6–10 | p-Value | |
|---|---|---|---|---|---|
| (ex + rest) | (ex + rest) | (ex + rest) | (ex + rest) | ||
| KE/EDV (J/mL) | 0.12 | 0.07 | 0.07 | 0.05 | 0.08 |
| VEL (m/s) | 0.10 | 0.03 | 0.06 | 0.02 | 0.01 |
| max dias KE/EDV (J/mL) | 0.45 | 0.30 | 0.20 | 0.19 | 0.03 |
| max sys KE/EDV (J/mL) | 0.11 | 0.11 | 0.10 | 0.11 | 0.80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korte, J.; Rauwolf, T.; Thiel, J.-N.; Mitrasch, A.; Groschopp, P.; Neidlin, M.; Schmeißer, A.; Braun-Dullaeus, R.; Berg, P. Hemodynamic Assessment of the Pathological Left Ventricle Function under Rest and Exercise Conditions. Fluids 2023, 8, 71. https://doi.org/10.3390/fluids8020071
Korte J, Rauwolf T, Thiel J-N, Mitrasch A, Groschopp P, Neidlin M, Schmeißer A, Braun-Dullaeus R, Berg P. Hemodynamic Assessment of the Pathological Left Ventricle Function under Rest and Exercise Conditions. Fluids. 2023; 8(2):71. https://doi.org/10.3390/fluids8020071
Chicago/Turabian StyleKorte, Jana, Thomas Rauwolf, Jan-Niklas Thiel, Andreas Mitrasch, Paulina Groschopp, Michael Neidlin, Alexander Schmeißer, Rüdiger Braun-Dullaeus, and Philipp Berg. 2023. "Hemodynamic Assessment of the Pathological Left Ventricle Function under Rest and Exercise Conditions" Fluids 8, no. 2: 71. https://doi.org/10.3390/fluids8020071