
A Review of Antifungal Susceptibility Testing for Dermatophyte Fungi and It’s Correlation with Previous Exposure and Clinical Responses


Abstract
:1. Introduction
2. Material and Methods
3. Results
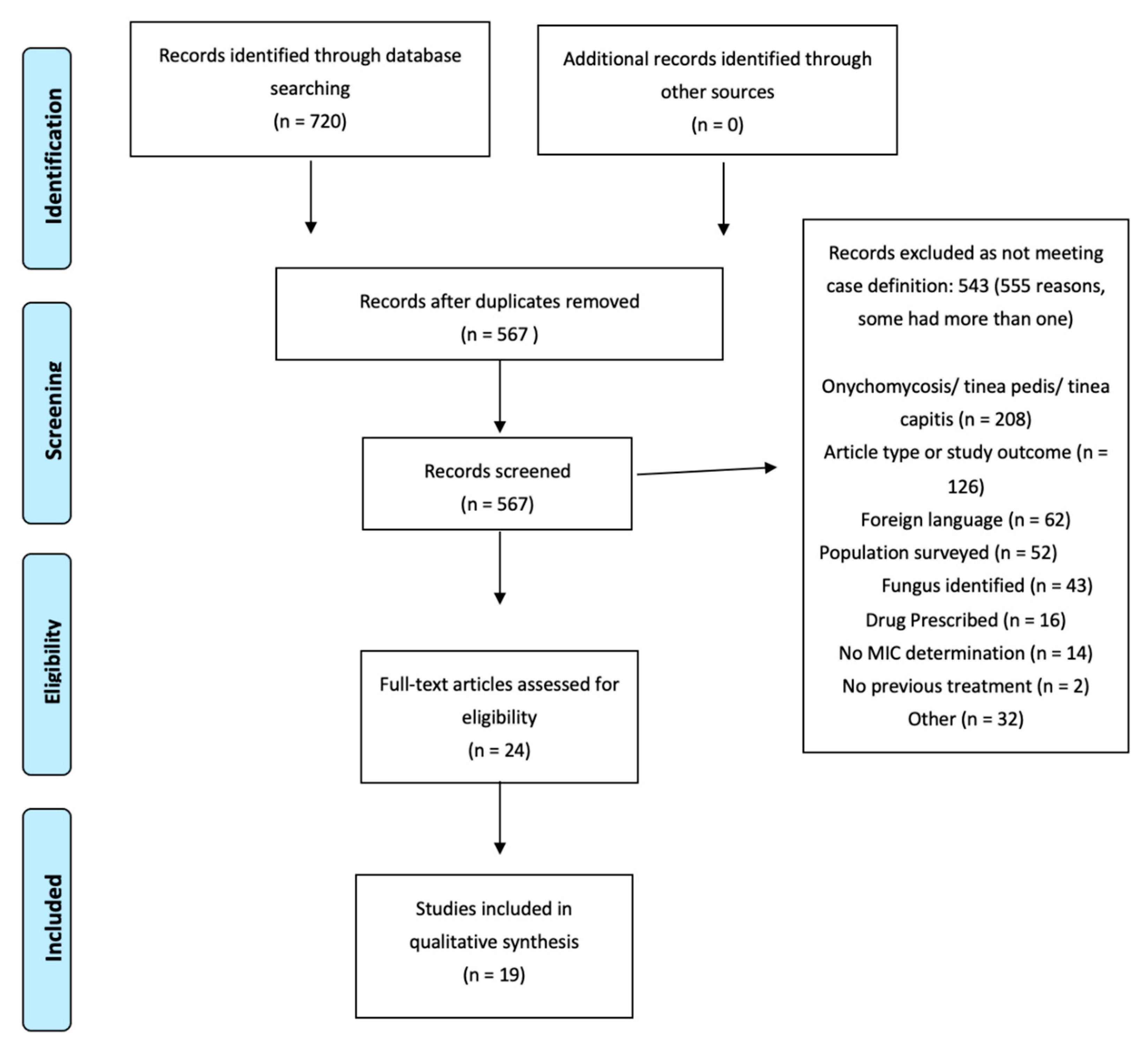
Literature Search
4. Discussion
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A
- (Dermatophytes AND/OR ringworm AND/OR tinea corporis) AND (resistance) AND (susceptibility test)
- (Dermatophytes AND/OR ringworm AND/OR tinea corporis) AND (treatment failure) AND (susceptibility test)
- (Dermatophytes AND/OR ringworm AND/OR tinea corporis) AND (resistance)
- (Dermatophytes AND/OR ringworm AND/OR tinea corporis) AND (treatment failure)
Appendix B
| Title | Authors | Journal |
| Terbinafine resistance in dermatophytes: Time to revisit alternate antifungal therapy | Gaurav, V.; Bhattacharya, S. N.; Sharma, N.; Datt, S.; Kumar, P.; Rai, G.; Singh, P. K.; Taneja, B.; Das, S.; | Journal De Mycologie Medicale—Volume 31, Issue 1, pp. 101087—published 2021-01-01 |
| Multidrug-resistant Trichophyton mentagrophytes genotype VIII in an Iranian family with generalized dermatophytosis: report of four cases and review of literature | Fattahi, Azam; Shirvani, Fariba; Ayatollahi, Azin; Rezaei-Matehkolaei, Ali; Badali, Hamid; Lotfali, Ensieh; Ghasemi, Reza; Pourpak, Zahra; Firooz, Alireza; | International Journal of Dermatology—Volume 60, Issue 6, pp. 686–692—published 2021-01-01 |
| Case of tinea corporis due to terbinafine-resistant Trichophyton interdigitale | Kakurai, Maki; Harada, Kazutoshi; Maeda, Tatsuo; Hiruma, Junichiro; Kano, Rui; Demitsu, Toshio; | The Journal of Dermatology—Volume 47, Issue 4, pp. e104–e105—published 2020-01-01 |
| Extensive Dermatophytosis Caused by Terbinafine-Resistant Trichophyton indotineae, France | Jabet, Arnaud; Brun, Sophie; Normand, Anne-Cecile; Imbert, Sebastien; Akhoundi, Mohammad; Dannaoui, Eric; Audiffred, Laeticia; Chasset, Francois; Izri, Arezki; Laroche, Liliane; Piarroux, Renaud; Bachmeyer, Claude; Hennequin, Christophe; Sabater, Alicia Moreno; | Emerging Infectious Diseases—Volume 28, Issue 1, pp. 229–233—published 2022-01-01 |
| Clinical Isolate of a Multi-Antifungal-Resistant Trichophyton rubrum | Kano, Rui; Kimura, Utako; Noguchi, Hiromitsu; Hiruma, Masataro; | Antimicrobial Agents and Chemotherapy—Volume 66, Issue 4, pp. e0239321—published 2022-01-01 |
| Griseofulvin-resistant dermatophytosis correlates with in vitro resistance | Artis, W. M.; Odle, B. M.; Jones, H. E.; | Archives of Dermatology—Volume 117, Issue 1, pp. 16–19—published 1981-01-01 |
| A new mutation in the SQLE gene of Trichophyton mentagrophytes associated to terbinafine resistance in a couple with disseminated tinea corporis | Hsieh, A.; Quenan, S.; Riat, A.; Toutous-Trellu, L.; Fontao, L.; | Journal De Mycologie Medicale—Volume 29, Issue 4, pp. 352–355—published 2019-01-01 |
| Correlation of In Vitro Susceptibility Based on MICs and Squalene Epoxidase Mutations with Clinical Response to Terbinafine in Patients with Tinea Corporis/Cruris | Khurana, Ananta; Masih, Aradhana; Chowdhary, Anuradha; Sardana, Kabir; Borker, Sagar; Gupta, Aastha; Gautam, R. K.; Sharma, P. K.; Jain, Dhruv; | Antimicrobial Agents and Chemotherapy—Volume 62, Issue 12, pp. e01038-18—published 2018-01-01 |
| Caution and warning: Arrival of terbinafine-resistant Trichophyton interdigitale of the Indian genotype, isolated from extensive dermatophytosis, in Japan | Kimura, Utako; Hiruma, Masataro; Kano, Rui; Matsumoto, Tadahiko; Noguchi, Hiromitsu; Takamori, Kenji; Suga, Yasushi; | The Journal of Dermatology—Volume 47, Issue 5, pp. e192–e193—published 2020-01-01 |
| Darier Disease Complicated by Terbinafine-resistant Trichophyton rubrum: A Case Report | Digby, Sanna S.; Hald, Marianne; Arendrup, Maiken C.; Hjort, Sofie V.; Kofoed, Kristian; | Acta Dermato-Venereologica—Volume 97, Issue 1, pp. 139–140—published 2017-01-01 |
| Antifungal susceptibility and genetic similarity of sequential isolates of Trichophyton rubrum from an immunocompetent patient with chronic dermatophytosis | Cordeiro, R. A.; Brilhante, R. S. N.; Rocha, M. F. G.; Rabenhorsch, S. H. B.; Moreira, J. L. B.; Grangeiro, T. B.; Sidrim, J. J. C.; | Clinical and Experimental Dermatology—Volume 31, Issue 1, pp. 122–124—published 2006-01-01 |
| Epidemiological study of terbinafine-resistant dermatophytes isolated from Japanese patients | Hiruma, Junichiro; Noguchi, Hiromitsu; Hase, Midori; Tokuhisa, Yumie; Shimizu, Tatsuya; Ogawa, Takasuke; Hiruma, Masataro; Harada, Kazutoshi; Kano, Rui; | The Journal of Dermatology—Volume 48, Issue 4, pp. 564–567—published 2021-01-01 |
| “Indian” strains of Trichophyton mentagrophytes with reduced itraconazole susceptibility in Germany | Brasch, Jochen; Gräser, Yvonne; Beck-Jendroscheck, Vera; Voss, Karen; Torz, Kaspar; Walther, Grit; Schwarz, Thomas; | Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology: JDDG—Volume 19, Issue 12, pp. 1723–1727—published 2021-01-01 |
| Trichophyton indotineae sp. nov.: A New Highly Terbinafine-Resistant Anthropophilic Dermatophyte Species | Kano, Rui; Kimura, Utako; Kakurai, Maki; Hiruma, Junichiro; Kamata, Hiroshi; Suga, Yasushi; Harada, Kazutoshi; | Mycopathologia—Volume 185, Issue 6, pp. 947–958—published 2020-01-01 |
| Tinea corporis caused by terbinafine-resistant Trichophyton rubrum successfully treated with fosravuconazole | Kitauchi, Yurie; Kumagai, Yoshiko; Inoue-Masuda, Yoko; Sugiura, Makoto; Sato, Tomotaka; Yaguchi, Takashi; Yokoyama, Tomoaki; | The Journal of Dermatology—Volume 48, Issue 7, pp. e329–e330—published 2021-01-01 |
| Rapid detection of terbinafine resistance in Trichophyton species by Amplified refractory mutation system-polymerase chain reaction | Shankarnarayan, Shamanth A.; Shaw, Dipika; Sharma, Arunima; Chakrabarti, Arunaloke; Dogra, Sunil; Kumaran, Muthu Sendhil; Kaur, Harsimran; Ghosh, Anup; Rudramurthy, Shivaprakash M.; | Scientific Reports—Volume 10, Issue 1, pp. 1297—published 2020-01-01 |
| Recurrent terbinafine resistant Trichophyton rubrum infection in a child with congenital ichthyosis | Schøsler, Louise; Andersen, Louise Kronborg; Arendrup, Maiken Cavling; Sommerlund, Mette; | Pediatric Dermatology—Volume 35, Issue 2, pp. 259–260—published 2018-01-01 |
| Emergence of Difficult-to-Treat Tinea Corporis Caused by Trichophyton mentagrophytes Complex Isolates, Paris, France | Dellière, Sarah; Joannard, Brune; Benderdouche, Mazouz; Mingui, Anselme; Gits-Muselli, Maud; Hamane, Samia; Alanio, Alexandre; Petit, Antoine; Gabison, Germaine; Bagot, Martine; Bretagne, Stéphane; | Emerging Infectious Diseases—Volume 28, Issue 1, pp. 224–228—published 2022-01-01 |
| Case of Terbinafine-Resistant Tinea Cruris Caused by Trichophyton tonsurans | Firooz, Alireza; Lotfali, Ensieh; Fattahi, Mahsa; Fattahi, Maryam; Miramin Mohammadi, Akram; Shahrzad Kavkani, Mahshid; | Case Reports in Dermatological Medicine—Volume 2021, Issue 0, pp. 9611072—published 2021-01-01 |
References
- Urban, K.; Chu, S.; Scheufele, C.; Giesey, R.L.; Mehrmal, S.; Uppal, P.; Delost, G.R. The global, regional, and national burden of fungal skin diseases in 195 countries and territories: A cross-sectional analysis from the Global Burden of Disease Study 2017. JAAD Int. 2020, 2, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Chacon, A.; Franca, K.; Fernandez, A.; Nouri, K. Psychosocial impact of onychomycosis: A review. Int. J. Dermatol. 2013, 52, 1300–1307. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.H.; Wong, E.T.; Yeung, C.K. Psychosocial perception of adults with onychomycosis: A blinded, controlled comparison of 1017 adult Hong Kong residents with or without onychomycosis. Biopsychosoc. Med. 2014, 81, 15. [Google Scholar]
- Shankarnarayan, S.A.; Shaw, D.; Sharma, A.; Chakrabarti, A.; Dogra, S.; Kumaran, M.S.; Kaur, H.; Ghosh, A.; Rudramurthy, S.M. Rapid detection of terbinafine resistance in Trichophyton species by Amplified refractory mutation system-polymerase chain reaction. Sci. Rep. 2020, 10, 1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sardana, K.; Gupta, A.; Sadhasivam, S.; Gautam, R.K.; Khurana, A.; Saini, S.; Gupta, S.; Ghosh, S. Checkerboard Analysis to Evaluate Synergistic Combinations of Existing Antifungal Drugs and Propylene Glycol Monocaprylate in Isolates from Recalcitrant Tinea Corporis and Cruris Patients Harboring Squalene Epoxidase Gene Mutation. Antimicrob Agents Chemother. 2021, 65, e0032121. [Google Scholar] [CrossRef]
- Shen, J.J.; Arendrup, M.C.; Verma, S.; Saunte, D.M.L. The Emerging Terbinafine-Resistant Trichophyton Epidemic: What Is the Role of Antifungal Susceptibility Testing? Dermatology 2022, 238, 60–79. [Google Scholar] [CrossRef]
- Astvad, K.M.T.; Hare, R.K.; Jørgensen, K.M.; Saunte, D.M.L.; Thomsen, P.K.; Arendrup, M.C. Increasing Terbinafine Resistance in Danish Trichophyton Isolates 2019–2020. J. Fungi 2022, 8, 150. [Google Scholar] [CrossRef]
- Siopi, M.; Efstathiou, I.; Theodoropoulos, K.; Pournaras, S.; Meletiadis, J. Molecular Epidemiology and Antifungal Susceptibility of Trichophyton Isolates in Greece: Emergence of Terbinafine-Resistant Trichophytonmentagrophytes Type VIII Locally and Globally. J. Fungi 2021, 7, 419. [Google Scholar] [CrossRef]
- Sacheli, R.; Hayette, M.P. Antifungal Resistance in Dermatophytes: Genetic Considerations, Clinical Presentations and Alternative Therapies. J. Fungi 2021, 7, 983. [Google Scholar] [CrossRef]
- Ebert, A.; Monod, M.; Salamin, K.; Burmester, A.; Uhrlaß, S.; Wiegand, C.; Hipler, U.-C.; Krüger, C.; Koch, D.; Wittig, F.; et al. Alarming India-wide phenomenon of antifungal resistance in dermatophytes: A multicentre study. Mycoses 2020, 63, 717–728. [Google Scholar] [CrossRef]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs for Antifungal Agents, Version 10.0. 2020. Available online: http://www.eucast.org/astoffungi/clinicalbreakpointsforantifungals/ (accessed on 11 March 2022).
- Wiederhold, N.P. Antifungal Susceptibility Testing: A Primer for Clinicians. Open Forum Infect Dis. 2021, 8, ofab444. [Google Scholar] [CrossRef] [PubMed]
- Dogra, S.; Shaw, D.; Rudramurthy, S. Antifungal Drug Susceptibility Testing of Dermatophytes: Laboratory Findings to Clinical Implications. Indian Derm. Online J. 2019, 10, 225. [Google Scholar]
- Aneke, C.I.; Rhimi, W.; Otranto, D.; Cafarchia, C. Comparative evaluation of E-test and CLSI methods for Itraconazole, Fluconazole and Ketoconazole susceptibilities of Microsporum canis strains. Mycopathologia 2020, 185, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Thatai, P.; Sapra, B. Critical review on retrospective and prospective changes in antifungal susceptibility testing for dermatophytes. Mycoses 2016, 59, 615–627. [Google Scholar] [CrossRef] [PubMed]
- Saunte, D.M.L.; Pereiro-Ferreirós, M.; Rodríguez-Cerdeira, C.; Sergeev, A.Y.; Arabatzis, M.; Prohić, A.; Piraccini, B.M.; Lecerf, P.; Nenoff, P.; Kotrekhova, L.P.; et al. Emerging antifungal treatment failure of dermatophytosis in Europe: Take care or it may become endemic. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1582–1586. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayyan. Available online: https://www.rayyan.ai/ (accessed on 31 July 2022).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Christenson, J.K.; Peterson, G.M.; Naunton, M.; Bushell, M.; Kosari, S.; Baby, K.E.; Thomas, J. Challenges and Opportunities in the Management of Onychomycosis. J. Fungi 2018, 4, 87. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, P.G. Hereditary palmoplantar keratoderma and dermatophytosis in the northernmost county of Sweden (Norrbotten). Acta Derm. Venereol. Suppl. 1994, 188, 57–60. [Google Scholar]
- Rengasamy, M.; Shenoy, M.M.; Dogra, S.; Asokan, N.; Khurana, A.; Poojary, S.; Jayaraman, J.; Valia, A.R.; Sardana, K.; Kolalapudi, S.; et al. Indian Association of Dermatologists, Venereologists and Leprologists (IADVL) Task Force against Recalcitrant Tinea (ITART) Consensus on the Management of Glabrous Tinea (INTACT). Indian Dermatol. Online J. 2020, 11, 502–519. [Google Scholar] [CrossRef]
- Robertson, M.H.; Rich, P.; Parker, F.; Hanifin, J.M. Ketoconazole in griseofulvin-resistant dermatophytosis. J. Am. Acad. Dermatol. 1982, 6, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Artis, W.M.; Odle, B.M.; Jones, H.E. Griseofulvin-resistant dermatophytosis correlates with in vitro resistance. Arch. Dermatol. 1981, 117, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Hay, R.J. Chronic dermatophyte infections. I. Clinical and mycological features. Br. J. Dermatol. 1982, 106, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kano, R.; Kimura, U.; Noguchi, H.; Hiruma, M. Clinical Isolate of a Multi-Antifungal-Resistant Trichophyton rubrum. Antimicrob Agents Chemother. 2022, 66, e0239321. [Google Scholar] [CrossRef] [PubMed]
- Digby, S.S.; Hald, M.; Arendrup, M.C.; Hjort, S.V.; Kofoed, K. Darier Disease Complicated by Terbinafine-resistant Trichophyton rubrum: A Case Report. Acta Derm.-Venereol. 2017, 97, 139–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schøsler, L.; Andersen, L.K.; Arendrup, M.C.; Sommerlund, M. Recurrent terbinafine resistant Trichophyton rubrum infection in a child with congenital ichthyosis. Pediatr. Dermatol. 2018, 35, 259–260. [Google Scholar] [CrossRef]
- Dellière, S.; Joannard, B.; Benderdouche, M.; Mingui, A.; Gits-Muselli, M.; Hamane, S.; Alanio, A.; Petit, A.; Gabison, G.; Bagot, M.; et al. Emergence of Difficult-to-Treat Tinea Corporis Caused by Trichophyton mentagrophytes Complex Isolates, Paris, France. Emerg. Infect. Dis. 2022, 28, 224–228. [Google Scholar] [CrossRef]
- Lanternier, F.; Pathan, S.; Vincent, Q.B.; Liu, L.; Cypowyj, S.; Prando, C.; Migaud, M.; Taibi, L.; Ammar-Khodja, A.; Stambouli, O.B.; et al. Deep Dermatophytosis and Inherited CARD9 Deficiency. N. Engl. J. Med. 2013, 369, 1704–1714. [Google Scholar] [CrossRef] [Green Version]
- Rex, J.H.; Pfaller, M.A. Has antifungal susceptibility testing come of age? Clin. Infect. Dis. 2002, 35, 982–989. [Google Scholar] [CrossRef] [Green Version]
- Arendrup, M.C.; Kahlmeter, G.; Guinea, J.; Meletiadis, J. Subcommittee on Antifungal Susceptibility Testing (AFST) of the ESCMID European Committee for Antimicrobial Susceptibility Testing EUCAST. How to: Perform antifungal susceptibility testing of microconidia-forming dermatophytes following the new reference EUCAST method E.Def 11.0, exemplified by Trichophyton. Clin. Microbiol. 2021, 27, 55–60. [Google Scholar]
- Chowdhary, A.; Singh, A.; Kaur, A.; Khurana, A. The emergence and worldwide spread of the species Trichophyton indotineae causing difficult-to-treat dermatophytosis: A new challenge in the management of dermatophytosis. PLoS Pathog. 2022, 18, e1010795. [Google Scholar] [CrossRef] [PubMed]
- WHO. Fungal Priority Pathogens List to Guide Research, Development and Public Health Action. 2022. Available online: https://www.who.int/publications/i/item/9789240060241 (accessed on 11 March 2022).


{kind=link}
| Total (n = 75) | Gender F/M/NA | Mean Age in Years (Range) | Contact with India/Asia n/Total (%) | Contact with Middle East | Disease Duration in Months (Range) or Chronic | Mutation |
|---|---|---|---|---|---|---|
| T. indotineae (n = 9) | NA | NA | 9/9 (100) Bangladesh (n = 6) Myanmar (n = 1 Japan (n = 2) | NA (n = 9) | L393S (n = 2) F397L (n = 4) A448T (n = 2) No mutation (n = 1) | |
| T. mentagrophytes/interdigitale (n = 4) | 1/1/2 | 24.5 (22–27) NA (n = 2) | 4/4 (100) India (n = 3) Nepal & India (n = 1) | 15.5 (7–24) Chronic (n = 0) NA (n = 2) | F397L (n = 4) | |
| T. mentagrophytes ITS type VIII (n = 20) | 11/9/0 | 39.4 (4–64) | India (n = 15) Bangladesh (n = 3) Sri Lanka (n = 1) | Iran (n = 4) Yemen (n = 1) | 7.9 (3–12) Chronic (n = 0) NA (n = 11) | F397L (n = 11) A448T (n = 2) c.1342G > A in the SQLE (n = 2) L393S (n = 1) n A1223T (n = 2) No mutation (n = 2) Two mutations (n = 1) |
| T. interdigitale (n = 11) | 0/1/10 | 47 (–) NA (n = 10) | India (n = 11) | NA (n = 11) | F397L (n = 7) L393F (n = 2) No mutation (n = 2) | |
| T. rubrum (n = 29) | 5/24/0 | 40.8 (9–81) NA (n = 1) | Japan (n = 1) | 65.0 (24–138) Chronic (n = 25) NA (n = 0) | ||
| T. tonsurans (n = 2) | 0/2/0 | 25.5 (25–26) NA (n = 0) | Iran (n = 2) | 12(–) Chronic (n = 0) NA (n = 1) |
| Terbinafine | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Species | MIC Value mg/L | 0.016 | 0.03 | 0.06 | 0.125 | 0.25 | 0.5 | 1 | 2 | 4 | 8 | >8 |
| T. indotineae (16) | Yes | 2 | 1 | 3 | 4 | 1 | ||||||
| No | 1 | 1 | 3 | |||||||||
| T. rubrum (2) | Yes | 1 | 1 | |||||||||
| No | ||||||||||||
| Itraconazole | ||||||||||||
| Species (n) | MIC value mg/L | 0.016 | 0.03 | 0.06 | 0.125 | 0.25 | 0.5 | 1 | 2 | 4 | 8 | >8 |
| T. indotineae (14) | Yes | 1 | ||||||||||
| No | 3 | 7 | 2 | 1 | ||||||||
| T. rubrum (2) | Yes | |||||||||||
| No | 1 | 1 | ||||||||||
| Terbinafine | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Species | MIC Value mg/L | 0.015 | 0.0625 | 0.03 | 0.06 | 0.125 | 0.25 | 0.5 | 1 | >1 | 2 | 4 | 8 | >8 | 16 | ≥32 |
| T. indotineae | Yes | 1 | 2 | 2 | 1 | 1 | 3 | 2 | ||||||||
| No | 1 | |||||||||||||||
| T. menta/inter complex | Yes | 2 | 2 | 1 | 1 | 9 | ||||||||||
| No | ||||||||||||||||
| T. rubrum | Yes | 3 | ||||||||||||||
| No | ||||||||||||||||
| T. tonsurans | Yes | 2 | ||||||||||||||
| No | ||||||||||||||||
| Itraconazole | ||||||||||||||||
| Species | MIC value mg/L | 0.015 | 0.0625 | 0.03 | 0.06 | 0.125 | 0.25 | 0.5 | 1 | >1 | 2 | 4 | 8 | >8 | 16 | ≥32 |
| T. indotineae | Yes | |||||||||||||||
| No | 2 | 4 | 1 | 1 | 1 | 3 | 1 | |||||||||
| T. menta/inter complex | Yes | |||||||||||||||
| No | 2 | 2 | ||||||||||||||
| T. rubrum | Yes | |||||||||||||||
| No | 1 | 1 | 1 | 1 | ||||||||||||
| T. tonsurans | Yes | |||||||||||||||
| No | 2 | |||||||||||||||
| Griseofulvin | ||||||||||||||||
| Species | MIC value mg/L | 0.015 | 0.0625 | 0.03 | 0.06 | 0.125 | 0.25 | 0.5 | 1 | >1 | 2 | 4 | 8 | >8 | 16 | ≥32 |
| T. menta/inter complex | Yes | |||||||||||||||
| No | 1 | 3 | 1 | 1 | ||||||||||||
| T. rubrum | Yes | |||||||||||||||
| No | 1 | 1 | ||||||||||||||
| MIC Value mg/L | 0.5 | 1 | 2 | 3 | 4 | 5 | 6 | 9 | >18 |
|---|---|---|---|---|---|---|---|---|---|
| Griseofulvin | |||||||||
| Yes | 1 | 4 | 2 | 3 | 3 | 3 | 2 | 1 | 2 |
| No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, S.S.; Hay, R.J.; Saunte, D.M.L. A Review of Antifungal Susceptibility Testing for Dermatophyte Fungi and It’s Correlation with Previous Exposure and Clinical Responses. J. Fungi 2022, 8, 1290. https://doi.org/10.3390/jof8121290
Khan SS, Hay RJ, Saunte DML. A Review of Antifungal Susceptibility Testing for Dermatophyte Fungi and It’s Correlation with Previous Exposure and Clinical Responses. Journal of Fungi. 2022; 8(12):1290. https://doi.org/10.3390/jof8121290
Chicago/Turabian StyleKhan, Sidra Saleem, Roderick James Hay, and Ditte Marie Lindhardt Saunte. 2022. "A Review of Antifungal Susceptibility Testing for Dermatophyte Fungi and It’s Correlation with Previous Exposure and Clinical Responses" Journal of Fungi 8, no. 12: 1290. https://doi.org/10.3390/jof8121290