
Association between Abnormal Echocardiography and Adverse Obstetric Outcomes in Low-Risk Pregnant Women
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- UNICEF. UNICEF Data Maternal Mortality. Available online: https://data.unicef.org/topic/maternal-health/maternal-mortality/ (accessed on 24 April 2022).
- Mehta, L.S.; Warnes, C.A.; Bradley, E.; Burton, T.; Economy, K.; Mehran, R.; Safdar, B.; Sharma, G.; Wood, M.; Valente, A.M.; et al. Cardiovascular Considerations in Caring for Pregnant Patients: A Scientific Statement from the American Heart Association. Circulation 2020, 141, e884–e903. [Google Scholar] [CrossRef] [PubMed]
- Luke, A.A.; Huang, K.; Lindley, K.J.; Carter, E.B.; Joynt Maddox, K.E.J. Severe Maternal Morbidity, Race, and Rurality: Trends Using the National Inpatient Sample, 2012–2017. J. Women’s Health 2021, 30, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, W.M. Overview of Maternal Mortality in the United States. Semin. Perinatol. 2012, 36, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Drenthen, W.; Boersma, E.; Balci, A.; Moons, P.; Roos-Hesselink, J.W.; Mulder, B.J.; Vliegen, H.W.; van Dijk, A.P.; Voors, A.A.; Yap, S.C.; et al. Predictors of pregnancy complications in women with congenital heart disease. Eur. Heart J. 2010, 31, 2124–2132. [Google Scholar] [CrossRef] [Green Version]
- Regitz-Zagrosek, V.; Lundqvist, C.B.; Borghi, C.; Cifkova, R.; Ferreira, R.; Foidart, J.-M.; Gibbs, J.S.R.; Gohlke-Baerwolf, C.; Gorenek, B.; Iung, B.; et al. ESC Guidelines on the management of cardiovascular diseases during pregnancy: The Task Force on the Management of Cardiovascular Diseases during Pregnancy of the European Society of Cardiology (ESC). Eur. Heart J. 2011, 32, 3147–3197. [Google Scholar] [CrossRef] [Green Version]
- Silversides, C.K.; Grewal, J.; Mason, J.; Sermer, M.; Kiess, M.; Rychel, V.; Wald, R.M.; Colman, J.M.; Siu, S.C. Pregnancy Outcomes in Women with Heart Disease: The CARPREG II Study. J. Am. Coll. Cardiol. 2018, 71, 2419–2430. [Google Scholar] [CrossRef]
- Goya, M.; Casellas, M.; Merced, C.; Pijuan-Domenech, A.; Galián, L.; Dos, L.; Casaldáliga, J.; Subirana, M.; Pedrosa, V.; Rojas, M.; et al. Predictors of obstetric complications in women with heart disease. J. Matern. Fetal Neonatal Med. 2016, 29, 2306–2311. [Google Scholar] [CrossRef]
- van Hagen, I.M.; Roos-Hesselink, J.W.; Donvito, V.; Liptai, C.; Morissens, M.; Murphy, D.J.; Galian, L.; Bazargani, N.M.; Cornette, J.; Hall, R.; et al. Incidence and predictors of obstetric and fetal complications in women with structural heart disease. Heart 2017, 103, 1610–1618. [Google Scholar] [CrossRef]
- Wu, P.; Chew-Graham, C.A.; Maas, A.H.; Chappell, L.C.; Potts, J.E.; Gulati, M.; Jordan, K.P.; Mamas, M.A. Temporal Changes in Hypertensive Disorders of Pregnancy and Impact on Cardiovascular and Obstetric Outcomes. Am. J. Cardiol. 2020, 125, 1508–1516. [Google Scholar] [CrossRef]
- Wu, P.; Chew-Graham, C.; Maas, A.; Chappell, L.; Potts, J.; Gulati, M.; Jordan, K.; Mamas, M. Hypertensive disorders of pregnancy and impact on in-hospital cardio-obstetric outcomes. Eur. Heart J. 2020, 41, ehaa946-3306. [Google Scholar] [CrossRef]
- Wang, Y.; Shi, H.; Chen, L.; Zheng, D.; Long, X.; Zhang, Y.; Wang, H.; Shi, Y.; Zhao, Y.; Wei, Y.; et al. Absolute Risk of Adverse Obstetric Outcomes Among Twin Pregnancies After In Vitro Fertilization by Maternal Age. JAMA Netw. Open 2021, 4, e2123634. [Google Scholar] [CrossRef] [PubMed]
- Cedergren, M.I. Maternal Morbid Obesity and the Risk of Adverse Pregnancy Outcome. Obstet. Gynecol. 2004, 103, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Cleary-Goldman, J.; Malone, F.D.; Vidaver, J.; Ball, R.H.; Nyberg, D.A.; Comstock, C.H.; Saade, G.R.; Eddleman, K.A.; Klugman, S.; Dugoff, L.; et al. Impact of Maternal Age on Obstetric Outcome. Obstet. Gynecol. 2005, 105, 983–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American College of Obstetricians and Gynecologists’ Presidential Task Force on Pregnancy and Heart Disease and Committee on Practice Bulletins—Obstetrics. ACOG practice bulletin no. 212: Pregnancy and heart disease. Obstet. Gynecol. 2019, 133, e320–e356. [Google Scholar] [CrossRef] [PubMed]
- Schnettler, W.T.; Zinn, C.K.; Devaiah, C.G.; Wilson, J. Indications for Maternal Echocardiography in Detecting Disease and the Impact on Pregnancy Management. Am. J. Perinatol. 2021. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [Green Version]
- Zoghbi, W.A.; Chambers, J.B.; Dumesnil, J.G.; Foster, E.; Gottdiener, J.S.; Grayburn, P.A.; Khandheria, B.K.; Levine, R.A.; Marx, G.R.; Miller, F.A.; et al. Recommendations for evaluation of prosthetic valves with echocardiography and doppler ultrasound: A report From the American Society of Echocardiography’s Guidelines and Standards Committee and the Task Force on Prosthetic Valves, developed in conjunction with the American College of Cardiology Cardiovascular Imaging Committee, Cardiac Imaging Committee of the American Heart Association, the European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography and the Canadian Society of Echocardiography, endorsed by the American College of Cardiology Foundation, American Heart Association, European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography, and Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2009, 22, 975–1014. [Google Scholar]
- Zoghbi, W.A.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Kraft, C.D.; Levine, R.A.; Nihoyannopoulos, P.; Otto, C.M.; Quinones, M.A.; Rakowski, H.; et al. American Society of Echocardiography. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J. Am. Soc. Echocardiogr. 2003, 16, 777–802. [Google Scholar] [CrossRef]
- Dharmarajan, L.; Hale, T.M.; Velastegui, Z.; Castillo, E.; Kanna, B. Utility of two-dimensional echocardiography in pregnancy and post-partum period and impact on management in an inner city hospital. J. Périnat. Med. 2009, 37, 663–668. [Google Scholar] [CrossRef]
- Hopkins, M.K.; Levine, L.D.; Koelper, N.C.; Durnwald, C. Screening Echocardiogram in High-Risk Women with Class III Obesity to Predict the Risk of Preeclampsia. Am. J. Perinatol. 2021, 39, 457–463. [Google Scholar] [CrossRef]
- Penning, S.; Robinson, K.D.; Major, C.A.; Garite, T.J. A comparison of echocardiography and pulmonary artery catheterization for evaluation of pulmonary artery pressures in pregnant patients with suspected pulmonary hypertension. Am. J. Obstet. Gynecol. 2001, 184, 1568–1570. [Google Scholar] [CrossRef] [PubMed]
- Bello, N.A.; Bairey Merz, C.N.; Brown, H.; Davis, M.B.; Dickert, N.W.; El Hajj, S.C.; Giullian, C.; Quesada, O.; Park, K.; Sanghani, R.M.; et al. Diagnostic Cardiovascular Imaging and Therapeutic Strategies in Pregnancy: JACC Focus Seminar 4/5. J. Am. Coll. Cardiol. 2021, 77, 1813–1822. [Google Scholar] [CrossRef] [PubMed]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [PubMed]
- Laughon, S.K.; Albert, P.S.; Leishear, K.; Mendola, P. The NICHD Consecutive Pregnancies Study: Recurrent preterm delivery by subtype. Am. J. Obstet. Gynecol. 2013, 210, 131.e1–131.e8. [Google Scholar] [CrossRef] [Green Version]
- Tita, A.T.N.; Lai, Y.; Landon, M.B.; Spong, C.Y.; Leveno, K.J.; Varner, M.; Caritis, S.; Meis, P.J.; Wapner, R.J.; Sorokin, Y.; et al. Timing of Elective Repeat Cesarean Delivery at Term and Maternal Perioperative Outcomes. Obstet. Gynecol. 2011, 117, 280–286. [Google Scholar] [CrossRef] [Green Version]
- Clark, S.L.; Miller, D.D.; Belfort, M.A.; Dildy, G.; Frye, D.K.; Meyers, J.A. Neonatal and maternal outcomes associated with elective term delivery. Am. J. Obstet. Gynecol. 2009, 200, 156.e1–156.e4. [Google Scholar] [CrossRef]
- Spong, C.Y.; Mercer, B.M.; D’Alton, M.; Kilpatrick, S.; Blackwell, S.; Saade, G. Timing of Indicated Late-Preterm and Early-Term Birth. Obstet. Gynecol. 2011, 118, 323–333. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable, No. (%) | ||
| N | 195 | |
| Twin gestation | 4 | (2) |
| Parity status | ||
| Nulliparous | 66 | (34) |
| Primiparous | 60 | (31) |
| Parity of 2 to 5 | 56 | (29) |
| Grand Multipara | 5 | (3) |
| Unknown | 8 | (4) |
| Race | ||
| African American | 79 | (41) |
| Multi-racial | 60 | (31) |
| White | 16 | (8) |
| Asian | 2 | (1) |
| Unidentified | 33 | (17) |
| Age, y | ||
| <20 | 6 | (3) |
| 20–24 | 34 | (18) |
| 25 to 29 | 55 | (28) |
| 30 to 34 | 46 | (24) |
| 35 to 39 | 39 | (20) |
| ≥40 | 15 | (8) |
| Obesity | ||
| Not obese | 87 | (45) |
| Class I | 44 | (23) |
| Class II | 28 | (14) |
| Class III | 29 | (15) |
| Unknown | 7 | (4) |
| Comorbidities | ||
| Arrhythmia | 5 | (3) |
| Hypertension | 34 | (17) |
| Diabetes | 23 | (12) |
| Anemia | 16 | (8) |
| Sickle Cell Disease | 10 | (5) |
| Connective Tissue Disease | 14 | (7) |
| HIV * | 6 | (3) |
| Pulmonary Embolism | 6 | (3) |
| Cerebrovascular Event | 3 | (2) |
| Gestational Age | ||
| 1st Trimester | 13 | (7) |
| 2nd Trimester | 108 | (55) |
| 3rd Trimester | 71 | (36) |
| Unknown | 3 | (2) |
| Population Total | Normal Echocardiogram | Abnormal Echocardiogram | p Value | ||||
|---|---|---|---|---|---|---|---|
| Variable, No. (%) | |||||||
| N | 195 | 174 | 21 | ||||
| Indication for Echocardiogram | |||||||
| Shortness of breath | 40 | (21) | 37 | (21) | 3 | (14) | 0.45 |
| Syncope | 18 | (9) | 17 | (10) | 1 | (5) | 0.56 |
| Chest pain | 10 | (5) | 9 | (5) | 1 | (5) | 0.94 |
| Palpitations | 23 | (12) | 22 | (13) | 1 | (5) | 0.29 |
| Murmur | 44 | (23) | 39 | (22) | 5 | (24) | 0.89 |
| Abnormal ECG or arrhythmia | 19 | (10) | 19 | (11) | 0 | (0) | |
| History of HTN * | 12 | (6) | 5 | (3) | 7 | (33) | <0.01 |
| History cardiac disease or pHTN + | 15 | (8) | 13 | (7) | 2 | (10) | 0.74 |
| Suspected cardiac disease or pHTN + | 12 | (6) | 11 | (6) | 1 | (5) | 0.78 |
| Twin pregnancy | 1 | (1) | 1 | (1) | 0 | (0) | |
| Unknown | 1 | (1) | 1 | (1) | 0 | (0) | |
| Variable, No. (%) | ||
| Total Abnormal | 21 | (11) |
| Abnormal Findings (% of Total Abnormal) | ||
| Pulmonary artery systolic pressure ≥ 40 mmHg | 10 | (48) |
| Left ventricular regional wall motion abnormality | 3 | (14) |
| Left ventricular diastolic dysfunction (impaired relaxation) | 2 | (10) |
| Right ventricular systolic dysfunction | 3 | (14) |
| Left ventricular hypertrophy (>1.2 cm thickness) | 2 | (10) |
| Valve disease (more than mild mitral regurgitation, any stenosis) | 3 | (14) |
| Left atrial dilatation (more than mild) | 3 | (14) |
| Normal Echocardiogram | Abnormal Echocardiogram | p Value | |||
|---|---|---|---|---|---|
| Variable, No. (%) | |||||
| N | 174 | 21 | |||
| Twin gestation | 4 | 0 | |||
| Parity status | <0.01 | ||||
| Nulliparous | 60 | (34) | 6 | (29) | |
| Primiparous | 54 | (31) | 6 | (29) | |
| Parity of 2 to 5 | 51 | (29) | 5 | (24) | |
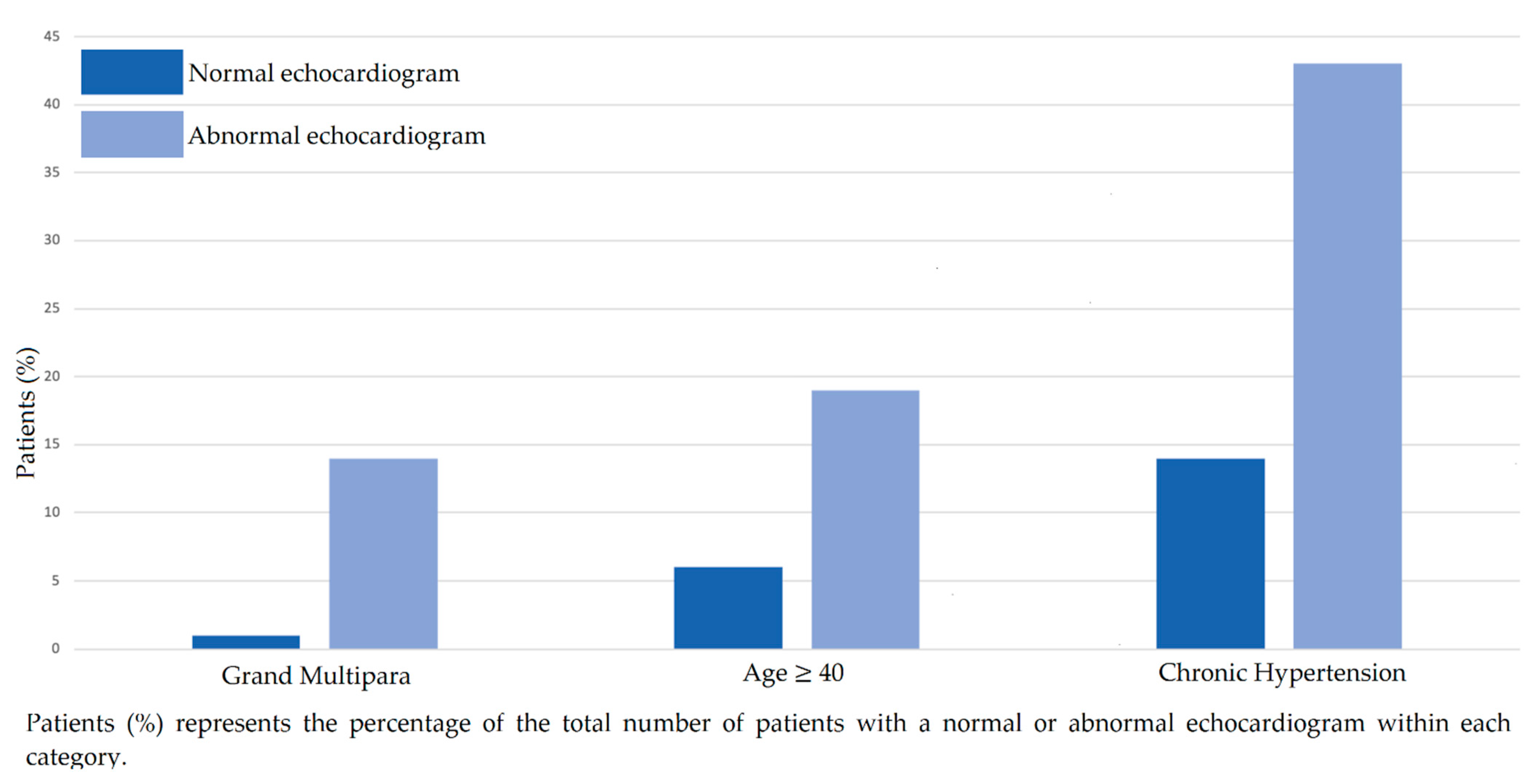
| Grand Multipara | 2 | (1) | 3 | (14) | |
| Unknown | 7 | (4) | 1 | (5) | |
| Race | |||||
| African American | 68 | (39) | 11 | (52) | 0.24 |
| Multi-racial | 57 | (33) | 5 | (24) | 0.41 |
| White | 14 | (8) | 2 | (10) | 0.82 |
| Asian | 2 | (1) | 0 | (0) | |
| Unidentified | 33 | (19) | 3 | (14) | |
| Age, y | 0.04 | ||||
| <20 | 6 | (3) | 0 | (0) | |
| 20–24 | 28 | (16) | 6 | (29) | |
| 25 to 29 | 53 | (30) | 2 | (10) | |
| 30 to 34 | 43 | (25) | 3 | (14) | |
| 35 to 39 | 33 | (19) | 6 | (29) | |
| ≥40 | 11 | (6) | 4 | (19) | |
| Obesity | 0.09 | ||||
| Not obese | 79 | (45) | 8 | (38) | |
| Class I | 43 | (25) | 1 | (5) | |
| Class II | 23 | (13) | 5 | (24) | |
| Class III | 24 | (14) | 5 | (24) | |
| Unknown | 5 | (3) | 2 | (10) | |
| Comorbidities | |||||
| Arrhythmia | 4 | (2) | 0 | (0) | |
| Hypertension | 25 | (14) | 9 | (43) | <0.01 |
| Diabetes | 19 | (11) | 4 | (19) | 0.28 |
| Anemia | 14 | (8) | 2 | (10) | 0.82 |
| Sickle Cell Disease | 10 | (6) | 3 | (14) | 0.14 |
| Connective Tissue Disease | 11 | (6) | 3 | (14) | 0.18 |
| HIV * | 5 | (3) | 1 | (5) | 0.64 |
| Pulmonary Embolism | 6 | (3) | 0 | (0) | |
| Cerebrovascular Event | 2 | (1) | 1 | (5) | 0.20 |
| Gestational Age | 0.60 | ||||
| 1st Trimester | 13 | (7) | 0 | (0) | |
| 2nd Trimester | 97 | (56) | 11 | (52) | |
| 3rd Trimester | 62 | (36) | 9 | (43) | |
| Unknown | 2 | (1) | 1 | (5) | |
| Population Total | Normal Echocardiogram | Abnormal Echocardiogram | p Value | ||||
|---|---|---|---|---|---|---|---|
| Variable, No. (%) | |||||||
| N | 195 | 174 | 21 | ||||
| Outcome of Delivery | |||||||
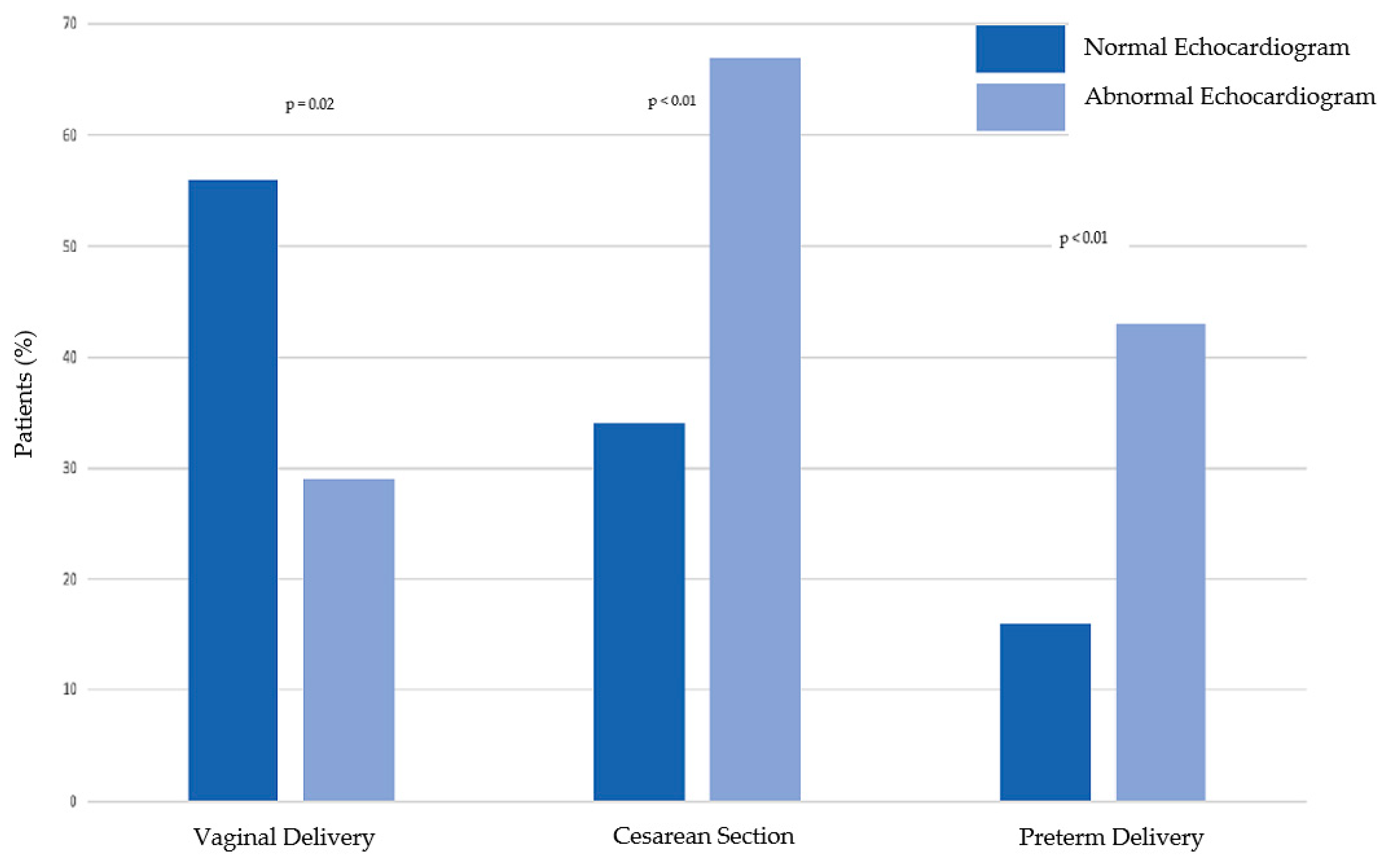
| Vaginal Delivery | 104 | (53) | 98 | (56) | 6 | (29) | 0.02 |
| Cesarean Section | 74 | (38) | 60 | (34) | 14 | (67) | <0.01 |
| Pregnancy Outcomes | |||||||
| Preterm Delivery | 37 | (19) | 27 | (16) | 9 | (43) | <0.01 |
| Spontaneous Abortion | 2 | (1) | 2 | (1) | 0 | (0) | |
| Intra-Uterine Fetal Demise | 2 | (1) | 2 | (1) | 0 | (0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hennessey, K.C.; Ali, T.S.; Choi, E.; Ortengren, A.R.; Hickerson, L.C.; Lee, J.M.; Taub, C.C. Association between Abnormal Echocardiography and Adverse Obstetric Outcomes in Low-Risk Pregnant Women. J. Cardiovasc. Dev. Dis. 2022, 9, 394. https://doi.org/10.3390/jcdd9110394
Hennessey KC, Ali TS, Choi E, Ortengren AR, Hickerson LC, Lee JM, Taub CC. Association between Abnormal Echocardiography and Adverse Obstetric Outcomes in Low-Risk Pregnant Women. Journal of Cardiovascular Development and Disease. 2022; 9(11):394. https://doi.org/10.3390/jcdd9110394
Chicago/Turabian StyleHennessey, Kerrilynn C., Thara S. Ali, Eunjung Choi, Alexandra R. Ortengren, Leigh C. Hickerson, Jennifer May Lee, and Cynthia C. Taub. 2022. "Association between Abnormal Echocardiography and Adverse Obstetric Outcomes in Low-Risk Pregnant Women" Journal of Cardiovascular Development and Disease 9, no. 11: 394. https://doi.org/10.3390/jcdd9110394