
Optimal Landmark for Chest Compressions during Cardiopulmonary Resuscitation Derived from a Chest Computed Tomography in Arms-Down Position

 , and
, and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Selection of Participants
2.3. Methods of Measurement
2.3.1. Rescuer’s Hand Measurement
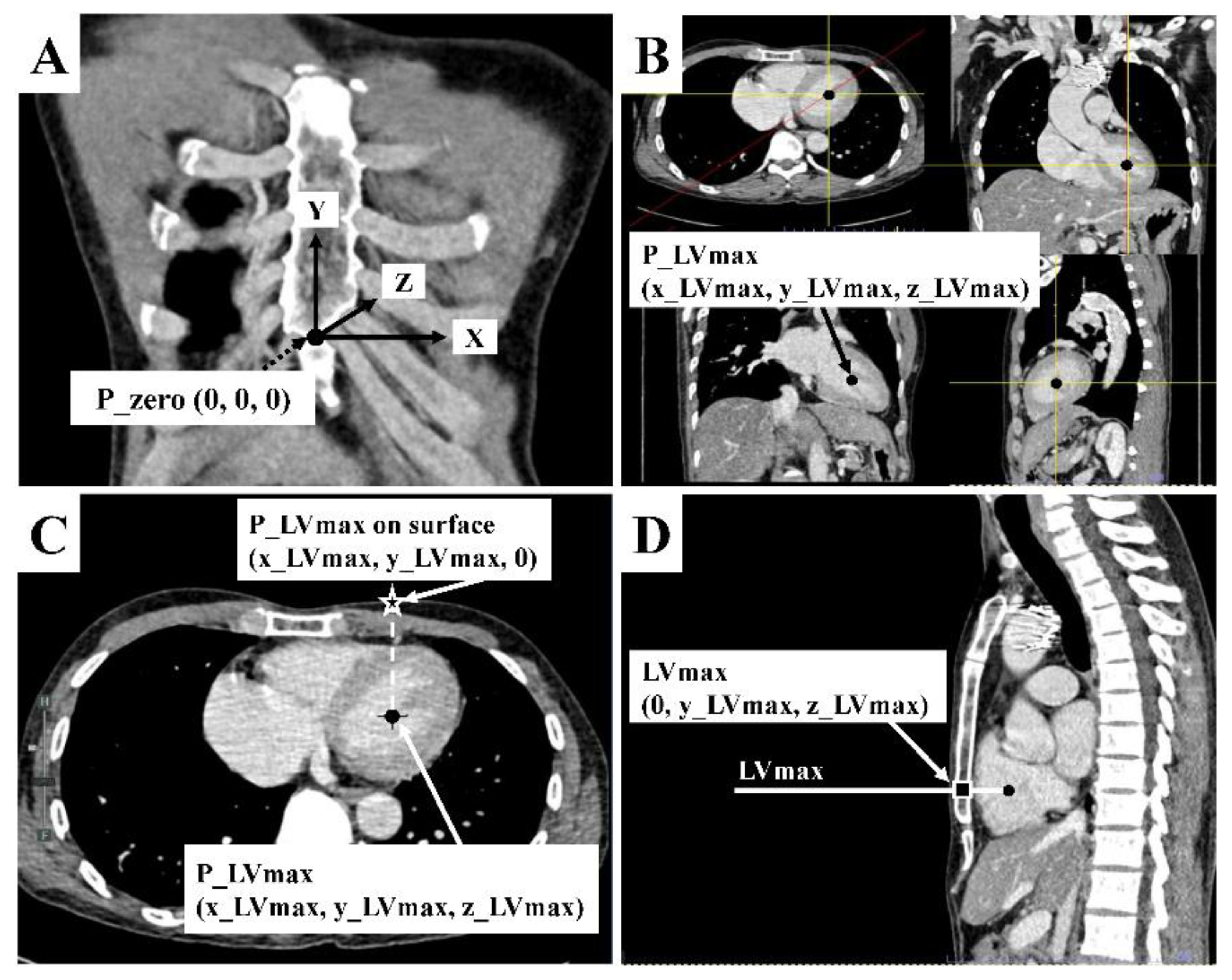
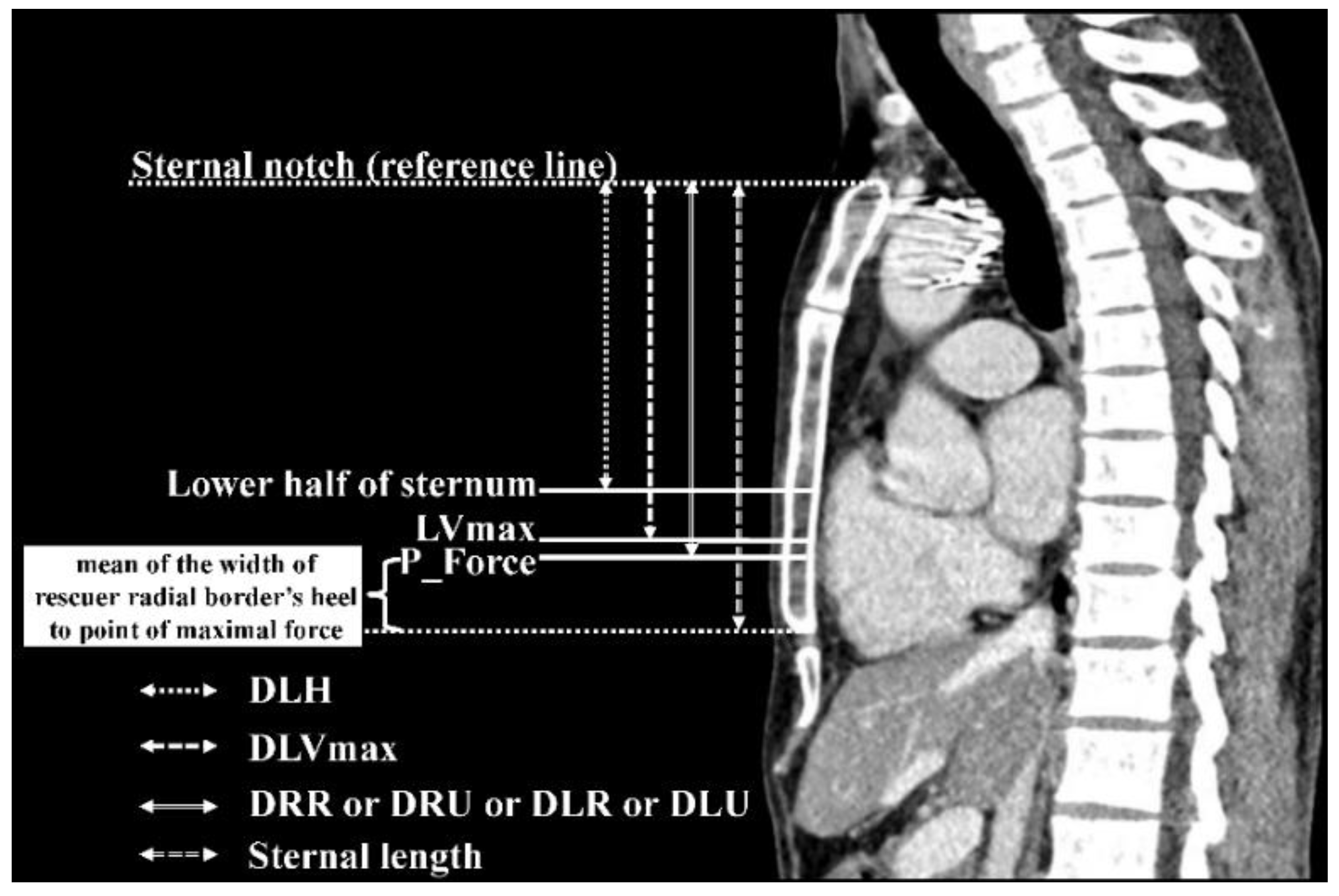
2.3.2. Patient’s CCT Measurement
2.4. Data Collection
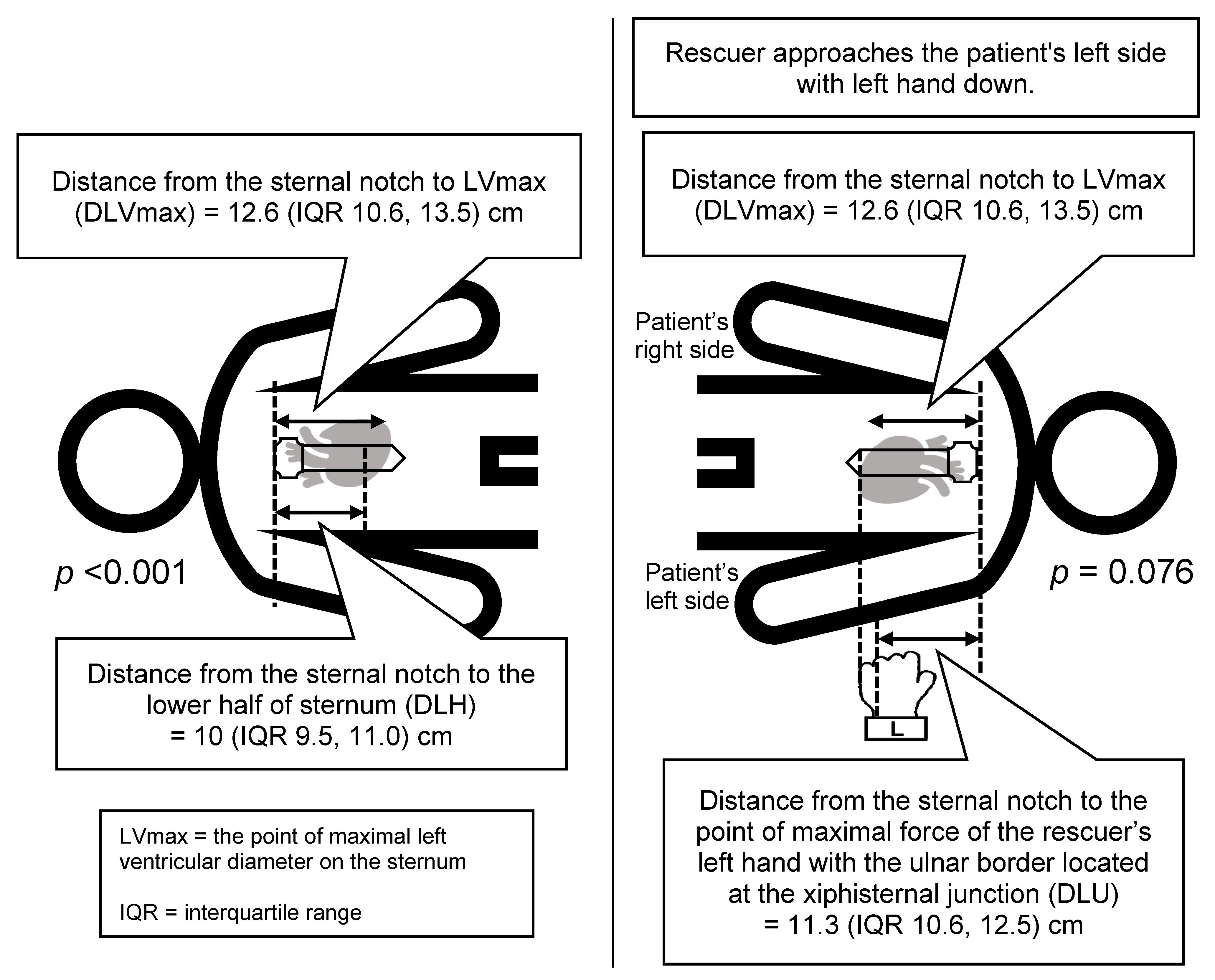
2.5. Outcome Measures
2.6. Sample Size Estimation
2.7. Data Analysis
3. Results
3.1. Characteristics of Participants
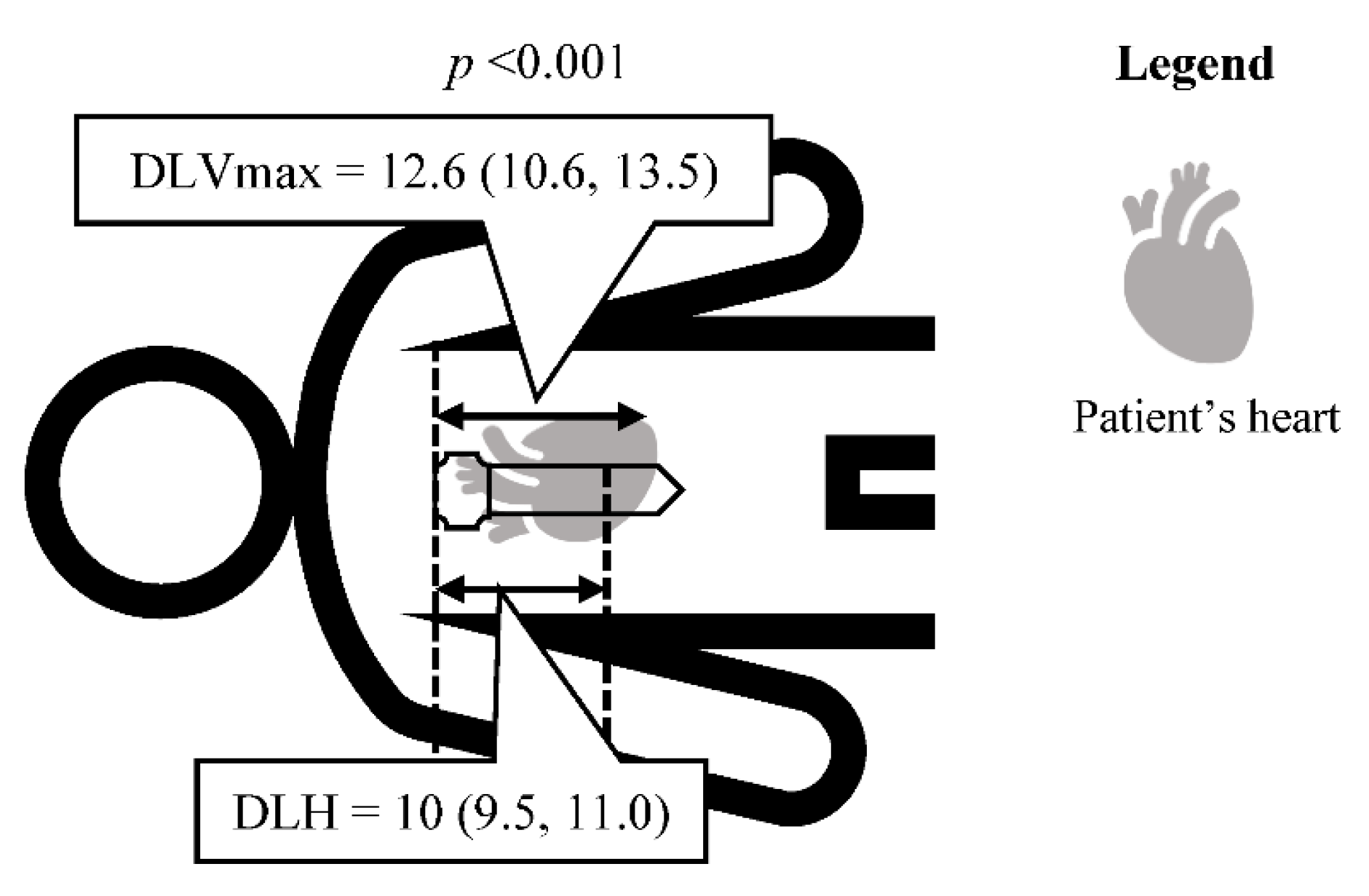
3.2. Primary Outcome
4. Discussion
5. Limitations
6. Conclusions
Presentation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Okubo, M.; Schmicker, R.H.; Wallace, D.J.; Idris, A.H.; Nichol, G.; Austin, M.A.; Grunau, B.; Wittwer, L.K.; Richmond, N.; Morrison, L.J.; et al. Variation in Survival After Out-of-Hospital Cardiac Arrest Between Emergency Medical Services Agencies. JAMA Cardiol. 2018, 3, 989–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navab, E.; Esmaeili, M.; Poorkhorshidi, N.; Salimi, R.; Khazaei, A.; Moghimbeigi, A. Predictors of Out of Hospital Cardiac Arrest Outcomes in Pre-Hospital Settings; a Retrospective Cross-Sectional Study. Arch. Acad Emerg. Med. 2019, 7, 36. [Google Scholar] [PubMed]
- Lurie, K.G.; Nemergut, E.C.; Yannopoulos, D.; Sweeney, M. The Physiology of Cardiopulmonary Resuscitation. Anesth. Analg. 2016, 122, 767–783. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.W.; Kudenchuk, P.J. Cardiopulmonary Resuscitation: The Science behind the Hands. Heart 2018, 104, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Ng, Q.X.; Han, M.X.; Lim, Y.L.; Arulanandam, S. A Systematic Review and Meta-Analysis of the Implementation of High-Performance Cardiopulmonary Resuscitation on Out-of-Hospital Cardiac Arrest Outcomes. J. Clin. Med. 2021, 10, 2098. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, J.C.; Salcido, D.D.; Menegazzi, J.J. Coronary Perfusion Pressure and Return of Spontaneous Circulation after Prolonged Cardiac Arrest. Prehosp. Emerg. Care 2010, 14, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, K.L.; Castaneda, M.G.; Boudreau, S.M.; Sharon, D.J.; Bebarta, V.S. Left Ventricular Compressions Improve Hemodynamics in a Swine Model of Out-of-Hospital Cardiac Arrest. Prehosp. Emerg. Care 2017, 21, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Rhee, J.E.; Kim, K. Is the Inter-Nipple Line the Correct Hand Position for Effective Chest Compression in Adult Cardiopulmonary Resuscitation? Resuscitation 2007, 75, 305–310. [Google Scholar] [CrossRef]
- Park, J.B.; Song, I.K.; Lee, J.H.; Kim, E.H.; Kim, H.S.; Kim, J.T. Optimal Chest Compression Position for Patients With a Single Ventricle During Cardiopulmonary Resuscitation. Pediatr. Crit. Care Med. 2016, 17, 303–306. [Google Scholar] [CrossRef]
- Hwang, K.; Chon, S.B.; Im, J.G. The Optimum Chest Compression Site with Regard to Heart Failure Demonstrated by Computed Tomography. Am. J. Emerg. Med. 2017, 35, 1899–1906. [Google Scholar] [CrossRef]
- Cha, K.C.; Kim, H.J.; Shin, H.J.; Kim, H.; Lee, K.H.; Hwang, S.O. Hemodynamic Effect of External Chest Compressions at the Lower End of the Sternum in Cardiac Arrest Patients. J. Emerg. Med. 2013, 44, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.O.; Zhao, P.G.; Choi, H.J.; Park, K.H.; Cha, K.C.; Park, S.M.; Kim, S.C.; Kim, H.; Lee, K.H. Compression of the Left Ventricular Outflow Tract during Cardiopulmonary Resuscitation. Acad Emerg. Med. 2009, 16, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Olasveengen, T.M.; Semeraro, F.; Ristagno, G.; Castren, M.; Handley, A.; Kuzovlev, A.; Monsieurs, K.G.; Raffay, V.; Smyth, M.; Soar, J.; et al. European Resuscitation Council Guidelines 2021: Basic Life Support. Resuscitation 2021, 161, 98–114. [Google Scholar] [CrossRef]
- Olasveengen, T.M.; Mancini, M.E.; Perkins, G.D.; Avis, S.; Brooks, S.; Castrén, M.; Chung, S.P.; Considine, J.; Couper, K.; Escalante, R.; et al. Adult Basic Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2020, 142, S41–S91. [Google Scholar] [CrossRef] [PubMed]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S366–S468. [Google Scholar] [CrossRef] [PubMed]
- Song, K.J.; Lee, S.Y.; Cho, G.C.; Kim, G.; Kim, J.Y.; Oh, J.; Oh, J.H.; Ryu, S.; Ryoo, S.M.; Lee, E.H.; et al. 2020 Korean Guidelines for Cardiopulmonary Resuscitation. Part 3. Adult Basic Life Support. Clin. Exp. Emerg. Med. 2021, 8, S15–S25. [Google Scholar] [CrossRef]
- Cha, K.C.; Kim, Y.J.; Shin, H.J.; Cha, Y.S.; Kim, H.; Lee, K.H.; Kwon, W.; Hwang, S.O. Optimal Position for External Chest Compression during Cardiopulmonary Resuscitation: An Analysis Based on Chest CT in Patients Resuscitated from Cardiac Arrest. Emerg. Med. J. 2013, 30, 615–619. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.; Oh, W.S.; Chon, S.B.; Kim, S.; Hwang, K. Theoretical Personalized Optimum Chest Compression Point Can Be Determined Using Posteroanterior Chest Radiography. Resuscitation 2018, 128, 97–105. [Google Scholar] [CrossRef]
- Jiang, L.; Min, J.; Yang, F.; Shao, X. The Optimal Chest Compression Point on Sternum Based on Chest-Computed Tomography: A Retrospective Study. Hong Kong J. Emerg. Med. 2020, 27, 197–201. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Chon, S.B.; Oh, W.S.; Cho, S. Determination of the Theoretical Personalized Optimum Chest Compression Point Using Anteroposterior Chest Radiography. Clin. Exp. Emerg. Med. 2019, 6, 303–313. [Google Scholar] [CrossRef]
- Al-Abed, Y.; Curtin, J.; Clark, A. Change in the Z-Axis Location of the Sternal Notch in an Arms-Raised vs Arms-down Position on CT Examinations. Br. J. Radiol. 2008, 81, 855–858. [Google Scholar] [CrossRef] [PubMed]
- Yue, B.; Ye, S.; Liu, F.; Huang, J.; Ji, Y.; Liu, D.; Chen, J. Bilateral Lung Transplantation for Patients With Destroyed Lung and Asymmetric Chest Deformity. Front. Surg. 2021, 8, 680207. [Google Scholar] [CrossRef]
- Rhee, C.K.; Yoo, K.H.; Lee, J.H.; Park, M.J.; Kim, W.J.; Park, Y.B.; Hwang, Y.I.; Kim, Y.S.; Jung, J.Y.; Moon, J.Y.; et al. Clinical Characteristics of Patients with Tuberculosis-Destroyed Lung. Int. J. Tuberc. Lung Dis. 2013, 17, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Ryu, Y.J.; Lee, J.H.; Chun, E.M.; Chang, J.H.; Shim, S.S. Clinical Outcomes and Prognostic Factors in Patients with Tuberculous Destroyed Lung. Int. J. Tuberc. Lung Dis. 2011, 15, 246–250. [Google Scholar] [PubMed]
- Choi, H.; Lee, C.C.; Kim, H.J.; Singer, A.J. Identifying the Optimal Hand Placement Site for Chest Compression by Measuring Hand Width and Sternal Length in Young Adults. Am. J. Emerg. Med. 2016, 34, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Oh, J.; Lim, T.H.; Kang, H.; Park, J.H.; Song, S.Y.; Shin, G.H.; Song, Y. Comparison of Optimal Point on the Sternum for Chest Compression between Obese and Normal Weight Individuals with Respect to Body Mass Index, Using Computer Tomography: A Retrospective Study. Resuscitation 2018, 128, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Qvigstad, E.; Kramer-Johansen, J.; Tømte, Ø.; Skålhegg, T.; Sørensen, Ø.; Sunde, K.; Olasveengen, T.M. Clinical Pilot Study of Different Hand Positions during Manual Chest Compressions Monitored with Capnography. Resuscitation 2013, 84, 1203–1207. [Google Scholar] [CrossRef]
- Kwon, H.; Kim, Y.; Kim, K.; Jung, J.Y.; Kim, J.; Choi, S.I.; Chun, E.J.; Bae, W.K. Where Is the Left Ventricle during Cardiopulmonary Resuscitation Based on Chest Computed Tomography in the Expiration with Arms down Position? PLoS ONE 2018, 13, e0193364. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall |
|---|---|
| Patient characteristics (n = 39) | |
| Age—year † | 67 (49, 78) |
| Male—n (%) | 22 (56.4) |
| Weight—kg * | 61.6 ± 14.8 |
| Height—cm * | 161.4 ± 8.5 |
| Body mass index (BMI)—kg/m2 † | 23.3 (19.7, 25) |
| Inspiratory hold—n (%) | 30 (76.9) |
| Co-morbidity—n (%) | |
| Hypertension | 22 (56.4) |
| Coronary artery disease | 10 (25.6) |
| Dyslipidemia | 10 (25.6) |
| Diabetes | 9 (23.1) |
| End-stage kidney disease | 9 (23.1) |
| Others | 24 (61.5) |
| None | 7 (18) |
| Rescuer’s hand measurement (n = 69) | |
| Age—year † | 26 (24, 31) |
| Male—n (%) | 37 (53.6) |
| Weight—kg † | 64 (56, 75) |
| Height—cm * | 167.3 ± 7.3 |
| Body mass index (BMI)—kg/m2 † | 22.3 (20, 26.2) |
| Career—n (%) | |
| Certified-BLS Lay rescuer | 18 (26.1) |
| Registered nurse | 16 (23.2) |
| Paramedic | 11 (15.9) |
| Medical student | 11 (15.9) |
| Physician | 6 (8.7) |
| Practical nurse | 4 (5.8) |
| Nurse aid | 2 (2.9) |
| Emergency nurse practitioner | 1 (1.5) |
| Right-hand as dominant hand—n (%) | 62 (90) |
| Preferred left hand underneath when performed chest compressions—n (%) | 41 (59.4) |
| Fingerbreadth width of dominant hand—cm * | |
| One FB (index finger) | 1.9 ± 0.3 |
| Two FB (index, middle fingers) | 3.6 ± 0.44 |
| Three FB (index, middle, ring fingers) | 5.4 ± 0.6 |
| Measurement (cm) | Overall (n = 39) | Inspiratory Hold (n = 30) | Expiratory Hold (n = 9) | Difference | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| DLVmax † | 12.6 (10.6, 13.5) | 12.4 (10.6, 13.4) | 12.7 (10.8, 15) | NA | NA | 0.527 |
| Sternal length * | 13.8 ± 1.6 | 13.7 ± 1.5 | 14.3 ± 2 | −0.6 | −2.2 to 1 | 0.441 |
| DLH † | 10 (9.5, 11) | 9.89 (9.5, 10.8) | 10.6 (10.2, 11.7) | NA | NA | 0.334 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Usawasuraiin, P.; Wittayachamnankul, B.; Chenthanakij, B.; Euathrongchit, J.; Phinyo, P.; Tangsuwanaruk, T. Optimal Landmark for Chest Compressions during Cardiopulmonary Resuscitation Derived from a Chest Computed Tomography in Arms-Down Position. J. Cardiovasc. Dev. Dis. 2022, 9, 100. https://doi.org/10.3390/jcdd9040100
Usawasuraiin P, Wittayachamnankul B, Chenthanakij B, Euathrongchit J, Phinyo P, Tangsuwanaruk T. Optimal Landmark for Chest Compressions during Cardiopulmonary Resuscitation Derived from a Chest Computed Tomography in Arms-Down Position. Journal of Cardiovascular Development and Disease. 2022; 9(4):100. https://doi.org/10.3390/jcdd9040100
Chicago/Turabian StyleUsawasuraiin, Pimpan, Borwon Wittayachamnankul, Boriboon Chenthanakij, Juntima Euathrongchit, Phichayut Phinyo, and Theerapon Tangsuwanaruk. 2022. "Optimal Landmark for Chest Compressions during Cardiopulmonary Resuscitation Derived from a Chest Computed Tomography in Arms-Down Position" Journal of Cardiovascular Development and Disease 9, no. 4: 100. https://doi.org/10.3390/jcdd9040100