
Safety and Efficacy of Tirofiban in Severe Ischemic Stroke Patients Undergoing Mechanical Thrombectomy
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Management of Tirofiban
2.3. Data Compilation
2.4. Assessment Criteria
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
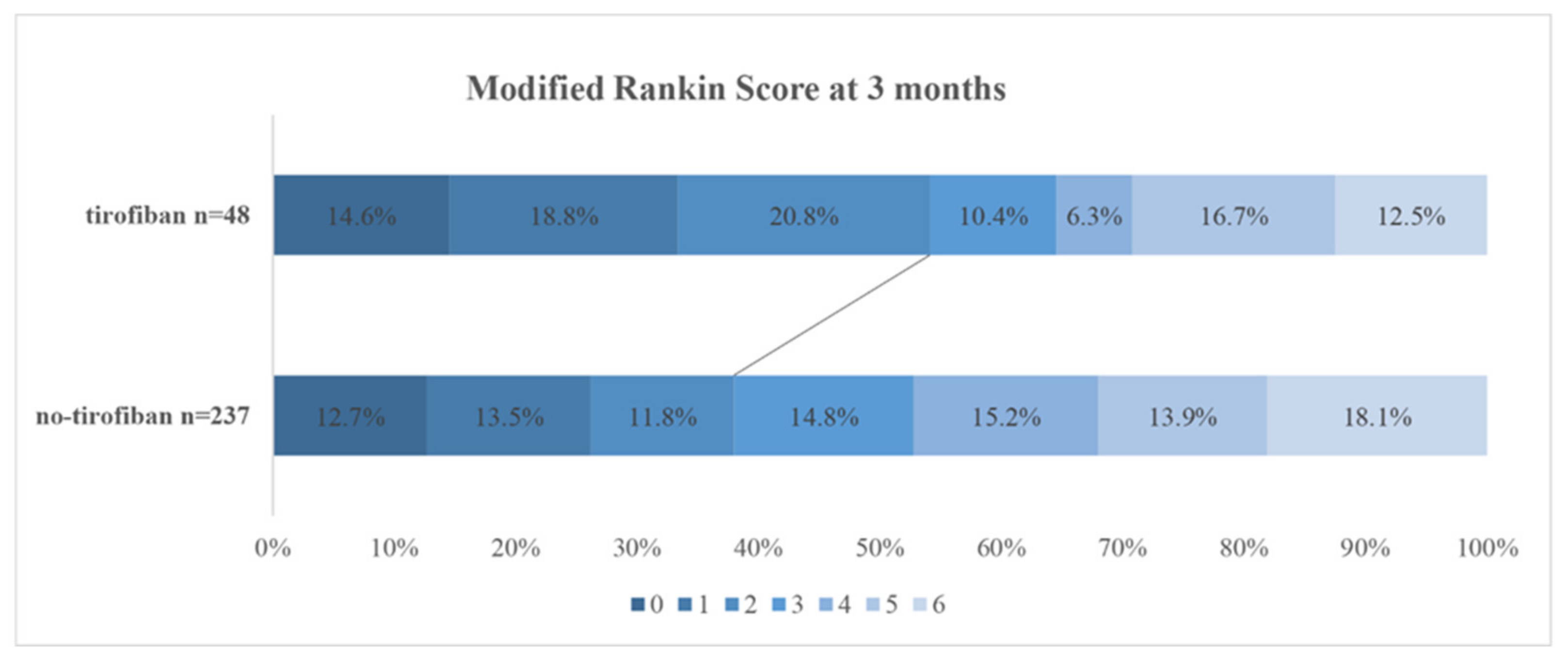
3.2. Favorable Functional Outcome
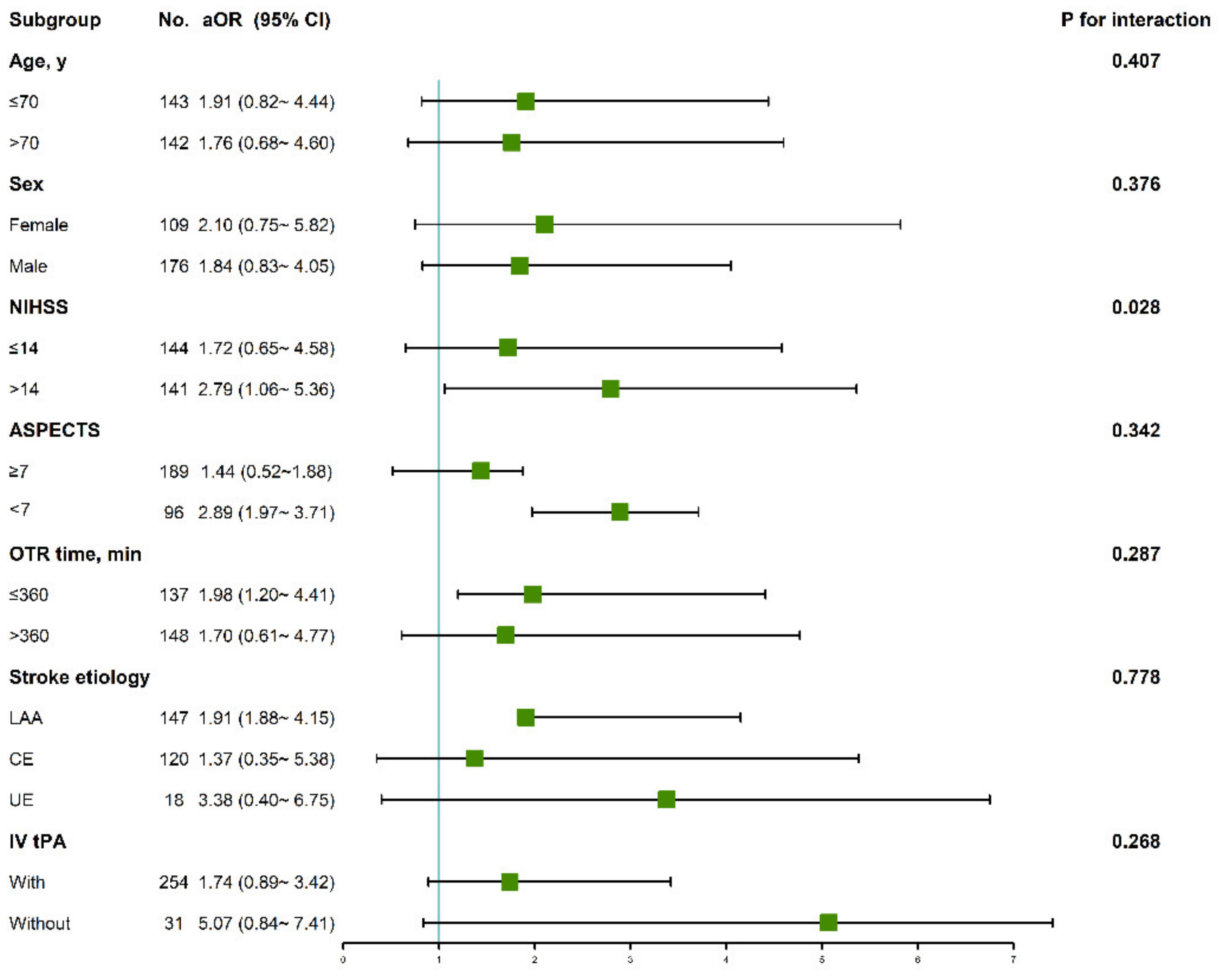
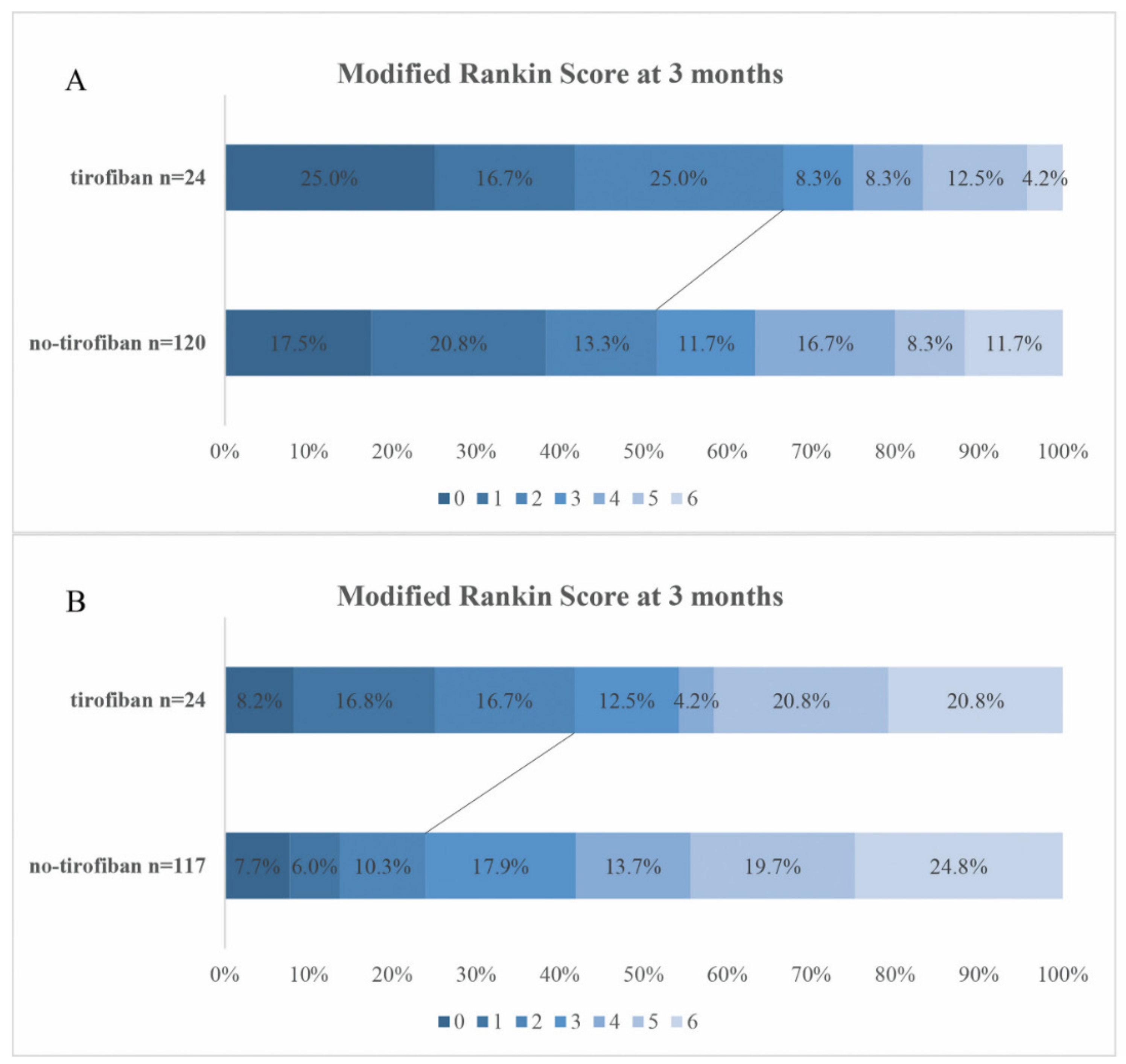
3.3. Subgroup Analysis
3.4. Safety Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Albers, G.W.; Marks, M.P.; Kemp, S.; Christensen, S.; Tsai, J.P.; Ortega-Gutierrez, S.; McTaggart, R.A.; Torbey, M.T.; Kim-Tenser, M.; Leslie-Mazwi, T.; et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N. Engl. J. Med. 2018, 378, 708–718. [Google Scholar] [CrossRef] [PubMed]
- Van Den Berg, L.A.; Dijkgraaf, M.G.W.; Berkhemer, O.A.; Fransen, P.S.S.; Beumer, D.; Lingsma, H.F.; Majoie, C.B.L.M.; Dippel, D.W.J.; Van Der Lugt, A.; Van Oostenbrugge, R.J.; et al. Two-Year Outcome after Endovascular Treatment for Acute Ischemic Stroke. N. Engl. J. Med. 2017, 376, 1341–1349. [Google Scholar] [CrossRef]
- Mosimann, P.J.; Kaesmacher, J.; Gautschi, D.; Bellwald, S.; Panos, L.; Piechowiak, E.; Dobrocky, T.; Zibold, F.; Mordasini, P.; El-Koussy, M.; et al. Predictors of Unexpected Early Re-occlusion After Successful Mechanical Thrombectomy in Acute Ischemic Stroke Patients. Stroke 2018, 49, 2643–2651. [Google Scholar] [CrossRef]
- Lee, J.S.; Hong, J.M.; Lee, K.S.; Suh, H.I.; Choi, J.W.; Kim, S.Y. Primary Stent Retrieval for Acute Intracranial Large Artery Occlusion Due to Atherosclerotic Disease. J. Stroke 2016, 18, 96–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, Y.H.; Kim, Y.W.; Kang, D.H.; Kim, Y.S.; Liebeskind, D.S. Impact of Target Arterial Residual Stenosis on Outcome After Endovascular Revascularization. Stroke 2016, 47, 1850–1857. [Google Scholar] [CrossRef] [Green Version]
- Pan, X.; Zheng, D.; Zheng, Y.; Chan, P.W.L.; Lin, Y.; Zou, J.; Zhou, J.; Yang, J. Safety and efficacy of tirofiban combined with endovascular treatment in acute ischaemic stroke. Eur. J. Neurol. 2019, 26, 1105–1110. [Google Scholar] [CrossRef]
- Yang, M.; Huo, X.; Gao, F.; Wang, A.; Ma, N.; Shi, H.; Chen, W.; Wang, S.; Wang, Y.; Miao, Z. Low-dose rescue tirofiban in mechanical thrombectomy for acute cerebral large-artery occlusion. Eur. J. Neurol. 2020, 27, 1056–1061. [Google Scholar] [CrossRef]
- Zhao, W.; Che, R.; Shang, S.; Wu, C.; Li, C.; Wu, L.; Chen, J.; Duan, J.; Song, H.; Zhang, H.; et al. Low-Dose Tirofiban Improves Functional Outcome in Acute Ischemic Stroke Patients Treated with Endovascular Thrombectomy. Stroke 2017, 48, 3289–3294. [Google Scholar] [CrossRef]
- Kellert, L.; Hametner, C.; Rohde, S.; Bendszus, M.; Hacke, W.; Ringleb, P.; Stampfl, S. Endovascular stroke therapy: Tirofiban is associated with risk of fatal intracerebral hemorrhage and poor outcome. Stroke 2013, 44, 1453–1455. [Google Scholar] [CrossRef] [Green Version]
- Larrue, V.; von Kummer, R.; Muller, A.; Bluhmki, E. Risk factors for severe hemorrhagic transformation in ischemic stroke patients treated with recombinant tissue plasminogen activator: A secondary analysis of the European-Australasian Acute Stroke Study (ECASS II). Stroke 2001, 32, 438–441. [Google Scholar] [CrossRef]
- Berkhemer, O.A.; Fransen, P.S.S.; Beumer, D.; Berg, L.A.V.D.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.H.; et al. A Randomized Trial of Intraarterial Treatment for Acute Ischemic Stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Campbell, B.C.; Hill, M.D.; Rubiera, M.; Menon, B.K.; Demchuk, A.; Donnan, G.A.; Roy, D.; Thornton, J.; Dorado, L.; Bonafe, A.; et al. Safety and Efficacy of Solitaire Stent Thrombectomy: Individual Patient Data Meta-Analysis of Randomized Trials. Stroke 2016, 47, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, X.; Liu, C.; Huang, S.; Liang, C.; Zhang, M. Effects of Oral Antiplatelet Agents and Tirofiban on Functional Outcomes of Patients with Non-Disabling Minor Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 104829. [Google Scholar] [CrossRef]
- Yang, M.; Huo, X.; Miao, Z.; Wang, Y. Platelet Glycoprotein IIb/IIIa Receptor Inhibitor Tirofiban in Acute Ischemic Stroke. Drugs 2019, 79, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Wu, Y.; Gao, X.; Bivard, A.; Levi, C.R.; Parsons, M.W.; Lin, L.; Spratt, N.; Esperon, C.G.; Miteff, F.; et al. Intraarterial Versus Intravenous Tirofiban as an Adjunct to Endovascular Thrombectomy for Acute Ischemic Stroke. Stroke 2020, 51, 2925–2933. [Google Scholar] [CrossRef] [PubMed]
- Aoki, J.; Suzuki, K.; Kanamaru, T.; Kutsuna, A.; Katano, T.; Takayama, Y.; Nishi, Y.; Takeshi, Y.; Nakagami, T.; Numao, S.; et al. Association between initial NIHSS score and recanalization rate after endovascular thrombectomy. J. Neurol. Sci. 2019, 403, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Derex, L.; Nighoghossian, N.; Hermier, M.; Adeleine, P.; Froment, J.; Trouillas, P. Early Detection of Cerebral Arterial Occlusion on Magnetic Resonance Angiography: Predictive Value of the Baseline NIHSS Score and Impact on Neurological Outcome. Cerebrovasc. Dis. 2002, 13, 225–229. [Google Scholar] [CrossRef]
- Marks, M.P.; Lansberg, M.; Mlynash, M.; Olivot, J.-M.; Straka, M.; Kemp, S.; McTaggart, R.; Inoue, M.; Zaharchuk, G.; Bammer, R.; et al. Effect of collateral blood flow on patients undergoing endovascular therapy for acute ischemic stroke. Stroke 2014, 45, 1035–1039. [Google Scholar] [CrossRef] [Green Version]
- Bang, O.Y.; Saver, J.; Kim, S.J.; Kim, G.-M.; Chung, C.-S.; Ovbiagele, B.; Lee, K.H.; Liebeskind, D.S. Collateral Flow Predicts Response to Endovascular Therapy for Acute Ischemic Stroke. Stroke 2011, 42, 693–699. [Google Scholar] [CrossRef] [Green Version]
- Fischer, U.; Arnold, M.; Nedeltchev, K.; Brekenfeld, C.; Ballinari, P.; Remonda, L.; Schroth, G.; Mattle, H.P. NIHSS Score and Arteriographic Findings in Acute Ischemic Stroke. Stroke 2005, 36, 2121–2125. [Google Scholar] [CrossRef]
- Sims, J.R.; Rordorf, G.; Smith, E.E.; Koroshetz, W.J.; Lev, M.H.; Buonanno, F.; Schwamm, L.H. Arterial occlusion revealed by CT angi-ography predicts NIH stroke score and acute outcomes after IV tPA treatment. AJNR Am. J. Neuroradiol. 2005, 26, 246–251. [Google Scholar]
- Maas, M.B.; Furie, K.L.; Lev, M.H.; Ay, H.; Singhal, A.B.; Greer, D.; Harris, G.J.; Halpern, E.; Koroshetz, W.J.; Smith, W.S. National Institutes of Health Stroke Scale Score Is Poorly Predictive of Proximal Occlusion in Acute Cerebral Ischemia. Stroke 2009, 40, 2988–2993. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.-H.; Yoon, W.; Kim, S.K.; Baek, B.H.; Lee, Y.Y.; Kim, Y.-W.; Hwang, Y.-H.; Kim, J.-T.; Park, M.S. Endovascular treatment for emergent large vessel occlusion due to severe intracranial atherosclerotic stenosis. J. Neurosurg. 2019, 130, 1949–1956. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.-J.; Xiong, W. Tirofiban combined with rt-PA intraarterial thrombolysis improves the recanalization rate of acute middle cerebral artery occlusion in rabbits. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 2888–2895. [Google Scholar]
- Sun, C.; Li, X.; Zhao, Z.; Chen, X.; Huang, C.; Li, X.; Shan, Y.; Zou, Y.; Liu, Y.; Ibrahim, M.; et al. Safety and Efficacy of Tirofiban Combined with Mechanical Thrombectomy Depend on Ischemic Stroke Etiology. Front. Neurol. 2019, 10, 1100. [Google Scholar] [CrossRef]
- Saver, J.L.; Goyal, M.; Van Der Lugt, A.; Menon, B.K.; Majoie, C.B.L.M.; Dippel, D.W.; Campbell, B.C.; Nogueira, R.G.; Demchuk, A.M.; Tomasello, A.; et al. Time to Treatment with Endovascular Thrombectomy and Outcomes From Ischemic Stroke: A Meta-analysis. JAMA 2016, 316, 1279–1289. [Google Scholar] [CrossRef] [PubMed]
- Bhan, C.; Koehler, T.J.; Elisevich, L.; Singer, J.; Mazaris, P.; James, E.; Zachariah, J.; Combs, J.; Dejesus, M.; Tubergen, T.; et al. Mechanical Thrombectomy for Acute Stroke: Early versus Late Time Window Outcomes. J. Neuroimaging 2020, 30, 315–320. [Google Scholar] [CrossRef]
- Zhao, H.; Feng, Y.; Rong, X.; Mao, Y.; Wang, Z.; Ling, Y.; Dong, Q.; Cao, W. Sequential tirofiban infusions combined with endovascular treatment may improve outcomes in acute ischemic stroke—A meta-analysis. Aging 2021, 13, 5426–5441. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No Tirofiban N = 237 | Tirofiban N = 48 | Overall N = 285 | p Value | |
|---|---|---|---|---|
| Age, y | 71 (64, 79) | 69 (58, 76) | 71 (63, 78) | 0.165 |
| Female, n (%) | 146 (61.6) | 30 (62.5) | 176 (61.7) | 0.907 |
| Stroke etiology, n (%) | 0.002 | |||
| LAA | 113 (47.6) | 34 (70.8) | 147 (51.5) | |
| CE | 111 (46.8) | 9 (18.7) | 120 (42.1) | |
| UE | 13 (5.5) | 5 (10.4) | 18 (6.3) | |
| NIHSS, median (IQR) | 14 (11, 18) | 14 (10, 17) | 14 (11,18) | 0.173 |
| ASPECTS, median (IQR) | 8 (7–9) | 8 (7–9) | 8 (7–9) | 0.788 |
| Systolic BP, mmHg | 142.5 ± 17.7 | 147.4 ± 21.4 | 143.4 ± 18.5 | 0.091 |
| Glucose, mmol/L | 8.6 ± 23.1 | 6.9 ± 1.6 | 8.3 ± 21.0 | 0.605 |
| Medical History | ||||
| Atrial fibrillation, n (%) | 147 (62.0) | 14 (29.1) | 161 (56.4) | 0.000 * |
| Hyperlipidemia, n (%) | 5 (2.1) | 1 (2.0) | 6 (2.11) | 0.991 |
| Hypertension, n (%) | 154 (64.9) | 29 (60.4) | 183 (64.2) | 0.548 |
| Diabetes mellitus, n (%) | 38 (16.0) | 6 (12.5) | 44 (15.4) | 0.537 |
| Previous stroke, n (%) | 39 (16.4) | 7 (14.5) | 46 (16.1) | 0.748 |
| Pre-antiplatelet, n (%) | 34 (14.3) | 7 (14.5) | 41 (14.3) | 0.966 |
| Pre-anticoagulation, n (%) | 23 (9.70) | 1 (2.0) | 24 (8.4) | 0.083 |
| Smoker, n (%) | 36 (15.1) | 9 (18.7) | 45 (15.7) | 0.537 |
| Procedural Variables | ||||
| t-PA, n (%) | 209 (88.2) | 45 (93.7) | 254 (89.1) | 0.351 |
| OTP time, min | 305 (190, 365) | 350 (245, 420) | 310 (215, 390) | 0.034 * |
| OTR time, min | 360 (285, 450) | 455 (355, 532) | 375 (290, 460) | 0.001 * |
| TICI 2b-3, n (%) | 219 (92.4) | 43 (89.5) | 262 (91.9) | 0.513 |
| Retrieval times ≥ 3, n (%) | 8 (3.4) | 5 (10.4) | 13 (4.6) | 0.045 * |
| Rescue therapy#, n (%) | 27 (11.4) | 11 (22.9) | 38 (13.3) | 0.024 * |
| Clinical Outcome | ||||
| Favorable outcome, n (%) | 90 (37.9) | 26 (54.1) | 116 (40.7) | 0.037 * |
| sICH, n (%) | 49 (20.7) | 10 (20.8) | 59 (20.7) | 0.980 |
| ICH, n (%) | 97 (40.9) | 20 (41.6) | 117 (41.0) | 0.924 |
| Mortality at 3 m, n (%) | 43 (18.1) | 6 (12.5) | 49 (17.1) | 0.345 |
| OR (95% CI) | p Value | aOR # (95% CI) | p Value | |
|---|---|---|---|---|
| Age | 0.958 (0.938~0.979) | 0.000 * | 0.953 (0.930~0.977) | 0.000 * |
| Stroke etiology | 0.665 (0.352~1.167) | 0.424 | 0.875 (0.662~1.158) | 0.353 |
| NIHSS | 0.873 (0.828~0.921) | 0.000 * | 0.877 (0.829~0.928) | 0.000 * |
| ASPECTS | 0.842 (0.723~0.839) | 0.024 * | 0.738 (0.796~0.916) | 0.039 * |
| Use of tirofiban | 1.930 (1.033~3.608) | 0.039 * | 2.033 (1.002~4.123) | 0.043 * |
| OTP time | 0.999 (0.998~1.002) | 0.892 | 0.993 (0.829~0.928) | 0.205 |
| OTR time | 0.993 (0.938~0.979) | 0.032 * | 0.993 (0.982~0.993) | 0.043 * |
| TICI 2b-3 | 4.539 (1.938~3.979) | 0.027 * | 3.167 (0.997~1.001) | 0.056 |
| NIHSS ≤ 14 (n = 141) | NIHSS > 14 (n = 144) | |||
|---|---|---|---|---|
| aOR (95% CI) | p Value | aOR (95% CI) | p Value | |
| ICH | 1.047 (0.396~2.770) | 0.926 | 1.812 (0.311~2.117) | 0.670 |
| sICH | 1.779 (0.530~1.980) | 0.717 | 1.024 (0.396~2.770) | 0.944 |
| Death | 0.530 (0.060~4.499) | 0.553 | 0.732 (0.495~1.055) | 0.092 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, L.; Wang, T.; Chen, A.; Ling, C.; Xu, J.; Qian, C.; Chen, G. Safety and Efficacy of Tirofiban in Severe Ischemic Stroke Patients Undergoing Mechanical Thrombectomy. J. Cardiovasc. Dev. Dis. 2022, 9, 408. https://doi.org/10.3390/jcdd9110408
Cai L, Wang T, Chen A, Ling C, Xu J, Qian C, Chen G. Safety and Efficacy of Tirofiban in Severe Ischemic Stroke Patients Undergoing Mechanical Thrombectomy. Journal of Cardiovascular Development and Disease. 2022; 9(11):408. https://doi.org/10.3390/jcdd9110408
Chicago/Turabian StyleCai, Lingxin, Tingting Wang, Aiqing Chen, Chenhan Ling, Jing Xu, Cong Qian, and Gao Chen. 2022. "Safety and Efficacy of Tirofiban in Severe Ischemic Stroke Patients Undergoing Mechanical Thrombectomy" Journal of Cardiovascular Development and Disease 9, no. 11: 408. https://doi.org/10.3390/jcdd9110408