
Potential Implication of Azole Persistence in the Treatment Failure of Two Haematological Patients Infected with Aspergillus fumigatus
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Aspergillus fumigatus Strains
2.2. Clinical Antifungal Drugs Susceptibility Testing
2.3. Determination of Persistence
2.4. Cyp51A and Cyp51B Amplification, PCR Conditions and Sequencing
2.5. Strains Genotyping
2.6. Monitoring Antifungal Levels
3. Results
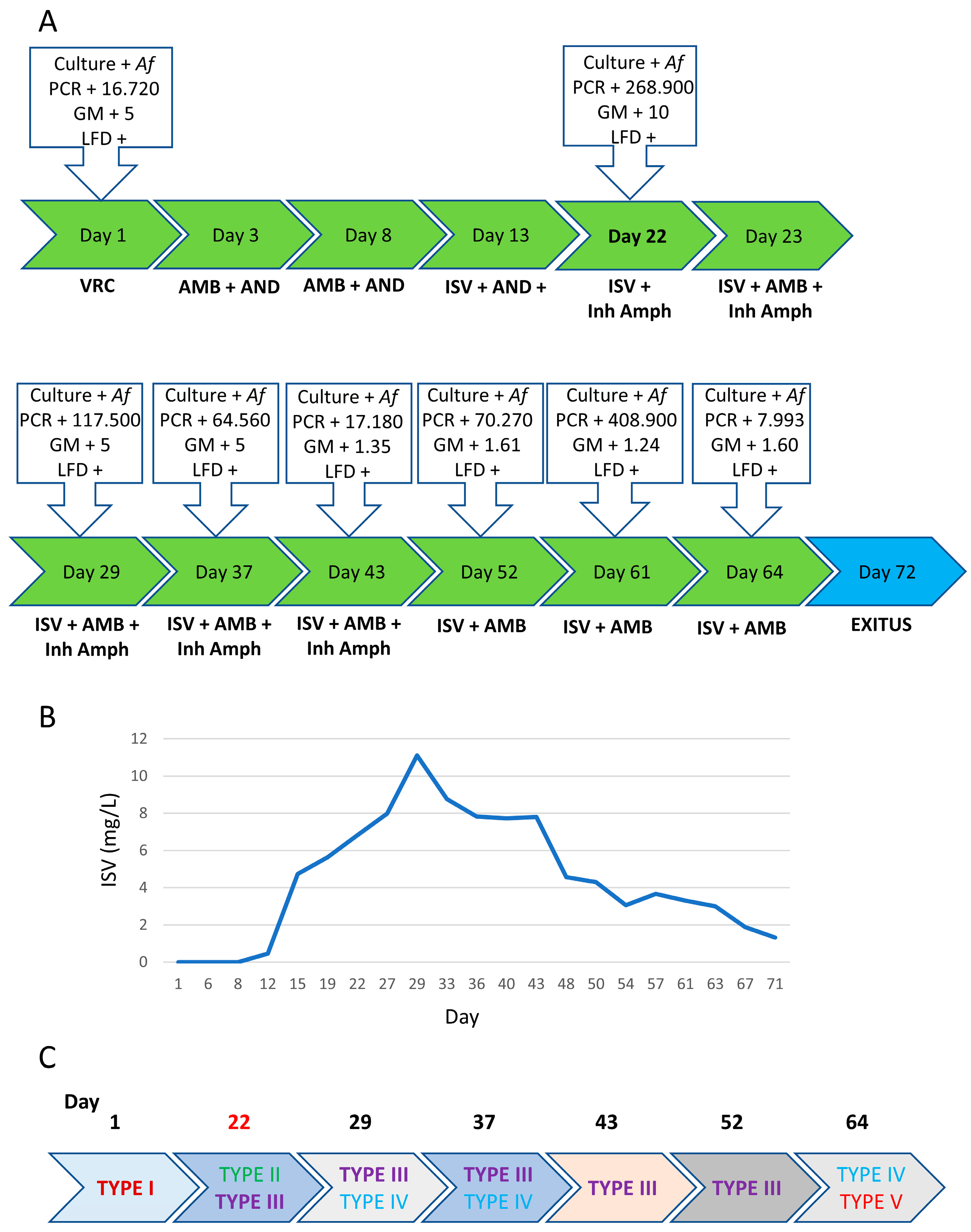
3.1. Patient 1
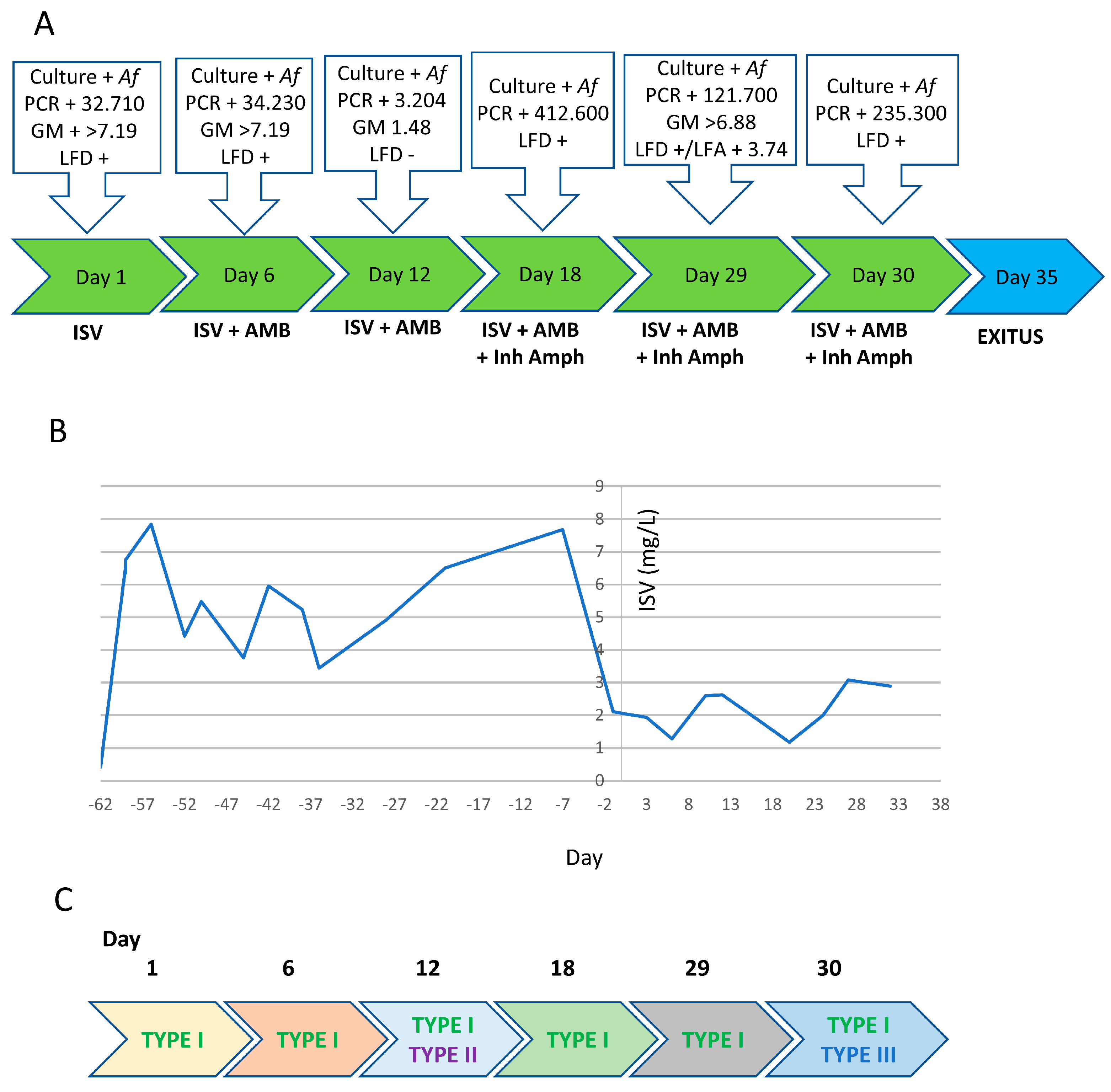
3.2. Patient 2
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Latgé, J.-P.; Chamilos, G. Aspergillus fumigatus and Aspergillosis in 2019. Clin. Microbiol. Rev. 2019, 33, e00140-18. [Google Scholar] [CrossRef]
- Thompson, G.R.; Young, J.-A.H. Aspergillus Infections. N. Engl. J. Med. 2021, 385, 1496–1509. [Google Scholar] [CrossRef] [PubMed]
- Baddley, J.W.; Andes, D.R.; Marr, K.A.; Kontoyiannis, D.P.; Alexander, B.D.; Kauffman, C.A.; Oster, R.A.; Anaissie, E.J.; Walsh, T.J.; Schuster, M.G.; et al. Factors Associated with Mortality in Transplant Patients with Invasive Aspergillosis. Clin. Infect. Dis. 2010, 50, 1559–1567. [Google Scholar] [CrossRef] [PubMed]
- Baddley, J.W.; Stephens, J.M.; Ji, X.; Gao, X.; Schlamm, H.T.; Tarallo, M. Aspergillosis in Intensive Care Unit (ICU) patients: Epidemiology and economic outcomes. BMC Infect. Dis. 2013, 13, 29. [Google Scholar] [CrossRef] [PubMed]
- González-García, P.; Alonso-Sardón, M.; Rodríguez-Alonso, B.; Almeida, H.; Romero-Alegría, Á.; Vega-Rodríguez, V.-J.; López-Bernús, A.; Muñoz-Bellido, J.L.; Muro, A.; Pardo-Lledías, J.; et al. How Has the Aspergillosis Case Fatality Rate Changed over the Last Two Decades in Spain? J. Fungi 2022, 8, 576. [Google Scholar] [CrossRef]
- Sun, K.-S.; Tsai, C.-F.; Chen, S.C.-C.; Huang, W.-C. Clinical outcome and prognostic factors associated with invasive pulmonary aspergillosis: An 11-year follow-up report from Taiwan. PLoS ONE 2017, 12, e0186422. [Google Scholar] [CrossRef] [PubMed]
- Wingard, J.R.; Ribaud, P.; Schlamm, H.T.; Herbrecht, R. Changes in causes of death over time after treatment for invasive aspergillosis. Cancer 2008, 112, 2309–2312. [Google Scholar] [CrossRef]
- van de Peppel, R.; Visser, L.; Dekkers, O.; de Boer, M. The burden of Invasive Aspergillosis in patients with haematological malignancy: A meta-analysis and systematic review. J. Infect. 2018, 76, 550–562. [Google Scholar] [CrossRef]
- Rahi, M.S.; Jindal, V.; Pednekar, P.; Parekh, J.; Gunasekaran, K.; Sharma, S.; Stender, M.; Jaiyesimi, I.A. Fungal infections in hematopoietic stem-cell transplant patients: A review of epidemiology, diagnosis, and management. Ther. Adv. Infect. Dis. 2021, 8, 20499361211039050. [Google Scholar] [CrossRef]
- Upton, A.; Kirby, K.A.; Carpenter, P.; Boeckh, M.; Marr, K.A. Invasive Aspergillosis following Hematopoietic Cell Transplantation: Outcomes and Prognostic Factors Associated with Mortality. Clin. Infect. Dis. 2007, 44, 531–540. [Google Scholar] [CrossRef]
- Nicolle, M.-C.; Bénet, T.; Thiebaut, A.; Bienvenu, A.-L.; Voirin, N.; Duclos, A.; Sobh, M.; Cannas, G.; Thomas, X.; Nicolini, F.-E.; et al. Invasive aspergillosis in patients with hematologic malignancies: Incidence and description of 127 cases enrolled in a single institution prospective survey from 2004 to 2009. Haematologica 2011, 96, 1685–1691. [Google Scholar] [CrossRef]
- Verweij, P.E.; Ananda-Rajah, M.; Andes, D.; Arendrup, M.C.; Brüggemann, R.J.; Chowdhary, A.; Cornely, O.A.; Denning, D.W.; Groll, A.H.; Izumikawa, K.; et al. International expert opinion on the management of infection caused by azole-resistant Aspergillus fumigatus. Drug Resist. Updat. 2015, 21–22, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.C.; Hawkins, N.J.; Sanglard, D.; Gurr, S.J. Worldwide emergence of resistance to antifungal drugs challenges human health and food security. Science 2018, 360, 739–742. [Google Scholar] [CrossRef]
- van der Linden, J.W.M.; Snelders, E.; Kampinga, G.A.; Rijnders, B.J.A.; Mattsson, E.; Debets-Ossenkopp, Y.J.; Kuijper, E.J.; Van Tiel, F.H.; Melchers, W.J.G.; Verweij, P.E. Clinical implications of azole resistance in Aspergillus fumigatus, The Netherlands, 2007–2009. Emerg. Infect. Dis. 2011, 17, 1846–1854. [Google Scholar] [CrossRef] [PubMed]
- Lestrade, P.P.; Bentvelsen, R.G.; Schauwvlieghe, A.F.A.D.; Schalekamp, S.; Van Der Velden, W.J.F.M.; Kuiper, E.J.; Van Paassen, J.; Van Der Hoven, B.; A Van Der Lee, H.; Melchers, W.J.G.; et al. Voriconazole Resistance and Mortality in Invasive Aspergillosis: A Multicenter Retrospective Cohort Study. Clin. Infect. Dis. 2019, 68, 1463–1471. [Google Scholar] [CrossRef] [PubMed]
- Arendrup, M.C.; Meletiadis, J.; Mouton, J.W.; Guinea, J.; Cuenca-Estrella, M.; Lagrou, K.; Howard, S.J.; Arendrup, M.C.; Howard, S.J.; Mouton, J.; et al. EUCAST technical note on isavuconazole breakpoints for Aspergillus, itraconazole breakpoints for Candida and updates for the antifungal susceptibility testing method documents. Clin. Microbiol. Infect. 2016, 22, 571.e1–571.e4. [Google Scholar] [CrossRef]
- CLSI. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi, Approved Standard—2nd ed.; CLSI Document M38-A2, Wayne, P., Eds.; Clinical and Laboratory Institute: Wayne, PA, USA, 2008. [Google Scholar]
- Pascual, A.; Calandra, T.; Bolay, S.; Buclin, T.; Bille, J.; Marchetti, O. Voriconazole Therapeutic Drug Monitoring in Patients with Invasive Mycoses Improves Efficacy and Safety Outcomes. Clin. Infect. Dis. 2008, 46, 201–211. [Google Scholar] [CrossRef]
- Chau, M.M.; Daveson, K.; Alffenaar, J.C.; Gwee, A.; Ho, S.A.; Marriott, D.J.E.; Trubiano, J.A.; Zhao, J.; Roberts, J.A.; Slavin, M.A.; et al. Consensus guidelines for optimising antifungal drug delivery and monitoring to avoid toxicity and improve outcomes in patients with haematological malignancy and haemopoietic stem cell transplant recipients, 2021. Intern. Med. J. 2021, 51, 37–66. [Google Scholar] [CrossRef]
- Patterson, T.F.; Thompson, G.R., III; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24, e1–e38. [Google Scholar] [CrossRef]
- Caillot, D.; Casasnovas, O.; Bernard, A.; Couaillier, J.F.; Durand, C.; Cuisenier, B.; Solary, E.; Piard, F.; Petrella, T.; Bonnin, A.; et al. Improved management of invasive pulmonary aspergillosis in neutropenic patients using early thoracic computed tomographic scan and surgery. J. Clin. Oncol. 1997, 15, 139–147. [Google Scholar] [CrossRef]
- Park, S.Y.; Yoon, J.-A.; Kim, S.-H. Voriconazole-refractory invasive aspergillosis. Korean J. Intern. Med. 2017, 32, 805–812. [Google Scholar] [CrossRef]
- Lee, A.; Prideaux, B.; Lee, M.H.; Zimmerman, M.; Dolgov, E.; Perlin, D.S.; Zhao, Y. Tissue Distribution and Penetration of Isavuconazole at the Site of Infection in Experimental Invasive Aspergillosis in Mice with Underlying Chronic Granulomatous Disease. Antimicrob. Agents Chemother. 2019, 63, e00524-19. [Google Scholar] [CrossRef]
- Zhao, Y.; Prideaux, B.; Baistrocchi, S.; Sheppard, D.C.; Perlin, D.S. Beyond tissue concentrations: Antifungal penetration at the site of infection. Med. Mycol. 2019, 57 (Suppl. 2), S161–S167. [Google Scholar] [CrossRef] [PubMed]
- Bergh, B.V.D.; Michiels, J.E.; Fauvart, M.; Michiels, J. Should we develop screens for multi-drug antibiotic tolerance? Expert Rev. Anti-Infect. Ther. 2016, 14, 613–616. [Google Scholar] [CrossRef]
- Fisher, R.A.; Gollan, B.; Helaine, S. Persistent bacterial infections and persister cells. Nat. Rev. Genet. 2017, 15, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Van den Bergh, B.; Fauvart, M.; Michiels, J. Formation, physiology, ecology, evolution and clinical importance of bacterial persisters. FEMS Microbiol. Rev. 2017, 41, 219–251. [Google Scholar] [CrossRef] [PubMed]
- Levinson, T.; Dahan, A.; Novikov, A.; Paran, Y.; Berman, J.; Ben-Ami, R. Impact of tolerance to fluconazole on treatment response in Candida albicans bloodstream infection. Mycoses 2020, 64, 78–85. [Google Scholar] [CrossRef]
- Rosenberg, A.; Ene, I.V.; Bibi, M.; Zakin, S.; Segal, E.S.; Ziv, N.; Dahan, A.M.; Colombo, A.L.; Bennett, R.J.; Berman, J. Antifungal tolerance is a subpopulation effect distinct from resistance and is associated with persistent candidemia. Nat. Commun. 2018, 9, 1–14. [Google Scholar] [CrossRef]
- Scott, J.; Valero, C.; Mato-López, Á.; Donaldson, I.J.; Roldán, A.; Chown, H.; Van Rhijn, N.; Lobo-Vega, R.; Gago, S.; Furukawa, T.; et al. Aspergillus fumigatus Can Display Persistence to the Fungicidal Drug Voriconazole. Microbiol. Spectr. 2023, 11, e0477022. [Google Scholar] [CrossRef]
- Alcazar-Fuoli, L.; Mellado, E.; Alastruey-Izquierdo, A.; Cuenca-Estrella, M.; Rodriguez-Tudela, J.L. Aspergillus Section Fumigati: Antifungal Susceptibility Patterns and Sequence-Based Identification. Antimicrob. Agents Chemother. 2008, 52, 1244–1251. [Google Scholar] [CrossRef] [PubMed]
- Guinea, J. Updated EUCAST Clinical Breakpoints against Aspergillus, Implications for the Clinical Microbiology Laboratory. J. Fungi 2020, 6, 343. [Google Scholar] [CrossRef] [PubMed]
- Mellado, E.; Garcia-Effron, G.; Alcázar-Fuoli, L.; Melchers, W.J.G.; Verweij, P.E.; Cuenca-Estrella, M.; Rodríguez-Tudela, J.L. A New Aspergillus fumigatus Resistance Mechanism Conferring In Vitro Cross-Resistance to Azole Antifungals Involves a Combination of cyp51A Alterations. Antimicrob. Agents Chemother. 2007, 51, 1897–1904. [Google Scholar] [CrossRef]
- Garcia-Rubio, R.; Escribano, P.; Gomez, A.; Guinea, J.; Mellado, E. Comparison of Two Highly Discriminatory Typing Methods to Analyze Aspergillus fumigatus Azole Resistance. Front. Microbiol. 2018, 9, 1626. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Lopez, A.; Alcazar-Fuoli, L.; Bernal-Martínez, L. Simultaneous quantification of systemic azoles and their major metabolites in human serum by HPLC/PDA: Role of azole metabolic rate. Diagn. Microbiol. Infect. Dis. 2018, 92, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Young, J.-A.H.; El Jurdi, N.; Rayes, A.; MacMillan, M.L.; Holtan, S.G.; Cao, Q.; Witte, J.; Arora, M.; Weisdorf, D.J. Steroid-Sensitive, but Not Steroid-Dependent or Steroid-Resistant Acute Graft-versus-Host Disease, Results in Similar Infection Risk as No Graft-versus-Host Disease following Allogeneic Hematopoietic Cell Transplantation. Transplant. Cell. Ther. 2022, 28, 509.e1–509.e11. [Google Scholar] [CrossRef]
- Zeiser, R.; Polverelli, N.; Ram, R.; Hashmi, S.K.; Chakraverty, R.; Middeke, J.M.; Musso, M.; Giebel, S.; Uzay, A.; Langmuir, P.; et al. Ruxolitinib for Glucocorticoid-Refractory Chronic Graft-versus-Host Disease. N. Engl. J. Med. 2021, 385, 228–238. [Google Scholar] [CrossRef]
- Gómez-López, A. Antifungal therapeutic drug monitoring: Focus on drugs without a clear recommendation. Clin. Microbiol. Infect. 2020, 26, 1481–1487. [Google Scholar] [CrossRef]
- Kably, B.; Launay, M.P.; Derobertmasure, A.M.; Lefeuvre, S.P.; Dannaoui, E.M.; Billaud, E.M.P. Antifungal Drugs TDM: Trends and Update. Ther. Drug Monit. 2022, 44, 166–197. [Google Scholar] [CrossRef]
- Bosetti, D.; Neofytos, D. Invasive Aspergillosis and the Impact of Azole-resistance. Curr. Fungal Infect. Rep. 2023, 17, 77–86. [Google Scholar] [CrossRef]
- Alvarez-Perez, S.; Garcia, M.E.; Bouza, E.; Pelaez, T.; Blanco, J.L. Characterization of multiple isolates of Aspergillus fumigatus from patients: Genotype, mating type and invasiveness. Med. Mycol. 2009, 47, 601–608. [Google Scholar] [CrossRef] [PubMed]
- van der Torre, M.H.; Shen, H.; Rautemaa-Richardson, R.; Richardson, M.D.; Novak-Frazer, L. Molecular Epidemiology of Aspergillus fumigatus in Chronic Pulmonary Aspergillosis Patients. J. Fungi 2021, 7, 152. [Google Scholar] [CrossRef] [PubMed]
- de Valk, H.A.; Meis, J.F.G.M.; de Pauw, B.E.; Donnelly, P.J.; Klaassen, C.H.W. Comparison of Two Highly Discriminatory Molecular Fingerprinting Assays for Analysis of Multiple Aspergillus fumigatus Isolates from Patients with Invasive Aspergillosis. J. Clin. Microbiol. 2007, 45, 1415–1419. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Jimenez, I.; Garcia-Rubio, R.; Monzon, S.; Lucio, J.; Cuesta, I.; Mellado, E. Multiresistance to Nonazole Fungicides in Aspergillus fumigatus TR34/L98H Azole-Resistant Isolates. Antimicrob. Agents Chemother. 2021, 65, e0064221. [Google Scholar] [CrossRef]
- Rhodes, J.; Abdolrasouli, A.; Dunne, K.; Sewell, T.R.; Zhang, Y.; Ballard, E.; Brackin, A.P.; van Rhijn, N.; Chown, H.; Tsitsopoulou, A.; et al. Population genomics confirms acquisition of drug-resistant Aspergillus fumigatus infection by humans from the environment. Nat. Microbiol. 2022, 7, 663–674. [Google Scholar] [CrossRef]
- Melchio, M.; Mikulska, M.; Nadir, U.; Giacobbe, D.R.; Magnasco, L.; Limongelli, A.; Sepulcri, C.; Dentone, C.; Portunato, F.; Balletto, E.; et al. Lower blood levels of isavuconazole in critically ill patients compared to other populations: Possible need for TDM. Abstract O0217. ECCMID Copenhagen 15–18 April 2023. ECCMID eLibrary.
- Tissot, F.; Agrawal, S.; Pagano, L.; Petrikkos, G.; Groll, A.H.; Skiada, A.; Lass-Flörl, C.; Calandra, T.; Viscoli, C.; Herbrecht, R. ECIL-6 guidelines for the treatment of invasive candidiasis, aspergillosis and mucormycosis in leukemia and hematopoietic stem cell transplant patients. Haematologica 2017, 102, 433–444. [Google Scholar] [CrossRef]
- Stein, G.E.; Wells, E.M. The importance of tissue penetration in achieving successful antimicrobial treatment of nosocomial pneumonia and complicated skin and soft-tissue infections caused by methicillin-resistant Staphylococcus aureus: Vancomycin and linezolid. Curr. Med. Res. Opin. 2010, 26, 571–588. [Google Scholar] [CrossRef]
- Rodvold, K.A.; Yoo, L.; George, J.M. Penetration of Anti-Infective Agents into PulmonaryEpithelial Lining Fluid. Clin. Pharmacokinet. 2011, 50, 689–704. [Google Scholar] [CrossRef]
- Paterson, P.J.; Seaton, S.; Prentice, H.G.; Kibbler, C.C. Treatment failure in invasive aspergillosis: Susceptibility of deep tissue isolates following treatment with amphotericin B. J. Antimicrob. Chemother. 2003, 52, 873–876. [Google Scholar] [CrossRef]
- Schmitt-Hoffmann, A.-H.; Kato, K.; Townsend, R.; Potchoiba, M.J.; Hope, W.W.; Andes, D.; Spickermann, J.; Schneidkraut, M.J. Tissue Distribution and Elimination of Isavuconazole following Single and Repeat Oral-Dose Administration of Isavuconazonium Sulfate to Rats. Antimicrob. Agents Chemother. 2017, 61, e01292-17. [Google Scholar] [CrossRef]
- Danion, F.; Duval, C.; Séverac, F.; Bachellier, P.; Candolfi, E.; Castelain, V.; Clere-Jehl, R.; Denis, J.; Dillenseger, L.; Epailly, E.; et al. Factors associated with coinfections in invasive aspergillosis: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 1644–1651. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Isolate | Sample Type * | Day | MIC (mg/L) | Genotype | Persistence VRC | Persistence ISV | Resistance Mechanism | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TRESPERG | ||||||||||||||||
| AmB | ITC | VRC | POS | ISV | CSP | MP2 | CFEM | ERG4B | cyp51A | cyp51B | ||||||
| H-2067 | BAL | 1 | 0.5 | 0.5 | 0.5 | 0.06 | 1 | t02 | m1.1 | c09 | e05 | TYPE I | - | - | WT | WT |
| H-2099 | SP | 22 | 0.5 | 0.125 | 0.5 | 0.06 | 0.5 | t04A | m5.1 | c09 | e06 | TYPE II | - | - | WT | WT |
| H-2100 | 22 | 1 | 0.5 | 1 | 0.125 | 1 | t04A | m5.1 | c09 | e06 | TYPE II | - | - | WT | WT | |
| H-2101 | 22 | 1 | 0.5 | 0.5 | 0.06 | 1 | t03 | m1.1 | c07 | e07 | TYPE III | + | + | WT | WT | |
| H-2116 | SP | 29 | 0.5 | 0.5 | 0.5 | 0.03 | 1 | t03 | m1.1 | c07 | e13 | TYPE III | + | + | WT | WT |
| H-2117 | 29 | 0.5 | 0.25 | 0.5 | 0.03 | 1 | t11 | m1.8 | c07 | e13 | TYPE IV | + | + | WT | WT | |
| H-2133 | SP | 37 | 1 | 0.5 | 0.5 | 0.06 | 2 | t11 | m1.8 | c07 | e07 | TYPE IV | + | + | WT | WT |
| H-2134 | 37 | 0.5 | 0.125 | 0.5 | 0.03 | 0.5 | t03 | m1.1 | c07 | e07 | TYPE III | + | + | WT | WT | |
| H-2154 | SP | 43 | 1 | 0.5 | 1 | 0.06 | 1 | t03 | m1.1 | c07 | e07 | TYPE III | + | + | WT | WT |
| H-2155 | 43 | 1 | 0.125 | 0.5 | 0.03 | 0.5 | t03 | m1.1 | c07 | e07 | TYPE III | + | + | WT | WT | |
| H-2165 | TA | 52 | 1 | 0.5 | 1 | 0.06 | 1 | t03 | m1.1 | c07 | e07 | TYPE III | + | + | WT | WT |
| H-2173 | 52 | 1 | 0.125 | 0.5 | 0.03 | 0.5 | t03 | m1.1 | c07 | e07 | TYPE III | + | + | WT | WT | |
| H-2226 | BAL | 64 | 1 | 0.5 | 0.5 | 0.125 | 1 | t11 | m1.8 | c07 | e13 | TYPE IV | + | - | WT | WT |
| H-2285 | 64 | 1 | >8 | 8 | 0.5 | 8 | t10 | m1.1 | c07 | e05 | TYPE V | TR34/L98H | WT | |||
| Isolate | Sample Type * | Day | MIC (mg/L) | Genotype | Persistence VRZ | Persistence ISV | Resistance Mechanism | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TRESPERG | ||||||||||||||||
| AmB | ITC | VRC | POS | ISV | CSP | MP2 | CFEM | ERG4B | cyp51A | cyp51B | ||||||
| H-3161 | SP | 1 | 0.5 | 0.5 | 0.5 | 0.125 | 0.5 | t04A | m3.4 | c22b | e11 | TYPE I | - | - | WT | WT |
| H-3168 | SP | 6 | 0.5 | 0.5 | 0.5 | 0.125 | 0.5 | t04A | m3.4 | c22b | e11 | TYPE I | + | + | WT | WT |
| H-3178 | 6 | 0.5 | 0.5 | 0.5 | 0.25 | 1 | t04A | m3.4 | c22b | e11 | TYPE I | - | + | WT | WT | |
| H-3180 | SP | 12 | 0.5 | 0.5 | 0.5 | 0.125 | 0.5 | t04A | m3.4 | c22b | e11 | TYPE I | + | + | WT | WT |
| H-3181 | 12 | 0.5 | 0.5 | 0.25 | 0.125 | 0.25 | t02 | m5.1 | c08A | e11 | TYPE II | + | + | WT | WT | |
| H-3183 | 12 | 0.5 | 0.5 | 0.25 | 0.125 | 0.5 | t04A | m3.4 | c22b | e11 | TYPE I | - | + | WT | WT | |
| H-3184 | 12 | 0.5 | 0.5 | 0.5 | 0.125 | 0.5 | t04A | m3.4 | c22b | e11 | TYPE I | - | - | WT | WT | |
| H-3185 | 12 | 0.5 | 0.5 | 0.5 | 0.125 | 0.5 | t04A | m3.4 | c22b | e11 | TYPE I | - | - | WT | WT | |
| H-3192 | TA | 18 | 0.5 | 0.5 | 0.5 | 0.125 | 0.5 | t04A | m3.4 | c22b | e11 | TYPE I | - | + | WT | WT |
| H-3200 | TA | 29 | 0.5 | 0.5 | 0.25 | 0.125 | 0.5 | t04A | m3.4 | c22b | e11 | TYPE I | - | + | WT | WT |
| H-3201 | TA | 30 | 0.5 | 0.5 | 0.25 | 0.125 | 0.5 | t02 | m1.1 | c09 | e11 | TYPE III | + | + | WT | WT |
| H-3202 | 30 | 1 | 0.5 | 0.25 | 0.125 | 0.5 | t04A | m3.4 | c22b | e11 | TYPE I | - | + | WT | WT | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peláez-García de la Rasilla, T.; Mato-López, Á.; Pablos-Puertas, C.E.; González-Huerta, A.J.; Gómez-López, A.; Mellado, E.; Amich, J. Potential Implication of Azole Persistence in the Treatment Failure of Two Haematological Patients Infected with Aspergillus fumigatus. J. Fungi 2023, 9, 805. https://doi.org/10.3390/jof9080805
Peláez-García de la Rasilla T, Mato-López Á, Pablos-Puertas CE, González-Huerta AJ, Gómez-López A, Mellado E, Amich J. Potential Implication of Azole Persistence in the Treatment Failure of Two Haematological Patients Infected with Aspergillus fumigatus. Journal of Fungi. 2023; 9(8):805. https://doi.org/10.3390/jof9080805
Chicago/Turabian StylePeláez-García de la Rasilla, Teresa, Álvaro Mato-López, Clara E. Pablos-Puertas, Ana Julia González-Huerta, Alicia Gómez-López, Emilia Mellado, and Jorge Amich. 2023. "Potential Implication of Azole Persistence in the Treatment Failure of Two Haematological Patients Infected with Aspergillus fumigatus" Journal of Fungi 9, no. 8: 805. https://doi.org/10.3390/jof9080805