
Pre-Stroke Statin Use Is Associated with Mild Neurological Deficits at the Onset of Acute Ischemic Stroke

Abstract
:1. Introduction
2. Materials and Methods
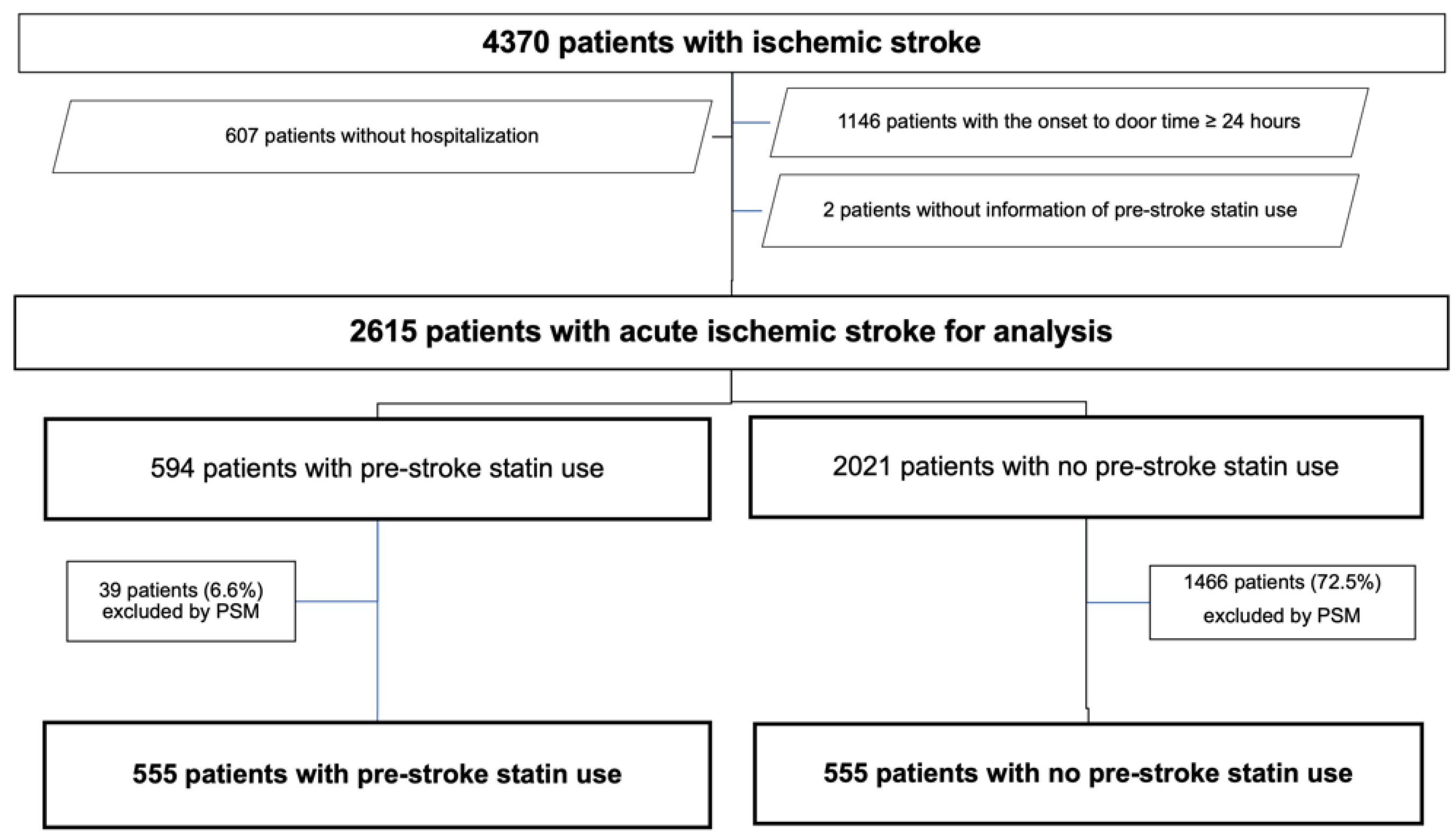
2.1. Patients
2.2. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baigent, C.; Blackwell, L.; Emberson, J.; Holland, L.E.; Reith, C.; Bhala, N.; Peto, R.; Barnes, R.H.; Keech, A.; Simes, J.; et al. Efficacy and safety of more intensive lowering of ldl cholesterol: A meta-analysis of data from 170 000 participants in 26 randomised trials. Lancet 2010, 376, 1670–1681. [Google Scholar] [PubMed] [Green Version]
- Saku, K.; Zhang, B.; Noda, K.; PATROL Trial Investigators. Randomized head-to-head comparison of pitavastatin, atorvastatin, and rosuvastatin for safety and efficacy (quantity and quality of ldl): The patrol trial. Circ. J. 2011, 75, 1493–1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikewaki, K.; Ayaori, M. Strong statins as the major players for dyslipidemia in high-risk patients: Are they all the same or not? Circ. J. 2011, 75, 1326–1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taqueti, V.R.; Ridker, P.M. Lipid-lowering and anti-inflammatory benefits of statin therapy: More than meets the plaque. Circ. Cardiovasc. Imaging 2017, 10, e006676. [Google Scholar] [CrossRef] [Green Version]
- Endres, M.; Laufs, U.; Huang, Z.; Nakamura, T.; Huang, P.; Moskowitz, M.A.; Liao, J.K. Stroke protection by 3-hydroxy-3-methylglutaryl (HMG)-CoA reductase inhibitors mediated by endothelial nitric oxide synthase. Proc. Natl. Acad. Sci. USA 1998, 95, 8880–8885. [Google Scholar] [CrossRef] [Green Version]
- Sato, S.; Toyoda, K.; Uehara, T.; Toratani, N.; Yokota, C.; Moriwaki, H.; Naritomi, H.; Minematsu, K. Baseline nih stroke scale score predicting outcome in anterior and posterior circulation strokes. Neurology 2008, 70, 2371–2377. [Google Scholar] [CrossRef]
- Fischer, U.; Baumgartner, A.; Arnold, M.; Nedeltchev, K.; Gralla, J.; De Marchis, G.M.; Kappeler, L.; Mono, M.L.; Brekenfeld, C.; Schroth, G.; et al. What is a minor stroke? Stroke 2010, 41, 661–666. [Google Scholar] [CrossRef] [Green Version]
- Reeves, M.; Khoury, J.; Alwell, K.; Moomaw, C.; Flaherty, M.; Woo, D.; Khatri, P.; Adeoye, O.; Ferioli, S.; Kissela, B.; et al. Distribution of National Institutes of Health stroke scale in the Cincinnati/northern Kentucky stroke study. Stroke 2013, 44, 3211–3213. [Google Scholar] [CrossRef] [Green Version]
- Dutrieux, R.D.; van Eijk, M.; van Mierlo, M.L.; van Heugten, C.M.; Visser-Meily, J.M.; Achterberg, W.P. Discharge home after acute stroke: Differences between older and younger patients. J. Rehabil. Med. 2016, 48, 14–18. [Google Scholar] [CrossRef] [Green Version]
- Yaghi, S.; Willey, J.Z.; Andrews, H.; Boehme, A.K.; Marshall, R.S.; Boden-Albala, B. The itemized nihss scores are associated with discharge disposition in patients with minor stroke. Neurohospitalist 2016, 6, 102–106. [Google Scholar] [CrossRef]
- Laufs, U.; Gertz, K.; Huang, P.; Nickenig, G.; Böhm, M.; Dirnagl, U.; Endres, M. Atorvastatin upregulates type III nitric oxide synthase in thrombocytes, decreases platelet activation, and protects from cerebral ischemia in normocholesterolemic mice. Stroke 2000, 31, 2442–2449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martí-Fàbregas, J.; Gomis, M.; Arboix, A.; Aleu, A.; Pagonabarraga, J.; Belvís, R.; Cocho, D.; Roquer, J.; Rodríguez, A.; García, M.D.; et al. Favorable outcome of ischemic stroke in patients pretreated with statins. Stroke 2004, 35, 1117–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elkind, M.S.; Flint, A.C.; Sciacca, R.R.; Sacco, R.L. Lipid-lowering agent use at ischemic stroke onset is associated with decreased mortality. Neurology 2005, 65, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Sacco, S.; Toni, D.; Bignamini, A.A.; Zaninelli, A.; Gensini, G.F.; Carolei, A.; SIRIO Study Group. Effect of prior medical treatments on ischemic stroke severity and outcome. Funct. Neurol. 2011, 26, 133–139. [Google Scholar]
- Wankowicz, P.; Staszewski, J.; Debiec, A.; Nowakowska-Kotas, M.; Szylinska, A.; Turon-Skrzypinska, A.; Rotter, I. Pre-St Therapy improves in-hospital prognosis following acute ischemic stroke associated with well-controlled nonvalvular atrial fibrillation. J. Clin. Med. 2021, 10, 3036. [Google Scholar] [CrossRef]
- Eun, M.Y.; Jung, J.M.; Choi, K.H.; Seo, W.K. Statin effects in atrial fibrillation-related stroke: A systematic review and meta-analysis. Front. Neurol. 2020, 11, 589684. [Google Scholar] [CrossRef]
- Martínez-Sánchez, P.; Fuentes, B.; Martínez-Martínez, M.; Ruiz-Ares, G.; Fernández-Travieso, J.; Sanz-Cuesta, B.E.; Cuéllar-Gamboa, L.; Díaz-Domínguez, E.; Díez-Tejedor, E. Treatment with statins and ischemic stroke severity: Does the dose matter? Neurology 2013, 80, 1800–1805. [Google Scholar] [CrossRef]
- Choi, J.C.; Lee, J.S.; Park, T.H.; Cho, Y.J.; Park, J.M.; Kang, K.; Lee, K.B.; Lee, S.J.; Ko, Y.; Lee, J.; et al. Effect of pre-stroke statin use on stroke severity and early functional recovery: A retrospective cohort study. BMC Neurol. 2015, 15, 120. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, H.; Wakisaka, Y.; Matsuo, R.; Makihara, N.; Hata, J.; Kuroda, J.; Ago, T.; Kitayama, J.; Nakane, H.; Kamouchi, M.; et al. Influence of statin pretreatment on initial neurological severity and short-term functional outcome in acute ischemic stroke patients: The fukuoka stroke registry. Cerebrovasc. Dis. 2016, 42, 395–403. [Google Scholar] [CrossRef]
- Kinoshita, M.; Yokote, K.; Arai, H.; Iida, M.; Ishigaki, Y.; Ishibashi, S.; Umemoto, S.; Egusa, G.; Ohmura, H.; Okamura, T.; et al. Japan Atherosclerosis Society (JAS) guidelines for prevention of atherosclerotic cardiovascular diseases 2017. J. Atheroscler. Thromb. 2018, 25, 846–984. [Google Scholar] [CrossRef] [Green Version]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 acc/aha guideline on the primary prevention of cardiovascular disease: A report of the american college of cardiology/american heart association task force on clinical practice guidelines. J. Am. Coll. Cardiol. 2019, 74, e177–e232. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 aha/acc/aacvpr/aapa/abc/acpm/ada/ags/apha/aspc/nla/pcna guideline on the management of blood cholesterol: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [PubMed]
- Laurencin, C.; Philippeau, F.; Blanc-Lasserre, K.; Vallet, A.E.; Cakmak, S.; Mechtouff, L.; Cho, T.H.; Ritzenthaler, T.; Flocard, E.; Bischoff, M.; et al. Thrombolysis for acute minor stroke: Outcome and barriers to management. Results from the resuval stroke network. Cerebrovasc. Dis. 2015, 40, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Khatri, P.; Conaway, M.R.; Johnston, K.C. Acute Stroke Accurate Prediction Study (ASAP) Investigators. Ninety-day outcome rates of a prospective cohort of consecutive patients with mild ischemic stroke. Stroke 2012, 43, 560–562. [Google Scholar] [CrossRef]
- Dargazanli, C.; Arquizan, C.; Gory, B.; Consoli, A.; Labreuche, J.; Redjem, H.; Eker, O.; Decroix, J.P.; Corlobé, A.; Mourand, I.; et al. Mechanical thrombectomy for minor and mild stroke patients harboring large vessel occlusion in the anterior circulation: A multicenter cohort study. Stroke 2017, 48, 3274–3281. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. Constructing a control group using multivariate matched sampling methods that incorporate the propensity score. Am. Stat. 1985, 39, 33–38. [Google Scholar]
- Austin, P.C. Statistical criteria for selecting the optimal number of untreated subjects matched to each treated subject when using many-to-one matching on the propensity score. Am. J. Epidemiol. 2010, 172, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 2011, 10, 150–161. [Google Scholar] [CrossRef] [Green Version]
- Yang, D.; Dalton, J.E. A Unified Approach to Measuring the Effect Size between Two Groups Using SAS. 2012. Available online: https://www.semanticscholar.org/paper/A-unified-approach-to-measuring-the-effect-size-two-Yang-Dalton/6cf4bd36ca4c90006a5d6563f646a391c255581b (accessed on 23 June 2022).
- Fagerland, M.W.; Lydersen, S.; Laake, P. The McNemar test for binary matched-pairs data: Mid-p and asymptotic are better than exact conditional. BMC Med. Res. Methodol. 2013, 13, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, R.; Dana, T.; Blazina, I.; Daeges, M.; Bougatsos, C.; Grusing, S.; Jeanne, T.L. Statin Use for the Prevention of Cardiovascular Disease in Adults: A Systematic Review for the U.S. Preventive Services Task Force; (Evidence Syntheses, Number. 139) [Interventions/Treatment]; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2016; p. 4. Available online: https://www.ncbi.nlm.nih.gov/books/NBK396415/pdf/Bookshelf_NBK396415.pdf (accessed on 23 June 2022).
- Taguchi, I.; Iimuro, S.; Iwata, H.; Takashima, H.; Abe, M.; Amiya, E.; Ogawa, T.; Ozaki, Y.; Sakuma, I.; Nakagawa, Y.; et al. High-dose versus low-dose pitavastatin in Japanese patients with stable coronary artery disease (real-cad): A randomized superiority trial. Circulation 2018, 137, 1997–2009. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, T. Extending the “lower is better” principle to Japanese and possibly other Asian populations. Circulation 2018, 137, 2010–2012. [Google Scholar] [CrossRef]
- Ovbiagele, B.; Saver, J.L.; Starkman, S.; Kim, D.; Ali, L.K.; Jahan, R.; Duckwiler, G.R.; Viñuela, F.; Pineda, S.; Liebeskind, D.S. Statin enhancement of collateralization in acute stroke. Neurology 2007, 68, 2129–2131. [Google Scholar] [CrossRef]
- Toyoda, K.; Yoshimura, S.; Nakai, M.; Koga, M.; Sasahara, Y.; Sonoda, K.; Kamiyama, K.; Yazawa, Y.; Kawada, S.; Sasaki, M.; et al. Twenty-Year Change in Severity and Outcome of Ischemic and Hemorrhagic Strokes. JAMA Neurol. 2022, 79, 61–69. [Google Scholar] [CrossRef]
- Hong, K.S.; Lee, J.S. Statins in acute ischemic stroke: A systematic review. J. Stroke 2015, 17, 282–301. [Google Scholar] [CrossRef]
- Tramacere, I.; Boncoraglio, G.B.; Banzi, R.; Del Giovane, C.; Kwag, K.H.; Squizzato, A.; Moja, L. Comparison of statins for secondary prevention in patients with ischemic stroke or transient ischemic attack: A systematic review and network meta-analysis. BMC Med. 2019, 17, 67. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, S.; Uchida, K.; Daimon, T.; Takashima, R.; Kimura, K.; Morimoto, T.; ASSORT Trial Investigator. Randomized controlled trial of early versus delayed statin therapy in patients with acute ischemic stroke: Assort trial (administration of statin on acute ischemic stroke patient). Stroke 2017, 48, 3057–3063. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Before PSM | After PSM | |
|---|---|---|
| Variables | n = 2615 | n = 1110 |
| Age, years | 78 (70–85) | 79 (72–85) |
| Age ≥ 75 years, n (%) | 1630 (62.3%) | 748 (67.4%) |
| Male sex, n (%) | 1463 (55.9%) | 633 (57.0%) |
| Pre-stroke mRS | 0 (0–2) | 0 (0–3) |
| Pre-stroke statin use, n (%) | 594 (22.7%) | 555 (50.0%) |
| Hx of anti-HT drugs, n (%) | 1441 (55.1%) | 818 (73.7%) |
| Hx of diabetes drugs, n (%) | 411 (15.7%) | 295 (26.6%) |
| Hx of antiplatelets drugs, n (%) | 666 (25.4%) | 470 (42.3%) |
| Hx of anticoagulants drugs, n (%) | 322 (12.3%) | 166 (15.0%) |
| Hx of hp-EPA drugs, n (%) | 72 (2.8%) | 48 (4.3%) |
| Albumin adm, g/L | 40 (37–43) | 40 (37–43) |
| Creatinine adm, μmol/L | 74.3 (61.0–92.8) | 76.9 (62.8–96.4) |
| Glucose adm, mmol/L | 6.72 (5.77–8.33) | 6.83 (5.82–8.62) |
| HbA1c adm, % (NGSP) | 5.8 (5.5–6.3) | 6.0 (5.6–6.6) |
| CRP adm, μg/L | 1200 (500–3800) | 1200 (500–3600) |
| HDL-C adm, mmol/L | 1.42 (1.17–1.73) | 1.41 (1.14–1.72) |
| TG adm, mmol/L | 1.10 (0.78–1.64) | 1.13 (0.81–1.65) |
| TCHO adm, mmol/L | 5.07 (4.34–5.79) | 4.81 (4.19–5.53) |
| LDL-C adm, mmol/L | 2.93 (2.38–3.58) | 2.73 (2.22–3.36) |
| SVO, n (%) | 429 (16.4%) | 159 (14.3%) |
| LAA, n (%) | 684 (26.2%) | 333 (30.0%) |
| Cardioembolism, n (%) | 857 (32.8%) | 366 (33.0%) |
| ODE or UE, n (%) | 645 (24.7%) | 252 (22.7%) |
| NIHSS score adm | 4 (1–11) | 4 (1–10) |
| NIHSS score adm ≤ 3, n (%) | 1203 (46.0%) | 538 (48.4%) |
| Hospitalization, days | 8 (7–9) | 8 (7–9) |
| Discharge to home, n (%) | 1240 (47.4%) | 542 (48.8%) |
| After PSM | ||||
|---|---|---|---|---|
| Variable | Statin Use | No Statin Use | p-Value | StD |
| n = 555 | n = 555 | |||
| Age, years | 78 (72–84) | 80 (71–86) | 0.0774 | 0.0233 |
| Male sex, n (%) | 316 (56.9%) | 317 (57.2%) | 0.9517 | 0.0036 |
| Pre-stroke mRS | 0 (0–2) | 0 (0–3) | 0.1656 | 0.0074 |
| Hx of anti-HT drugs, n (%) | 408 (73.5%) | 410 (73.9%) | 0.8916 | 0.0082 |
| Hx of diabetes drugs, n (%) | 150 (27.0%) | 145 (26.1%) | 0.7341 | 0.0204 |
| Hx of antiplatelets drugs, n (%) | 234 (42.2%) | 236 (42.5%) | 0.9033 | 0.0073 |
| Hx of anticoagulants drugs, n (%) | 85 (15.3%) | 81 (14.6%) | 0.7364 | 0.0205 |
| Hx of hp-EPA drugs, n (%) | 25 (4.5%) | 23 (4.1%) | 0.7679 | 0.0177 |
| Albumin adm, g/L | 40 (37–43) | 40 (37–43) | 0.3403 | 0.0626 |
| Creatinine adm, μmol/L | 77.8 (63.6–95.5) | 76.0 (61.0–97.2) | 0.1113 | 0.0323 |
| Glucose adm, mmol/L | 6.94 (5.83–8.77) | 6.77 (5.83–8.54) | 0.4978 | 0.0269 |
| HbA1c adm, % (NGSP) | 6.0 (5.7–6.6) | 5.9 (5.6–6.6) | 0.0972 | 0.0016 |
| CRP adm, μg/L | 1100 (400–3600) | 1300 (500–3700) | 0.1142 | 0.0454 |
| After PSM | ||||
|---|---|---|---|---|
| Variables | Statin Use | No Statin Use | p-Value | StD |
| n = 555 | n = 555 | |||
| HDL-C adm, mmol/L | 1.41 (1.17–1.72) | 1.41 (1.12–1.74) | 0.8870 | 0.0342 |
| TG adm, mmol/L | 1.17 (0.83–1.65) | 1.11 (0.79–1.64) | 0.2502 | 0.0122 |
| TCHO adm, mmol/L | 4.63 (3.98–5.25) | 5.12 (4.42–5.77) | <0.0001 | 0.4583 |
| LDL-C adm, mmol/L | 2.54 (2.03–3.03) | 2.99 (2.44–3.57) | <0.0001 | 0.3668 |
| SVO, n (%) | 73 (13.2%) | 86 (15.5%) | 0.2651 | 0.0671 |
| LAA, n (%) | 175 (31.5%) | 158 (28.5%) | 0.2654 | 0.0668 |
| Cardioembolism, n (%) | 170 (30.6%) | 196 (35.3%) | 0.0968 | 0.0999 |
| ODE or UE, n (%) | 137 (24.7%) | 115 (20.7%) | 0.1148 | 0.0946 |
| NIHSS score adm | 3 (1–9) | 4 (2–11) | 0.0009 | 0.1145 |
| NIHSS score adm ≤3, n (%) | 286 (51.5%) | 252 (45.4%) | 0.0411 | 0.1227 |
| Hospitalization, days | 8 (7–9) | 8 (7–9) | 0.6212 | 0.0412 |
| Discharge to home, n (%) | 289 (52.1%) | 253 (45.6%) | 0.0306 | 0.1299 |
| No Pre-Stroke Statin | Total | p-Value | |||
|---|---|---|---|---|---|
| NIHSS Score Adm ≤ 3 | NIHSS Score Adm ≥ 4 | ||||
| Pre-stroke statin use | NIHSS score adm ≤ 3 | 134 | 152 | 286 | 0.0385 |
| NIHSS score adm ≥ 4 | 118 | 151 | 269 | ||
| Total | 252 | 303 | 555 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, T.; Yoshioka, K.; Miyazaki, Y. Pre-Stroke Statin Use Is Associated with Mild Neurological Deficits at the Onset of Acute Ischemic Stroke. J. Cardiovasc. Dev. Dis. 2022, 9, 396. https://doi.org/10.3390/jcdd9110396
Mori T, Yoshioka K, Miyazaki Y. Pre-Stroke Statin Use Is Associated with Mild Neurological Deficits at the Onset of Acute Ischemic Stroke. Journal of Cardiovascular Development and Disease. 2022; 9(11):396. https://doi.org/10.3390/jcdd9110396
Chicago/Turabian StyleMori, Takahisa, Kazuhiro Yoshioka, and Yuichi Miyazaki. 2022. "Pre-Stroke Statin Use Is Associated with Mild Neurological Deficits at the Onset of Acute Ischemic Stroke" Journal of Cardiovascular Development and Disease 9, no. 11: 396. https://doi.org/10.3390/jcdd9110396