


Invasive Aspergillosis after Renal Transplantation

{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Incidence
1.2. Disease Burden (Mortality and Morbidity)
1.3. Risk Factors for IA in RT
1.4. Timing of Infection
1.5. Clinical Picture
1.6. Diagnosis
1.6.1. Histology, Direct Microscopic Examination, and Culture
1.6.2. Use of Galactomannan ELISA Assay
1.6.3. (1,3)-Beta-D-glucan
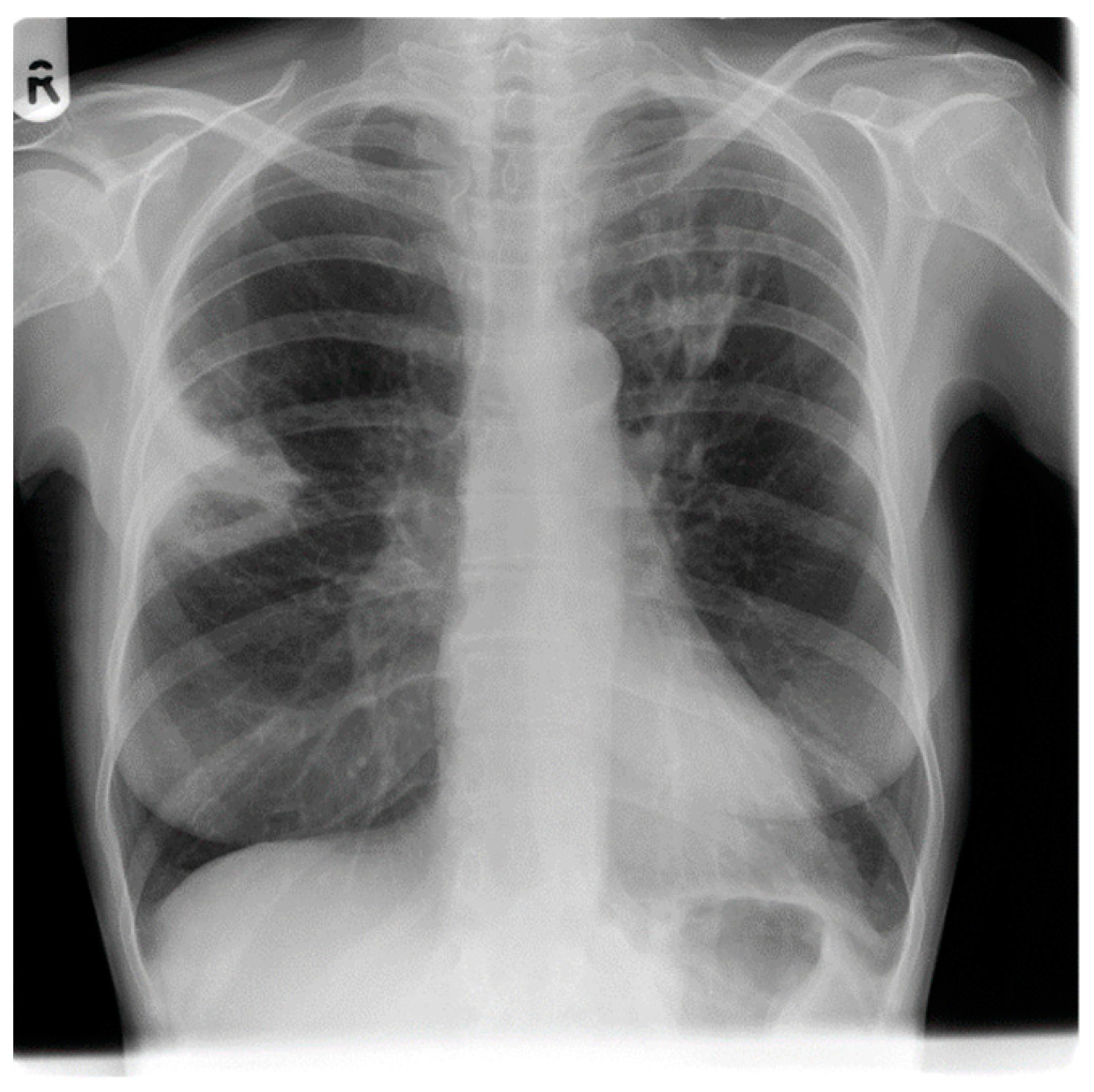
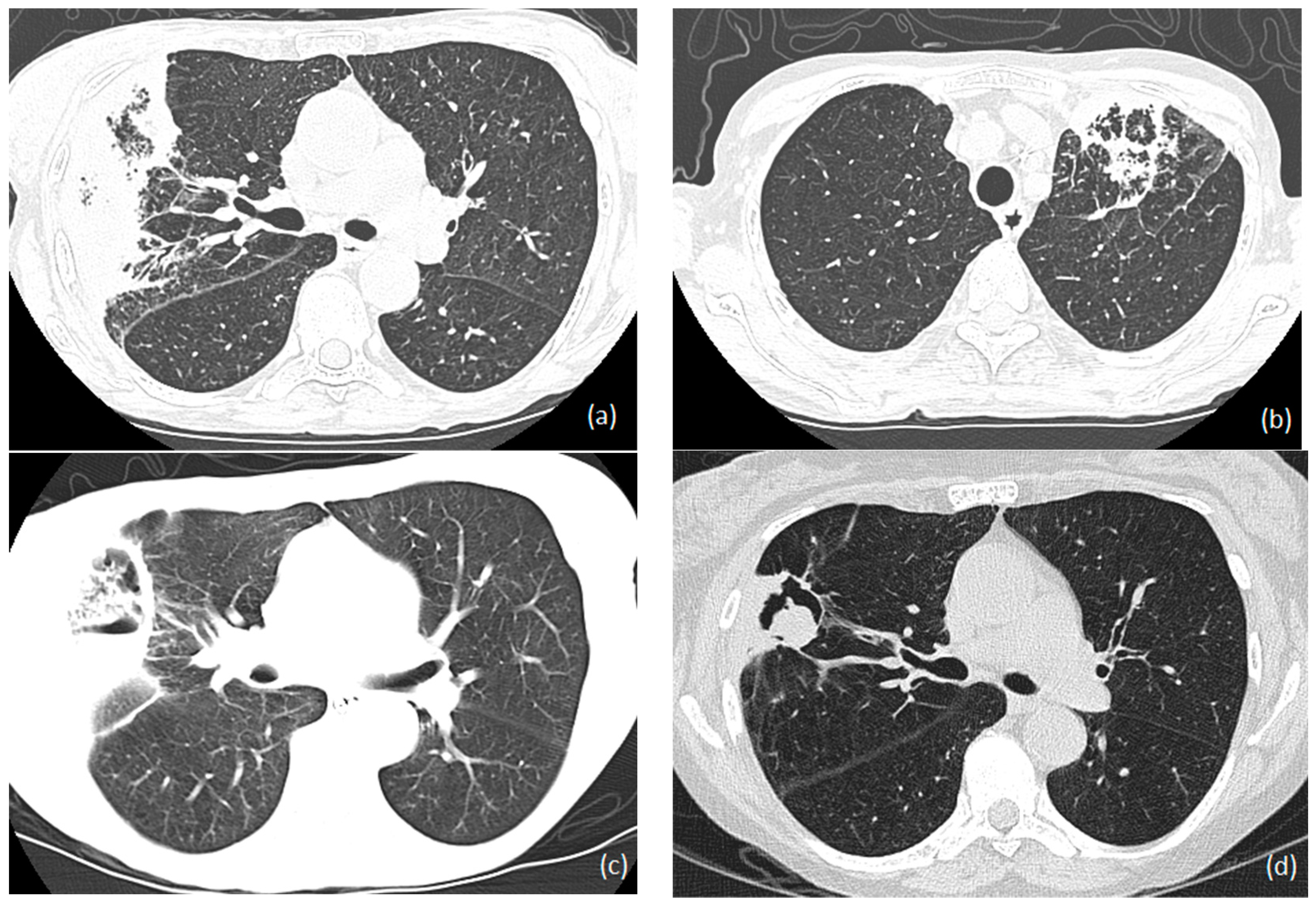
1.6.4. Radiology
1.7. Management
1.7.1. Antifungals
Voriconazole
Isavuconazole and Posaconazole
Itraconazole
Polyenes
Echinocandins
Combination of Antifungals
Duration of Antifungals
1.7.2. Surgical Treatment
1.7.3. Immunomodulation (GCSF/Gamma Interferon)
1.8. Prevention
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, Z.W.; Peng, F.H.; Yan, M.; Liang, W.; Liu, X.L.; Wu, Y.Q.; Lin, X.B.; Tan, S.L.; Wang, F.; Xu, P.; et al. Impact of CYP2C19 genotype and liver function on voriconazole pharmacokinetics in renal transplant recipients. Ther. Drug Monit. 2017, 39, 422–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seok, H.; Huh, K.; Cho, S.Y.; Kang, C.I.; Chung, D.R.; Huh, W.S.; Park, J.B.; Peck, K.R. Risk factors for development and mortality of invasive pulmonary Aspergillosis in kidney transplantation recipients. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1543–1550. [Google Scholar] [CrossRef] [PubMed]
- Mouloudi, E.; Massa, E.; Georgiadou, E.; Iosifidis, E.; Katsika, E.; Rembelakos, G.; Gakis, D.; Imvrios, G.; Papanikolaou, V.; Papadopoulos, S.; et al. Infections related to renal transplantation requiring intensive care admission: A 20-year study. Transplant. Proc. 2012, 44, 2721–2723. [Google Scholar] [CrossRef] [PubMed]
- López-Medrano, F.; Fernández-Ruiz, M.; Silva, J.T.; Carver, P.L.; van Delden, C.; Merino, E.; Pérez-Saez, M.J.; Montero, M.; Coussement, J.; de Abreu, M.M.; et al. Clinical presentation and determinants of mortality of invasive pulmonary aspergillosis in kidney transplant recipients: A multinational cohort study. Am. J. Transplant. 2016, 16, 3220–3234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Observatory on Donation and Transplantation. Available online: www.transplant-observatory.org/ (accessed on 11 January 2022).
- Vinod, P.B.; Sharma, R.K. Opportunistic infections (non-cytomegalovirus) in live related renal transplant recipients. Indian J. Urol. 2009, 25, 161–168. [Google Scholar]
- Balcan, B.; Ozcelik, U.; Ugurlu, A.O.; Aydin, M.; Nalcaci, S.; Yarbug, K.F. Increased mortality among renal transplant patients with invasive pulmonary aspergillus infection. Prog. Transplant. 2018, 28, 349–353. [Google Scholar] [CrossRef]
- Trabelsi, H.; Néji, S.; Sellami, H.; Yaich, S.; Cheikhrouhou, F.; Guidara, R.; Charffedine, K.; Makni, F.; Hachicha, J.; Ayadi, A. Invasive fungal infections in renal transplant recipients: About 11 cases. J. Mycol. Med. 2013, 23, 255–260. [Google Scholar] [CrossRef]
- Altiparmak, M.R.; Apaydin, S.; Trablus, S.; Serdengecti, K.; Ataman, R.; Ozturk, R.; Erek, E. Systemic fungal infections after renal transplantation. Scand. J. Infect. Dis. 2002, 34, 284–288. [Google Scholar] [CrossRef]
- López-Medrano, F.; Silva, J.T.; Fernández-Ruiz, M.; Carver, P.L.; van Delden, C.; Merino, E.; Pérez-Saez, M.J.; Montero, M.; Coussement, J.; de Abreu Mazzolin, M.; et al. Risk factors associated with early invasive pulmonary aspergillosis in kidney transplant recipients: Results from a multinational matched case–control study. Am. J. Transplant. 2016, 16, 2148–2157. [Google Scholar] [CrossRef] [Green Version]
- Trnacevic, S.; Mujkanovic, A.; Nislic, E.; Begic, E.; Karasalihovic, Z.; Cickusic, A.; Trnacevic, A.; Halilovic, M.A. Invasive Aspergillosis After Kidney Transplant–Treatment Approach. Med. Arch. 2018, 72, 456–458. [Google Scholar] [CrossRef]
- Heylen, L.; Maertens, J.; Naesens, M.; Van Wijngaerden, E.; Lagrou, K.; Bammens, B.; Claes, K.; Evenepoel, P.; Meijers, B.; Kuypers, D.; et al. Invasive aspergillosis after kidney transplant: Case-control study. Clin. Infect. Dis. 2015, 60, 1505–1511. [Google Scholar] [CrossRef] [PubMed]
- 13 Gavalda, J.; Len, O.; San Juan, R.; Aguado, J.M.; Fortun, J.; Lumbreras, C.; Moreno, A.; Munoz, P.; Blanes, M.; Ramos, A.; et al. Risk factors for invasive aspergillosis in solid-organ transplant recipients: A case-control study. Clin. Infect. Dis. 2005, 41, 52–59. [Google Scholar] [CrossRef] [Green Version]
- Abbott, K.C.; Hypolite, I.; Poropatich, R.K.; Hshieh, P.; Cruess, D.; Hawkes, C.A.; Agodoa, L.Y.; Keller, R.A. Hospitalizations for fungal infections after renal transplantation in the United States. Transpl. Infect. Dis. 2001, 3, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Kabir, V.; Maertens, J.; Kuypers, D. Fungal infections in solid organ transplantation: An update on diagnosis and treatment. Transplant. Rev. 2019, 33, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Kunthara, M.G.; Sahay, M.; Hussain, H.I.; Ismal, K.; Vali, P.S.; Kavadi, A.; Kumar, B.V. Posttransplant renal allograft dysfunction–A retrospective observational study. Indian J. Transplant. 2021, 15, 232–240. [Google Scholar]
- López-Medrano, F.; Fernández-Ruiz, M.; Silva, J.T.; Carver, P.L.; van Delden, C.; Merino, E.; Pérez-Saez, M.J.; Montero, M.; Coussement, J.; de Abreu, M.M.; et al. Multinational case-control study of risk factors for the development of late invasive pulmonary aspergillosis following kidney transplantation. Clin. Microbiol. Infect. 2018, 24, 192–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jha, V.; Chugh, S.; Chugh, K.S. Infections in dialysis and transplant patients in tropical countries. Kidney Int. 2000, 57, S85–S93. [Google Scholar] [CrossRef] [Green Version]
- Sadon, A.A.; Al Otaibi, T.; Nair, P.; Gheith, O.; Abd El, M.M.; Abd El, T.K.; Maher, A. Pulmonary complications within the first year after renal transplantation. Egypt. J. Chest Dis. Tuberc. 2020, 69, 739–746. [Google Scholar]
- Heylen, L.; Maertens, J.; Bammens, B.; Claes, K.; Evenepoel, P.; Meijers, B.; Naesens, M.; Kuypers, D.; Sprangers, B. Invasive aspergillosis after kidney transplantation: A monocentric retrospective experience. Acta Clin. Belg. 2015, 70, S3-1. [Google Scholar]
- Schelenz, S.; Goldsmith, D.J. Aspergillus endophthalmitis: An unusual complication of disseminated infection in renal transplant patients. J. Infect. 2003, 47, 336–343. [Google Scholar] [CrossRef]
- Coates, M.; Wilson, J. Central nervous system aspergillus infection complicating renal transplantation. Australas Radiol. 2001, 45, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24, e1–e38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von, E.M.; Roos, N.; Schulten, R.; Hesse, M.; Zühlsdorf, M.; Van de Loo, J. Pulmonary aspergillosis: Early diagnosis improves survival. Respiration 1995, 62, 341–347. [Google Scholar]
- Douglas, A.P.; Smibert, O.C.; Bajel, A.; Halliday, C.L.; Lavee, O.; McMullan, B.; Yong, M.K.; van Hal, S.J.; Chen, S.C.; Australasian Antifungal Guidelines Steering Committee, Slavin MA. Consensus guidelines for the diagnosis and management of invasive aspergillosis, 2021. Intern. Med. J. 2021, 51, 143–176. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W. Diagnosing pulmonary aspergillosis is much easier than it used to be: A new diagnostic landscape. Int. J. Tuberc. Lung Dis. 2021, 25, 525–536. [Google Scholar] [CrossRef]
- Brown, R.S., Jr.; Lake, J.R.; Katzman, B.A.; Ascher, N.L.; Somberg, K.A.; Emond, J.C.; Roberts, J.P. Incidence and significance of Aspergillus cultures following liver and kidney transplantation. Transplantation 1996, 61, 666–669. [Google Scholar] [CrossRef]
- Muthu, V.; Gandra, R.R.; Dhooria, S.; Sehgal, I.S.; Prasad, K.T.; Kaur, H.; Gupta, N.; Bal, A.; Ram, B.; Aggarwal, A.N.; et al. Role of flexible bronchoscopy in the diagnosis of invasive fungal infections. Mycoses 2021, 64, 668–677. [Google Scholar] [CrossRef]
- Küpeli, E.; Eyüboglu, F.Ö.; Haberal, M. Pulmonary infections in transplant recipients. Curr. Opin. Pulm. Med. 2012, 18, 202–212. [Google Scholar] [CrossRef]
- Patterson, T.F.; Thompson III, G.R.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef] [Green Version]
- Pfeiffer, C.D.; Fine, J.P.; Safdar, N. Diagnosis of invasive aspergillosis using a galactomannan assay: A meta-analysis. Clin. Infect. Dis. 2006, 42, 1417–1727. [Google Scholar] [CrossRef]
- Park, S.Y.; Yoon, J.A.; Kim, S.H. Voriconazole-refractory invasive aspergillosis. Korean J. Intern. Med. 2017, 32, 805–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoyo, I.; Sanclemente, G.; de la Bellacasa, J.P.; Cofán, F.; Ricart, M.J.; Cardona, M.; Colmenero, J.; Fernández, J.; Escorsell, A.; Navasa, M.; et al. Epidemiology, clinical characteristics, and outcome of invasive aspergillosis in renal transplant patients. Transpl. Infect. Dis. 2014, 16, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Mutschlechner, W.; Risslegger, B.; Willinger, B.; Hoenigl, M.; Bucher, B.; Eschertzhuber, S.; Lass-Flörl, C. Bronchoalveolar lavage fluid (1, 3) β-D-glucan for the diagnosis of invasive fungal infections in solid organ transplantation: A prospective multicenter study. Transplantation 2015, 99, e140–e144. [Google Scholar] [CrossRef]
- Estrada, C.; Desai, A.G.; Chirch, L.M.; Suh, H.; Seidman, R.; Darras, F.; Nord, E.P. Invasive aspergillosis in a renal transplant recipient successfully treated with interferon-gamma. Case Rep. Transplant. 2012, 2012, 1–5. [Google Scholar] [CrossRef]
- Ma, X.; Zhang, S.; Xing, H.; Li, H.; Chen, J.; Li, H.; Jiao, M.; Shi, Q.; Xu, A.; Xing, L.; et al. Invasive Pulmonary Aspergillosis Diagnosis via Peripheral Blood Metagenomic Next-Generation Sequencing. Front. Med. 2022, 9, 751617. [Google Scholar] [CrossRef] [PubMed]
- Rahatli, F.K.; Agildere, M.; Donmez, F.Y.; Can, U.; Benli, S.; Gulsen, S.; Altinors, N.; Haberal, M. Brain Computed Tomography and Magnetic Resonance Imaging in Neurological Complications of Liver and Kidney Transplantation. Transplantation 2018, 102, S640. [Google Scholar] [CrossRef]
- Denning, D.W. Therapeutic outcome in invasive aspergillosis. Clin. Infect. Dis. 1996, 23, 608–615. [Google Scholar] [CrossRef]
- Fernando, M.E.; Praveen, R.V.; Ishwarya, A. Modulation of maintenance immunosuppression during infection in renal transplant recipients. Indian J. Transplant. 2018, 12, 236–242. [Google Scholar]
- Li, Z.; Denning, D.W. The impact of corticosteroids on the outcome of fungal disease: A systematic review and meta-analysis. Curr. Fungal Infect. Rep. 2023; accepted, in press. [Google Scholar]
- Armstrong-James, D.; Teo, I.A.; Shrivastava, S.; Petrou, M.A.; Taube, D.; Dorling, A.; Shaunak, S. Exogenous interferon-γ immunotherapy for invasive fungal infections in kidney transplant patients. Am. J. Transplant. 2010, 10, 1796–1803. [Google Scholar] [CrossRef] [Green Version]
- Vanhove, T.; Bouwsma, H.; Hilbrands, L.; Swen, J.J.; Spriet, I.; Annaert, P.; Vanaudenaerde, B.; Verleden, G.; Vos, R.; Kuypers, D.R. Determinants of the magnitude of interaction between tacrolimus and voriconazole/posaconazole in solid organ recipients. Am. J. Transplant. 2017, 17, 2372–2380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herbrecht, R.; Denning, D.W.; Patterson, T.F.; Bennett, J.E.; Greene, R.E.; Oestmann, J.W.; Kern, W.V.; Marr, K.A.; Ribaud, P.; Lortholary, O.; et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N. Engl. J. Med. 2002, 347, 408–415. [Google Scholar] [CrossRef] [Green Version]
- Nivoix, Y.; Velten, M.; Letscher-Bru, V.; Moghaddam, A.; Natarajan-Amé, S.; Fohrer, C.; Lioure, B.; Bilger, K.; Lutun, P.; Marcellin, L.; et al. Factors associated with overall and attributable mortality in invasive aspergillosis. Clin. Infect. Dis. 2008, 47, 1176–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raad, I.I.; El Zakhem, A.; El Helou, G.; Jiang, Y.; Kontoyiannis, D.P.; Hachem, R. Clinical experience of the use of voriconazole, caspofungin or the combination in primary and salvage therapy of invasive aspergillosis in haematological malignancies. Int. J. Antimicrob. Agents 2015, 45, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Barchiesi, F.; Mazzocato, S.; Mazzanti, S.; Gesuita, R.; Skrami, E.; Fiorentini, A.; Singh, N. Invasive aspergillosis in liver transplant recipients: Epidemiology, clinical characteristics, treatment, and outcomes in 116 cases. Liver Transplant. 2015, 21, 204–212. [Google Scholar] [CrossRef]
- Denning, D.W. Comparison of 2 studies of treatment of invasive aspergillosis. Clin. Infect. Dis. 2007, 45, 1106–1108. [Google Scholar] [CrossRef] [Green Version]
- Vanstraelen, K.; Maertens, J.; Augustijns, P.; Lagrou, K.; de Loor, H.; Mols, R.; Annaert, P.; Malfroot, A.; Spriet, I. Investigation of saliva as an alternative to plasma monitoring of voriconazole. Clin. Pharmacokinet. 2015, 54, 1151–1160. [Google Scholar] [CrossRef]
- Maertens, J.A.; Raad, I.I.; Marr, K.A.; Patterson, T.F.; Kontoyiannis, D.P.; Cornely, O.A.; Bow, E.J.; Rahav, G.; Neofytos, D.; Aoun, M.; et al. Isavuconazole versus voriconazole for primary treatment of invasive mould disease caused by Aspergillus and other filamentous fungi (SECURE): A phase 3, randomised-controlled, non-inferiority trial. Lancet 2016, 387, 760–769. [Google Scholar] [CrossRef] [PubMed]
- Maertens, J.A.; Rahav, G.; Lee, D.G.; Ponce-de-León, A.; Sánchez, I.C.; Klimko, N.; Sonet, A.; Haider, S.; Vélez, J.D.; Raad, I.; et al. Posaconazole versus voriconazole for primary treatment of invasive aspergillosis: A phase 3, randomised, controlled, non-inferiority trial. Lancet 2021, 397, 499–509. [Google Scholar] [CrossRef]
- Ganesh, K.; Abi Abraham, M.; Kumar, J.S.; Simon, S. Invasive fungal diseases in renal transplantation-Case series. Indian J. Transplant. 2021, 15, 169–175. [Google Scholar] [CrossRef]
- Scanagatta, P.; Terzi, A.; Boschiero, L.; Cazzadori, A.; Lonardoni, A.; Calabrò, F. Invasive pulmonary aspergillosis after renal transplantation treated by surgery. Asian Cardiovasc. Thorac. Ann. 2004, 12, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Alkhunaizi, A.M.; Amir, A.A.; Al-Tawfiq, J.A. Invasive fungal infections in living unrelated renal transplantation. Transplant. Proc. 2005, 37, 3034–3037. [Google Scholar] [CrossRef]
- Parasuraman, R.; Samarapungavan, D.; Venkat, K.K. Updated principles and clinical caveats in the management of infection in renal transplant recipients. Transplant. Rev. 2010, 24, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Delsing, C.E.; Gresnigt, M.S.; Leentjens, J.; Preijers, F.; Frager, F.A.; Kox, M.; Monneret, G.; Venet, F.; Bleeker-Rovers, C.P.; van de Veerdonk, F.L.; et al. Interferon-gamma as adjunctive immunotherapy for invasive fungal infections: A case series. BMC Infect. Dis. 2014, 14, 166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopkins, C.C.; Weber, D.J.; Rubin, R.H. Invasive aspergillus infection: Possible non-ward common source within the hospital environment. J Hosp Infect. 1989, 13, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Neofytos, D.; Garcia-Vidal, C.; Lamoth, F.; Lichtenstern, C.; Perrella, A.; Vehreschild, J.J. Invasive aspergillosis in solid organ transplant patients: Diagnosis, prophylaxis, treatment, and assessment of response. BMC Infect. Dis. 2021, 21, 296. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sigera, L.S.M.; Denning, D.W. Invasive Aspergillosis after Renal Transplantation. J. Fungi 2023, 9, 255. https://doi.org/10.3390/jof9020255
Sigera LSM, Denning DW. Invasive Aspergillosis after Renal Transplantation. Journal of Fungi. 2023; 9(2):255. https://doi.org/10.3390/jof9020255
Chicago/Turabian StyleSigera, Liyanage Shamithra Madhumali, and David W. Denning. 2023. "Invasive Aspergillosis after Renal Transplantation" Journal of Fungi 9, no. 2: 255. https://doi.org/10.3390/jof9020255