

Post-Partum Depression Lactating Rat Model for Evaluating Ketamine’s Safety as a Pharmacotherapeutic Treatment: Roles in Cardiac and Urinary Function
 , , , , , and
, , , , , and
Abstract
:1. Introduction
1.1. General Mechanism of Action and Safety of Ketamine
1.2. Effects on Cardiac and Urinary Function
2. Materials and Methods
2.1. Animals
2.2. Experimental Design
2.3. Model of Depression Induction by Maternal Separation
2.4. Timeline and Experimental Design
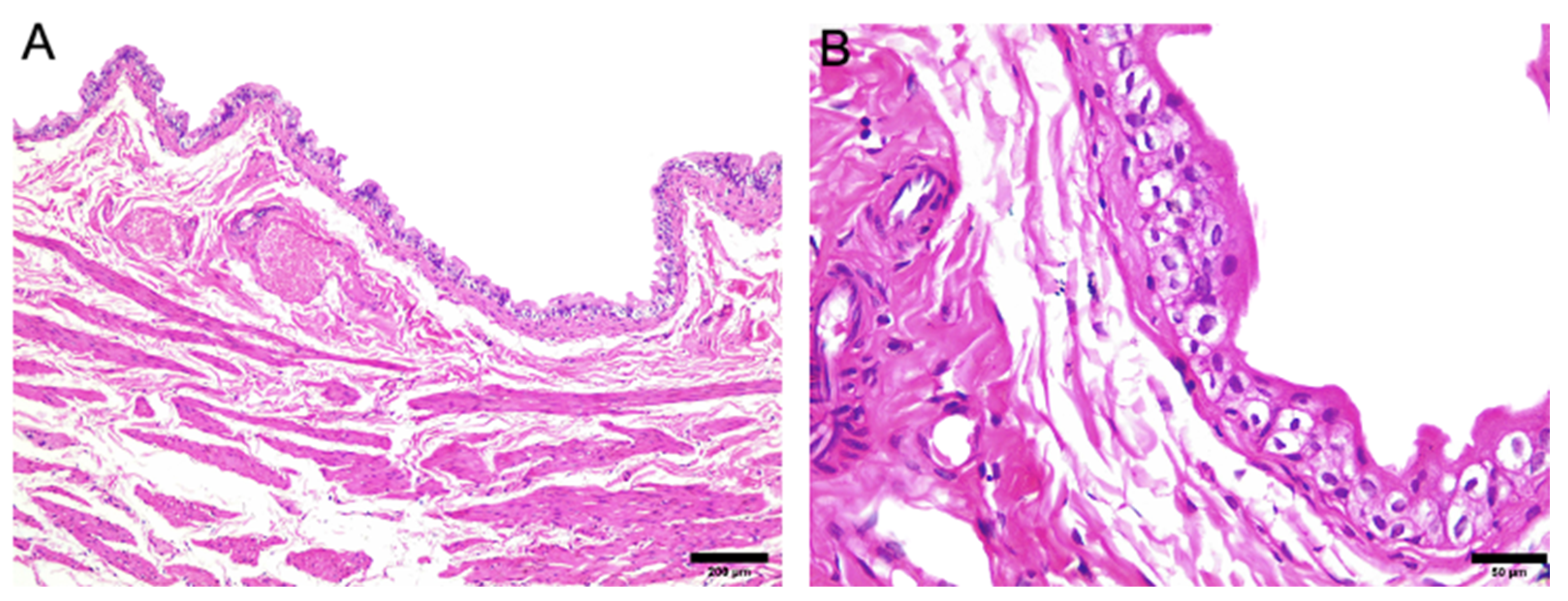
2.5. Histopathological Evaluation
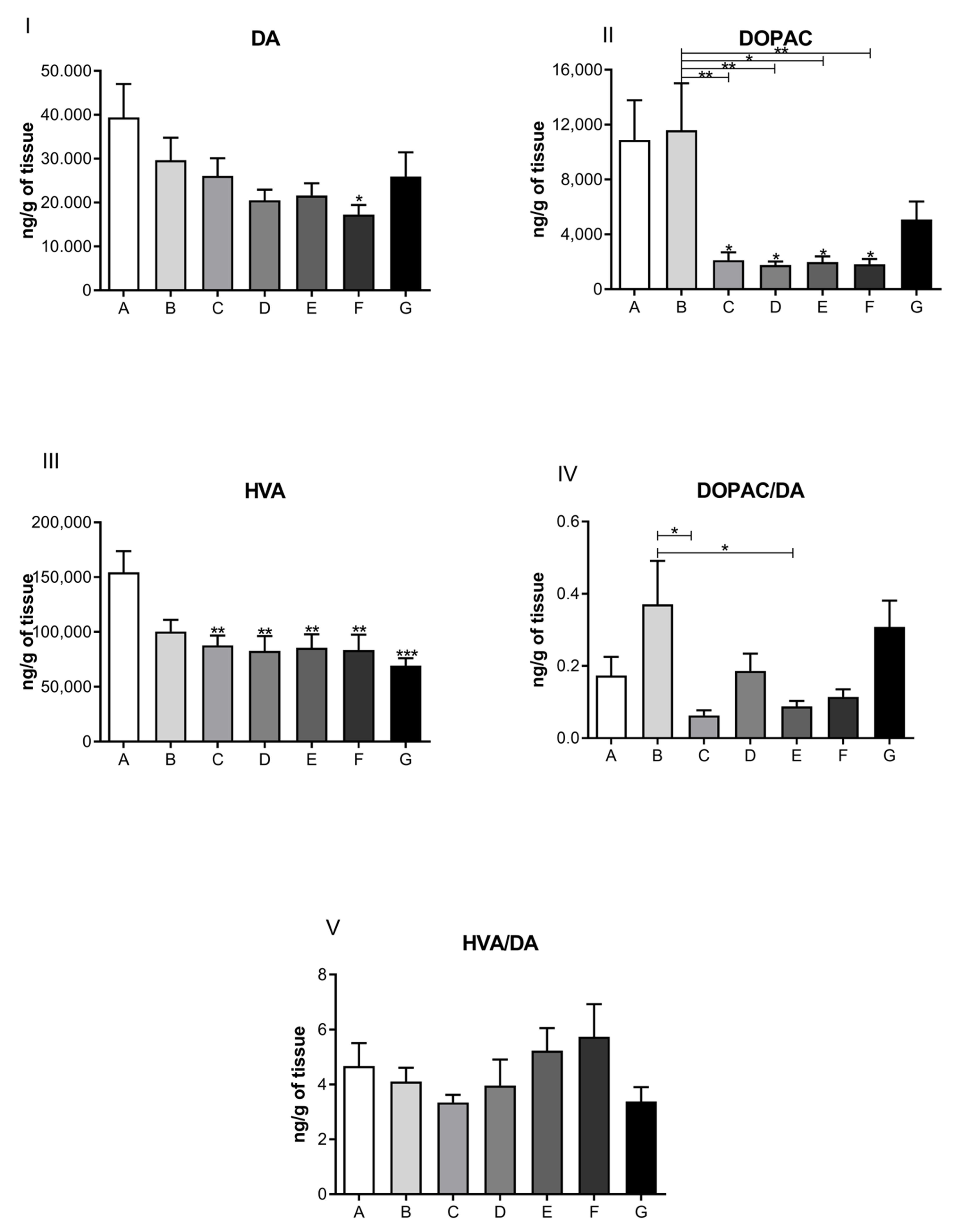
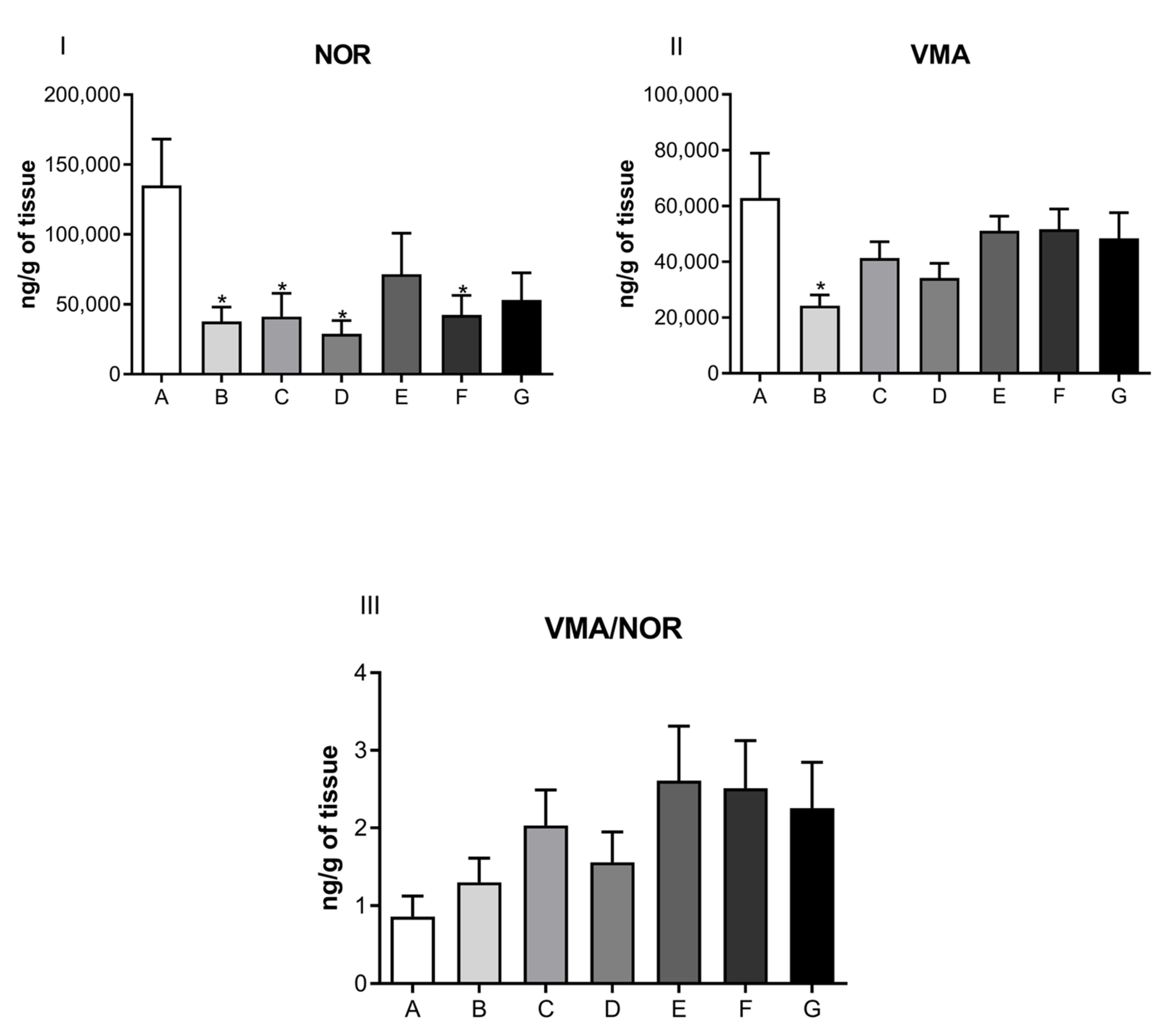
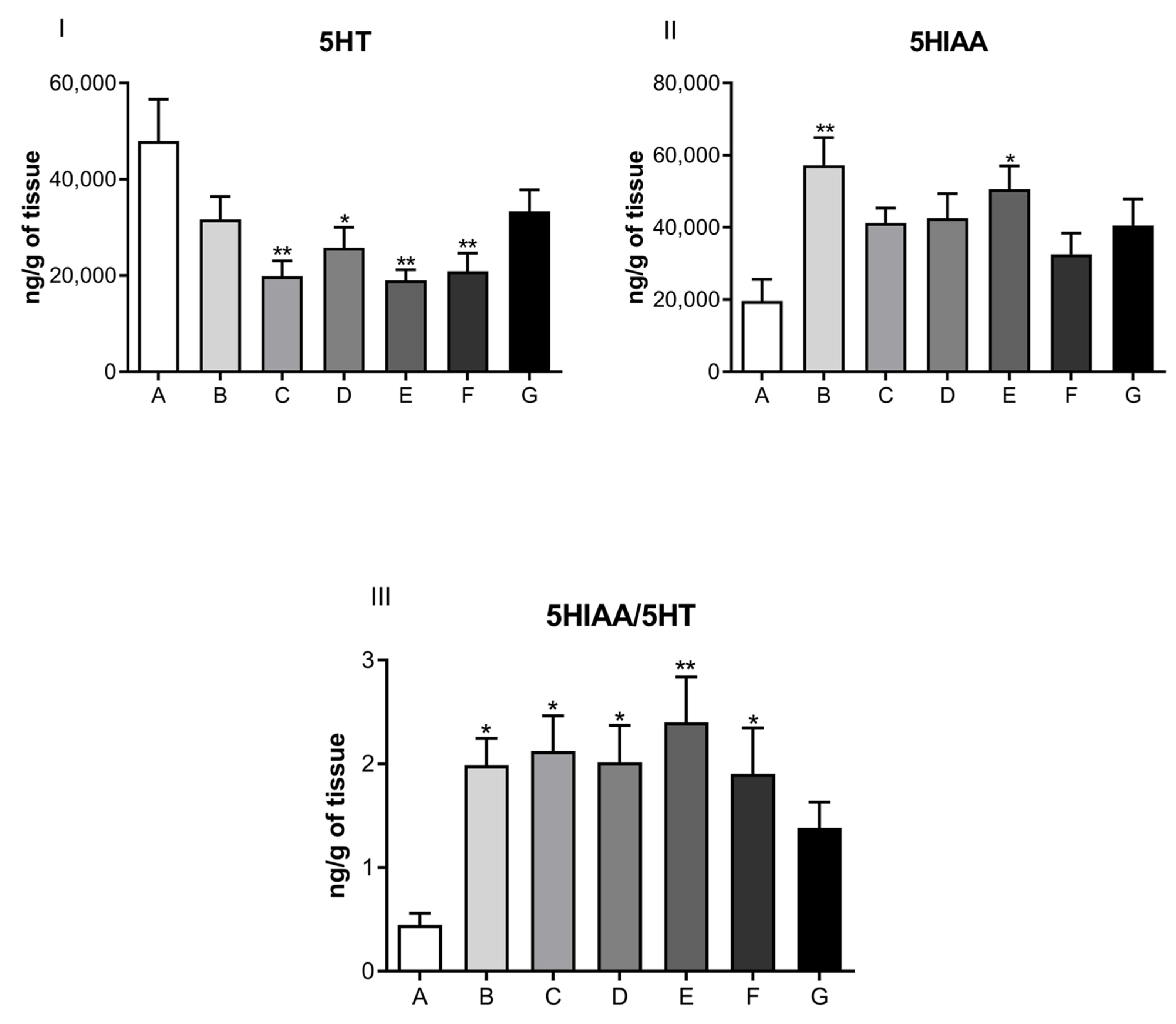
2.6. Cardiochemical Assessment
- -
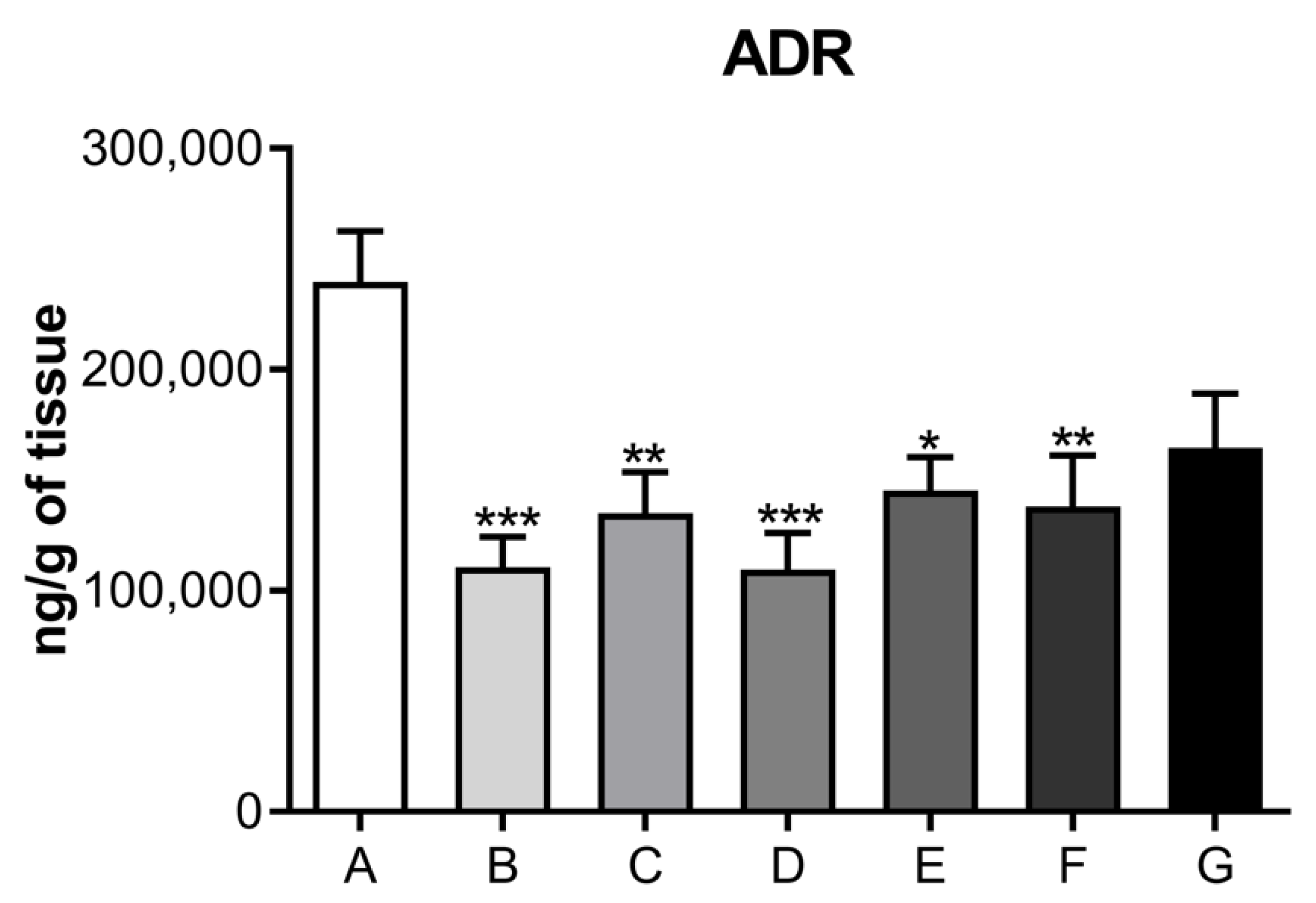
- Adrenaline (ADR);
- -
- Noradrenaline (NOR) and its metabolite vanillylmandelic acid (VMA);
- -
- Dopamine (DA) and its metabolites, 4,4-dihydroxyphenylacetic acid (DOPAC) and homovanillic acid (HVA);
- -
- Serotonin (5HT) and its metabolite 5-hydroindole, 3-acetic acid (5HIAA).
2.7. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Werner, E.; Miller, M.; Osborne, L.M.; Kuzava, S.; Monk, C. Preventing postpartum depression: Review and recommendations. Arch. Women’s Ment. Health 2015, 18, 41–60. [Google Scholar] [CrossRef] [PubMed]
- Osborne, L.M.; Gilden, J.; Kamperman, A.M.; Hoogendijk, W.J.; Spicer, J.; Drexhage, H.A.; Bergink, V. T-cell defects and postpartum depression. Brain Behav. Immun. 2020, 87, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Lindahl, V.; Pearson, J.L.; Colpe, L. Prevalence of suicidality during pregnancy and the postpartum. Arch. Women’s Ment. Health 2005, 8, 77–87. [Google Scholar] [CrossRef]
- Fava, M.; Rush, A.J.; Alpert, J.E.; Carmin, C.N.; Balasubramani, G.; Wisniewski, S.R.; Trivedi, M.H.; Biggs, M.M.; Shores-Wilson, K. What clinical and symptom features and comorbid disorders characterize outpatients with anxious major depressive disorder: A replication and extension. Can. J. Psychiatry 2006, 51, 823–835. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Choi, A.Y.; Park, E.; Park, H.J.; Lee, J.; Lee, H.; Kim, J.; Cho, J. Effects of continuous ketamine infusion on hemodynamics and mortality in critically ill children. PLoS ONE 2019, 14, e0224035. [Google Scholar] [CrossRef]
- Wilkowska, A.; Szałach, Ł.; Cubała, W.J. Ketamine in bipolar disorder: A review. Neuropsychiatr. Dis. Treat. 2020, 16, 2707. [Google Scholar] [CrossRef]
- Langmia, I.M.; Just, K.S.; Yamoune, S.; Muller, J.P.; Stingl, J.C. Pharmacogenetic and drug interaction aspects on ketamine safety in its use as antidepressant—Implications for precision dosing in a global perspective. Br. J. Clin. Pharmacol. 2022. [Google Scholar] [CrossRef]
- Da Silva, F.C.C.; Dantas, R.T.; de Oliveira, M.d.d.C.; de Vasconcelos, S.M.M.; de França Fonteles, M.M.; de Barros Viana, G.S.; de Sousa, F.C.F. Ketamina, da anestesia ao uso abusivo: Artigo de revisão. Rev. Neurociênc. 2010, 18, 227–237. [Google Scholar] [CrossRef]
- Hirota, K.; Lambert, D. Ketamine: New Uses for an Old Drug? Oxford University Press: Oxford, UK, 2011; Volume 107, pp. 123–126. [Google Scholar]
- Rofael, H.Z.; Abdel-Rahman, M.S. Development and validation of a high-performance liquid chromatography method for the determination of cocaine, its metabolites and ketamine. J. Appl. Toxicol. Int. J. 2002, 22, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Bergman, S.A. Ketamine: Review of its pharmacology and its use in pediatric anesthesia. Anesth. Prog. 1999, 46, 10–20. [Google Scholar] [PubMed]
- Kritzer, M.D.; Pae, C.U.; Masand, P.S. Key considerations for the use of ketamine and esketamine for the treatment of depression: Focusing on administration, safety, and tolerability. Expert Opin. Drug Saf. 2022, 21, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, J.M.; Loeb, A.L.; Reichard, P.S.; Irvine, S. Ketamine inhibits glutamate-, N-methyl-D-aspartate-, and quisqualate-stimulated cGMP production in cultured cerebral neurons. J. Am. Soc. Anesthesiol. 1995, 82, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Ponce, F.; Fukushima, A.R. Aspectos farmacológicos e toxicológicos da cetamina: Uma revisão de literatura. Braz. J. Forensic Sci. Med. Law Bioeth. 2017, 6, 210–227. [Google Scholar] [CrossRef]
- Santiago, C.d.M.; Fernandes, C.H.; Nogueira, M.S.; Veiga, E.V.; Cárnio, E.C. Utilização do óxido nítrico como terapêutica: Implicações para a enfermagem. Rev. Lat.—Am. Enferm. 2000, 8, 76–82. [Google Scholar] [CrossRef]
- Craven, R. Ketamine. Anaesthesia 2007, 62, 48–53. [Google Scholar] [CrossRef]
- Reich, D.L.; Silvay, G. Ketamine: An update on the first twenty-five years of clinical experience. Can. J. Anaesth. 1989, 36, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Ahiskalioglu, A.; Ince, I.; Aksoy, M.; Ahiskalioglu, E.O.; Comez, M.; Dostbil, A.; Celik, M.; Alp, H.H.; Coskun, R.; Taghizadehghalehjoughi, A.; et al. Comparative investigation of protective effects of metyrosine and metoprolol against ketamine cardiotoxicity in rats. Cardiovasc. Toxicol. 2015, 15, 336–344. [Google Scholar] [CrossRef]
- Ahiskalioglu, E.O.; Aydin, P.; Ahiskalioglu, A.; Suleyman, B.; Kuyrukluyildiz, U.; Kurt, N.; Altuner, D.; Coskun, R.; Suleyman, H. The effects of ketamine and thiopental used alone or in combination on the brain, heart, and bronchial tissues of rats. Arch. Med. Sci. AMS 2018, 14, 645–654. [Google Scholar] [CrossRef] [PubMed]
- White, J.M.; Ryan, C.F. Pharmacological properties of ketamine. Drug Alcohol Rev. 1996, 15, 145–155. [Google Scholar] [CrossRef]
- Hašková, P.; Koubková, L.; Vávrová, A.; Macková, E.; Hrušková, K.; Kovaříková, P.; Vávrová, K.; Šimůnek, T. Comparison of various iron chelators used in clinical practice as protecting agents against catecholamine-induced oxidative injury and cardiotoxicity. Toxicology 2011, 289, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Shi, J.; Yang, B.; Liu, L.; Han, C.; Li, W.; Dong, D.; Pan, Z.; Liu, G.; Geng, J.; et al. Ketamine-induced ventricular structural, sympathetic and electrophysiological remodelling: Pathological consequences and protective effects of metoprolol. Br. J. Pharmacol. 2012, 165, 1748–1756. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Sood, S.; Dinda, A.; Das, T.; Maulik, S. Chronic oral administration of raw garlic protects against isoproterenol-induced myocardial necrosis in rat. Comp. Biochem. Physiol. C Toxicol. Pharmacol. 2003, 136, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Shahani, R.; Streutker, C.; Dickson, B.; Stewart, R.J. Ketamine-associated ulcerative cystitis: A new clinical entity. Urology 2007, 69, 810–812. [Google Scholar] [CrossRef] [PubMed]
- Chu, P.S.K.; Ma, W.K.; Wong, S.C.W.; Chu, R.W.H.; Cheng, C.H.; Wong, S.; Tse, J.M.l.; Lau, F.L.; Yiu, M.K.; Man, C.W. The destruction of the lower urinary tract by ketamine abuse: A new syndrome? BJU Int. 2008, 102, 1616–1622. [Google Scholar] [CrossRef]
- Gu, D.; Huang, J.; Yin, Y.; Shan, Z.; Zheng, S.; Wu, P. Long-term ketamine abuse induces cystitis in rats by impairing the bladder epithelial barrier. Mol. Biol. Rep. 2014, 41, 7313–7322. [Google Scholar] [CrossRef]
- Middela, S.; Pearce, I. Ketamine-induced vesicopathy: A literature review. Int. J. Clin. Pract. 2011, 65, 27–30. [Google Scholar] [CrossRef]
- Vetulani, J. Early maternal separation: A rodent model of depression and a prevailing human condition. Pharmacol. Rep. 2013, 65, 1451–1461. [Google Scholar] [CrossRef]
- Kritzer, M.D.; Mischel, N.A.; Young, J.R.; Lai, C.S.; Masand, P.S.; Szabo, S.T.; Mathew, S.J. Ketamine for treatment of mood disorders and suicidality: A narrative review of recent progress. Ann. Clin. Psychiatry—Off. J. Am. Acad. Clin. Psychiatr. 2022, 34, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Salvadore, G.; Singh, J.B. Ketamine as a fast acting antidepressant: Current knowledge and open questions. CNS Neurosci. Ther. 2013, 19, 428–436. [Google Scholar] [CrossRef]
- Kohtala, S. Ketamine—50 years in use: From anesthesia to rapid antidepressant effects and neurobiological mechanisms. Pharmacol. Rep. 2021, 73, 323–345. [Google Scholar] [CrossRef]
- Szarmach, J.; Cubała, W.J.; Włodarczyk, A.; S Wiglusz, M. Short-term ketamine administration in treatment-resistant depression: Focus on cardiovascular safety. Psychiatr. Danub. 2019, 31, 585–590. [Google Scholar] [PubMed]
- Krystal, J.H.; Petrakis, I.L.; Webb, E.; Cooney, N.L.; Karper, L.P.; Namanworth, S.; Stetson, P.; Trevisan, L.A.; Charney, D.S. Dose-related ethanol-like effects of the NMDA antagonist, ketamine, in recently detoxified alcoholics. Arch. Gen. Psychiatry 1998, 55, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Jaber, S.M.; Hankenson, F.C.; Heng, K.; McKinstry-Wu, A.; Kelz, M.B.; Marx, J.O. Dose regimens, variability, and complications associated with using repeat-bolus dosing to extend a surgical plane of anesthesia in laboratory mice. J. Am. Assoc. Lab. Anim. Sci. 2014, 53, 684–691. [Google Scholar] [PubMed]
- Wang, J.; Chen, Y.; Gu, D.; Zhang, G.; Chen, J.; Zhao, J.; Wu, P. Ketamine-induced bladder fibrosis involves epithelial-to-mesenchymal transition mediated by transforming growth factor-β1. Am. J. Physiol.—Ren. Physiol. 2017, 313, F961–F972. [Google Scholar] [CrossRef] [PubMed]
- Yeung, L.; Rudd, J.; Lam, W.; Mak, Y.; Yew, D. Mice are prone to kidney pathology after prolonged ketamine addiction. Toxicol. Lett. 2009, 191, 275–278. [Google Scholar] [CrossRef]
- Huang, P.-W.; Meng, E.; Cha, T.-L.; Sun, G.-H.; Yu, D.-S.; Chang, S.-Y. ‘Walking-stick ureters’ in ketamine abuse. Kidney Int. 2011, 80, 895. [Google Scholar] [CrossRef] [PubMed]
- Vinholi, A.; Fagundes, M.D.C.; Pigozzo, D.C.; Kubrusly, F.B.; Kubrusly, L.F.; Marques, C.A.M. Involvement of catecholamines in the myocardium of rats submitted to experimental model of portal hypertension. ABCD. Arq. Bras. Cir. Dig. (São Paulo) 2018, 31, 1–4. [Google Scholar] [CrossRef]
- Franchini, K.G. Hipertrofia cardíaca: Mecanismos moleculares. Rev. Bras. Hipertens. 2001, 8, 125–142. [Google Scholar]
- Lindpaintner, K.; Lund, D.D.; Schmid, P.G. Role of myocardial hypertrophy in trophic stimulation of indices of sympathetic cardiac innervation. J. Cardiovasc. Pharmacol. 1987, 10, S211–S220. [Google Scholar] [CrossRef]
- Yamada, Y.; Okumura, K.; Hashimoto, H.; Ito, T.; Satake, T. Altered myocardial acetylcholine and norepinephrine concentrations in right ventricular hypertrophy and failure. Heart Vessel. 1991, 6, 150–157. [Google Scholar] [CrossRef]
- Zouhal, H.; Jacob, C.; Delamarche, P.; Gratas-Delamarche, A. Catecholamines and the effects of exercise, training and gender. Sports Med. 2008, 38, 401–423. [Google Scholar] [CrossRef] [PubMed]
- Ghimire, L.V.; Kohli, U.; Chun, L.; Sofowora, G.G.; Muszkat, M.; Friedman, E.A.; Solus, J.F.; Wood, A.J.; Stein, C.M.; Kurnik, D. Catecholamine pathway gene variation is associated with norepinephrine and epinephrine concentrations at rest and exercise. Pharm. Genom. 2012, 22, 254–260. [Google Scholar] [CrossRef]
- Ziegler, M.; Kennedy, B.; Holland, O.; Murphy, D.; Lake, C. The effects of dopamine agonists on human cardiovascular and sympathetic nervous systems. Int. J. Clin. Pharmacol. Ther. Toxicol. 1985, 23, 175–179. [Google Scholar]
- Ayme-Dietrich, E.; Aubertin-Kirch, G.; Maroteaux, L.; Monassier, L. Cardiovascular remodeling and the peripheral serotonergic system. Arch. Cardiovasc. Dis. 2017, 110, 51–59. [Google Scholar] [CrossRef]
- Côté, F.; Fligny, C.; Fromes, Y.; Mallet, J.; Vodjdani, G. Recent advances in understanding serotonin regulation of cardiovascular function. Trends Mol. Med. 2004, 10, 232–238. [Google Scholar] [CrossRef]
- Rothman, R.B.; Baumann, M.H.; Savage, J.E.; Rauser, L.; McBride, A.; Hufeisen, S.J.; Roth, B.L. Evidence for possible involvement of 5-HT2B receptors in the cardiac valvulopathy associated with fenfluramine and other serotonergic medications. Circulation 2000, 102, 2836–2841. [Google Scholar] [CrossRef]
- Chiladakis, J.A.; Patsouras, N.; Manolis, A.S. The bezold-jarisch reflex in acute inferior myocardial infarction: Clinical and sympathovagal spectral correlates. Clin. Cardiol. Int. Index. Peer-Rev. J. Adv. Treat. Cardiovasc. Dis. 2003, 26, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Kaumann, A.J.; Levy, F.O. 5-hydroxytryptamine receptors in the human cardiovascular system. Pharmacol. Ther. 2006, 111, 674–706. [Google Scholar] [CrossRef] [PubMed]
- Monassier, L.; Laplante, M.A.; Ayadi, T.; Doly, S.; Maroteaux, L. Contribution of gene-modified mice and rats to our understanding of the cardiovascular pharmacology of serotonin. Pharmacol. Ther. 2010, 128, 559–567. [Google Scholar] [CrossRef]
- Du Jardin, K.G.; Müller, H.K.; Elfving, B.; Dale, E.; Wegener, G.; Sanchez, C. Potential involvement of serotonergic signaling in ketamine’s antidepressant actions: A critical review. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2016, 71, 27–38. [Google Scholar] [CrossRef]
- Du Jardin, K.G.; Liebenberg, N.; Müller, H.K.; Elfving, B.; Sanchez, C.; Wegener, G. Differential interaction with the serotonin system by S-ketamine, vortioxetine, and fluoxetine in a genetic rat model of depression. Psychopharmacology 2016, 233, 2813–2825. [Google Scholar] [CrossRef] [PubMed]
- Gigliucci, V.; O’Dowd, G.; Casey, S.; Egan, D.; Gibney, S.; Harkin, A. Ketamine elicits sustained antidepressant-like activity via a serotonin-dependent mechanism. Psychopharmacology 2013, 228, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Fukumoto, K.; Iijima, M.; Chaki, S. Serotonin-1A receptor stimulation mediates effects of a metabotropic glutamate 2/3 receptor antagonist, 2S-2-amino-2-(1S, 2S-2-carboxycycloprop-1-yl)-3-(xanth-9-yl) propanoic acid (LY341495), and an N-methyl-D-aspartate receptor antagonist, ketamine, in the novelty-suppressed feeding test. Psychopharmacology 2014, 231, 2291–2298. [Google Scholar] [PubMed]
- Fukumoto, K.; Iijima, M.; Chaki, S. The antidepressant effects of an mGlu2/3 receptor antagonist and ketamine require AMPA receptor stimulation in the mPFC and subsequent activation of the 5-HT neurons in the DRN. Neuropsychopharmacology 2016, 41, 1046–1056. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Description | Treatment Period |
|---|---|---|
| A | Control (normal, not treated) | |
| B | Control (normal) + saline | PND2 to PND21 |
| C | Depressed + saline | PND2 to PND21 |
| D | Depressed + ketamine 5 mg/kg | PND2 to PND21 |
| E | Depressed + ketamine 10 mg/kg | PND2 to PND21 |
| F | Depressed + ketamine 20 mg/kg | PND2 to PND21 |
| G | Depressed + Ketamine 10 mg/kg on | Single dose on PND12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukushima, A.R.; Navas-Suárez, P.E.; Peña Muñoz, J.W.; Ricci, E.L.; Leoni, L.A.B.; Caperuto, É.C.; Yanase, L.; Santana, J.; de França, E.; Delorenzi, J.C.M.O.B.; et al. Post-Partum Depression Lactating Rat Model for Evaluating Ketamine’s Safety as a Pharmacotherapeutic Treatment: Roles in Cardiac and Urinary Function. J. Cardiovasc. Dev. Dis. 2022, 9, 299. https://doi.org/10.3390/jcdd9090299
Fukushima AR, Navas-Suárez PE, Peña Muñoz JW, Ricci EL, Leoni LAB, Caperuto ÉC, Yanase L, Santana J, de França E, Delorenzi JCMOB, et al. Post-Partum Depression Lactating Rat Model for Evaluating Ketamine’s Safety as a Pharmacotherapeutic Treatment: Roles in Cardiac and Urinary Function. Journal of Cardiovascular Development and Disease. 2022; 9(9):299. https://doi.org/10.3390/jcdd9090299
Chicago/Turabian StyleFukushima, André Rinaldi, Pedro Enrique Navas-Suárez, Juliana Weckx Peña Muñoz, Esther Lopes Ricci, Luís Antônio Baffile Leoni, Érico C. Caperuto, Leandro Yanase, Jeferson Santana, Elias de França, Jan Carlo Morais O. Bertassoni Delorenzi, and et al. 2022. "Post-Partum Depression Lactating Rat Model for Evaluating Ketamine’s Safety as a Pharmacotherapeutic Treatment: Roles in Cardiac and Urinary Function" Journal of Cardiovascular Development and Disease 9, no. 9: 299. https://doi.org/10.3390/jcdd9090299