1. Introduction
Fungal keratitis (FK) is an opportunistic corneal infection of fungi predisposed by corneal surface trauma [
1]. According to the Asia Cornea Society Infectious Keratitis Study (ACS IKS) [
2], FK was one of the most common microbial keratitis (MK), which was secondary to bacterial keratitis (BK) (FK:BK = 33%:38%). In addition, they found that trauma was the most common risk factor for MK. However, FK is easily overlooked due to its relatively sluggish progressive course. In addition, less intense pain in the early phase [
3] often leads to longer delay before seeking medical care, which results in a worse visual outcome than BK. Previous reports showed clinical diagnosis of FK is highly challenging [
4,
5]. The sensitivity and specificity of clinical diagnosis of FK were 38% and 45%, respectively [
4]. Even for an experienced corneal physician, the diagnostic accuracy via slit lamp image was only about 76% [
6]. Consequently, about 12 to 58% of FK patients needed therapeutic keratoplasty or other surgeries to quiet down their infection episodes [
7,
8,
9], and the surgical cure rate of FK was the worst among various MKs [
10]. Finally, up to 25% of FK patients might lose their vision [
11].
Among the 2831 isolated microorganisms in the ACS IKS [
2], the top 3 pathogens were
Fusarium spp. (18%),
Pseudomonas spp. (10%), and
Aspergillus spp. (8%). A recent comprehensive review confirmed
Fusarium and
Aspergillus as FK’s most common fungal isolates globally [
11]. FK responds poorly to anti-fungal agents once the deep invasion of fungi occurs, which is why early diagnosis of FK is crucial. If diagnosis and treatment are made early, polyenes and azoles were active against
Fusarium spp. and
Aspergillus spp., respectively [
12]. Moreover, the Mycotic Ulcer Treatment Trial (MUTT) also found that
Fusarium spp. were least susceptible to voriconazole, whereas
Aspergillus spp. were least susceptible to natamycin [
13,
14]. For advanced FK shown in MUTT 2, by adjunctive oral voriconazole to topical natamycin, only
Fusarium keratitis cases may get better visual outcome [
15]. Furthermore, compared to other
Fusarium spp.,
F. solani has been shown to have higher voriconazole resistance and a worse visual outcome [
16]. The evidence above suggests that the overall prognosis of FK will be increased by prompt diagnosis of FK, differentiation of
Fusarium and
Aspergillus, and identification of critical fungal species such as
F. solani.
We previously developed a dot hybridization array (DHA) for rapid diagnosis of FK, of which this assay provided much higher sensitivity than that of the culture [
17]. This assay was accomplished by amplifying the internal transcribed spacer region (ITS) that contained the target gene (5.8 S rRNA gene) by polymerase chain reaction (PCR), followed by hybridization of the PCR amplicon to a fungus-specific oligonucleotide probe immobilized on a nylon membrane. It can detect fungi in the corneal scrapes within a shorter turnaround time (one working day) than that of the culture. Based on the superiority of this molecular technique, this study aimed to develop and verify a novel DHA for fulfilling the unmet clinical need by expanding its detection potential from not only diagnosing FK, but also differentiating
Fusarium and
Aspergillus keratitis, as well as identifying target fungal species.
4. Discussion
FK is acknowledged as a catastrophic MK with a slow yet relentless clinical course. It had a changeable presentation during the progression of corneal infection. FK should be differentiated from herpetic and acanthamoebic keratitis in the early epithelitis dominant phase, while it should be distinguished from bacterial, necrotizing herpetic, and microsporidial stromal keratitis in the late stromal infiltration stage. Moreover, FK carried a higher failure rate of medical treatment than other MK, especially for patients with delayed diagnosis and erratic application of corticosteroids.
Fusarium and
Aspergillus are two major genera that cause FK. However,
Fusarium spp. is more susceptible to natamycin than to voriconazole, whereas
Aspergillus spp. is more sensitive to voriconazole than to natamycin [
14,
24,
25]. Accordingly, the treatment outcome via topical voriconazole was inferior to that via natamycin for a FK cohort with a higher prevalence of
Fusarium keratitis [
26], and
Aspergillus keratitis had a higher medical failure and surgical rate under natamycin treatment [
27]. The novel DHA developed in this study had an excellent diagnostic performance in diagnosing FK. Moreover, it was capable of differentiating between
Fusarium and
Aspergillus keratitis and recognizing
F. solani keratitis. Therefore, our DHA is helpful in providing an earlier diagnosis and the opportunity for a more precise treatment for FK.
DHA is a highly sensitive technique with the potential to develop an oligonucleotide array for identifying fungal pathogens to species level [
18]. We previously applied this technique to diagnose FK [
17] and assessed the bacterial bioburden for the orthokeratology lens care system [
28]. However, FK has broad spectra of fungal pathogens, which are almost opportunistic by means of ocular trauma. A universal probe for detecting fungus is not enough to help physicians in determining a personalized anti-fungal strategy. In this study, the novel DHA showed promising results for this goal because it is capable of diagnosing FK and differentiating between
Fusarium and
Aspergillus keratitis.
Among seven patients with culture-positive but DHA-negative for fungi (
Table 4), only one patient was confirmed by DNA sequencing. The possible cause of failed DHA detection for this patient was that simultaneous detection of several targets may have dispersed DNA amplicons to different probes, which increased the detection limit of the universal probe and would have needed more microorganisms in a scrapping sample. The other six patients could not be confirmed by DNA sequencing for fungi. We speculated that the result was caused by sampling failure, which led to no or insufficient microorganisms in the scrape for the DHA assessment. Among the 27 patients with culture negative but DHA positive (
Table 4), 26 patients were confirmed positive but 1 patient was false-positive by discrepant analysis. DHA was more sensitive than culture, which cannot detect fastidious or nonviable microorganisms [
17]. However, DHA is a susceptible molecular test, which may detect very few contaminated fungi or fungal amplicons and cause a false-positive result.
Too few
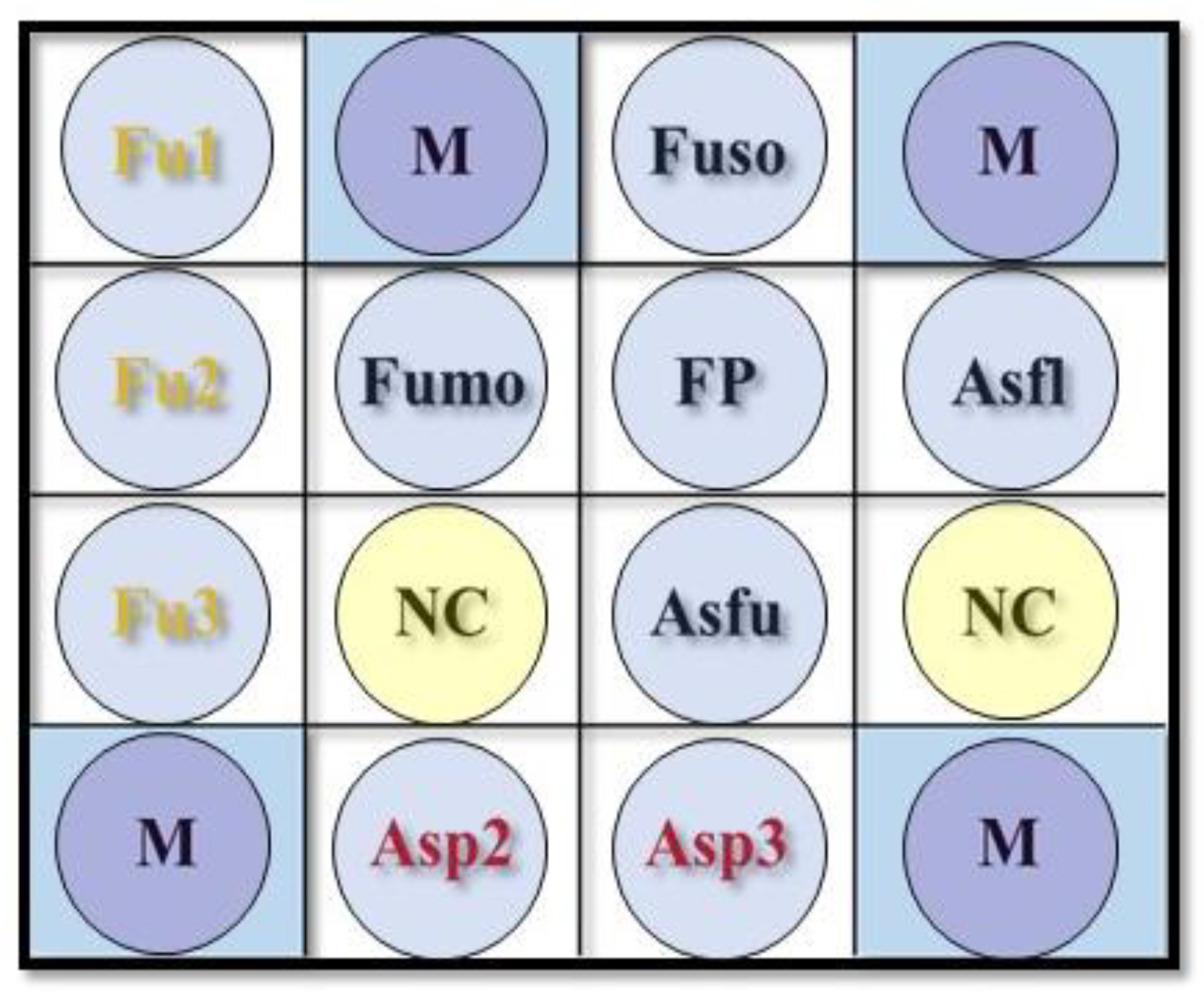
F. verticillioides keratitis led to failure to estimate sensitivity and PPR, and therefore, we could only conclude that probe Fumo had reasonable specificity and NPR (
Table 5). Thus, the DHA’s performance for diagnosing
F. verticillioides keratitis could not be sufficiently verified. However, the DHA’s performance was well-validated for diagnosing
Fusarium keratitis and
F. solani with high accuracies of 93.6% and 96.4%, respectively. Among the three false-negative scrapes via probes Fu1, Fu2, and Fu3 for detecting
Fusarium spp., two samples with
F. solani and one sample with
Fusarium spp. were confirmed by DNA sequencing. Amplicons distributed to the universal probe FP and the species probe Fuso could be the false-negative reason. Among the six false-positive scrapes via probe Fuso for detecting
F. solani, four samples were recognized as
Colletotrichum spp. (two
C. siamense, one
C. fructicola, and one
C. gloeosporioides), one sample was identified as
Scedosporium apiospermum, and one sample was confirmed as
Gjaerumia spp. One sample was a false-positive detection for
F. verticillioides, where the DNA sequencing result was
F. solani. Modifying the species’ probes Fuso and Fumo for specific detection of
F. solani and
F. verticillioides, or designing new probes for
Colletotrichum,
Scedosporium, and
Gjaerumia will be considered.
There were only six scrapes with
Aspergillus spp., including two
A. flavus keratitis, two
A. fumigatus keratitis, one
A. niger, and one
A. tamarii. Therefore, it was weak to estimate sensitivity and PPR for the probes for diagnosing
Aspergillus genera,
A. flavus, and
A. fumigatus (
Table 6). Only reasonable specificity and NPR could be claimed for these probes. For the sample with false-negative detection for
Aspergillus spp. (by probes Asp2 and Asp3), the result of DNA sequencing was
A. tamarii. The design of a new probe for detecting
A. tamarii or the modification of current genus probes will be the solution for avoiding misdiagnosis for the species.
Due to the limitation in which some target pathogens were rare, the sensitivity and PPR of the probes for identifying
Aspergillus keratitis and the species probes for recognizing
F. verticillioides,
A. flavus, and
A. fumigatus could not be confidently validated. However, these probes undoubtedly had acceptable specificity and NPR. Moreover, they were speculated to have a similar performance to the probes for diagnosing
Fusarium keratitis and
F. solani keratitis because all probes had passed the preclinical challenge with target and non-target microorganisms (
Table 1).
According to the comprehensive review of Hoffman et al. [
11], filamentous FK, particularly
Fusarium and
Aspergillus keratitis, is a global treat. FK has an apparent geographical variation, and
Fusarium or
Aspergillus keratitis often accounted for the top two prevalent pathogens, even in North America. In some temperate areas such as Europe and North America,
Candida spp. has a chance to be in the top two most common pathogens of FK. The severity of
Candida keratitis is less than that of filamentous FK. Thus, the DHA can also be used in non-Asian countries to detect
Candida spp. via probe FP and exclude vision-threatening
Fusarium and
Aspergillus keratitis via species and genus probes. The DHA can be used as an adjunctive clinical test of conventional culture for a mycology laboratory to increase the recovery rate and efficiency in diagnosing FK and differentiating
Fusarium from
Aspergillus keratitis for early precise anti-fungal treatment. However, the procedures need well-trained staff and sterile technique in the laboratory.
There are several novel antifungal regimens for FK [
29,
30,
31]. Keratosept ophthalmic solution containing hexamidine diisethionate 0.05% is a potential candidate for the treatment of
Candida and staphylococcal infections of the ocular surface [
29]. Corneal collagen cross-linking treatment via Riboflavin/UVA (CXL) showed therapeutic efficacy against FK [
30]. CXL combined with 0.02% chlorhexidine is also an effective therapy against FK, particularly for multi-resistant
Fusarium keratitis [
31]. Following the development of novel anti-fungal treatments, we believe the DHA, or a modified DHA targeting specific fungal species or genus, can provide a rapid and precise diagnosis helping physicians to choose a suitable anti-fungal treatment.


 ,
, 



{kind=link}
{kind=link}