
Early and Long-Term Outcomes after On-Pump and Off-Pump Coronary-Artery Bypass Grafting in Patients with Severe Left Ventricular Dysfunction and a Giant Left Ventricle
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Surgical Technique
2.3. Study Variables
2.4. Following Up
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Revascularization Data and Early Outcomes
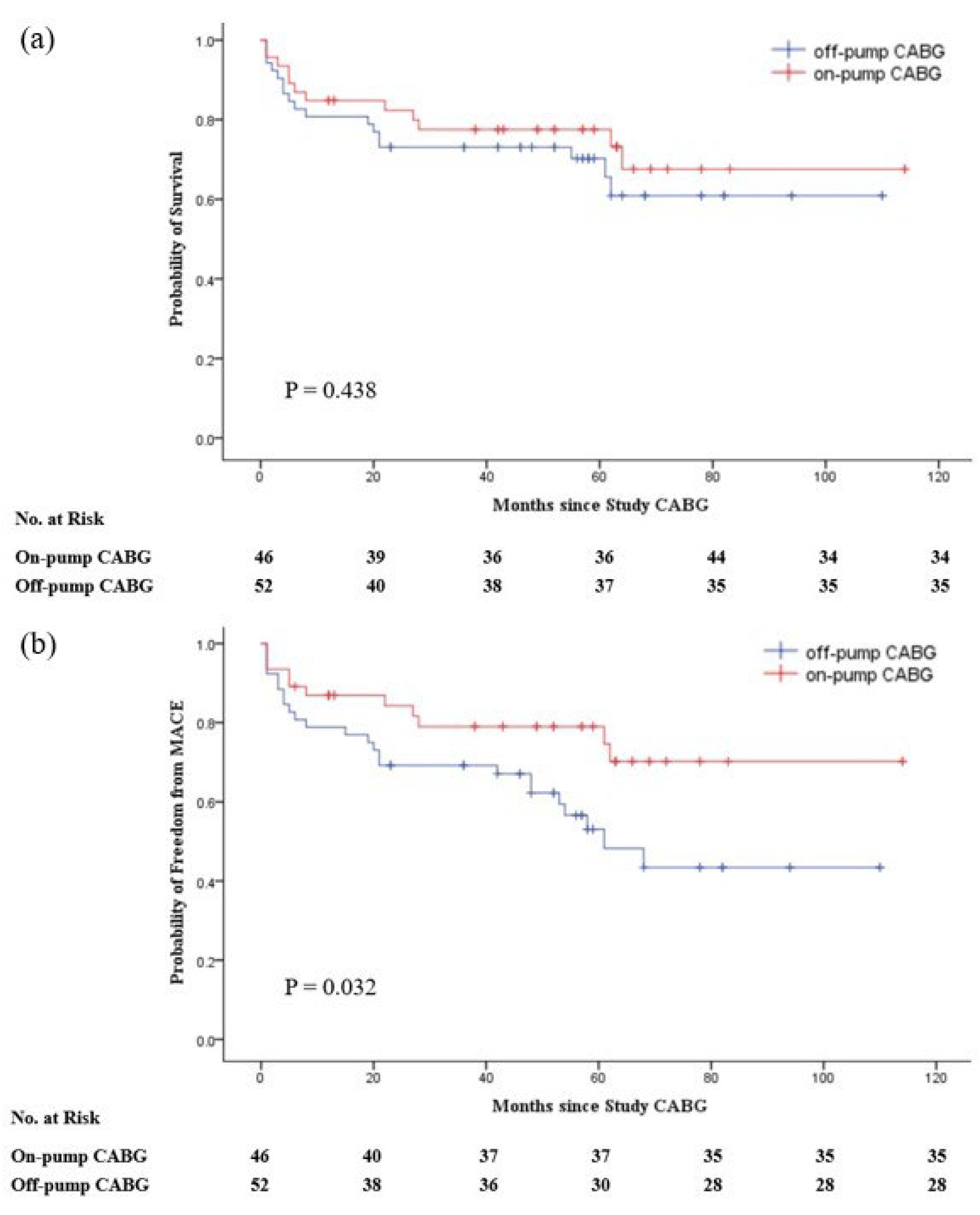
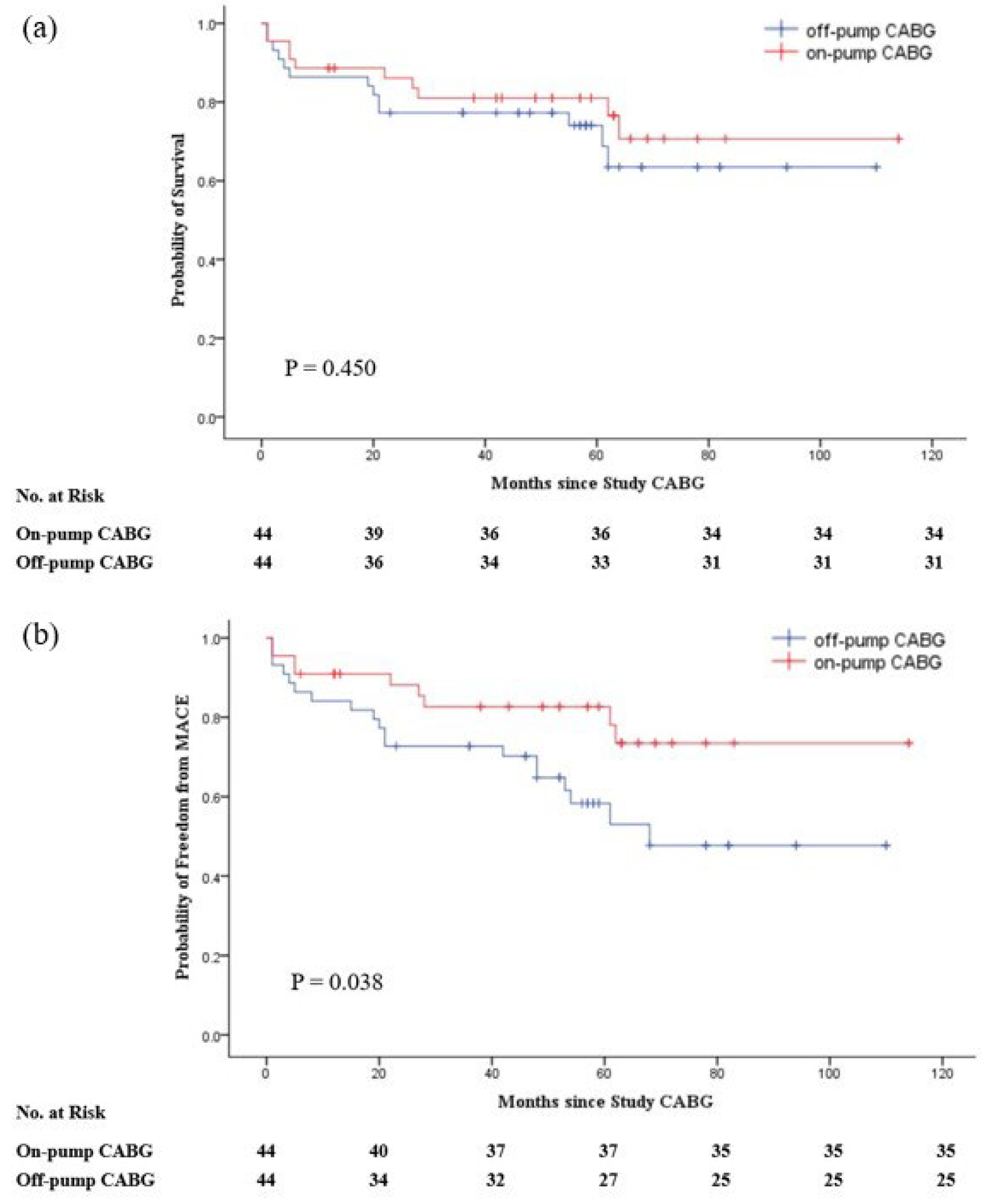
3.3. Long-Term Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CABG | coronary artery bypass grafting |
| OPCAB | off-pump CABG |
| ONCAB | on-pump CABG |
| LVD | left ventricular dysfunction |
| LVEF | left ventricular ejection fraction |
| LVEDD | left ventricular end-diastolic diameter |
| LCOS | low cardiac output syndrome |
| MACE | major adverse cardiovascular events |
| CAD | coronary heart disease |
| PCI | percutaneous coronary intervention |
| CPB | cardiopulmonary bypass |
| LIMA | left internal mammary artery |
| BMI | body mass index |
| COPD | chronic obstructive pulmonary disease |
| IABP | intra-aortic balloon pump |
| ICU | intensive care unit |
References
- Howlett, J.G.; Stebbins, A.; Petrie, M.C.; Jhund, P.S.; Castelvecchio, S.; Cherniavsky, A.; Sueta, C.A.; Roy, A.; Piña, I.L.; Wurm, R.; et al. CABG Improves Outcomes in Patients with Ischemic Cardiomyopathy: 10-Year Follow-Up of the STICH Trial. JACC Heart Fail. 2019, 7, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Velazquez, E.J.; Lee, K.L.; Deja, M.A.; Jain, A.; Sopko, G.; Marchenko, A.; Ali, I.S.; Pohost, G.; Gradinac, S.; Abraham, W.T.; et al. Coronary-Artery Bypass Surgery in Patients with Left Ventricular Dysfunction. N. Engl. J. Med. 2011, 364, 1607–1616. [Google Scholar] [CrossRef] [PubMed]
- Velazquez, E.J.; Lee, K.L.; Jones, R.H.; Al-Khalidi, H.R.; Hill, J.A.; Panza, J.A.; Michler, R.E.; Bonow, R.O.; Doenst, T.; Petrie, M.C.; et al. Coronary-Artery Bypass Surgery in Patients with Ischemic Cardiomyopathy. N. Engl. J. Med. 2016, 374, 1511–1520. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Hannan, E.L.; Farrell, L.S.; Wechsler, A.; Jordan, D.; Lahey, S.J.; Culliford, A.T.; Gold, J.P.; Higgins, R.S.; Smith, C.R. The New York Risk Score for In-Hospital and 30-Day Mortality for Coronary Artery Bypass Graft Surgery. Ann. Thorac. Surg. 2013, 95, 46–52. [Google Scholar] [CrossRef]
- Herlitz, J.; Brandrup-Wognsen, G.; Haglid, M.; Karlson, B.W.; Hartford, M.; Karlsson, T. Predictors of death during 5 years after coronary artery bypass grafting. Int. J. Cardiol. 1998, 64, 15–23. [Google Scholar] [CrossRef]
- Nashef, S.A.M.; Roques, F.; Michel, P.; Gauducheau, E.; Lemeshow, S.; Salamon, R. European system for cardiac operative risk evaluation (EuroSCORE). Eur. J. Cardio Thorac. Surg. 1999, 16, 9–13. [Google Scholar] [CrossRef]
- Wrobel, K.; Stevens, S.R.; Jones, R.H.; Selzman, C.H.; Lamy, A.; Beaver, T.M.; Djokovic, L.T.; Wang, N.; Velazquez, E.J.; Sopko, G.; et al. Influence of Baseline Characteristics, Operative Conduct, and Postoperative Course on 30-Day Outcomes of Coronary Artery Bypass Grafting Among Patients with Left Ventricular Dysfunction: Results From the Surgical Treatment for Ischemic Heart Failure (STICH) Trial. Circulation 2015, 132, 720–730. [Google Scholar] [CrossRef]
- Seropian, I.M.; Toldo, S.; Van Tassell, B.W.; Abbate, A. Anti-Inflammatory Strategies for Ventricular Remodeling Following ST-Segment Elevation Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2014, 63, 1593–1603. [Google Scholar] [CrossRef]
- Li, S.; Gong, W.; Qi, Q.; Yuan, Z.; Chen, A.; Liu, J.; Cai, J.; Zhou, M.; Wang, Z.; Ye, X.; et al. Outcomes of off-pump versus on-pump coronary artery bypass graft surgery in patients with severely dilated left ventricle. Ann. Transl. Med. 2016, 4, 340. [Google Scholar] [CrossRef] [Green Version]
- Diegeler, A.; Börgermann, J.; Kappert, U.; Breuer, M.; Böning, A.; Ursulescu, A.; Rastan, A.; Holzhey, D.; Treede, H.; Rieß, F.-C.; et al. Off-Pump versus On-Pump Coronary-Artery Bypass Grafting in Elderly Patients. N. Engl. J. Med. 2013, 368, 1189–1198. [Google Scholar] [CrossRef] [PubMed]
- Lamy, A.; Devereaux, P.; Prabhakaran, D.; Taggart, D.P.; Hu, S.; Paolasso, E.; Straka, Z.; Piegas, L.S.; Akar, A.R.; Jain, A.R.; et al. Off-Pump or On-Pump Coronary-Artery Bypass Grafting at 30 Days. N. Engl. J. Med. 2012, 366, 1489–1497. [Google Scholar] [CrossRef] [PubMed]
- Ascione, R.; Narayan, P.; Rogers, C.A.; Lim, K.H.; Capoun, R.; Angelini, G.D. Early and midterm clinical outcome in patients with severe left ventricular dysfunction undergoing coronary artery surgery. Ann. Thorac. Surg. 2003, 76, 793–799. [Google Scholar] [CrossRef]
- Kunadian, V.; Zaman, A.; Qiu, W. Revascularization among patients with severe left ventricular dysfunction: A meta-analysis of observational studies. Eur. J. Heart Fail. 2011, 13, 773–784. [Google Scholar] [CrossRef]
- Marin-Cuartas, M.; Deo, S.V.; Ramirez, P.; Verevkin, A.; Leontyev, S.; Borger, M.A.; Davierwala, P.M. Off-pump coronary artery bypass grafting is safe and effective in patients with severe left ventricular dysfunction. Eur. J. Cardio Thorac. Surg. 2022, 61, 705–713. [Google Scholar] [CrossRef]
- Keeling, W.B.; Williams, M.L.; Slaughter, M.S.; Zhao, Y.; Puskas, J.D. Off-Pump and On-Pump Coronary Revascularization in Patients with Low Ejection Fraction: A Report From The Society of Thoracic Surgeons National Database. Ann. Thorac. Surg. 2013, 96, 83–89. [Google Scholar] [CrossRef]
- Ueki, C.; Miyata, H.; Motomura, N.; Sakaguchi, G.; Akimoto, T.; Takamoto, S. Off-pump versus on-pump coronary artery bypass grafting in patients with left ventricular dysfunction. J. Thorac. Cardiovasc. Surg. 2016, 151, 1092–1098. [Google Scholar] [CrossRef]
- Chawla, L.; Zhao, Y.; Lough, F.C.; Schroeder, E.; Seneff, M.G.; Brennan, J.M. Off-Pump versus On-Pump Coronary Artery Bypass Grafting Outcomes Stratified by Preoperative Renal Function. J. Am. Soc. Nephrol. 2012, 23, 1389–1397. [Google Scholar] [CrossRef]
- Bronicki, R.A.; Hall, M. Cardiopulmonary Bypass-Induced Inflammatory Response: Pathophysiology and Treatment. Pediatr. Crit. Care Med. 2016, 17, S272–S278. [Google Scholar] [CrossRef]
- Chenoweth, D.E.; Cooper, S.W.; Hugli, T.E.; Stewart, R.W.; Blackstone, E.H.; Kirklin, J.W. Complement Activation during Cardiopulmonary Bypass: Evidence for generation of C3a and C5a anaphylatoxins. N. Engl. J. Med. 1981, 304, 497–503. [Google Scholar] [CrossRef]
- Rothenburger, M.; Tjan, T.D.; Schneider, M.; Berendes, E.; Schmid, C.; Wilhelm, M.J.; Böcker, D.; Scheld, H.H.; Soeparwata, R. The impact of the pro- and anti-inflammatory immune response on ventilation time after cardiac surgery. Cytom. Part B Clin. Cytom. J. Int. Soc. Anal. Cytol. 2003, 53B, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Klausner, J.M.; Paterson, I.S.; Goldman, G.; Kobzik, L.; Rodzen, C.; Lawrence, R.; Valeri, C.R.; Shepro, D.; Hechtman, H.B. Postischemic renal injury is mediated by neutrophils and leukotrienes. Am. J. Physiol. Ren. Physiol. 1989, 256, F794–F802. [Google Scholar] [CrossRef] [PubMed]
- Murphy, G.J.; Lin, H.; Coward, R.; Toth, T.; Holmes, R.; Hall, D.; Angelini, G.D. An initial evaluation of post-cardiopulmonary bypass acute kidney injury in swine. Eur. J. Cardio Thorac. Surg. 2009, 36, 849–855. [Google Scholar] [CrossRef] [PubMed]
- Billings, F.T., 4th; Ball, S.K.; Roberts, L.J., 2nd; Pretorius, M. Postoperative acute kidney injury is associated with hemoglobinemia and an enhanced oxidative stress response. Free Radic. Biol. Med. 2011, 50, 1480–1487. [Google Scholar] [CrossRef] [PubMed]
- Wan, S.; Yim, A.P. Cytokines in myocardial injury: Impact on cardiac surgical approach. Eur. J. Cardio Thorac. Surg. 1999, 16, S107–S111. [Google Scholar] [CrossRef]
- Blackstone, E.H.; Sabik, J.F., 3rd. Changing the Discussion about On-Pump versus Off-Pump CABG. N. Engl. J. Med. 2017, 377, 692–693. [Google Scholar] [CrossRef]
- Rastan, A.J.; Walther, T.; Falk, V.; Kempfert, J.; Merk, D.; Lehmann, S.; Holzhey, D.; Mohr, F.W. Does Reasonable Incomplete Surgical Revascularization Affect Early or Long-Term Survival in Patients with Multivessel Coronary Artery Disease Receiving Left Internal Mammary Artery Bypass to Left Anterior Descending Artery? Circulation 2009, 120, 70–77. [Google Scholar] [CrossRef]
- Benedetto, U.; Gaudino, M.; Di Franco, A.; Caputo, M.; Ohmes, L.B.; Grau, J.; Glineur, D.; Girardi, L.N.; Angelini, G.D. Incomplete revascularization and long-term survival after coronary artery bypass surgery. Int. J. Cardiol. 2018, 254, 59–63. [Google Scholar] [CrossRef]
- Bell, M.R.; Gersh, B.J.; Schaff, H.V.; Holmes, D.R.; Fisher, L.D.; Alderman, E.L.; Myers, W.O.; Parsons, L.S.; Reeder, G.S. Effect of completeness of revascularization on long-term outcome of patients with three-vessel disease undergoing coronary artery bypass surgery. A report from the Coronary Artery Surgery Study (CASS) Registry. Circulation 1992, 86, 446–457. [Google Scholar] [CrossRef]
- Yang, Z.K.; Zhang, R.Y.; Hu, J.; Zhang, Q.; Ding, F.H.; Shen, W.F. Impact of successful staged revascularization of a chronic total occlusion in the non-infarct-related artery on long-term outcome in patients with acute ST-segment elevation myocardial infarction. Int. J. Cardiol. 2013, 165, 76–79. [Google Scholar] [CrossRef]
- Shroyer, A.L.; Hattler, B.; Wagner, T.H.; Collins, J.F.; Baltz, J.H.; Quin, J.A.; Almassi, G.H.; Kozora, E.; Bakaeen, F.; Cleveland, J.C., Jr.; et al. Five-Year Outcomes after On-Pump and Off-Pump Coronary-Artery Bypass. N. Engl. J. Med. 2017, 377, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Lamy, A.; Devereaux, P.J.; Prabhakaran, D.; Taggart, D.P.; Hu, S.; Straka, Z.; Piegas, L.S.; Avezum, A.; Akar, A.R.; Zanetti, F.L.; et al. Five-Year Outcomes after Off-Pump or On-Pump Coronary-Artery Bypass Grafting. N. Engl. J. Med. 2016, 375, 2359–2368. [Google Scholar] [CrossRef] [PubMed]
- Quin, J.A.; Wagner, T.H.; Hattler, B.; Carr, B.M.; Collins, J.; Almassi, G.H.; Grover, F.L.; Shroyer, A.L. Ten-Year Outcomes of Off-Pump vs. On-Pump Coronary Artery Bypass Grafting in the Department of Veterans Affairs: A Randomized Clinical Trial. JAMA Surg. 2022, 157, 303. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Off-Pump CABG (n = 52) | On-Pump CABG (n = 46) | p Value |
|---|---|---|---|
| Age—year | 58.4 ± 14.1 | 52.2 ± 11.5 | 0.019 |
| Male sex—no. (%) | 40 (76.9%) | 38 (82.6%) | 0.486 |
| BMI | 24.1 ± 3.0 | 23.5 ± 2.9 | 0.345 |
| Smoke | 26 (50.0%) | 22 (47.8%) | 0.830 |
| Clinical history—no. (%) | |||
| Hypertension | 38 (73.1%) | 22 (47.8%) | 0.010 |
| Diabetes | 24 (46.2%) | 16 (34.8%) | 0.253 |
| Myocardial infarction | 36 (69.2%) | 26 (56.5%) | 0.193 |
| PCI | 18 (34.6%) | 18 (39.1%) | 0.644 |
| Peripheral arterial disease | 10 (19.2%) | 4 (8.7%) | 0.137 |
| Stroke | 20 (38.5%) | 18 (39.1%) | 0.946 |
| Renal insufficiency | 10 (19.2%) | 4 (8.7%) | 0.137 |
| Hepatic insufficiency | 10 (19.2%) | 6 (13.0%) | 0.408 |
| COPD | 18 (34.6%) | 24 (52.2%) | 0.080 |
| Atrial fibrillation | 9 (17.3%) | 6 (13.0%) | 0.558 |
| LVEF—% | 31.3 ± 3.3 | 31.6 ± 2.6 | 0.404 |
| LVEDD—cm | 6.3 ± 0.4 | 6.4 ± 0.5 | 0.394 |
| IABP use—no. (%) | 4 (7.7%) | 4 (8.7%) | 1.000 |
| Urgent surgery—no. (%) | 4 (7.7%) | 2 (4.3%) | 0.681 |
| Diseased vessels—no./total no. (%) | |||
| 1-Vessel | 0 (0.0%) | 0 (0.0%) | - |
| 2-Vessel | 8 (15.4%) | 4 (8.7%) | 0.313 |
| 3-Vessel | 44 (84.6%) | 42 (91.3%) | 0.313 |
| Mean of diseased vessels | 2.8 ± 0.4 | 2.9 ± 0.3 | 0.311 |
| Left main > 50% | 16 (30.8%) | 10 (21.7%) | 0.312 |
| Characteristic | Off-Pump CABG (n = 44) | On-Pump CABG (n = 44) | p Value |
|---|---|---|---|
| Age—year | 56.9 ± 13.8 | 52.6 ± 11.6 | 0.116 |
| Male sex—no. (%) | 32 (72.7%) | 36 (81.8%) | 0.309 |
| BMI | 24.3 ± 3.1 | 23.4 ± 2.9 | 0.164 |
| Smoke | 25 (56.8%) | 21 (47.7%) | 0.393 |
| Clinical history—no. (%) | |||
| Hypertension | 30 (68.2%) | 22 (50.0%) | 0.083 |
| Diabetes | 19 (43.2%) | 16 (36.4%) | 0.513 |
| Myocardial infarction | 31 (70.5%) | 24 (54.5%) | 0.123 |
| PCI | 17 (38.6%) | 18 (40.9%) | 0.828 |
| Peripheral arterial disease | 7 (15.9%) | 4 (9.1%) | 0.334 |
| Stroke | 16 (36.4%) | 18 (40.9%) | 0.661 |
| Renal insufficiency | 10 (22.7%) | 4 (9.1%) | 0.080 |
| Hepatic insufficiency | 9 (20.5%) | 6 (13.6%) | 0.395 |
| COPD | 18 (40.9%) | 22 (50.0%) | 0.392 |
| Atrial fibrillation | 8 (18.2%) | 5 (11.4%) | 0.367 |
| LVEF—% | 31.3 ± 3.1 | 31.5 ± 2.7 | 0.640 |
| LVEDD—cm | 6.4 ± 0.4 | 6.4 ± 0.5 | 0.550 |
| IABP use—no. (%) | 3 (6.8%) | 2 (4.5%) | 1.000 |
| Urgent surgery—no. (%) | 4 (9.1%) | 2 (4.5%) | 0.676 |
| Diseased vessels—no./total no. (%) | |||
| 1-Vessel | 0 (0.0%) | 0 (0.0%) | - |
| 2-Vessel | 7 (15.9%) | 3 (6.8%) | 0.179 |
| 3-Vessel | 37 (84.1%) | 41 (93.2%) | 0.179 |
| Mean of diseased vessels | 2.8 ± 0.4 | 2.9 ± 0.3 | 0.184 |
| Left main > 50% | 12 (27.3%) | 10 (22.7%) | 0.622 |
| Characteristics | Off-Pump CABG (n = 52) | On-Pump CABG (n = 46) | p Value |
|---|---|---|---|
| Operative characteristics | |||
| No. of distal anastomosis—mean | 3.2 ± 0.8 | 3.6 ± 0.9 | 0.023 |
| LIMA use—no. (%) | 47 (90.4%) | 41 (89.1%) | 1.000 |
| Incomplete revascularization—no. (%) | 13 (25.0%) | 4 (8.7%) | 0.033 |
| Ventilator assistance time—hours, mean | 35.7 ± 37.1 | 46.2 ± 35.4 | 0.156 |
| Postoperative ICU stay—days, mean | 3.1 ± 4.2 | 4.7 ± 7.7 | 0.200 |
| Hospital stay time—days, mean | 28.4 ± 8.3 | 30.4 ± 9.7 | 0.713 |
| Mean of postoperative LVEF | 42.9 ± 8.2 | 41.3 ± 9.9 | 0.733 |
| Mean of postoperative LVEDD | 5.6 ± 0.6 | 5.8 ± 0.8 | 0.189 |
| Early outcome | |||
| Primary outcomes—no. (%) | |||
| Death | 3 (5.8%) | 2 (4.3%) | 1.000 |
| Myocardial infarction | 3 (5.8%) | 3 (6.5%) | 1.000 |
| Stroke | 4 (7.7%) | 4 (8.7%) | 1.000 |
| New renal failure requiring dialysis | 2 (3.8%) | 6 (13.0%) | 0.142 |
| Other outcomes—no. (%) | |||
| New-onset atrial fibrillation | 8 (15.4%) | 12 (26.1%) | 0.190 |
| Low cardiac output syndrome | 14 (26.9%) | 18 (39.1%) | 0.198 |
| IABP use | 5 (9.6%) | 12 (26.1%) | 0.032 |
| Respiratory failure or infection | 6 (11.5%) | 6 (13.0%) | 0.821 |
| Renal insufficiency | 7 (13.5%) | 13 (28.3%) | 0.070 |
| Hepatic insufficiency | 10 (19.2%) | 12 (26.1%) | 0.417 |
| Reoperation for bleeding | 1 (1.9%) | 4 (8.7%) | 0.183 |
| Sternum Infection | 0 (0.0%) | 2 (4.3%) | 0.218 |
| Characteristics | Off-Pump CABG (n = 44) | On-Pump CABG (n = 44) | p Value |
|---|---|---|---|
| Operative characteristics | |||
| No. of distal anastomosis—mean | 3.2 ± 0.9 | 3.6 ± 1.0 | 0.080 |
| LIMA use—no. (%) | 41 (93.2%) | 40 (90.9%) | 1.000 |
| Incomplete revascularization—no. (%) | 11 (25.0%) | 4 (9.1%) | 0.047 |
| Ventilator assistance time—hours, mean | 36.7 ± 39.2 | 47.1 ± 35.9 | 0.199 |
| Postoperative ICU stay—days, mean | 3.1 ± 4.4 | 4.4 ± 7.8 | 0.358 |
| Hospital stay time—days, mean | 29.6 ± 23.0 | 28.8. ± 15.1 | 0.852 |
| Mean of postoperative LVEF | 42.0 ± 8.6 | 41.3 ± 10.1 | 0.742 |
| Mean of postoperative LVEDD | 5.7 ± 0.6 | 5.8 ± 0.8 | 0.253 |
| Early outcome | |||
| Primary outcomes—no. (%) | |||
| Death | 2 (4.5%) | 2 (4.5%) | 1.000 |
| Myocardial infarction | 3 (6.8%) | 4 (9.1%) | 1.000 |
| Stroke | 3 (4.5%) | 3 (4.5%) | 1.000 |
| New renal failure requiring dialysis | 2 (4.5%) | 5 (11.4%) | 0.434 |
| Other outcomes—no. (%) | |||
| New-onset atrial fibrillation | 7 (15.9%) | 12 (27.3%) | 0.195 |
| Low cardiac output syndrome | 13 (29.5%) | 17 (38.6%) | 0.368 |
| IABP use | 4 (9.1%) | 11 (25.0%) | 0.047 |
| Respiratory failure or infection | 4 (9.1%) | 6 (13.6%) | 0.502 |
| Renal insufficiency | 5 (11.4%) | 13 (29.5%) | 0.034 |
| Hepatic insufficiency | 9 (20.5%) | 12 (27.3%) | 0.453 |
| Reoperation for bleeding | 1 (2.3%) | 4 (9.1%) | 0.360 |
| Sternum Infection | 0 (0.0%) | 2 (4.5%) | 0.494 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Jiang, Y.; Wang, Q.; Tian, R.; Wang, D.; Jiang, X.; Dong, N.; Chen, S.; Chen, X. Early and Long-Term Outcomes after On-Pump and Off-Pump Coronary-Artery Bypass Grafting in Patients with Severe Left Ventricular Dysfunction and a Giant Left Ventricle. J. Cardiovasc. Dev. Dis. 2022, 9, 298. https://doi.org/10.3390/jcdd9090298
Wang C, Jiang Y, Wang Q, Tian R, Wang D, Jiang X, Dong N, Chen S, Chen X. Early and Long-Term Outcomes after On-Pump and Off-Pump Coronary-Artery Bypass Grafting in Patients with Severe Left Ventricular Dysfunction and a Giant Left Ventricle. Journal of Cardiovascular Development and Disease. 2022; 9(9):298. https://doi.org/10.3390/jcdd9090298
Chicago/Turabian StyleWang, Chen, Yefan Jiang, Qingpeng Wang, Rui Tian, Dashuai Wang, Xionggang Jiang, Nianguo Dong, Si Chen, and Xinzhong Chen. 2022. "Early and Long-Term Outcomes after On-Pump and Off-Pump Coronary-Artery Bypass Grafting in Patients with Severe Left Ventricular Dysfunction and a Giant Left Ventricle" Journal of Cardiovascular Development and Disease 9, no. 9: 298. https://doi.org/10.3390/jcdd9090298