
Stroke Risks in Primary Aldosteronism with Different Treatments: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Quality Assessment
2.3. Outcomes of Interest
2.4. Statistical Analysis
3. Results
3.1. Included Studies
3.2. Risk of Bias Assessment
3.3. PA Patients Receiving Surgical Adrenalectomy Treatment Compared to the PA Patients Receiving Medical Treatment
3.4. PA Patients Receiving Medical Treatment Compared to the EH Patients
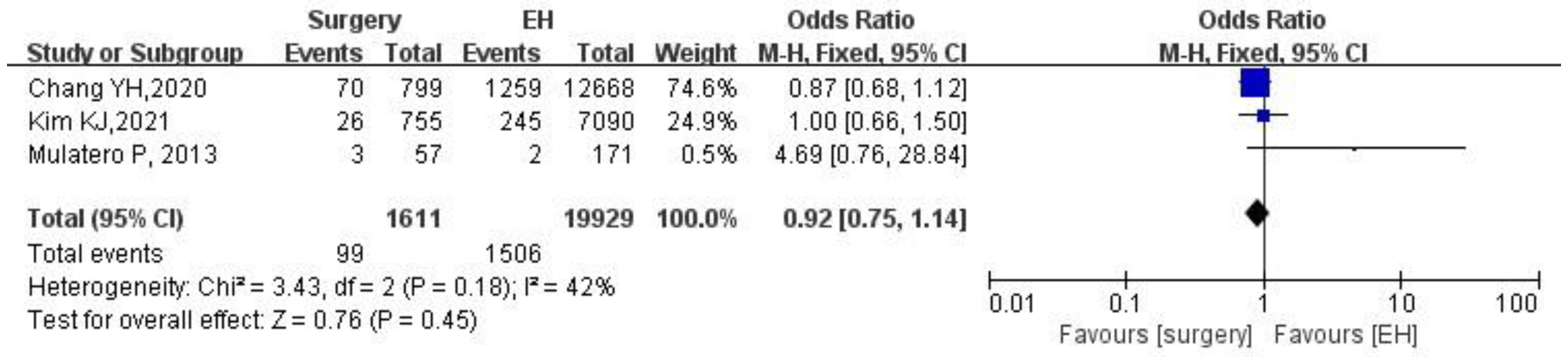
3.5. PA Patients Receiving Surgical Adrenalectomy Treatment Compared to the EH Patients
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stowasse, M.; Gordon, R.D. Primary Aldosteronism: Changing Definitions and New Concepts of Physiology and Pathophysiology Both Inside and Outside the Kidney. Physiol. Rev. 2016, 96, 1327–1384. [Google Scholar] [CrossRef] [PubMed]
- Funder, J.W.; Carey, R.M.; Mantero, F.; Murad, M.H.; Reincke, M.; Shibata, H.; Stowasser, M.; Young, W.F. The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2016, 101, 1889–1916. [Google Scholar] [CrossRef] [PubMed]
- Monticone, S.; Burrello, J.; Tizzani, D.; Bertello, C.; Viola, A.; Buffolo, F.; Gabetti, L.; Mengozzi, G.; Williams, T.A.; Rabbia, F.; et al. Prevalence and Clinical Manifestations of Primary Aldosteronism Encountered in Primary Care Practice. J. Am. Coll. Cardiol. 2017, 69, 1811–1820. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.M.; Robinson-Cohen, C.; Luque-Fernandez, M.A.; Allison, M.A.; Baudrand, R.; Ix, J.H.; Kestenbaum, B.; De Boer, I.H.; Vaidya, A. The Spectrum of Subclinical Primary Aldosteronism and Incident Hypertension: A Cohort Study. Ann. Intern. Med. 2017, 167, 630–641. [Google Scholar] [CrossRef]
- Calhoun, D.A.; Nishizaka, M.K.; Zaman, M.A.; Thakkar, R.B.; Weissmann, P. Hyperaldosteronism Among Black and White Subjects with Resistant Hypertension. Hypertension 2002, 40, 892–896. [Google Scholar] [CrossRef]
- Monticone, S.; D’Ascenzo, F.; Moretti, C.; Williams, T.A.; Veglio, F.; Gaita, F.; Mulatero, P. Cardiovascular events and target organ damage in primary aldosteronism compared with essential hypertension: A systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2018, 6, 41–50. [Google Scholar] [CrossRef]
- Feigin, V.L.; Vos, T.; Nichols, E.; Owolabi, M.O.; Carroll, W.M.; Dichgans, M.; Deuschl, G.; Parmar, P.; Brainin, M.; Murray, C. The global burden of neurological disorders: Translating evidence into policy. Lancet Neurol. 2019, 19, 255–265. [Google Scholar] [CrossRef]
- Feigin, V.L. Primary stroke prevention: Useful thresholds? Lancet Neurol. 2021, 21, 116. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-analyses of Health Care Interventions: Checklist and Explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.J.; Hong, N.; Yu, M.H.; Lee, H.; Lee, S.; Lim, J.S.; Rhee, Y. Time-Dependent Risk of Atrial Fibrillation in Patients with Primary Aldosteronism After Medical or Surgical Treatment Initiation. Hypertension 2021, 77, 1964–1973. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-H.; Chung, S.-D.; Wu, C.-H.; Chueh, J.S.; Chen, L.; Lin, P.-C.; Lin, Y.-H.; Huang, K.-H.; Wu, V.-C.; Chu, T.-S. Surgery decreases the long-term incident stroke risk in patients with primary aldosteronism. Surgery 2020, 167, 367–377. [Google Scholar] [CrossRef] [PubMed]
- Mulatero, P.; Monticone, S.; Bertello, C.; Viola, A.; Tizzani, D.; Iannaccone, A.; Crudo, V.; Burrello, J.; Milan, A.; Rabbia, F.; et al. Long-Term Cardio- and Cerebrovascular Events in Patients with Primary Aldosteronism. J. Clin. Endocrinol. Metab. 2013, 98, 4826–4833. [Google Scholar] [CrossRef]
- McCarthy, J.; Yang, J.; Clissold, B.; Young, M.J.; Fuller, P.J.; Phan, T. Hypertension Management in Stroke Prevention: Time to Consider Primary Aldosteronism. Stroke 2021, 52, e626–e634. [Google Scholar] [CrossRef]
- Picado, O.; Whitfield, B.W.; Khan, Z.F.; Jeraq, M.; Farrá, J.C.; Lew, J.I. Long-term outcome success after operative treatment for primary aldosteronism. Surgery 2020, 169, 528–532. [Google Scholar] [CrossRef]
- Williams, A.T.; Lenders, J.W.M.; Mulatero, P.; Burrello, J.; Rottenkolber, M.; Adolf, C.; Satoh, F.; Amar, L.; Quinkler, M.; Deinum, J.; et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: An international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol. 2017, 5, 689–699. [Google Scholar] [CrossRef]
- Sawka, A.M.; Young, W.F.; Thompson, G.B.; Grant, C.S.; Farley, D.R.; Leibson, C.; Van Heerden, J.A. Primary Aldosteronism: Factors Associated with Normalization of Blood Pressure after Surgery. Ann. Intern. Med. 2001, 135, 258–261. [Google Scholar] [CrossRef]
- Huang, W.-C.; Chen, Y.-Y.; Lin, Y.-H.; Chueh, J.S. Composite Cardiovascular Outcomes in Patients with Primary Aldosteronism Undergoing Medical Versus Surgical Treatment: A Meta-Analysis. Front. Endocrinol. 2021, 12, 644260. [Google Scholar] [CrossRef]
- Savard, S.; Amar, L.; Plouin, P.F.; Steichen, O. Cardiovascular complications associated with primary aldosteronism: A controlled cross-sectional study. Hypertension 2013, 62, 331–336. [Google Scholar] [CrossRef] [Green Version]
- Milliez, P.; Girerd, X.; Plouin, P.-F.; Blacher, J.; Safar, M.E.; Mourad, J.-J. Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. J. Am. Coll. Cardiol. 2005, 45, 1243–1248. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Seccia, T.M.; Caroccia, B.; Adler, G.K.; Maiolino, G.; Cesari, M.; Rossi, G.P. Arterial Hypertension, Atrial Fibrillation, and Hyperaldosteronism: The Triple Trouble. Hypertension 2017, 69, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.-H.; Chen, Y.-L.; Pan, C.-T.; Lin, Y.-T.; Lee, P.-C.; Chiu, Y.-W.; Liao, C.-W.; Chen, Z.-W.; Chang, C.-C.; Chang, Y.-Y.; et al. New-Onset Atrial Fibrillation in Patients with Primary Aldosteronism Receiving Different Treatment Strategies: Systematic Review and Pooled Analysis of Three Studies. Front. Endocrinol. 2021, 12, 646933. [Google Scholar] [CrossRef]
- Rocha, R.; Rudolph, A.E.; Frierdich, G.E.; Nachowiak, D.A.; Kekec, B.K.; Blomme, E.A.G.; McMahon, E.G.; Delyani, J.A. Aldosterone induces a vascular inflammatory phenotype in the rat heart. Am. J. Physiol. Circ. Physiol. 2002, 283, H1802–H1810. [Google Scholar] [CrossRef]
- Kuster, G.M.; Kotlyar, E.; Rude, M.K.; Siwik, D.A.; Liao, R.; Colucci, W.S.; Sam, F. Mineralocorticoid Receptor Inhibition Ameliorates the Transition to Myocardial Failure and Decreases Oxidative Stress and Inflammation in Mice with Chronic Pressure Overload. Circulation 2005, 111, 420–427. [Google Scholar] [CrossRef]
- Blasi, E.R.; Rocha, R.; Rudolph, A.E.; Blomme, E.A.; Polly, M.L.; McMahon, E.G. Aldosterone/salt induces renal inflammation and fibrosis in hypertensive rats. Kidney Int. 2003, 63, 1791–1800. [Google Scholar] [CrossRef]
- Lin, X.; Ullah, M.H.E.; Wu, X.; Xu, F.; Shan, S.-K.; Lei, L.-M.; Yuan, L.-Q.; Liu, J. Cerebro-Cardiovascular Risk, Target Organ Damage, and Treatment Outcomes in Primary Aldosteronism. Front. Cardiovasc. Med. 2022, 8, 621. [Google Scholar] [CrossRef]
- Reincke, M.; Bancos, I.; Mulatero, P.; Scholl, I.U.; Stowasser, M.; Williams, T.A. Diagnosis and treatment of primary aldosteronism. Lancet Diabetes Endocrinol. 2021, 9, 876–892. [Google Scholar] [CrossRef]
- Pillai, P.R.; Griffith, M.; Schwarcz, M.D.; Weiss, I.A. Primary Aldosteronism: Cardiovascular Risk, Diagnosis, and Management. Cardiol. Rev. 2020, 28, 84–91. [Google Scholar] [CrossRef]
- Magill, S.B.; Raff, H.; Shaker, J.L.; Brickner, R.C.; Knechtges, T.E.; Kehoe, M.E.; Findling, J.W. Comparison of Adrenal Vein Sampling and Computed Tomography in the Differentiation of Primary Aldosteronism. J. Clin. Endocrinol. Metab. 2001, 86, 1066–1071. [Google Scholar] [CrossRef] [PubMed]
- Hundemer, G.L.; Curhan, G.C.; Yozamp, N.; Wang, M.; Vaidya, A. Renal Outcomes in Medically and Surgically Treated Primary Aldosteronism. Hypertension 2018, 72, 658–666. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Kim KJ, 2021 [12] | Chang YH, 2020 [13] | Mulatero P, 2013 [14] | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PA | EH | p Value | PA | EH | p Value | PA | EH | p Value | ||||
| Medical | Surgery | Medical | Surgery | Medical | Surgery | |||||||
| Study nature | Retrospective | Retrospective | Retrospective | |||||||||
| Duration of follow-up | Median 5 years | Minimum 1 year, maximum 13 years | Median 12 years | |||||||||
| Number of patients | 663 | 755 | 7090 | 2368 | 799 | 12,668 | 213 | 57 | 810 | |||
| Male, N (%) | 657 (46.33) | 3285 (46.33) | 0.999 | 1443 (45.6) | 5988 (47.3) | 0.087 | 161(59.63) | 483(59.63) | 1 | |||
| Age, y | 48.83 ± 11.32 | 48.99 ± 11.34 | 0.639 | 50.8 ± 14.5 | 50.8 ± 14.5 | 0.992 | 44 ± 8.5 | 44 ± 11.4 | 0.98 | |||
| Diabetes, N (%) | 244 (17.21) | 1404 (19.80) | 0.005 | 425(13.4) | 1841(14.5) | 0.112 | 11(4.1) | 33(4.1) | 1 | |||
| Dyslipidemia, N (%) | 579 (40.83) | 3506 (49.45) | <0.001 | 465(14.7) | 2007 (15.8) | 0.112 | 74(27,3) | 241(29.7) | 0.46 | |||
| CKD, N (%) | 137 (9.66) | 236 (3.33) | <0.001 | 70(2.2) | 271(2.1) | 0.785 | N/R | N/R | N/R | |||
| Domain 1: Confounding | Domain 2: Selection | Domain 3: Classification of Intervention | Domain 4: Deviation from Interventions | Domain 5: Missing Data | Domain 6: Measurement of Outcomes | Domain 7: Selection of Reported Result | ROBINS-I Overall | |
|---|---|---|---|---|---|---|---|---|
| Kim KJ, 2021 [12] | 2–3 | 2–3 | 1 | 1–2 | 1 | 1–2 | 1 | 2 Moderate |
| Chang YH, 2020 [13] | 3 | 1–2 | 1 | 1–2 | 1 | 2–3 | 1 | 2 Moderate |
| Mulatero P, 2013 [14] | 2 | 2 | 1 | 1–2 | 1–2 | 2 | 2 | 2 Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qian, N.; Xu, J.; Wang, Y. Stroke Risks in Primary Aldosteronism with Different Treatments: A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2022, 9, 300. https://doi.org/10.3390/jcdd9090300
Qian N, Xu J, Wang Y. Stroke Risks in Primary Aldosteronism with Different Treatments: A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease. 2022; 9(9):300. https://doi.org/10.3390/jcdd9090300
Chicago/Turabian StyleQian, Ningjing, Jingmiao Xu, and Yaping Wang. 2022. "Stroke Risks in Primary Aldosteronism with Different Treatments: A Systematic Review and Meta-Analysis" Journal of Cardiovascular Development and Disease 9, no. 9: 300. https://doi.org/10.3390/jcdd9090300