
Personalised Treatment in Aortic Stenosis: A Patient-Tailored Transcatheter Aortic Valve Implantation Approach
 , ,
, ,
Abstract
:1. Introduction
2. Overview of the Available THVs
2.1. SAPIEN Family BEV
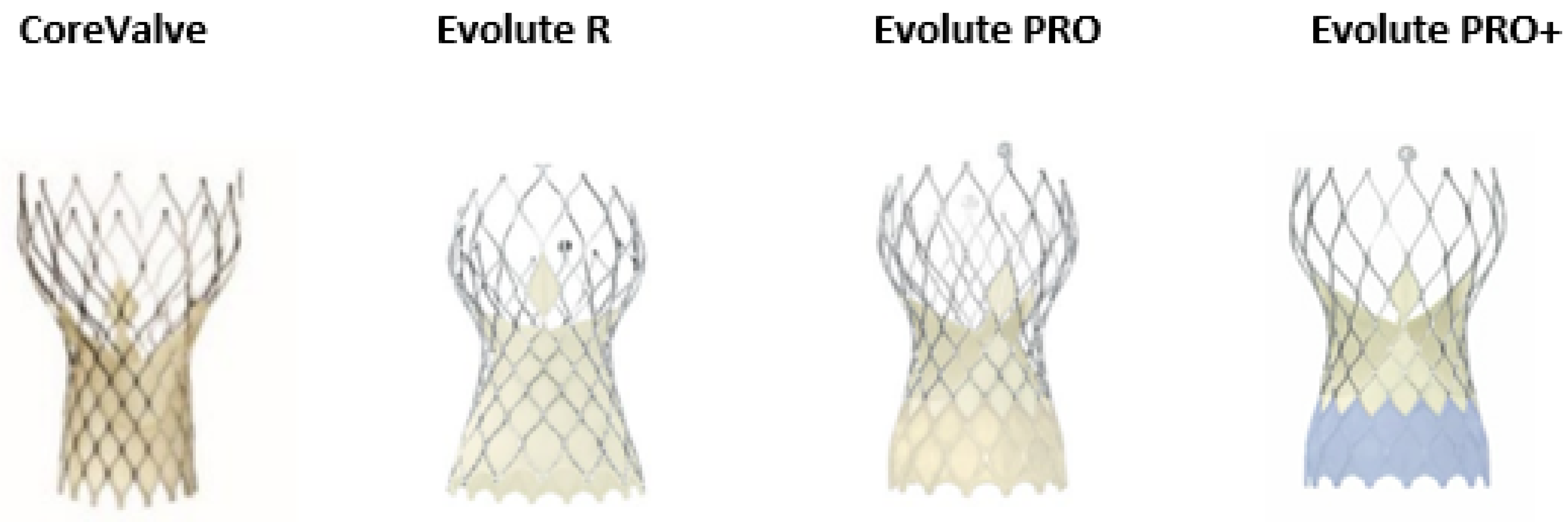
2.2. The CoreValve/Evolut Family SEV
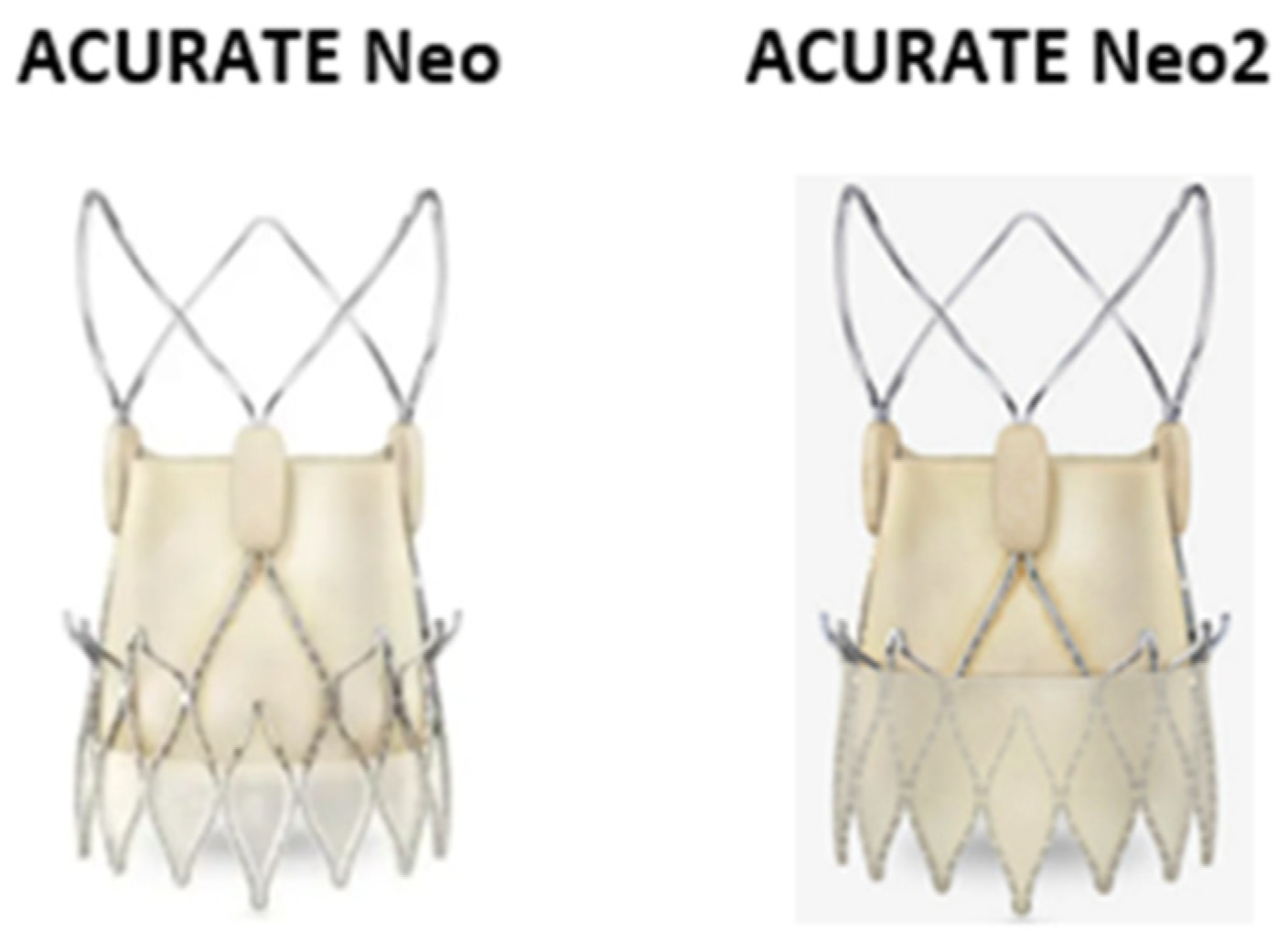
2.3. The ACURATE Neo/ACURATE Neo 2 SEV
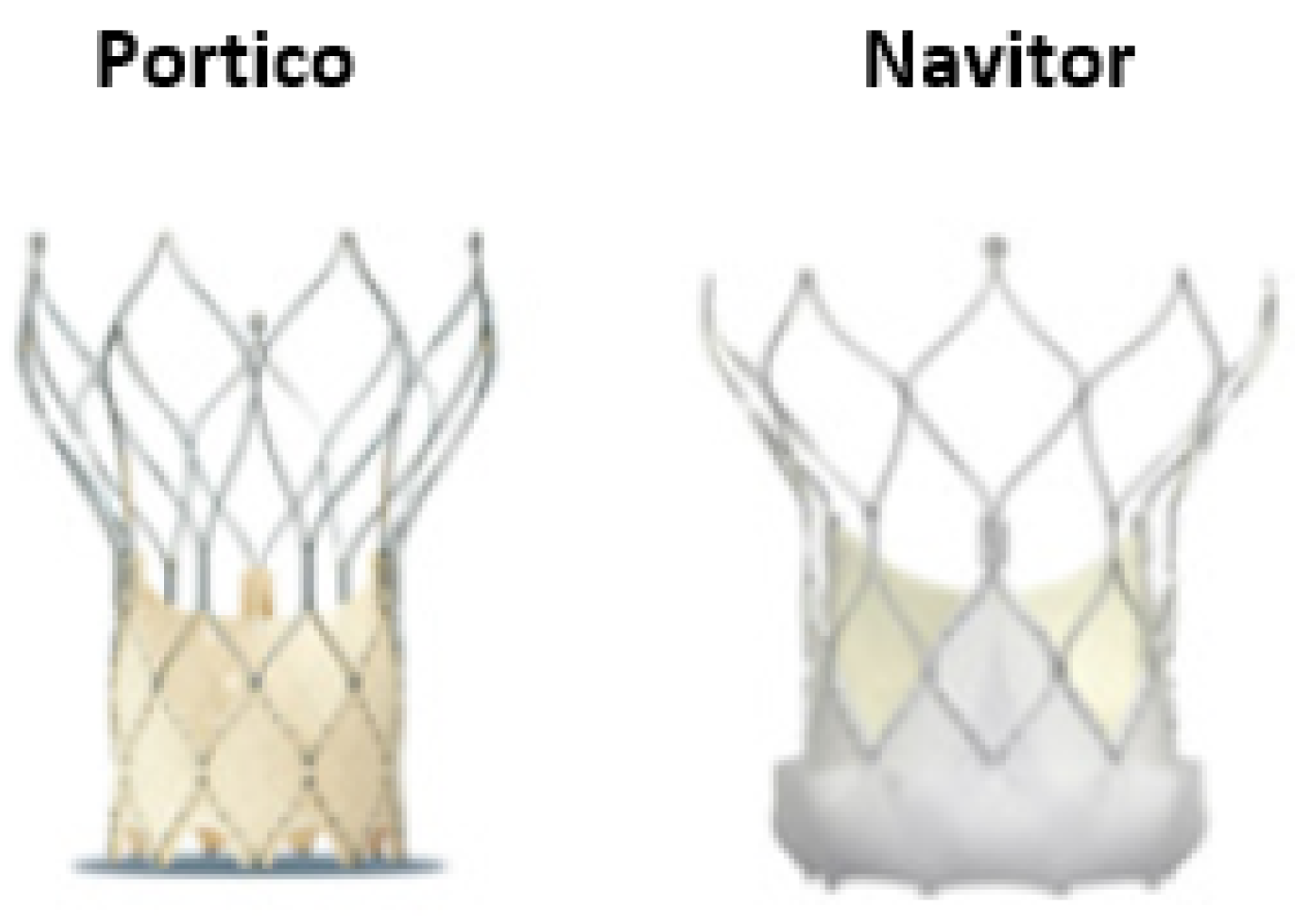
2.4. Portico and Navitor SEV
2.5. Myval BEV
3. Patient-Specific Characteristics
3.1. Patients with a Severely Calcified Annulus
3.2. Patients with Horizontal Aorta
3.3. Patients with Extreme Annulus Dimensions or Difficult Sizing
3.4. Patients with Bicuspid Aortic Valve
3.5. Patients with Limited Transfemoral Access
3.6. Patients at High Risk for Conduction Abnormalities
3.7. Patients with a Need for Future Coronary Engagement
3.8. Life-Time Management of Patients with Severe Aortic Stenosis
4. Conclusions
5. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef] [PubMed]
- Rotman, O.M.; Bianchi, M.; Ghosh, R.P.; Kovarovic, B.; Bluestein, D. Principles of TAVR Valve Design, Modelling, and Testing. Expert Rev. Med. Devices 2018, 15, 771–791. [Google Scholar] [CrossRef] [PubMed]
- Hahn, R.T.; Leipsic, J.; Douglas, P.S.; Jaber, W.A.; Weissman, N.J.; Pibarot, P.; Blanke, P.; Oh, J.K. Comprehensive Echocardiographic Assessment of Normal Transcatheter Valve Function. JACC Cardiovasc. Imaging 2019, 12, 25–34. [Google Scholar] [CrossRef]
- Pellegrini, C.; Rheude, T.; Michel, J.; Alvarez-Covarrubias, H.A.; Wünsch, S.; Mayr, N.P.; Xhepa, E.; Kastrati, A.; Schunkert, H.; Joner, M.; et al. Comparison of Latest Generation Supra-Annular and Intra-Annular Self-Expanding Transcatheter Heart Valves. J. Thorac. Dis. 2020, 12, 6769–6779. [Google Scholar] [CrossRef]
- Leon, M.B.; Smith, C.R.; Mack, M.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter Aortic-Valve Implantation for Aortic Stenosis in Patients Who Cannot Undergo Surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus Surgical Aortic-Valve Replacement in High-Risk Patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef] [Green Version]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef]
- Herrmann, H.C.; Thourani, V.H.; Kodali, S.K.; Makkar, R.R.; Szeto, W.Y.; Anwaruddin, S.; Desai, N.; Lim, S.; Malaisrie, S.C.; Kereiakes, D.J.; et al. One-Year Clinical Outcomes With SAPIEN 3 Transcatheter Aortic Valve Replacement in High-Risk and Inoperable Patients With Severe Aortic Stenosis. Circulation 2016, 134, 130–140. [Google Scholar] [CrossRef]
- Thourani, V.H.; Kodali, S.; Makkar, R.R.; Herrmann, H.H.C.; Williams, M.; Babaliaros, V.; Smalling, R.; Lim, S.; Malaisrie, S.C.; Kapadia, S.; et al. Transcatheter Aortic Valve Replacement versus Surgical Valve Replacement in Intermediate-Risk Patients: A Propensity Score Analysis. Lancet 2016, 387, 2218–2225. [Google Scholar] [CrossRef]
- Barbanti, M.; Costa, G. SAPIEN 3 Ultra Transcatheter Aortic Valve Device. JACC Cardiovasc. Interv. 2020, 13, 2639–2641. [Google Scholar] [CrossRef] [PubMed]
- Rheude, T.; Pellegrini, C.; Lutz, J.; Alvarez-Covarrubias, H.A.; Lahmann, A.L.; Mayr, N.P.; Michel, J.; Kasel, M.A.; Joner, M.; Xhepa, E. Transcatheter Aortic Valve Replacement With Balloon-Expandable Valves: Comparison of SAPIEN 3 Ultra Versus SAPIEN 3. JACC Cardiovasc. Interv. 2020, 13, 2631–2638. [Google Scholar] [CrossRef]
- Adams, D.H.; Popma, J.J.; Reardon, M.J.; Yakubov, S.J.; Coselli, J.S.; Deeb, G.M.; Gleason, T.G.; Buchbinder, M.; Hermiller, J.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Prosthesis. N. Engl. J. Med. 2014, 370, 1790–1798. [Google Scholar] [CrossRef] [Green Version]
- Van Mieghem, N.M.; Nuis, R.-J.; Piazza, N.; Apostolos, T.; Ligthart, J.; Schultz, C.; de Jaegere, P.P.; Serruys, P.W. Vascular Complications with Transcatheter Aortic Valve Implantation Using the 18 Fr Medtronic CoreValve System: The Rotterdam Experience. EuroIntervention 2010, 5, 673–679. [Google Scholar] [CrossRef]
- Van der Boon, R.M.; Nuis, R.-J.; Van Mieghem, N.M.; Jordaens, L.; Rodés-Cabau, J.; van Domburg, R.T.; Serruys, P.W.; Anderson, R.H.; de Jaegere, P.P.T. New Conduction Abnormalities after TAVI--Frequency and Causes. Nat. Rev. Cardiol. 2012, 9, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Sherif, M.A.; Abdel-Wahab, M.; Stöcker, B.; Geist, V.; Richardt, D.; Tölg, R.; Richardt, G. Anatomic and Procedural Predictors of Paravalvular Aortic Regurgitation after Implantation of the Medtronic CoreValve Bioprosthesis. J. Am. Coll. Cardiol. 2010, 56, 1623–1629. [Google Scholar] [CrossRef] [Green Version]
- Eggebrecht, H.; Schmermund, A.; Voigtländer, T.; Kahlert, P.; Erbel, R.; Mehta, R.H. Risk of Stroke after Transcatheter Aortic Valve Implantation (TAVI): A Meta-Analysis of 10,037 Published Patients. EuroIntervention 2012, 8, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Reardon, M.J.; Khabbaz, K.; Harrison, J.K.; Hughes, G.C.; Kodali, S.; George, I.; Deeb, G.M.; Chetcuti, S.; Kipperman, R.; et al. Early Clinical Outcomes After Transcatheter Aortic Valve Replacement Using a Novel Self-Expanding Bioprosthesis in Patients With Severe Aortic Stenosis Who Are Suboptimal for Surgery: Results of the Evolut R U.S. Study. JACC Cardiovasc. Interv. 2017, 10, 268–275. [Google Scholar] [CrossRef]
- Gomes, B.; Geis, N.A.; Chorianopoulos, E.; Meder, B.; Leuschner, F.; Katus, H.A.; Bekeredjian, R. Improvements of Procedural Results With a New-Generation Self-Expanding Transfemoral Aortic Valve Prosthesis in Comparison to the Old-Generation Device. J. Interv. Cardiol. 2017, 30, 72–78. [Google Scholar] [CrossRef] [Green Version]
- Kalra, S.S.; Firoozi, S.; Yeh, J.; Blackman, D.J.; Rashid, S.; Davies, S.; Moat, N.; Dalby, M.; Kabir, T.; Khogali, S.S.; et al. Initial Experience of a Second-Generation Self-Expanding Transcatheter Aortic Valve: The UK & Ireland Evolut R Implanters’ Registry. JACC Cardiovasc. Interv. 2017, 10, 276–282. [Google Scholar] [CrossRef]
- Forrest, J.K.; Mangi, A.A.; Popma, J.J.; Khabbaz, K.; Reardon, M.J.; Kleiman, N.S.; Yakubov, S.J.; Watson, D.; Kodali, S.; George, I.; et al. Early Outcomes With the Evolut PRO Repositionable Self-Expanding Transcatheter Aortic Valve With Pericardial Wrap. JACC Cardiovasc. Interv. 2018, 11, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Jilaihawi, H.; Zhao, Z.; Du, R.; Staniloae, C.; Saric, M.; Neuburger, P.J.; Querijero, M.; Vainrib, A.; Hisamoto, K.; Ibrahim, H.; et al. Minimizing Permanent Pacemaker Following Repositionable Self-Expanding Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2019, 12, 1796–1807. [Google Scholar] [CrossRef]
- Eikelboom, R.; Moran, R.M.; Yan, W.; Yamashita, M.; Patel, A.; Reardon, M.; Spooner, A. Current and Future Transcatheter Aortic Valve Replacement Valves. Curr. Opin. Cardiol. 2022, 37, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Panagides, V.; Mesnier, J.; Nuche, J.; Delarochellière, R.; Paradis, J.-M.; Kalavrouziotis, D.; Dumont, E.; Mohammadi, S.; Rodes-Cabau, J. From the Evolut Pro to the Evolut FX Self-Expanding Transcatheter Aortic Valve Replacement Systems: Current Status and Future Perspectives. Expert Rev. Med. Devices 2022, 19, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Möllmann, H.; Walther, T.; Siqueira, D.; Diemert, P.; Treede, H.; Grube, E.; Nickenig, G.; Baldus, S.; Rudolph, T.; Kuratani, T.; et al. Transfemoral TAVI Using the Self-Expanding ACURATE Neo Prosthesis: One-Year Outcomes of the Multicentre “CE-Approval Cohort”. EuroIntervention 2017, 13, e1040–e1046. [Google Scholar] [CrossRef] [PubMed]
- Scotti, A.; Pagnesi, M.; Kim, W.-K.; Schäfer, U.; Barbanti, M.; Costa, G.; Baggio, S.; Casenghi, M.; De Marco, F.; Vanhaverbeke, M.; et al. Haemodynamic Performance and Clinical Outcomes of Transcatheter Aortic Valve Replacement with the Self-Expanding ACURATE Neo2. EuroIntervention 2022, 18, EIJ-D-22-00289. [Google Scholar] [CrossRef]
- Buono, A.; Gorla, R.; Ielasi, A.; Costa, G.; Cozzi, O.; Ancona, M.; Soriano, F.; De Carlo, M.; Ferrara, E.; Giannini, F.; et al. Transcatheter Aortic Valve Replacement With Self-Expanding ACURATE Neo2: Postprocedural Hemodynamic and Short-Term Clinical Outcomes. JACC Cardiovasc. Interv. 2022, 15, 1101–1110. [Google Scholar] [CrossRef]
- Lanz, J.; Kim, W.-K.; Walther, T.; Burgdorf, C.; Möllmann, H.; Linke, A.; Redwood, S.; Thilo, C.; Hilker, M.; Joner, M.; et al. Safety and Efficacy of a Self-Expanding versus a Balloon-Expandable Bioprosthesis for Transcatheter Aortic Valve Replacement in Patients with Symptomatic Severe Aortic Stenosis: A Randomised Non-Inferiority Trial. Lancet 2019, 394, 1619–1628. [Google Scholar] [CrossRef]
- Moriyama, N.; Vento, A.; Laine, M. Safety of Next-Day Discharge After Transfemoral Transcatheter Aortic Valve Replacement With a Self-Expandable Versus Balloon-Expandable Valve Prosthesis. Circ. Cardiovasc. Interv. 2019, 12, e007756. [Google Scholar] [CrossRef]
- Purita, P.A.M.; Tahoces, L.S.; Fraccaro, C.; Nai Fovino, L.; Kim, W.-K.; Espada-Guerreiro, C.; De Backer, O.; Seiffert, M.; Nombela-Franco, L.; Gomez, R.M.; et al. Transcatheter Treatment of Native Aortic Valve Regurgitation: Results from an International Registry Using the Transfemoral ACURATE Neo Valve. Int. J. Cardiol. Heart Vasc. 2020, 27, 100480. [Google Scholar] [CrossRef]
- Wong, I.; Bajoras, V.; Wang, X.; Bieliauskas, G.; De Backer, O.; Søndergaard, L. Technical Considerations for Transcatheter Aortic Valve Replacement With the Navitor Transcatheter Heart Valve. JACC Cardiovasc. Interv. 2021, 14, e259–e261. [Google Scholar] [CrossRef] [PubMed]
- Corcione, N.; Morello, A.; Ferraro, P.; Cimmino, M.; Albanese, M.; Ausiello, A.; Pepe, M.; Biondi-Zoccai, G.; Giordano, A. The Novel FlexNav Delivery System for Transcatheter Aortic Valve Implantation With the Portico Device: A Case Series. J. Invasive Cardiol. 2021, 33, E474–E478. [Google Scholar] [PubMed]
- Kawashima, H.; Soliman, O.; Wang, R.; Ono, M.; Hara, H.; Gao, C.; Zeller, E.; Thakkar, A.; Tamburino, C.; Bedogni, F.; et al. Rationale and Design of a Randomized Clinical Trial Comparing Safety and Efficacy of Myval Transcatheter Heart Valve versus Contemporary Transcatheter Heart Valves in Patients with Severe Symptomatic Aortic Valve Stenosis: The LANDMARK Trial. Am. Heart J. 2021, 232, 23–38. [Google Scholar] [CrossRef]
- Sharma, S.K.; Rao, R.S.; Chandra, P.; Goel, P.K.; Bharadwaj, P.; Joseph, G.; Jose, J.; Mahajan, A.U.; Mehrotra, S.; Sengottovelu, G.; et al. First-in-Human Evaluation of a Novel Balloon-Expandable Transcatheter Heart Valve in Patients with Severe Symptomatic Native Aortic Stenosis: The MyVal-1 Study. EuroIntervention 2020, 16, 421–429. [Google Scholar] [CrossRef]
- Ko, E.; Kang, D.-Y.; Ahn, J.-M.; Kim, T.O.; Kim, J.H.; Lee, J.; Lee, S.-A.; Kim, D.-H.; Kim, H.J.; Kim, J.B.; et al. Association of Aortic Valvular Complex Calcification Burden with Procedural and Long-Term Clinical Outcomes after Transcatheter Aortic Valve Replacement. Eur. Heart J. Cardiovasc. Imaging 2021, 23, 1502–1510. [Google Scholar] [CrossRef]
- Kim, W.-K.; Bhumimuang, K.; Renker, M.; Fischer-Rasokat, U.; Möllmann, H.; Walther, T.; Choi, Y.-H.; Nef, H.; Hamm, C.W. Determinants of Paravalvular Leakage Following Transcatheter Aortic Valve Replacement in Patients with Bicuspid and Tricuspid Aortic Stenosis. Eur. Heart J. Cardiovasc. Imaging 2021, 12, 1387–1396. [Google Scholar] [CrossRef] [PubMed]
- Larroche, J.; Panh, L.; Lhermusier, T.; Bataille, V.; Marachet, M.-A.; Chollet, T.; Petermann, A.; Bouisset, F.; Boudou, N.; Marcheix, B.; et al. Impact of Aortic Valve Calcification Severity on Device Success after Transcatheter Aortic Valve Replacement. Int. J. Cardiovasc. Imaging 2020, 36, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Akodad, M.; Lattuca, B.; Agullo, A.; Macia, J.-C.; Gandet, T.; Marin, G.; Iemmi, A.; Vernhet, H.; Schmutz, L.; Nagot, N.; et al. Prognostic Impact of Calcium Score after Transcatheter Aortic Valve Implantation Performed With New Generation Prosthesis. Am. J. Cardiol. 2018, 121, 1225–1230. [Google Scholar] [CrossRef]
- Okuno, T.; Asami, M.; Heg, D.; Lanz, J.; Praz, F.; Hagemeyer, D.; Brugger, N.; Gräni, C.; Huber, A.; Spirito, A.; et al. Impact of Left Ventricular Outflow Tract Calcification on Procedural Outcomes After Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2020, 13, 1789–1799. [Google Scholar] [CrossRef]
- Blanke, P.; Reinöhl, J.; Schlensak, C.; Siepe, M.; Pache, G.; Euringer, W.; Geibel-Zehender, A.; Bode, C.; Langer, M.; Beyersdorf, F.; et al. Prosthesis Oversizing in Balloon-Expandable Transcatheter Aortic Valve Implantation Is Associated with Contained Rupture of the Aortic Root. Circ. Cardiovasc. Interv. 2012, 5, 540–548. [Google Scholar] [CrossRef]
- Barbanti, M.; Yang, T.-H.; Rodès Cabau, J.; Tamburino, C.; Wood, D.A.; Jilaihawi, H.; Blanke, P.; Makkar, R.R.; Latib, A.; Colombo, A.; et al. Anatomical and Procedural Features Associated with Aortic Root Rupture during Balloon-Expandable Transcatheter Aortic Valve Replacement. Circulation 2013, 128, 244–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, W.-K.; Schäfer, U.; Tchetche, D.; Nef, H.; Arnold, M.; Avanzas, P.; Rudolph, T.; Scholtz, S.; Barbanti, M.; Kempfert, J.; et al. Incidence and Outcome of Peri-Procedural Transcatheter Heart Valve Embolization and Migration: The TRAVEL Registry (TranscatheteR HeArt Valve EmboLization and Migration). Eur. Heart J. 2019, 40, 3156–3165. [Google Scholar] [CrossRef] [Green Version]
- Kunkel, K.J.; Fiorilli, P.; Kobayashi, T.; Desai, N.D.; Anwaruddin, S.; Herrmann, H.C. Snare-Assisted Valve Positioning of Self-Expanding Valves for Transcatheter Aortic Valve Replacement. JACC Case Rep. 2021, 3, 658–662. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Dai, H.; Wang, L.; Fan, J.; Wang, J. Novel Apical-to-Femoral Rail Technique for Horizontal Aorta in Transcatheter Aortic Valve Replacement. J. Zhejiang Univ. Sci. B 2022, 23, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Gorla, R.; De Marco, F.; Garatti, A.; Bianchi, G.; Popolo Rubbio, A.; Acerbi, E.; Casenghi, M.; Spagnolo, P.; Brambilla, N.; Testa, L.; et al. Impact of Aortic Angle on Transcatheter Aortic Valve Implantation Outcome with Evolut-R, Portico, and Acurate-NEO. Catheter. Cardiovasc. Interv. 2021, 97, E135–E145. [Google Scholar] [CrossRef]
- Gallo, F.; Gallone, G.; Kim, W.-K.; Reifart, J.; Veulemans, V.; Zeus, T.; Toggweiler, S.; De Backer, O.; Søndergaard, L.; Mangieri, A.; et al. Horizontal Aorta in Transcatheter Self-Expanding Valves: Insights From the HORSE International Multicentre Registry. Circ. Cardiovasc. Interv. 2021, 14, e010641. [Google Scholar] [CrossRef]
- Veulemans, V.; Maier, O.; Bosbach, G.; Polzin, A.; Piayda, K.; Afzal, S.; Jung, C.; Westenfeld, R.; Kelm, M.; Zeus, T. Novel Insights on Outcome in Horizontal Aorta with Self-Expandable New-Generation Transcatheter Aortic Valve Replacement Devices. Catheter. Cardiovasc. Interv. 2020, 96, 1511–1519. [Google Scholar] [CrossRef]
- Medranda, G.A.; Musallam, A.; Zhang, C.; Rappaport, H.; Gallino, P.E.; Case, B.C.; Satler, L.F.; Ben-Dor, I.; Rogers, T.; Waksman, R. The Impact of Aortic Angulation on Contemporary Transcatheter Aortic Valve Replacement Outcomes. JACC Cardiovasc. Interv. 2021, 14, 1209–1215. [Google Scholar] [CrossRef]
- Abramowitz, Y.; Maeno, Y.; Chakravarty, T.; Kazuno, Y.; Takahashi, N.; Kawamori, H.; Mangat, G.; Cheng, W.; Jilaihawi, H.; Makkar, R.R. Aortic Angulation Attenuates Procedural Success Following Self-Expandable But Not Balloon-Expandable TAVR. JACC Cardiovasc. Imaging 2016, 9, 964–972. [Google Scholar] [CrossRef]
- Bax, J.J.; Delgado, V.; Bapat, V.; Baumgartner, H.; Collet, J.P.; Erbel, R.; Hamm, C.; Kappetein, A.P.; Leipsic, J.; Leon, M.B.; et al. Open Issues in Transcatheter Aortic Valve Implantation. Part 2: Procedural Issues and Outcomes after Transcatheter Aortic Valve Implantation. Eur. Heart J. 2014, 35, 2639–2654. [Google Scholar] [CrossRef]
- Rao, V.; Jamieson, W.R.; Ivanov, J.; Armstrong, S.; David, T.E. Prosthesis-Patient Mismatch Affects Survival after Aortic Valve Replacement. Circulation 2000, 102, III5-9. [Google Scholar] [CrossRef] [PubMed]
- Walther, T.; Rastan, A.; Falk, V.; Lehmann, S.; Garbade, J.; Funkat, A.K.; Mohr, F.W.; Gummert, J.F. Patient Prosthesis Mismatch Affects Short- and Long-Term Outcomes after Aortic Valve Replacement. Eur. J. Cardiothorac. Surg. 2006, 30, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Takagi, H.; Yamamoto, H.; Iwata, K.; Goto, S.-N.; Umemoto, T. A Meta-Analysis of Effects of Prosthesis-Patient Mismatch after Aortic Valve Replacement on Late Mortality. Int. J. Cardiol. 2012, 159, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Takagi, H.; Umemoto, T. ALICE (All-Literature Investigation of Cardiovascular Evidence) Group Prosthesis-Patient Mismatch After Transcatheter Aortic Valve Implantation. Ann. Thorac. Surg. 2016, 101, 872–880. [Google Scholar] [CrossRef] [Green Version]
- Herrmann, H.C.; Daneshvar, S.A.; Fonarow, G.C.; Stebbins, A.; Vemulapalli, S.; Desai, N.D.; Malenka, D.J.; Thourani, V.H.; Rymer, J.; Kosinski, A.S. Prosthesis-Patient Mismatch in Patients Undergoing Transcatheter Aortic Valve Replacement: From the STS/ACC TVT Registry. J. Am. Coll. Cardiol. 2018, 72, 2701–2711. [Google Scholar] [CrossRef] [PubMed]
- Abbas, A.E.; Ternacle, J.; Pibarot, P.; Xu, K.; Alu, M.; Rogers, E.; Hahn, R.T.; Leon, M.; Thourani, V.H. Impact of Flow on Prosthesis-Patient Mismatch Following Transcatheter and Surgical Aortic Valve Replacement. Circ. Cardiovasc. Imaging 2021, 14, e012364. [Google Scholar] [CrossRef]
- Yanagisawa, R.; Tanaka, M.; Yashima, F.; Arai, T.; Jinzaki, M.; Shimizu, H.; Fukuda, K.; Watanabe, Y.; Naganuma, T.; Higashimori, A.; et al. Early and Late Leaflet Thrombosis After Transcatheter Aortic Valve Replacement. Circ. Cardiovasc. Interv. 2019, 12, e007349. [Google Scholar] [CrossRef]
- Kagemoto, Y.; Weintraub, A.; Pandian, N.G.; Rastegar, H.; Halin, N.; Cobey, F.C. Late Clinical Presentation of Prosthesis-Patient Mismatch Following Transcatheter Aortic Valve Replacement. J. Cardiothorac. Vasc. Anesth. 2019, 33, 245–248. [Google Scholar] [CrossRef] [Green Version]
- Leone, P.P.; Regazzoli, D.; Pagnesi, M.; Sanz-Sanchez, J.; Chiarito, M.; Cannata, F.; Van Mieghem, N.M.; Barbanti, M.; Tamburino, C.; Teles, R.; et al. Predictors and Clinical Impact of Prosthesis-Patient Mismatch After Self-Expandable TAVR in Small Annuli. JACC Cardiovasc. Interv. 2021, 14, 1218–1228. [Google Scholar] [CrossRef]
- Tang, G.H.L.; Sengupta, A.; Alexis, S.L.; Bapat, V.N.; Adams, D.H.; Sharma, S.K.; Kini, A.S.; Kodali, S.K.; Ramlawi, B.; Gada, H.; et al. Outcomes of Prosthesis-Patient Mismatch Following Supra-Annular Transcatheter Aortic Valve Replacement: From the STS/ACC TVT Registry. JACC Cardiovasc. Interv. 2021, 14, 964–976. [Google Scholar] [CrossRef]
- Potratz, M.; Mohemed, K.; Omran, H.; Gortamashvili, L.; Friedrichs, K.P.; Scholtz, W.; Scholtz, S.; Rudolph, V.; Piper, C.; Gilis-Januszewski, T.; et al. Hemodynamic Performance of Two Current-Generation Transcatheter Heart Valve Prostheses in Severely Calcified Aortic Valve Stenosis. J. Clin. Med. 2022, 11, 4570. [Google Scholar] [CrossRef] [PubMed]
- Okuno, T.; Khan, F.; Asami, M.; Praz, F.; Heg, D.; Winkel, M.G.; Lanz, J.; Huber, A.; Gräni, C.; Räber, L.; et al. Prosthesis-Patient Mismatch Following Transcatheter Aortic Valve Replacement With Supra-Annular and Intra-Annular Prostheses. JACC Cardiovasc. Interv. 2019, 12, 2173–2182. [Google Scholar] [CrossRef] [PubMed]
- Mauri, V.; Kim, W.K.; Abumayyaleh, M.; Walther, T.; Moellmann, H.; Schaefer, U.; Conradi, L.; Hengstenberg, C.; Hilker, M.; Wahlers, T.; et al. Short-Term Outcome and Hemodynamic Performance of Next-Generation Self-Expanding Versus Balloon-Expandable Transcatheter Aortic Valves in Patients With Small Aortic Annulus: A Multicenter Propensity-Matched Comparison. Circ. Cardiovasc. Interv. 2017, 10, e005013. [Google Scholar] [CrossRef] [PubMed]
- Abdelghani, M.; Mankerious, N.; Allali, A.; Landt, M.; Kaur, J.; Sulimov, D.S.; Merten, C.; Sachse, S.; Mehilli, J.; Neumann, F.-J.; et al. Bioprosthetic Valve Performance After Transcatheter Aortic Valve Replacement With Self-Expanding Versus Balloon-Expandable Valves in Large Versus Small Aortic Valve Annuli. JACC Cardiovascular. Interv. 2018, 11, 2507–2518. [Google Scholar] [CrossRef]
- Tang, G.H.L.; Zaid, S.; George, I.; Khalique, O.K.; Abramowitz, Y.; Maeno, Y.; Makkar, R.R.; Jilaihawi, H.; Kamioka, N.; Thourani, V.H.; et al. Impact of Aortic Root Anatomy and Geometry on Paravalvular Leak in Transcatheter Aortic Valve Replacement With Extremely Large Annuli Using the Edwards SAPIEN 3 Valve. JACC Cardiovasc. Interv. 2018, 11, 1377–1387. [Google Scholar] [CrossRef]
- Sengupta, A.; Zaid, S.; Kamioka, N.; Terre, J.; Miyasaka, M.; Hirji, S.A.; Hensey, M.; Geloo, N.; Petrossian, G.; Robinson, N.; et al. Mid-Term Outcomes of Transcatheter Aortic Valve Replacement in Extremely Large Annuli With Edwards SAPIEN 3 Valve. JACC Cardiovasc. Interv. 2020, 13, 210–216. [Google Scholar] [CrossRef]
- Armijo, G.; Tang, G.H.L.; Kooistra, N.; Ferreira-Neto, A.N.; Toggweiler, S.; Amat-Santos, I.J.; Keller, L.S.; Urena, M.; Ahmad, H.; Tafur Soto, J.; et al. Third-Generation Balloon and Self-Expandable Valves for Aortic Stenosis in Large and Extra-Large Aortic Annuli From the TAVR-LARGE Registry. Circ. Cardiovasc. Interv. 2020, 13, e009047. [Google Scholar] [CrossRef]
- Okuno, T.; Heg, D.; Lanz, J.; Praz, F.; Gräni, C.; Langhammer, B.; Reineke, D.; Räber, L.; Wenaweser, P.; Pilgrim, T.; et al. Heart Valve Sizing and Clinical Outcomes in Patients Undergoing Transcatheter Aortic Valve Implantation. Catheter. Cardiovasc. Interv. 2021, 98, E768–E779. [Google Scholar] [CrossRef]
- Acconcia, M.C.; Caretta, Q.; Monzo, L.; Tanzilli, G.; Sili Scavalli, A.; Sergi, D.; Di Luozzo, M.; Marchei, M.; Chiocchi, M.; Romeo, F.; et al. Effectiveness of the New Generation Transcatheter Aortic Valve in the Real Life Studies. Review and Meta-Analysis. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 8018–8027. [Google Scholar] [CrossRef]
- Alperi, A.; Faroux, L.; Muntané-Carol, G.; Rodés-Cabau, J. Meta-Analysis Comparing Early Outcomes Following Transcatheter Aortic Valve Implantation With the Evolut Versus Sapien 3 Valves. Am. J. Cardiol. 2021, 139, 87–96. [Google Scholar] [CrossRef]
- Sakellaropoulos, S.; Mohammed, M.; Svab, S.; Lekaditi, D.; Sakellaropoulos, P.; Mitsis, A. Causes, Diagnosis, Risk Stratification and Treatment of Bicuspid Aortic Valve Disease: An Updated Review. Cardiol. Res. 2020, 11, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.V.; Omar, W.; Gonzalez, P.E.; Jessen, M.E.; Huffman, L.; Kumbhani, D.J.; Bavry, A.A. Expansion of TAVR into Low-Risk Patients and Who to Consider for SAVR. Cardiol. Ther. 2020, 9, 377–394. [Google Scholar] [CrossRef] [PubMed]
- Tchetche, D.; de Biase, C.; van Gils, L.; Parma, R.; Ochala, A.; Lefevre, T.; Hovasse, T.; De Backer, O.; Sondergaard, L.; Bleiziffer, S.; et al. Bicuspid Aortic Valve Anatomy and Relationship With Devices: The BAVARD Multicenter Registry. Circ. Cardiovasc. Interv. 2019, 12, e007107. [Google Scholar] [CrossRef]
- Shibayama, K.; Harada, K.; Berdejo, J.; Tanaka, J.; Mihara, H.; Itabashi, Y.; Shiota, T. Comparison of Aortic Root Geometry with Bicuspid versus Tricuspid Aortic Valve: Real-Time Three-Dimensional Transesophageal Echocardiographic Study. J. Am. Soc. Echocardiogr. 2014, 27, 1143–1152. [Google Scholar] [CrossRef] [PubMed]
- Montalto, C.; Sticchi, A.; Crimi, G.; Laricchia, A.; Khokhar, A.A.; Giannini, F.; Reimers, B.; Colombo, A.; Latib, A.; Waksman, R.; et al. Outcomes After Transcatheter Aortic Valve Replacement in Bicuspid Versus Tricuspid Anatomy: A Systematic Review and Meta-Analysis. JACC Cardiovasc. Interv. 2021, 14, 2144–2155. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.-K.; Renker, M.; Rolf, A.; Fischer-Rasokat, U.; Wiedemeyer, J.; Doss, M.; Möllmann, H.; Walther, T.; Nef, H.; Hamm, C.W.; et al. Annular versus Supra-Annular Sizing for TAVI in Bicuspid Aortic Valve Stenosis. EuroIntervention 2019, 15, e231–e238. [Google Scholar] [CrossRef] [Green Version]
- Michelena, H.I.; Prakash, S.K.; Della Corte, A.; Bissell, M.M.; Anavekar, N.; Mathieu, P.; Bossé, Y.; Limongelli, G.; Bossone, E.; Benson, D.W.; et al. Bicuspid Aortic Valve: Identifying Knowledge Gaps and Rising to the Challenge from the International Bicuspid Aortic Valve Consortium (BAVCon). Circulation 2014, 129, 2691–2704. [Google Scholar] [CrossRef] [Green Version]
- Makkar, R.R.; Yoon, S.-H.; Leon, M.B.; Chakravarty, T.; Rinaldi, M.; Shah, P.B.; Skipper, E.R.; Thourani, V.H.; Babaliaros, V.; Cheng, W.; et al. Association Between Transcatheter Aortic Valve Replacement for Bicuspid vs Tricuspid Aortic Stenosis and Mortality or Stroke. JAMA 2019, 321, 2193–2202. [Google Scholar] [CrossRef] [Green Version]
- Yoon, S.-H.; Bleiziffer, S.; De Backer, O.; Delgado, V.; Arai, T.; Ziegelmueller, J.; Barbanti, M.; Sharma, R.; Perlman, G.Y.; Khalique, O.K.; et al. Outcomes in Transcatheter Aortic Valve Replacement for Bicuspid Versus Tricuspid Aortic Valve Stenosis. J. Am. Coll. Cardiol. 2017, 69, 2579–2589. [Google Scholar] [CrossRef] [Green Version]
- Mangieri, A.; Tchetchè, D.; Kim, W.-K.; Pagnesi, M.; Sinning, J.-M.; Landes, U.; Kornowski, R.; De Backer, O.; Nickenig, G.; Ielasi, A.; et al. Balloon Versus Self-Expandable Valve for the Treatment of Bicuspid Aortic Valve Stenosis: Insights From the BEAT International Collaborative Registrys. Circ. Cardiovasc. Interv. 2020, 13, e008714. [Google Scholar] [CrossRef]
- Forrest, J.K.; Ramlawi, B.; Deeb, G.M.; Zahr, F.; Song, H.K.; Kleiman, N.S.; Chetcuti, S.J.; Michelena, H.I.; Mangi, A.A.; Skiles, J.A.; et al. Transcatheter Aortic Valve Replacement in Low-Risk Patients With Bicuspid Aortic Valve Stenosis. JAMA Cardiol. 2021, 6, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.R.; Jilaihawi, H.; Makkar, R.; O’Neill, W.W.; Guyton, R.; Malaisrie, S.C.; Brown, D.L.; Blanke, P.; Leipsic, J.A.; Pibarot, P.; et al. The PARTNER 3 Bicuspid Registry for Transcatheter Aortic Valve Replacement in Low-Surgical-Risk Patients. JACC Cardiovasc. Interv. 2022, 15, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Vemulapalli, S.; Carroll, J.D.; Mack, M.J.; Li, Z.; Dai, D.; Kosinski, A.S.; Kumbhani, D.J.; Ruiz, C.E.; Thourani, V.H.; Hanzel, G.; et al. Procedural Volume and Outcomes for Transcatheter Aortic-Valve Replacement. N. Engl. J. Med. 2019, 380, 2541–2550. [Google Scholar] [CrossRef] [PubMed]
- Nuyens, P.; Wong, I.; Vanhaverbeke, M.; Wang, X.; Bieliauskas, G.; Sondergaard, L.; De Backer, O. Intravascular Lithotripsy-Assisted Transfemoral Transcatheter Aortic Valve Implantation. J. Vis. Exp. 2022, Mar 9, 181. [Google Scholar] [CrossRef]
- Masiero, G.; D’Angelo, L.; Fovino, L.N.; Fabris, T.; Cardaioli, F.; Rodinò, G.; Benedetti, A.; Boiago, M.; Continisio, S.; Montonati, C.; et al. Real-World Experience With a Large Bore Vascular Closure Device During TAVI Procedure: Features and Predictors of Access-Site Vascular Complications. Front. Cardiovasc. Med. 2022, 9, 832242. [Google Scholar] [CrossRef]
- Mitsis, A.; Eftychiou, C.; Eteokleous, N.; Papadopoulos, K.; Zittis, I.; Avraamides, P. Current Trends in TAVI Access. Curr. Probl. Cardiol. 2021, 46, 100844. [Google Scholar] [CrossRef]
- Uguz, E.; Gokcimen, M.; Ali, S.; Alsancak, Y.; Bastug, S.; Ahmet Kasapkara, H.; Canyigit, M.; Hıdıroglu, M.; Sener, E. Predictability and Outcome of Vascular Complications after Transfemoral Transcatheter Aortic Valve Implantation. J. Heart Valve Dis. 2016, 25, 173–181. [Google Scholar]
- Sinclair, N.; Mordhorst, A.; Yang, G.K.; MacDonald, P.S.; Sidhu, R.; Reid, J.D.S. Vascular Access Complications and Clinical Outcomes of Vascular Surgical Repairs Following Transcatheter Aortic Valve Implantation (TAVI). Ann. Vasc. Surg. 2021, 74, 258–263. [Google Scholar] [CrossRef]
- Barbanti, M.; Binder, R.K.; Freeman, M.; Wood, D.A.; Leipsic, J.; Cheung, A.; Ye, J.; Tan, J.; Toggweiler, S.; Yang, T.-H.; et al. Impact of Low-Profile Sheaths on Vascular Complications during Transfemoral Transcatheter Aortic Valve Replacement. EuroIntervention 2013, 9, 929–935. [Google Scholar] [CrossRef]
- Freeman, M.; Rodés-Cabau, J.; Urena, M.; DeLarochelliere, R.; Dumont, E.; Masson, J.-B.; Willson, A.B.; Binder, R.K.; Toggweiler, S.; Leipsic, J.; et al. First-in-Man Transfemoral Transcatheter Aortic Valve Replacement with the 29 Mm Edwards SAPIEN XT Valve. Catheter. Cardiovasc. Interv. 2013, 82, 664–670. [Google Scholar] [CrossRef]
- Glaser, N.; O’Sullivan, C.J.; Saleh, N.; Verouhis, D.; Settergren, M.; Linder, R.; Rück, A. Transcatheter Aortic Valve Replacement Using the ISleeve Expandable Sheath in Small Femoral Arteries. Open Heart 2021, 8, e001703. [Google Scholar] [CrossRef] [PubMed]
- Auffret, V.; Puri, R.; Urena, M.; Chamandi, C.; Rodriguez-Gabella, T.; Philippon, F.; Rodés-Cabau, J. Conduction Disturbances After Transcatheter Aortic Valve Replacement: Current Status and Future Perspectives. Circulation 2017, 136, 1049–1069. [Google Scholar] [CrossRef] [PubMed]
- Mitsis, A.; Eftychiou, C.; Christophides, T.; Sakellaropoulos, S.; Avraamides, P. The Conjunction Conundrum in Transcatheter Aortic Valve Implantation. Curr. Probl. Cardiol. 2022, 101130. [Google Scholar] [CrossRef] [PubMed]
- Bruno, F.; D’Ascenzo, F.; Vaira, M.P.; Elia, E.; Omedè, P.; Kodali, S.; Barbanti, M.; Rodès-Cabau, J.; Husser, O.; Sossalla, S.; et al. Predictors of Pacemaker Implantation after Transcatheter Aortic Valve Implantation According to Kind of Prosthesis and Risk Profile: A Systematic Review and Contemporary Meta-Analysis. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 143–153. [Google Scholar] [CrossRef]
- Wang, T.; Ou, A.; Xia, P.; Tian, J.; Wang, H.; Cheng, Z. Predictors for the Risk of Permanent Pacemaker Implantation after Transcatheter Aortic Valve Replacement: A Systematic Review and Meta-Analysis. J. Card. Surg. 2022, 37, 377–405. [Google Scholar] [CrossRef]
- Siontis, G.C.M.; Jüni, P.; Pilgrim, T.; Stortecky, S.; Büllesfeld, L.; Meier, B.; Wenaweser, P.; Windecker, S. Predictors of Permanent Pacemaker Implantation in Patients with Severe Aortic Stenosis Undergoing TAVR: A Meta-Analysis. J. Am. Coll. Cardiol. 2014, 64, 129–140. [Google Scholar] [CrossRef] [Green Version]
- Nazif, T.M.; Dizon, J.M.; Hahn, R.T.; Xu, K.; Babaliaros, V.; Douglas, P.S.; El-Chami, M.F.; Herrmann, H.C.; Mack, M.; Makkar, R.R.; et al. Predictors and Clinical Outcomes of Permanent Pacemaker Implantation after Transcatheter Aortic Valve Replacement: The PARTNER (Placement of AoRtic TraNscathetER Valves) Trial and Registry. JACC Cardiovasc. Interv. 2015, 8, 60–69. [Google Scholar] [CrossRef] [Green Version]
- Sathananthan, J.; Ding, L.; Yu, M.; Catlin, B.; Chan, A.; Charania, J.; Cheung, A.; Cook, R.; Murdoch, D.J.; Della Siega, A.; et al. Implications of Transcatheter Heart Valve Selection on Early and Late Pacemaker Rate and on Length of Stay. Can. J. Cardiol. 2018, 34, 1165–1173. [Google Scholar] [CrossRef]
- Vlastra, W.; Chandrasekhar, J.; Muñoz-Garcia, A.J.; Tchétché, D.; de Brito, F.S.; Barbanti, M.; Kornowski, R.; Latib, A.; D’Onofrio, A.; Ribichini, F.; et al. Comparison of Balloon-Expandable vs. Self-Expandable Valves in Patients Undergoing Transfemoral Transcatheter Aortic Valve Implantation: From the CENTER-Collaboration. Eur. Heart J. 2019, 40, 456–465. [Google Scholar] [CrossRef]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef]
- Santos-Martinez, S.; Halim, J.; Castro-Mejía, A.; De Marco, F.; Trani, C.; Martin, P.; Infusino, F.; Ancona, M.; Moreno, R.; den Heijer, P.; et al. Myval versus Alternative Balloon- and Self-Expandable Transcatheter Heart Valves: A Central Core Lab Analysis of Conduction Disturbances. Int. J. Cardiol. 2022, 351, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Van Belle, E.; Vincent, F.; Labreuche, J.; Auffret, V.; Debry, N.; Lefèvre, T.; Eltchaninoff, H.; Manigold, T.; Gilard, M.; Verhoye, J.-P.; et al. Balloon-Expandable Versus Self-Expanding Transcatheter Aortic Valve Replacement: A Propensity-Matched Comparison From the FRANCE-TAVI Registry. Circulation 2020, 141, 243–259. [Google Scholar] [CrossRef] [PubMed]
- Deharo, P.; Bisson, A.; Herbert, J.; Lacour, T.; Saint Etienne, C.; Grammatico-Guillon, L.; Porto, A.; Collart, F.; Bourguignon, T.; Cuisset, T.; et al. Impact of Sapien 3 Balloon-Expandable Versus Evolut R Self-Expandable Transcatheter Aortic Valve Implantation in Patients With Aortic Stenosis: Data From a Nationwide Analysis. Circulation 2020, 141, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Alperi, A.; Muntané-Carol, G.; Freitas-Ferraz, A.B.; Junquera, L.; Del Val, D.; Faroux, L.; Philippon, F.; Rodés-Cabau, J. Overcoming the Transcatheter Aortic Valve Replacement Achilles Heel: Conduction Abnormalities-a Systematic Review. Ann. Cardiothorac. Surg. 2020, 9, 429–441. [Google Scholar] [CrossRef]
- van Rosendael, P.J.; Delgado, V.; Bax, J.J. Pacemaker Implantation Rate after Transcatheter Aortic Valve Implantation with Early and New-Generation Devices: A Systematic Review. Eur. Heart J. 2018, 39, 2003–2013. [Google Scholar] [CrossRef]
- Tamburino, C.; Bleiziffer, S.; Thiele, H.; Scholtz, S.; Hildick-Smith, D.; Cunnington, M.; Wolf, A.; Barbanti, M.; Tchetchè, D.; Garot, P.; et al. Comparison of Self-Expanding Bioprostheses for Transcatheter Aortic Valve Replacement in Patients With Symptomatic Severe Aortic Stenosis: SCOPE 2 Randomized Clinical Trial. Circulation 2020, 142, 2431–2442. [Google Scholar] [CrossRef]
- Kim, W.-K.; Thiele, H.; Linke, A.; Kuntze, T.; Fichtlscherer, S.; Webb, J.; Chu, M.W.A.; Adam, M.; Schymik, G.; Geisler, T.; et al. Transcatheter Aortic Valve Implantation with ACURATE Neo: Results from the PROGRESS PVL Registry. J. Interv. Cardiol. 2022, 2022, 9138403. [Google Scholar] [CrossRef]
- Choudhury, T.; Solomonica, A.; Bagur, R. The ACURATE Neo Transcatheter Aortic Valve System. Expert Rev. Med. Devices 2018, 15, 693–699. [Google Scholar] [CrossRef]
- Lefèvre, T.; Kappetein, A.P.; Wolner, E.; Nataf, P.; Thomas, M.; Schächinger, V.; De Bruyne, B.; Eltchaninoff, H.; Thielmann, M.; Himbert, D.; et al. One Year Follow-up of the Multi-Centre European PARTNER Transcatheter Heart Valve Study. Eur. Heart J. 2011, 32, 148–157. [Google Scholar] [CrossRef] [Green Version]
- Keller, L.S.; Panagides, V.; Mesnier, J.; Nuche, J.; Rodés-Cabau, J. Percutaneous Coronary Intervention Pre-TAVR: Current State of the Evidence. Curr. Cardiol. Rep. 2022, 24, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, T.; Chakravarty, T.; Yoon, S.-H.; Kaewkes, D.; Flint, N.; Patel, V.; Mahani, S.; Tiwana, R.; Sekhon, N.; Nakamura, M.; et al. Coronary Access After TAVR. JACC Cardiovasc. Interv. 2020, 13, 693–705. [Google Scholar] [CrossRef] [PubMed]
- Yudi, M.B.; Sharma, S.K.; Tang, G.H.L.; Kini, A. Coronary Angiography and Percutaneous Coronary Intervention After Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2018, 71, 1360–1378. [Google Scholar] [CrossRef]
- Blumenstein, J.; Kim, W.-K.; Liebetrau, C.; Gaede, L.; Kempfert, J.; Walther, T.; Hamm, C.; Möllmann, H. Challenges of Coronary Angiography and Intervention in Patients Previously Treated by TAVI. Clin. Res. Cardiol. 2015, 104, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, M.; Costa, G.; Picci, A.; Criscione, E.; Reddavid, C.; Valvo, R.; Todaro, D.; Deste, W.; Condorelli, A.; Scalia, M.; et al. Coronary Cannulation After Transcatheter Aortic Valve Replacement: The RE-ACCESS Study. JACC Cardiovasc. Interv. 2020, 13, 2542–2555. [Google Scholar] [CrossRef] [PubMed]
- Bieliauskas, G.; Wong, I.; Bajoras, V.; Wang, X.; Kofoed, K.F.; De Backer, O.; Søndergaard, L. Patient-Specific Implantation Technique to Obtain Neo-Commissural Alignment With Self-Expanding Transcatheter Aortic Valves. JACC Cardiovasc. Interv. 2021, 14, 2097–2108. [Google Scholar] [CrossRef]
- Kitamura, M.; Wilde, J.; Gohmann, R.; Majunke, N.; Gutberlet, M.; Shibata, M.; Kiefer, P.; Desch, S.; Thiele, H.; Holzhey, D.; et al. Commissural Alignment of the ACURATE Neo Valve in Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2021, 14, 1740–1742. [Google Scholar] [CrossRef]
- Tang, G.H.L.; Zaid, S.; Fuchs, A.; Yamabe, T.; Yazdchi, F.; Gupta, E.; Ahmad, H.; Kofoed, K.F.; Goldberg, J.B.; Undemir, C.; et al. Alignment of Transcatheter Aortic-Valve Neo-Commissures (ALIGN TAVR): Impact on Final Valve Orientation and Coronary Artery Overlap. JACC Cardiovasc. Interv. 2020, 13, 1030–1042. [Google Scholar] [CrossRef]
- Tarantini, G.; Nai Fovino, L.; Scotti, A.; Massussi, M.; Cardaioli, F.; Rodinò, G.; Benedetti, A.; Boiago, M.; Matsuda, Y.; Continisio, S.; et al. Coronary Access After Transcatheter Aortic Valve Replacement With Commissural Alignment: The ALIGN-ACCESS Study. Circ. Cardiovasc. Interv. 2022, 15, e011045. [Google Scholar] [CrossRef]
- Vrachatis, D.A.; Vavuranakis, M.; Tsoukala, S.; Giotaki, S.; Papaioannou, T.G.; Siasos, G.; Deftereos, G.; Giannopoulos, G.; Raisakis, K.; Tousoulis, D.; et al. TAVI: Valve in Valve. A New Field for Structuralists? Literature Review. Hellenic. J. Cardiol. 2020, 61, 148–153. [Google Scholar] [CrossRef]
- Tang, G.H.L.; Zaid, S.; Gupta, E.; Ahmad, H.; Khan, A.; Kovacic, J.C.; Lansman, S.L.; Dangas, G.D.; Sharma, S.K.; Kini, A. Feasibility of Repeat TAVR After SAPIEN 3 TAVR: A Novel Classification Scheme and Pilot Angiographic Study. JACC Cardiovasc. Interv. 2019, 12, 1290–1292. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, I.; Mackensen, G.B.; Aldea, G.S.; Reisman, M.; Dvir, D. Bioprosthetic or Native Aortic Scallop Intentional Laceration to Prevent Iatrogenic Coronary Artery Obstruction. Part 2: How to Perform BASILICA. EuroIntervention 2019, 15, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Percy, E.D.; Harloff, M.T.; Hirji, S.; McGurk, S.; Yazdchi, F.; Newell, P.; Malarczyk, A.; Sabe, A.; Landes, U.; Webb, J.; et al. Nationally Representative Repeat Transcatheter Aortic Valve Replacement Outcomes: Report From the Centers for Medicare and Medicaid Services. JACC Cardiovasc. Interv. 2021, 14, 1717–1726. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.M.; Dvir, D.; Greenbaum, A.B.; Babaliaros, V.C.; Rogers, T.; Aldea, G.; Reisman, M.; Mackensen, G.B.; Eng, M.H.K.; Paone, G.; et al. Transcatheter Laceration of Aortic Leaflets to Prevent Coronary Obstruction During Transcatheter Aortic Valve Replacement: Concept to First-in-Human. JACC Cardiovasc. Interv. 2018, 11, 677–689. [Google Scholar] [CrossRef] [PubMed]
- Romano, V.; Buzzatti, N.; Latib, A.; Colombo, A.; Montorfano, M. Chimney Technique for Coronary Obstruction after Aortic Valve in Valve: Pros and Cons. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1194. [Google Scholar] [CrossRef]
- Medranda, G.A.; Soria Jimenez, C.E.; Torguson, R.; Case, B.C.; Forrestal, B.J.; Ali, S.W.; Shea, C.; Zhang, C.; Wang, J.C.; Gordon, P.; et al. Lifetime Management of Patients with Symptomatic Severe Aortic Stenosis: A Computed Tomography Simulation Study. EuroIntervention 2022, 18, e407–e416. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| THV | Frame Material | Leaflet Material | Supraannular or Intraannular | Repositionability | Retrievability | Available Valve Sizes Based on the Correspondence Aortic Valve Area (in mm2) for BEVs or Aortic Perimeter (in mm) for SEVs | Available Sheath Sizes | Delivery Routes | Approval |
|---|---|---|---|---|---|---|---|---|---|
| BEVs | |||||||||
| Sapien 3 | Cobalt-chromium | Bovine pericardium | Intraannular | No | No | 20 (273–345 mm2), 23 (338–430 mm2), 26 (430–546 mm2), 29 (540–680 mm2) | 14 F (20, 23, 26 mm), 16F (29 mm) | TF, TA, TAo | FDA, CE Mark |
| Sapien 3 Ultra | Cobalt-chromium | Bovine pericardium | Intraannular | No | No | 20 (273–345 mm2), 23 (338–430 mm2), 26 (430–546 mm2), 29 (540–680 mm2) | 14 F | TF, TA | FDA, CE Mark |
| Myval | Nickel-cobalt | Bovine pericardium | Intraannular | No | No | 20 (270–330 mm2), 21.5 (314–380 mm2), 23 (360–440 mm2), 24.5 (410–500 mm2), 26 (460–560 mm2), 27.5 (510–630 mm2), 29 (570–700 mm2) 30.5 (630–770 mm2), 32 (700–840 mm2) | 14 F | TF | CE Mark |
| SEVs | |||||||||
| Evolut PRO | Nitinol | Porcine pericardium | Supraannular | Yes | Yes | 23 (56.5–62.8 mm), 26 (62.8–72.3 mm), 29 (72.3–81.7 mm), 34 (81.7–94.2 mm) | 16 F | TF, TAo, SC | FDA, CE Mark |
| Evolut PRO + | Nitinol | Porcine pericardium | Supraannular | Yes | Yes | 23 26, 29, 34 | 14 F (23, 26, 29 mm), 16F (34 mm) | TF, TAo, SC | FDA, CE Mark |
| ACURATE neo2 | Nitinol | Porcine pericardium | Supraannular | No | No | Small (66–72 mm), Medium (72–79 mm), Large (79–85 mm) | 14 F | TF, TA | CE Mark |
| Portico | Nitinol | Bovine pericardium | Intraannular | Yes | Yes | 23 (60–66 mm), 25 (66–73 mm), 27 (72–79 mm), 29 (79–85 mm) | 18 F (23, 25 mm), 19 F (27, 29 mm) | TF, TAo, TAx, SC | CE Mark |
| Navitor | Nitinol | Bovine pericardium | Intraannular | Yes | Yes | 23 (60–66 mm), 25 (66–73 mm), 27 (72–79 mm), 29 (79–85 mm) | 14 F (23, 25 mm), 15 F (27, 29 mm) | TF, TAo, TAx, SC | CE Mark |
| Scenario | Risk | Recommended | Valve |
|---|---|---|---|
| BEV | SEV | ||
| Anatomic Characteristics | |||
| Severely calcified annulus | Elevated risk for annulus rupture, PVL, or stroke | √ | |
| Horizontal Aorta | Difficult delivery and precise positioning of the valve | √ | |
| Small annulus size | Elevated risk for PPM and annulus rupture | √ | |
| Large annulus size | Limited commercially available options | √ | |
| Bicuspid Aortic Valve | Difficult sizing and higher risk of annulus rupture and PVL | √ | √ |
| Limited transfemoral access | Elevated risk for vascular complications | √ | |
| Clinical characteristics | |||
| Pre-existing risk factors for conduction abnormalities | High risk for post-procedural permanent pacing | √ | |
| Concomitant Coronary Artery Disease | Future need for coronary engagement | √ | |
| Grater Life-expectancy | Possible need for aortic valve re-intervention (TAVI-in-TAVI) | √ | |
| Patients with reduced ejection fraction of the left ventricle | Poor tolerance to rapid pacing | √ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitsis, A.; Yuan, X.; Eftychiou, C.; Avraamides, P.; Nienaber, C.A. Personalised Treatment in Aortic Stenosis: A Patient-Tailored Transcatheter Aortic Valve Implantation Approach. J. Cardiovasc. Dev. Dis. 2022, 9, 407. https://doi.org/10.3390/jcdd9110407
Mitsis A, Yuan X, Eftychiou C, Avraamides P, Nienaber CA. Personalised Treatment in Aortic Stenosis: A Patient-Tailored Transcatheter Aortic Valve Implantation Approach. Journal of Cardiovascular Development and Disease. 2022; 9(11):407. https://doi.org/10.3390/jcdd9110407
Chicago/Turabian StyleMitsis, Andreas, Xun Yuan, Christos Eftychiou, Panayiotis Avraamides, and Christoph A. Nienaber. 2022. "Personalised Treatment in Aortic Stenosis: A Patient-Tailored Transcatheter Aortic Valve Implantation Approach" Journal of Cardiovascular Development and Disease 9, no. 11: 407. https://doi.org/10.3390/jcdd9110407