
Impact of Clinical and Morphological Factors on Long-Term Mortality in Patients with Myocardial Bridge

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistics
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, M.S.; Chen, C.H. Myocardial Bridging: An Up-to-Date Review. J. Invasive Cardiol. 2015, 27, 521–528. [Google Scholar]
- Soran, O.; Pamir, G.; Erol, C.; Kocakavak, C.; Sabah, I. The incidence and significance of myocardial bridge in a prospectively defined population of patients undergoing coronary angiography for chest pain. Tokai J. Exp. Clin. Med. 2000, 25, 57–60. [Google Scholar] [PubMed]
- Mohlenkamp, S.; Hort, W.; Ge, J.; Erbel, R. Update on myocardial bridging. Circulation 2002, 106, 2616–2622. [Google Scholar] [CrossRef]
- Lubarsky, L.; Gupta, M.P.; Hecht, H.S. Evaluation of myocardial bridging of the left anterior descending coronary artery by 64-slice multidetector computed tomographic angiography. Am. J. Cardiol. 2007, 100, 1081–1082. [Google Scholar] [CrossRef] [PubMed]
- Tarantini, G.; Migliore, F.; Cademartiri, F.; Fraccaro, C.; Iliceto, S. Left Anterior Descending Artery Myocardial Bridging: A Clinical Approach. J. Am. Coll. Cardiol. 2016, 68, 2887–2899. [Google Scholar] [CrossRef] [PubMed]
- Yan, F.; Chen, Y. A case of sudden death due to myocardial bridging of the left anterior descending coronary artery. Chin. Med. J. 2014, 127, 2553. [Google Scholar] [PubMed]
- Arjomand, H.; AlSalman, J.; Azain, J.; Amin, D. Myocardial bridging of left circumflex coronary artery associated with acute myocardial infarction. J. Invasive Cardiol. 2000, 12, 431–434. [Google Scholar]
- Zóka, A.; Andreka, P.; Becker, D.; Fontos, G.; Merkely, B.; Szabó, G.; Szatmári, A.; Bárczi, G. Ventricular septal rupture caused by myocardial bridge, solved by interventional closure device. Croat. Med. J. 2012, 53, 627–630. [Google Scholar] [CrossRef]
- Cutler, D.; Wallace, J.M. Myocardial bridging in a young patient with sudden death. Clin. Cardiol. 1997, 20, 581–583. [Google Scholar] [CrossRef]
- Roul, G.; Sens, P.; Germain, P.; Bareiss, P. Myocardial bridging as a cause of acute transient left heart dysfunction. Chest 1999, 116, 574–580. [Google Scholar] [CrossRef]
- Alegria, J.R.; Herrmann, J.; Holmes, D.R., Jr.; Lerman, A.; Rihal, C.S. Myocardial bridging. Eur. Heart J. 2005, 26, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Haager, P.K.; Schwarz, E.R.; Vom Dahl, J.; Klues, H.G.; Reffelmann, T.; Hanrath, P. Long term angiographic and clinical follow up in patients with stent implantation for symptomatic myocardial bridging. Heart 2000, 84, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Ge, J.; Erbel, R.; Rupprecht, H.J.; Koch, L.; Kearney, P.; Görge, G.; Haude, M.; Meyer, J. Comparison of intravascular ultrasound and angiography in the assessment of myocardial bridging. Circulation 1994, 89, 1725–1732. [Google Scholar] [CrossRef] [Green Version]
- Cao, H.M.; Jiang, J.F.; Deng, B.; Xu, J.H.; Xu, W.J. Evaluation of myocardial bridges with optical coherence tomography. J. Int. Med. Res. 2010, 38, 681–685. [Google Scholar] [CrossRef] [PubMed]
- Kurtoglu, N.; Mutlu, B.; Soydinc, S.; Tanalp, C.; Izgi, A.; Dagdelen, S.; Bakkal, R.B.; Dindar, I. Normalization of coronary fractional flow reserve with successful intracoronary stent placement to a myocardial bridge. J. Interv. Cardiol. 2004, 17, 33–36. [Google Scholar] [CrossRef]
- Cay, S.; Ozturk, S.; Cihan, G.; Kisacik, H.L.; Korkmaz, S. Angiographic prevalence of myocardial bridging. Anadolu Kardiyol. Derg. 2006, 6, 9–12. [Google Scholar] [PubMed]
- Lazoura, O.; Kanavou, T.; Vassiou, K.; Gkiokas, S.; Fezoulidis, I.V. Myocardial bridging evaluated with 128-multi detector computed tomography coronary angiography. Surg. Radiol. Anat. 2010, 32, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.H.; Yang, Q.; Chen, J.H.; Wang, X.M.; Wang, M.; Liu, C. Myocardial bridging on dual-source computed tomography: Degree of systolic compression of mural coronary artery correlating with length and depth of the myocardial bridge. Clin. Imaging 2010, 34, 83–88. [Google Scholar] [CrossRef]
- Elmali, M.; Soylu, K.; Gulel, O.; Bayrak, I.K.; Koprulu, D.; Diren, H.B.; Celenk, C. Correlation between depth of myocardial bridging and coronary angiography findings. Acta Radiol. 2008, 49, 883–888. [Google Scholar] [CrossRef]
- Tsujita, K.; Maehara, A.; Mintz, G.S.; Doi, H.; Kubo, T.; Castellanos, C.; Liu, J.; Yang, J.; Oviedo, C.; Franklin-Bond, T.; et al. Comparison of angiographic and intravascular ultrasonic detection of myocardial bridging of the left anterior descending coronary artery. Am. J. Cardiol. 2008, 102, 1608–1613. [Google Scholar] [CrossRef]
- Ge, J.; Jeremias, A.; Rupp, A.; Abels, M.; Baumgart, D.; Liu, F.; Haude, M.; Görge, G.; Von Birgelen, C.; Sack, S.; et al. New signs characteristic of myocardial bridging demonstrated by intracoronary ultrasound and Doppler. Eur. Heart J. 1999, 20, 1707–1716. [Google Scholar] [CrossRef] [PubMed]
- Ciçek, D.; Kalay, N.; Müderrisoğlu, H. Incidence, clinical characteristics, and 4-year follow-up of patients with isolated myocardial bridge: A retrospective, single-center, epidemiologic, coronary arteriographic follow-up study in southern Turkey. Cardiovasc. Revasc. Med. 2011, 12, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Kramer, J.R.; Kitazume, H.; Proudfit, W.L.; Sones, F.M., Jr. Clinical significance of isolated coronary bridges: Benign and frequent condition involving the left anterior descending artery. Am. Heart J. 1982, 103, 283–288. [Google Scholar] [CrossRef]
- Lozano, I.; Baz, J.A.; López Palop, R.; Pinar, E.; Picó, F.; Valdés, M.; Larman, M.; Martínez Ubago, J.L. Long-term prognosis of patients with myocardial bridge and angiographic milking of the left anterior descending coronary artery. Rev. Esp. Cardiol. 2002, 55, 359–364. [Google Scholar] [CrossRef]
- Harikrishnan, S.; Sunder, K.R.; Tharakan, J.; Titus, T.; Bhat, A.; Sivasankaran, S.; Bimal, F. Clinical and angiographic profile and follow-up of myocardial bridges: A study of 21 cases. Indian Heart J. 1999, 51, 503–507. [Google Scholar] [PubMed]
- Lindahl, B.; Baron, T.; Albertucci, M.; Prati, F. Myocardial infarction with non-obstructive coronary artery disease. Eurointervention J. Eur. Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2021, 17, e875–e887. [Google Scholar] [CrossRef]
- Bayrak, F.; Degertekin, M.; Eroglu, E.; Guneysu, T.; Sevinc, D.; Gemici, G.; Mutlu, B.; Aytaclar, S. Evaluation of myocardial bridges with 64-slice computed tomography coronary angiography. Acta Cardiologica 2009, 64, 341–346. [Google Scholar] [CrossRef]
- Kursaklioglu, H.; Barcin, C.; Iyisoy, A.; Kose, S.; Amasyali, B.; Isik, E. Angiographic restenosis after myocardial bridge stenting. Jpn. Heart J. 2004, 45, 581–589. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.S.; Jeong, M.H.; Kim, H.K.; Kim, M.C.; Cho, K.H.; Lee, M.G.; Ko, J.S.; Park, K.H.; Sim, D.S.; Yoon, N.S.; et al. Long-term clinical course of patients with isolated myocardial bridge. Circ. J. 2010, 74, 538–543. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
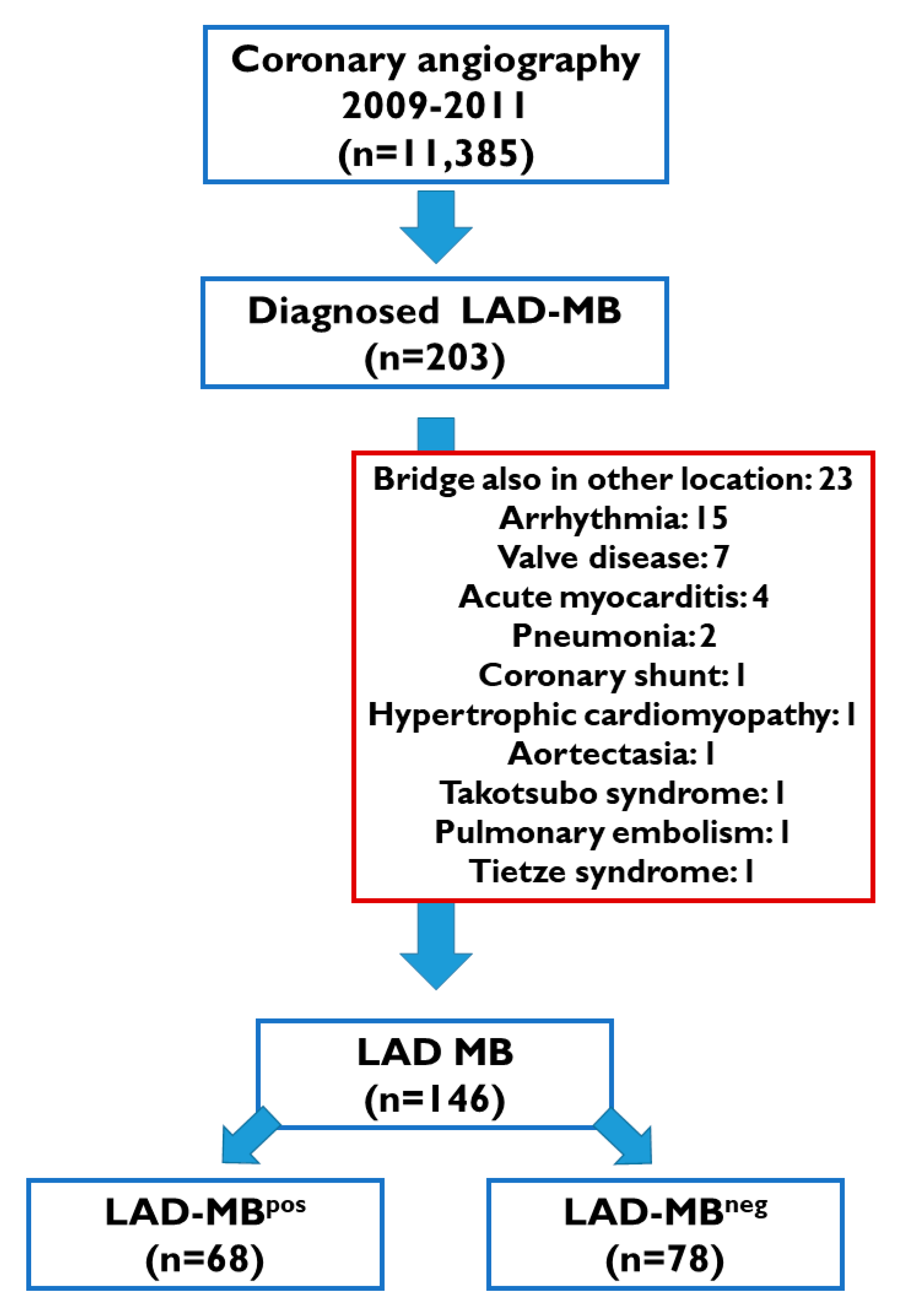
| Overall LAD-MB Population n = 146 | LAD-MBneg n = 78 | LAD-MBpos n = 68 | LAD-MBneg vs. LAD-MBpos | |
|---|---|---|---|---|
| Mean age (years) | 60.6 (12.7) | 57.6 (12.4) | 64.5 (11.5) | 0.001 |
| Male sex | 94 (64%) | 50 (64%) | 43 (64%) | 0.99 |
| Hypertension | 105 (72%) | 57 (73%) | 48 (72%) | 0.87 |
| Type 2 diabetes mellitus | 36 (25%) | 13 (17%) | 24 (36%) | 0.008 |
| Hyperlipidemia | 77 (53%) | 37 (47%) | 40 (60%) | 0.14 |
| Body mass index (kg/m2) | 27.6 (3.8) | 27.2 (3.4) | 28.2 (4.3) | 0.11 |
| LAD-MB length (mm) | 21.4 (8.2) | 23.4 (8.3) | 20.0 (7.7) | 0.05 |
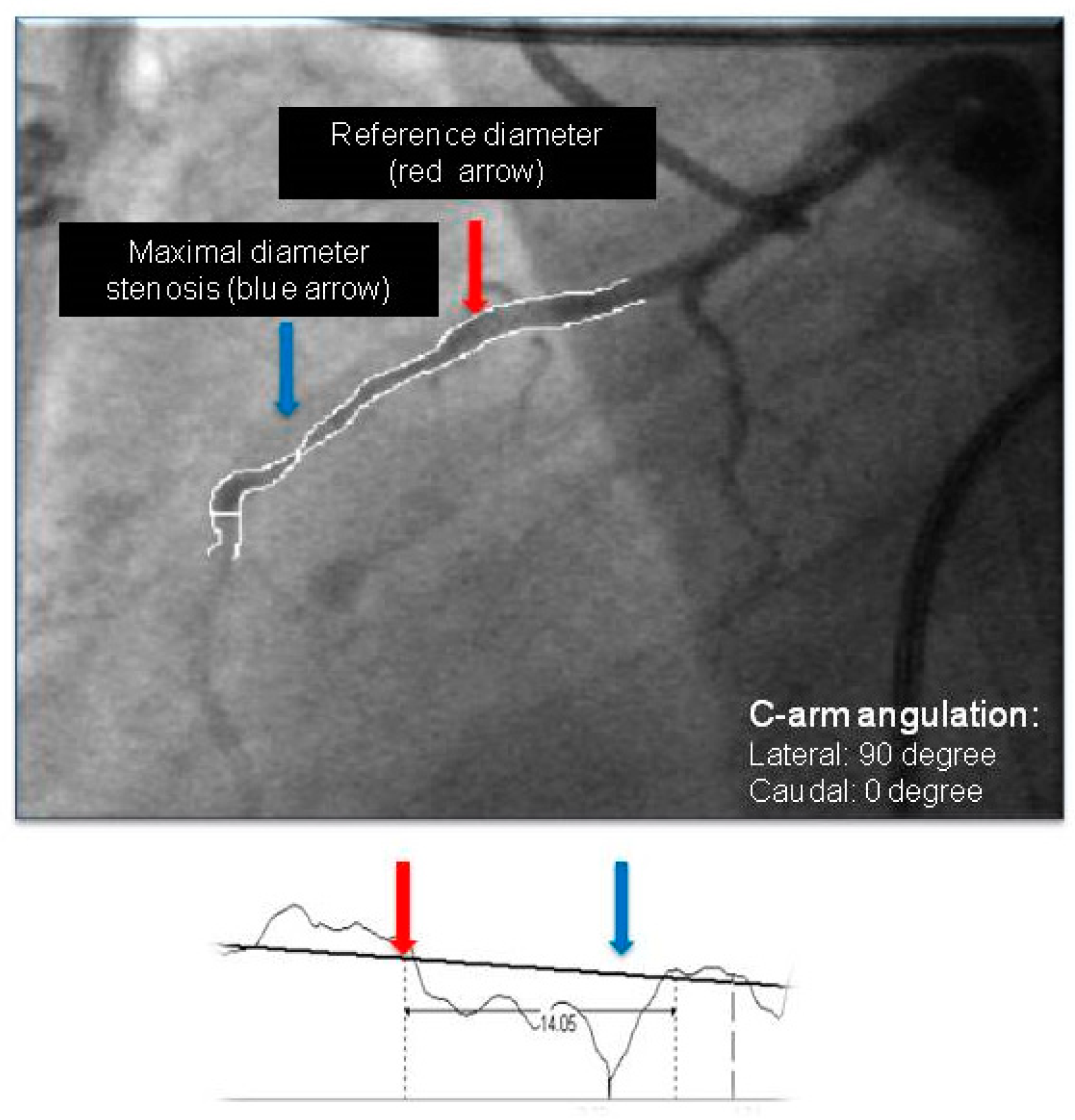
| Reference diameter (mm) | 2.18 (0.46) | 2.23 (0.42) | 2.09 (0.41) | 0.06 |
| Minimal diameter (mm) | 1.10 (0.41) | 1.02 (0.36) | 1.11 (0.38) | 0.39 |
| Minimal diameter to reference diameter (%) | 49.5 (15.5) | 54.5 (13.1) | 46.5 (16.4) | 0.006 |
| Overall LAD-MB Population n = 146 | LAD-MBneg n = 78 | |||
|---|---|---|---|---|
| Single Variable Analysis | Multiple Variable Analysis | Single Variable Analysis | Multiple Variable Analysis | |
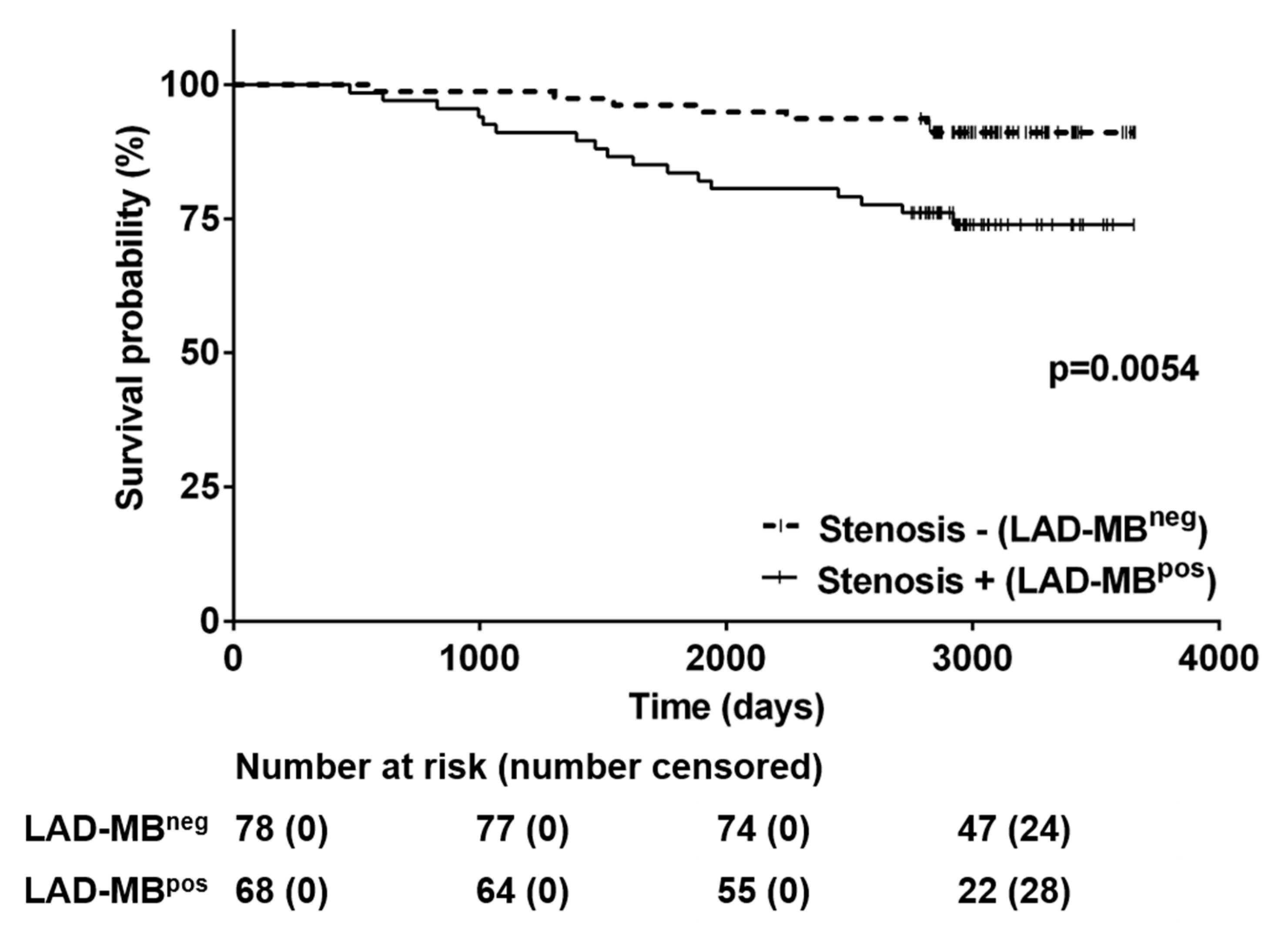
| Stenosis | HR: 3.45 p = 0.005 | HR: 2.14 (0.84–5.46) p = 0.111 | NA | NA |
| Mean age (years) | HR: 1.08 (1.04–1.12) p < 0.001 | HR: 1.08 (1.03–1.13) p = 0.001 | HR: 1.07 (1.01–1.13) p = 0.033 | HR: 1.09 (1.01–1.18) p = 0.030 |
| Male sex | HR: 0.89 (0.40–1.98) p = 0.770 | NA | HR: 0.56 (0.14–2.26) p = 0.419 | NA |
| Hypertension | HR: 1.26 (0.50–3.17) p = 0.618 | NA | HR: 1.07 (0.22–5.30) p = 0.934 | NA |
| Type 2 diabetes mellitus | HR: 2.14 (0.96–4.77) p = 0.062 | HR: 1.62 (0.71-3.71) p=0.251 | HR: 0.69 (0.09–5.59) p = 0.726 | NA |
| Hyperlipidaemia | HR: 0.69 (0.31–1.52) p = 0.355 | NA | HR: 0.64 (0.15–2.69) p = 0.546 | NA |
| BMI (kg/m2) | HR: 1.01 (0.91–1.12) p = 0.857 | NA | HR: 1.01 (0.82–1.24) p = 0.954 | NA |
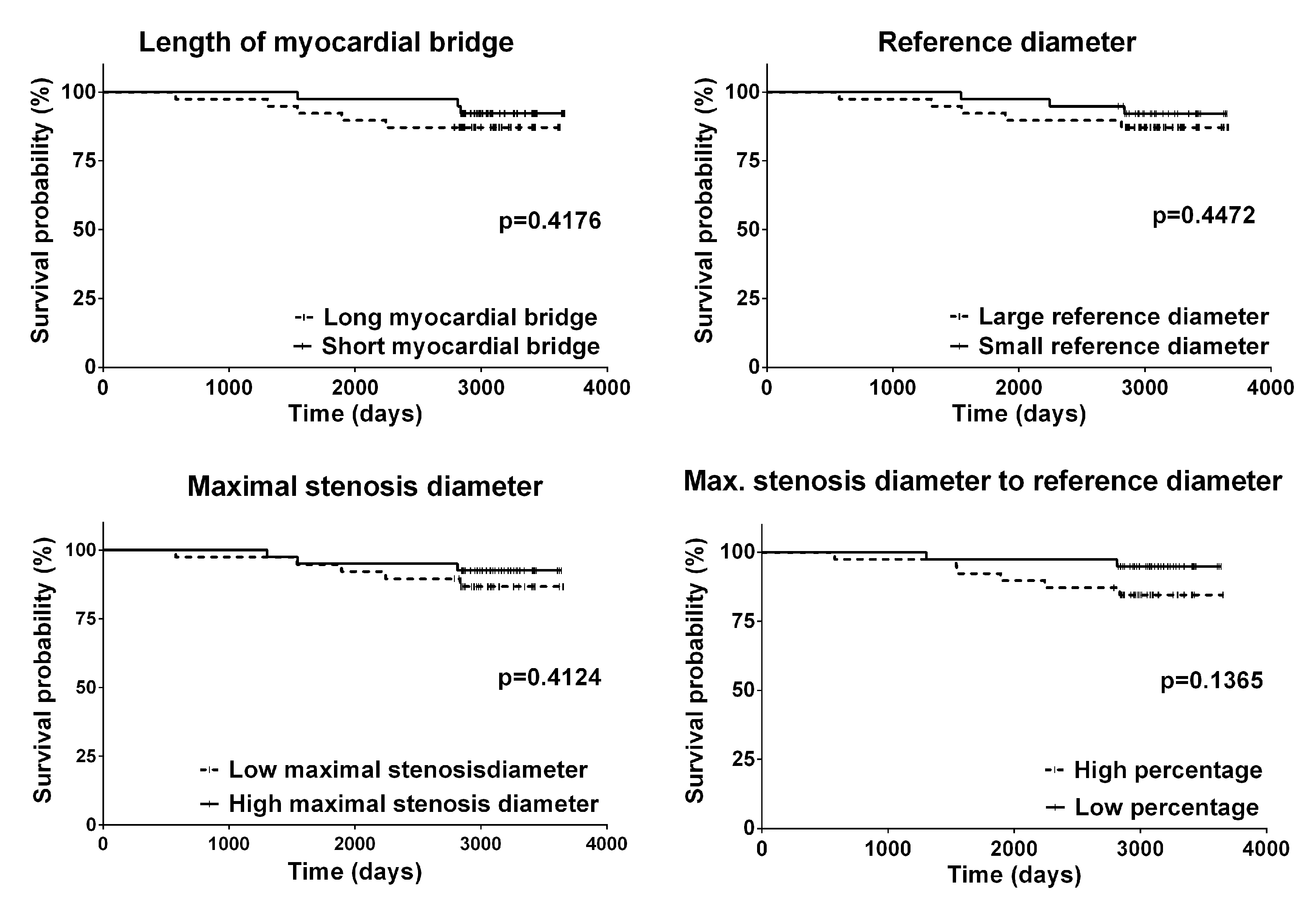
| LAD-MB length (mm) | NA | HR: 1.01 (0.96–1.06) p = 0.827 | NA | HR: 1.07 (0.97–1.19) p = 0.150 |
| Reference diameter (mm) | NA | HR: 2.73 (0.17–44.8) p = 0.482 | NA | HR: 6.30 (0.03–1534)] p = 0.512 |
| Minimal stenosis (mm) | NA | HR: 0.45 (0.01–86.8) p = 0.768 | NA | HR: 0.02 (0.01–1568) p = 0.503 |
| Minimal stenosis to reference diameter (%) | NA | HR: 0.98 (0.88–1.09) p = 0.704 | NA | HR: 0.94 (0.74–1.19) p = 0.592 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bárczi, G.; Becker, D.; Sydó, N.; Ruzsa, Z.; Vágó, H.; Oláh, A.; Merkely, B. Impact of Clinical and Morphological Factors on Long-Term Mortality in Patients with Myocardial Bridge. J. Cardiovasc. Dev. Dis. 2022, 9, 129. https://doi.org/10.3390/jcdd9050129
Bárczi G, Becker D, Sydó N, Ruzsa Z, Vágó H, Oláh A, Merkely B. Impact of Clinical and Morphological Factors on Long-Term Mortality in Patients with Myocardial Bridge. Journal of Cardiovascular Development and Disease. 2022; 9(5):129. https://doi.org/10.3390/jcdd9050129
Chicago/Turabian StyleBárczi, György, Dávid Becker, Nóra Sydó, Zoltán Ruzsa, Hajnalka Vágó, Attila Oláh, and Béla Merkely. 2022. "Impact of Clinical and Morphological Factors on Long-Term Mortality in Patients with Myocardial Bridge" Journal of Cardiovascular Development and Disease 9, no. 5: 129. https://doi.org/10.3390/jcdd9050129