
Sporotrichosis in Older Adults: A Cohort Study of 911 Patients from a Hyperendemic Area of Zoonotic Transmission in Rio de Janeiro, Brazil
 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Location, Design, and Patients
2.2. Definitions
2.3. Patient Management
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Socio-Demographic and Epidemiological Characteristics
3.2. Clinical Forms
3.3. Hypersensitivity Reactions
3.4. Comorbidities and Concomitant Medication Use
3.5. Blood Alterations in Routine Laboratory Examinations
3.6. Serology for Sporotrichosis
3.7. Antifungal Treatment, Duration, and Adverse Events
3.8. Other Treatments and Procedures
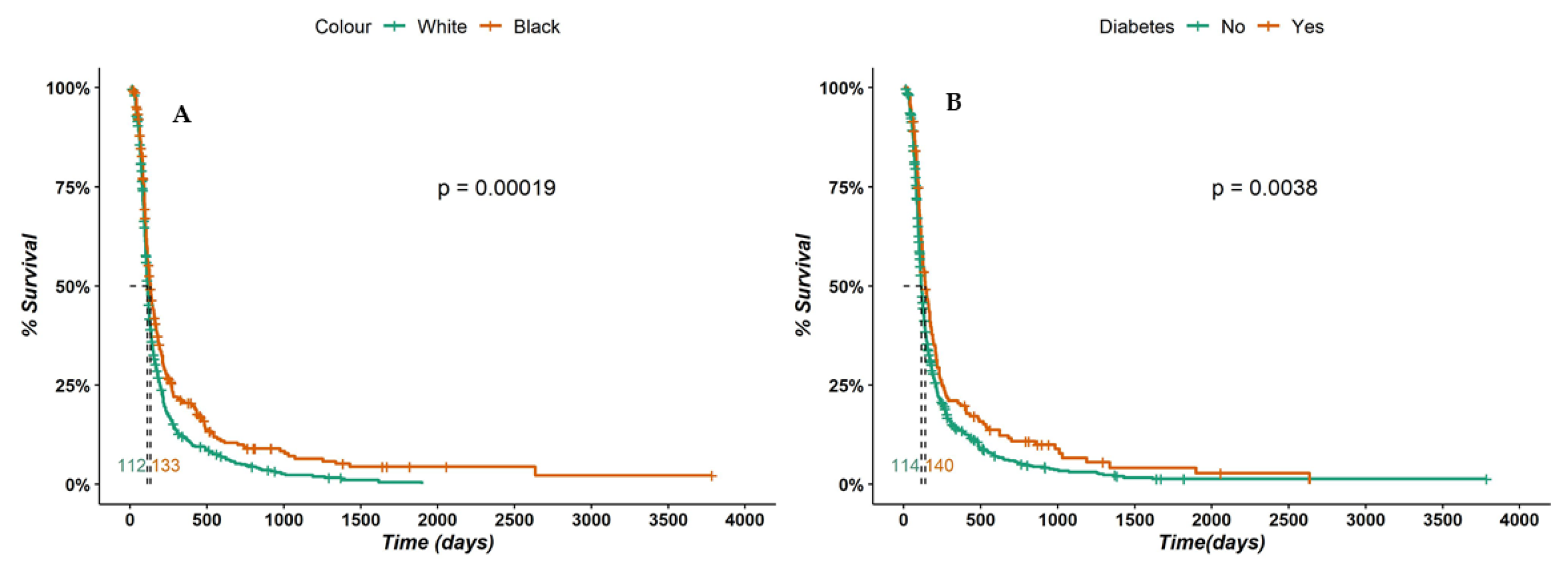
3.9. Outcomes and Survival Analysis
3.10. Recurrence and Reinfection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barros, M.B.; de Almeida-Paes, R.; Schubach, A.O. Sporothrix schenckii and Sporotrichosis. Clin. Microbiol. Rev. 2011, 24, 633–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Lima Barros, M.B.; de Oliveira Schubach, A.; do Valle, A.C.F.; Galhardo, M.C.G.; Conceição-Silva, F.; Schubach, T.M.P.; Reis, R.S.; Wanke, B.; Marzochi, K.B.F.; Conceição, M.J. Cat-Transmitted Sporotrichosis Epidemic in Rio de Janeiro. Brazil: Description of a Series of Cases. Clin. Infect. Dis. 2004, 38, 529–535. [Google Scholar] [CrossRef] [Green Version]
- Freitas, D.F.S.; Do Valle, A.C.F.; De Almeida Paes, R.; Bastos, F.I.; Galhardo, M.C.G. Zoonotic sporotrichosis in Rio de Janeiro. Brazil: A protracted Epidemic yet to be curbed. Clin. Infect. Dis. 2010, 50, 453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, M.B.T.; Costa, M.M.M.; Torres, C.C.S.; Galhardo, M.C.G.; do Valle, A.C.F.; Magalhães, M.A.F.M.; Sabroza, P.C.; de Oliveira, R.M. Esporotricose urbana: Epidemia negligenciada no Rio de Janeiro. Brasil. Cad. Saude Publica 2012, 28, 1867–1880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossow, J.A.; Queiroz-Telles, F.; Caceres, D.H.; Beer, K.D.; Jackson, B.R.; Pereira, J.G.; Gremião, I.D.F.; Pereira, S.A. A One Health Approach to Combatting Sporothrix brasiliensis: Narrative Review of an Emerging Zoonotic Fungal Pathogen in South America. J. Fungi 2020, 6, 247. [Google Scholar] [CrossRef]
- Thomson, P.; González, C.; Blank, O.; Ramírez, V.; Río, C.D.; Santibáñez, S.; Pena, P. Sporotrichosis Outbreak Due to Sporothrix brasiliensis in Domestic Cats in Magallanes, Chile: A One-Health-Approach Study. J. Fungi 2023, 9, 226. [Google Scholar] [CrossRef]
- Barnacle, J.R.; Chow, Y.J.; Borman, A.M.; Wyllie, S.; Dominguez, V.; Russell, K.; Roberts, H.; Armstrong-James, D.; Whittington, A.M. The first three reported cases of Sporothrix brasiliensis cat-transmitted sporotrichosis outside South America. Med. Mycol. Case Rep. 2022, 39, 14–17. [Google Scholar] [CrossRef]
- Arrillaga-Moncrieff, I.; Capilla, J.; Mayayo, E.; Marimon, R.; Marine, M.; Gene, J.; Cano, J.; Guarro, J. Different virulence levels of the species of Sporothrix in a murine model. Clin. Microbiol. Infect. 2009, 15, 651–655. [Google Scholar] [CrossRef] [Green Version]
- Freitas, D.F.S.; do Valle, A.C.F.; da Silva, M.B.T.; Campos, D.P.; Lyra, M.R.; de Souza, R.V.; Veloso, V.G.; Zancopé-Oliveira, R.M.; Bastos, F.I.; Galhardo, M.C.G. Sporotrichosis: An emerging neglected opportunistic infection in HIV-infected patients in Rio de Janeiro. Brazil. PLoS Negl. Trop. Dis. 2014, 8, e3110. [Google Scholar] [CrossRef]
- Falcão, E.M.M.; Pires, M.C.D.S.; Andrade, H.B.; Gonçalves, M.L.C.; Almeida-Paes, R.; Do Valle, A.C.F.; Bastos, F.I.; Gutierrez-Galhardo, M.C.; Freitas, D.F.S. Zoonotic sporotrichosis with greater severity in Rio de Janeiro. Brazil: 118 hospitalizations and 11 deaths in the last 2 decades in a reference institution. Med. Mycol. 2020, 58, 141–143. [Google Scholar] [CrossRef]
- Fichman, V.; Freitas, D.F.S.; do Valle, A.C.F.; de Souza, R.V.; Curi, A.L.L.; Valete-Rosalino, C.M.; de Macedo, P.M.; Varon, A.G.; Figueiredo-Carvalho, M.H.G.; Almeida-Silva, F.; et al. Severe Sporotrichosis Treated with Amphotericin B: A 20-Year Cohort Study in an Endemic Area of Zoonotic Transmission. J. Fungi 2022, 8, 469. [Google Scholar] [CrossRef] [PubMed]
- High, K.P. Infections in Older Adults. In Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases, 9th ed.; Bennett, J.E., Dolin, R., Blaser, M.J., Eds.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2019; pp. 24713–24750. [Google Scholar]
- Barbé-Tuana, F.; Funchal, G.; Schmitz, C.R.R.; Maurmann, R.M.; Bauer, M.E. The interplay between immunosenescence and age-related diseases. Semin. Immunopathol. 2020, 42, 545–557. [Google Scholar] [CrossRef]
- Franceschi, C.; Capri, M.; Monti, D.; Giunta, S.; Olivieri, F.; Sevini, F.; Panourgia, M.P.; Invidia, L.; Celani, L.; Scurti, M.; et al. Inflammaging and anti-inflammaging: A systemic perspective on aging and longevity emerged from studies in humans. Mech. Ageing Dev. 2007, 128, 92–105. [Google Scholar] [CrossRef]
- Shaw, A.C.; Goldstein, D.R.; Montgomery, R.R. Age-dependent dysregulation of innate immunity. Nat. Rev. Immunol. 2013, 13, 875–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walston, J.; Hadley, E.C.; Ferrucci, L.; Guralnik, J.M.; Newman, A.B.; Studenski, S.A.; Ershler, W.B.; Harris, T.; Fried, L.P. Research agenda for frailty in older adults: Toward a better understanding of physiology and etiology: Summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J. Am. Geriatr. Soc. 2006, 54, 991–1001. [Google Scholar] [CrossRef]
- Almeida-Paes, R.; Pimenta, M.A.; Pizzini, C.V.; Monteiro, P.C.; Peralta, J.M.; Nosanchuk, J.D.; Zancopé-Oliveira, R.M. Use of mycelial-phase Sporothrix schenckii exoantigens in an enzyme-linked immunosorbent assay for diagnosis of sporotrichosis by antibody detection. Clin. Vaccine Immunol. 2007, 14, 244–249. [Google Scholar] [CrossRef] [Green Version]
- Kauffman, C.A.; Bustamante, B.; Chapman, S.W.; Pappas, P.G. Clinical Practice Guidelines for the Management of Sporotrichosis: 2007 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2007, 45, 1255–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francesconi, G.; Valle, A.C.; Passos, S.; Reis, R.; Galhardo, M.C. Terbinafine (250 mg/day): An effective and safe treatment of cutaneous sporotrichosis. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 1273–1276. [Google Scholar] [CrossRef]
- Fichman, V.; do Valle, A.C.F.; Freitas, D.F.S.; Sampaio, F.M.S.; Lyra, M.R.; de Macedo, P.M.; Almeida-Paes, R.; de Oliveira, R.V.C.; Gutierrez-Galhardo, M.C. Cryosurgery for the treatment of cutaneous sporotrichosis: Experience with 199 cases. Br. J. Dermatol. 2019, 180, 1541–1542. [Google Scholar] [CrossRef]
- Kauffman, C.A. Fungal infections in older adults. Clin. Infect. Dis. 2001, 33, 550–555. [Google Scholar] [CrossRef]
- Suzman, R.; Beard, J.R.; Boerma, T.; Chatterji, S. Health in an ageing world—What do we know? Lancet 2015, 385, 484–486. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística. Agência de Notícias. Available online: https://agenciadenoticias.ibge.gov.br/agencia-noticias/2012-agencia-de-noticias/noticias/20980-numero-de-idosos-cresce-18-em-5-anos-e-ultrapassa-30-milhoes-em-2017 (accessed on 2 June 2023).
- Instituto Brasileiro de Geografia e Estatística. Agência de Notícias. Available online: https://agenciabrasil.ebc.com.br/geral/noticia/2016-10/brasil-tera-19-milhoes-de-idosos-com-mais-de-80-anos-em-2060-estima-ibge (accessed on 2 June 2023).
- Lloyd-Sherlock, P. Ageing. Development and Social Protection: Generalizations, Myths and Stereotypes. In Living Longer: Ageing, Development and Social Protection; Lloyd-Sherlock, P., Ed.; United Nations Research Institute for Social Development: London, UK, Zed Books: Nova York, NY, USA; 2004; ISBN 978-1-84277-356-7. [Google Scholar]
- Rex Pablo, C.; Rex, J.H.; Okhuysen, P.C. Sporothrix schenckii. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 9th ed.; Bennett, J.E., Dolin, R., Blaser, M.J., Eds.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2019; pp. 20979–21011. [Google Scholar]
- Laube, S. Skin infections and ageing. Ageing Res. Rev. 2004, 3, 69–89. [Google Scholar] [CrossRef] [PubMed]
- Sociedade Brasileira de Dermatologia. Envelhecimento: O Processo. Envelhecer com Saúde. Cuidados—SBD. Available online: https://www.sbd.org.br/doencas/envelhecimento/ (accessed on 31 May 2023).
- Almeida-Paes, R.; Marques, M.E.d.O.; Freitas, D.F.S.; do Valle, A.C.F.; Zancopé-Oliveira, M.R.; Gutierrez-Galhardo, M.C. Sporotrichosis in Rio de Janeiro. Brazil: Sporothrix brasiliensis is associated with atypical clinical presentations. PLoS Negl. Trop. Dis. 2014, 8, e3094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frontera, W.R. Physiologic Changes of the Musculoskeletal System with Aging: A Brief Review. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Fichman, V.; Mota-Damasceno, C.G.; Procópio-Azevedo, A.C.; Almeida-Silva, F.; de Macedo, P.M.; Medeiros, D.M.; Astacio, G.S.; Zancopé-Oliveira, R.M.; Almeida-Paes, R.; Freitas, D.F.S.; et al. Pulmonary Sporotrichosis Caused by Sporothrix brasiliensis: A 22-Year, Single-Center, Retrospective Cohort Study. J. Fungi 2022, 8, 536. [Google Scholar] [CrossRef]
- Aung, A.K.; Spelman, D.W.; Thompson, P.J. Pulmonary Sporotrichosis: An Evolving Clinical Paradigm. Semin. Respir. Crit. Care Med. 2015, 36, 756–766. [Google Scholar] [CrossRef]
- Queiroz-Telles, F.; Buccheri, R.; Benard, G. Sporotrichosis In Immunocompromised Hosts. J. Fungi 2019, 5, 8. [Google Scholar] [CrossRef] [Green Version]
- Mialski, R.; de Almeida, J.N., Jr.; da Silva, L.H.; Kono, A.; Pinheiro, R.L.; Teixeira, M.J.; Gomes, R.R.; de Queiroz-Telles, F.; Pinto, F.G.; Benard, G. Chronic Meningitis and Hydrocephalus due to Sporothrix brasiliensis in Immunocompetent Adults: A Challenging Entity. Open Forum Infect. Dis. 2018, 5, ofy081. [Google Scholar] [CrossRef]
- Lima, M.A.; Freitas, D.F.S.; Oliveira, R.V.C.; Fichman, V.; Varon, A.G.; Freitas, A.D.; Lamas, C.C.; Andrade, H.B.; Veloso, V.G.; Almeida-Paes, R.; et al. Meningeal Sporotrichosis Due to Sporothrix brasiliensis: A 21-Year Cohort Study from a Brazilian Reference Center. J. Fungi 2022, 9, 17. [Google Scholar] [CrossRef]
- Fichman, V.; Marques de Macedo, P.; Francis Saraiva Freitas, D.; do Valle, A.C.F.; Almeida-Silva, F.; Reis Bernardes-Engemann, A.; Zancopé-Oliveira, R.M.; Almeida-Paes, R.; Gutierrez-Galhardo, M.C. Zoonotic sporotrichosis in renal transplant recipients from Rio de Janeiro, Brazil. Transpl. Infect. Dis. 2021, 23, e13485. [Google Scholar] [CrossRef]
- Procópio-Azevedo, A.C.; Rabello, V.B.S.; Muniz, M.M.; Figueiredo-Carvalho, M.H.G.; Almeida-Paes, R.; Zancopé-Oliveira, R.M.; Silva, J.C.A.L.; de Macedo, P.M.; Valle, A.C.F.; Gutierrez-Galhardo, M.C.; et al. Hypersensitivity reactions in sporotrichosis: A retrospective cohort of 325 patients from a reference hospital in Rio de Janeiro. Brazil (2005–2018). Br. J. Dermatol. 2021, 185, 1272–1274. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.C.; Almeida-Paes, R.; Pizzini, C.V.; Gutierrez-Galhardo, M.C.; Freitas, D.F.S.; Zancopé-Oliveira, R.M. Diagnostic performance of mycologic and serologic methods in a cohort of patients with suspected sporotrichosis. Rev. Iberoam. Micol. 2019, 36, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Malafaia, G. Implicações da imunossenescência na vacinação de idosos. Rev Bras. Geriatr. Gerontol. 2008, 11, 433–441. [Google Scholar] [CrossRef] [Green Version]
- Da Veiga, A.M. Imunidade e Envelhecimento. In Tratado de Geriatria e Gerontologia; 5th E-Book; Freitas, E.V., Py, L., Eds.; Guanabara Koogan: Rio de Janeiro, Brasil, 2022; p. 4009. [Google Scholar]
- Wastesson, J.W.; Morin, L.; Tan, E.C.K.; Johnell, K. An update on the clinical consequences of polypharmacy in older adults: A narrative review. Expert Opin. Drug Saf. 2018, 17, 1185–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Lima Barros, M.B.; Schubach, A.O.; Oliveira, R.d.O.C.; Martins, E.B.; Teixeira, J.L.; Wanke, B. Treatment of cutaneous sporotrichosis with itraconazole—Study of 645 patients. Clin. Infect. Dis. 2011, 52, e200–e206. [Google Scholar] [CrossRef] [PubMed]
- Francesconi, G.; do Valle, A.C.F.; Passos, S.L.; Barros, M.L.B.; de Almeida Paes, R.; Curi, A.L.L.A.; Liporage, J.; Porto, C.F.; Gutierrez-Galhardo, M.C. Comparative Study of 250 mg/day Terbinafine and 100 mg/day Itraconazole for the Treatment of Cutaneous Sporotrichosis. Mycopathologia 2011, 171, 349–354. [Google Scholar] [CrossRef]
- Shi, S.; Klotz, U. Age-related changes in pharmacokinetics. Curr. Drug Metab. 2011, 12, 601–610. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística. Desigualdades Sociais por Cor ou Raça no Brasil. 2ª Edição. Estudos e Pesquisas. In: Informação Demográfica e Socioeconômica no 48. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv101972_informativo.pdf (accessed on 2 June 2023).
- Instituto de Pesquisa Econômica Aplicada; Tomasiello, D.B.; Bazzo, J.; Parga, J.; Servo, L.M.; Pereira, R.H.M. Desigualdades raciais e de Renda no Acesso à Saúde nas Cidades Brasileiras. 2021; 1st ed. Available online: https://repositorio.ipea.gov.br/bitstream/11058/11454/1/td_desigualdades_raciais_renda_publicacao_preliminar.pdf (accessed on 3 June 2023).
- Low Wang, C.C.; Hess, C.N.; Hiatt, W.R.; Goldfine, A.B. Clinical Update: Cardiovascular Disease in Diabetes Mellitus: Atherosclerotic Cardiovascular Disease and Heart Failure in Type 2 Diabetes Mellitus—Mechanisms, Management, and Clinical Considerations. Circulation 2016, 133, 2459–2502. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Status | n = 911 (100%) |
|---|---|---|
| Sex | Female | 666 (73.1) |
| Male | 245 (26.9) | |
| Skin color | White | 530 (62.1) |
| Black a | 323 (37.9) | |
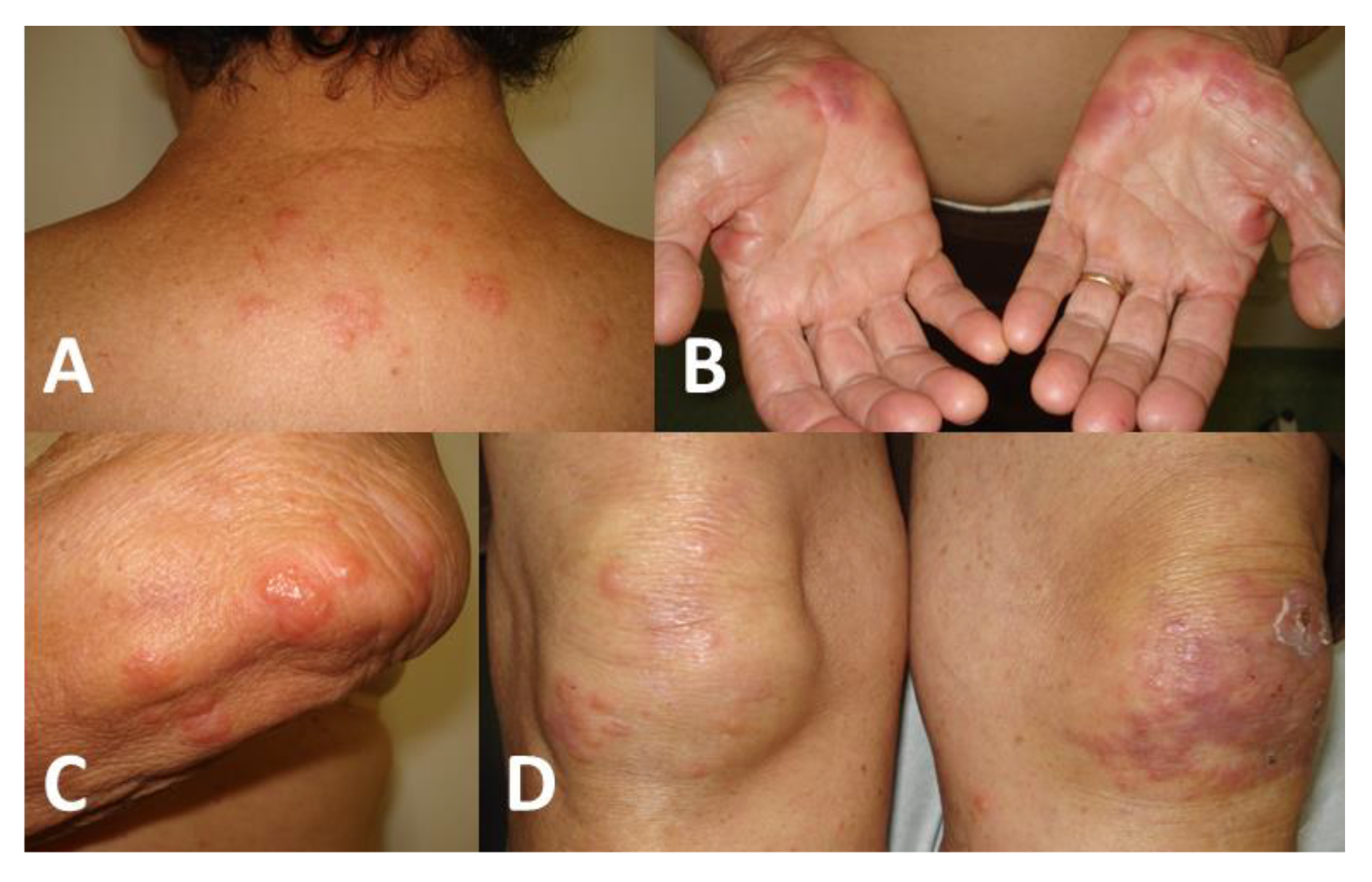
| Clinical presentation | Lymphocutaneous | 562 (62) |
| Fixed cutaneous | 233 (25.7) | |
| Cutaneous disseminated | 81 (8.9) | |
| Extracutaneous/Disseminated b | 30 (3.3) | |
| Organs affected c | Skin | 900 (99.3) |
| Osteoarticular | 19 (2.1) | |
| Ocular | 6 (0.7) | |
| Upper airways | 3 (0.3) | |
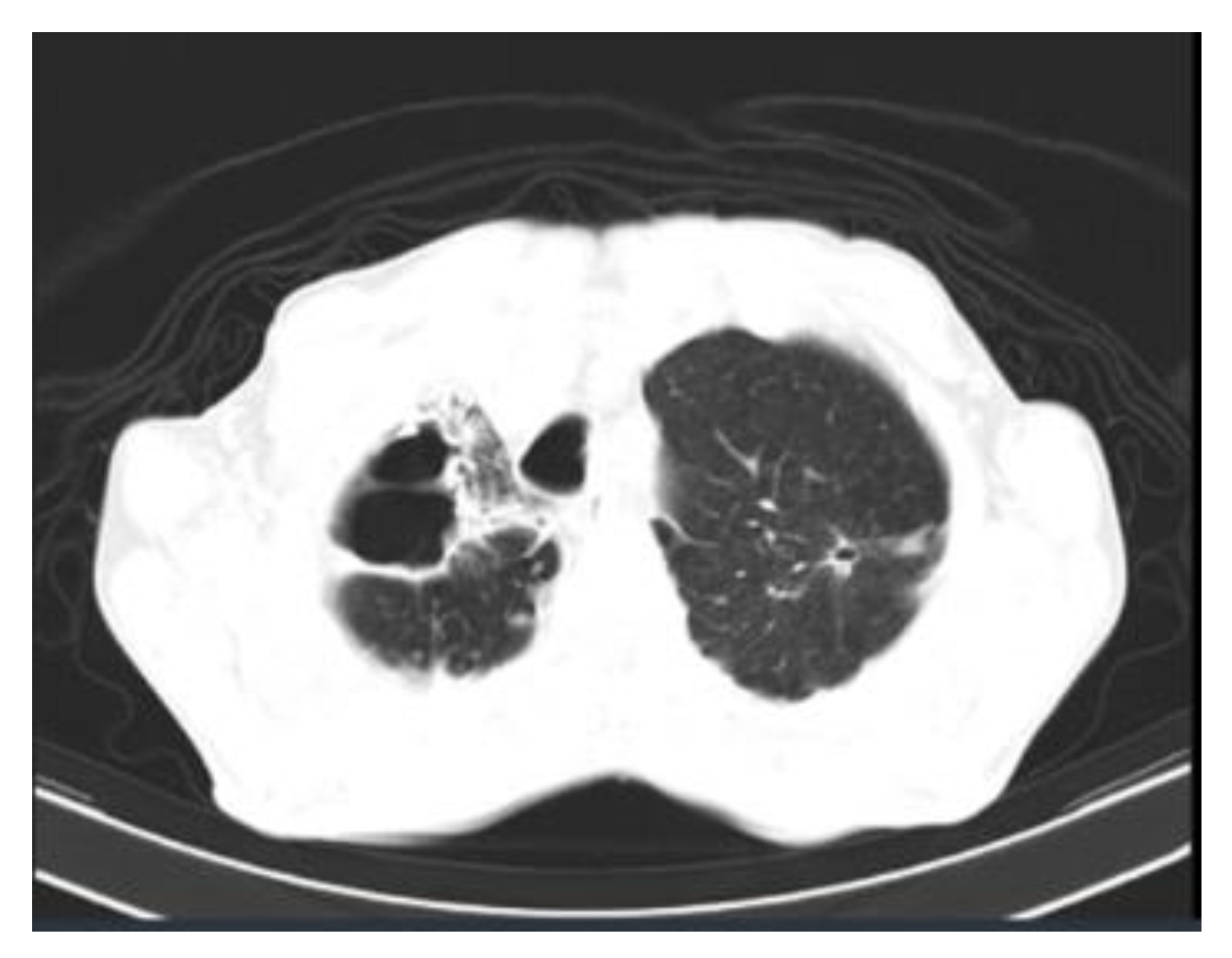
| Lungs | 3 (0.3) | |
| Hypersensitivity reactions | 25 (2.8) | |
| Comorbidities (number) | 1 | 376 (43.1) |
| 2 | 191 (21.9) | |
| 3 | 52 (5.9) | |
| ≥4 | 17 (1.9) | |
| Treatment | Itraconazole | 696 (81.1) |
| Terbinafine | 195 (22.7) | |
| Iodide solution | 5 (0.5) | |
| Amphotericin | 8 (0.9) | |
| Outcome | Cure | 795 (87.3) |
| Death due to sporotrichosis | 4 (0.4) | |
| Death due to other causes | 3 (0.3) | |
| Still under treatment | 3 (0.3) | |
| Lost to follow-up | 106 (11.6) |
| Variables | Status | |
|---|---|---|
| Unifocal extracutaneous sporotrichosis | ocular mucosa | 4 |
| nasal mucosa | 2 | |
| pulmonary | 2 | |
| arthritis | 1 | |
| Contiguity unifocal extracutaneous sporotrichosis | lymphocutaneous + osteomyelitis | 2 |
| fixed cutaneous + osteomyelitis | 2 | |
| lymphocutaneous + osteomyelitis + synovitis | 1 | |
| lymphocutaneous + synovitis | 3 | |
| Multifocal/disseminated sporotrichosis | disseminated skin lesions + osteomyelitis | 6 |
| disseminated skin lesions + osteomyelitis + tenosynovitis | 2 | |
| lymphocutaneous + ocular mucosa | 2 | |
| lymphocutaneous + nasal mucosa | 1 | |
| primary pulmonary sporotrichosis + wrist synovitis | 1 | |
| arthritis (in the knee and wrist) | 1 |
| Variables/Categories | HR | (95% CI) * | p-Value | aHR | (95% CI) * | p-Value | |
|---|---|---|---|---|---|---|---|
| Black skin color | Yes | 0.74 | (0.64–0.86) | p = 0.001 | 0.74 | (0.63–0.87) | p < 0.001 |
| Diabetes mellitus | Yes | 0.77 | (0.64–0.92) | p = 0.004 | 0.76 | (0.62–0.93) | p = 0.007 |
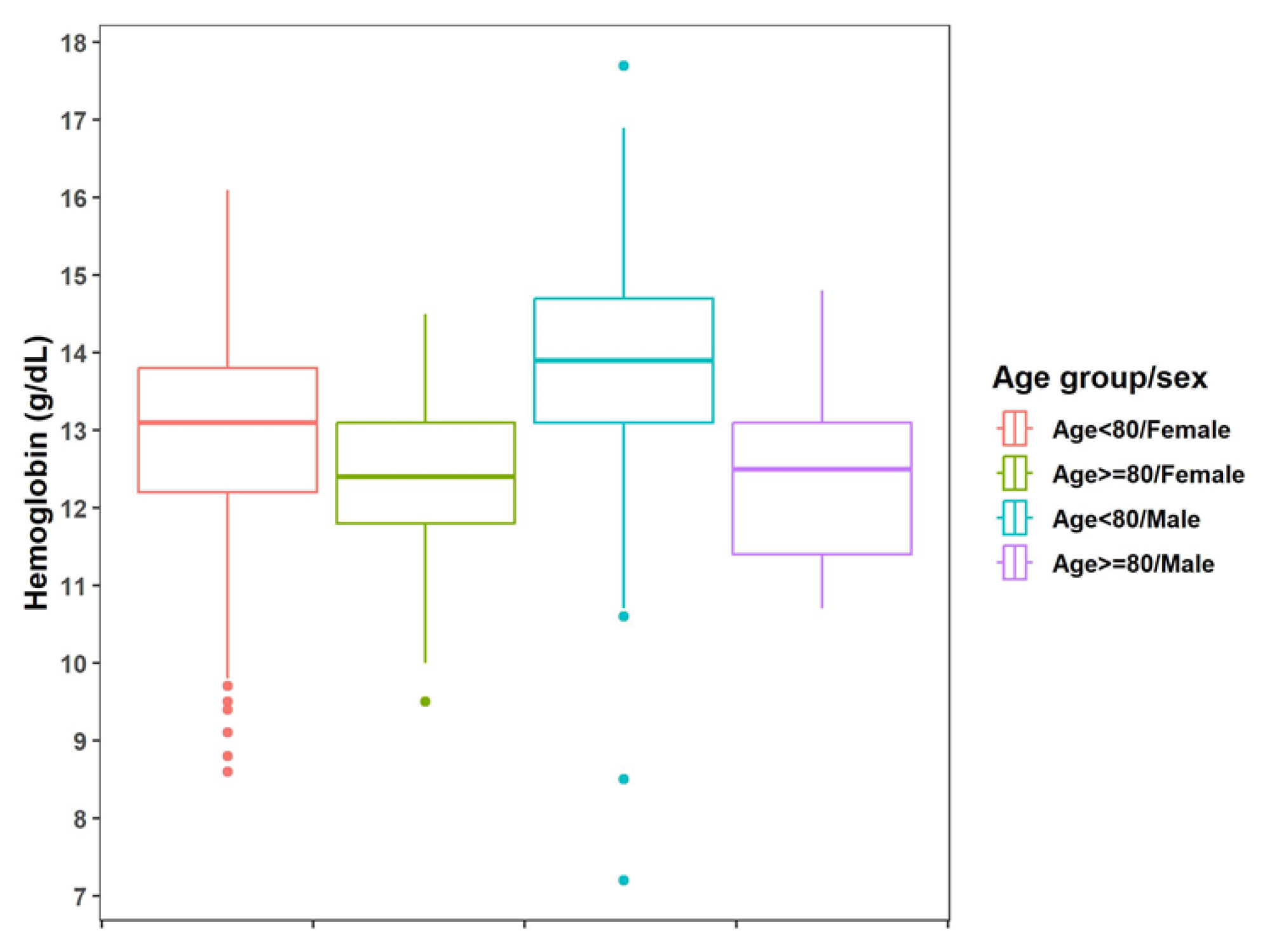
| Anemia | Yes | 0.80 | (0.66–0.97) | p = 0.023 | 0.84 | (0.69–1.03) | p = 0.086 |
| Age ≥ 80 years old | Yes | 0.87 | (0.68–1.12) | p = 0.286 | 0.83 | (0.62–1.10) | p = 0.187 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomes, R.d.S.R.; do Valle, A.C.F.; Freitas, D.F.S.; de Macedo, P.M.; Oliveira, R.d.V.C.; Almeida-Paes, R.; Zancopé-Oliveira, R.M.; Gutierrez-Galhardo, M.C. Sporotrichosis in Older Adults: A Cohort Study of 911 Patients from a Hyperendemic Area of Zoonotic Transmission in Rio de Janeiro, Brazil. J. Fungi 2023, 9, 804. https://doi.org/10.3390/jof9080804
Gomes RdSR, do Valle ACF, Freitas DFS, de Macedo PM, Oliveira RdVC, Almeida-Paes R, Zancopé-Oliveira RM, Gutierrez-Galhardo MC. Sporotrichosis in Older Adults: A Cohort Study of 911 Patients from a Hyperendemic Area of Zoonotic Transmission in Rio de Janeiro, Brazil. Journal of Fungi. 2023; 9(8):804. https://doi.org/10.3390/jof9080804
Chicago/Turabian StyleGomes, Rachel da Silva Ribeiro, Antonio Carlos Francesconi do Valle, Dayvison Francis Saraiva Freitas, Priscila Marques de Macedo, Raquel de Vasconcellos Carvalhaes Oliveira, Rodrigo Almeida-Paes, Rosely Maria Zancopé-Oliveira, and Maria Clara Gutierrez-Galhardo. 2023. "Sporotrichosis in Older Adults: A Cohort Study of 911 Patients from a Hyperendemic Area of Zoonotic Transmission in Rio de Janeiro, Brazil" Journal of Fungi 9, no. 8: 804. https://doi.org/10.3390/jof9080804