
Implantable Cardioverter Defibrillator Tachycardia Therapies: Past, Present and Future Directions

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. A Brief History of the Implantable Defibrillator
2. Supporting Evidence for ICD Use
2.1. Secondary Prevention
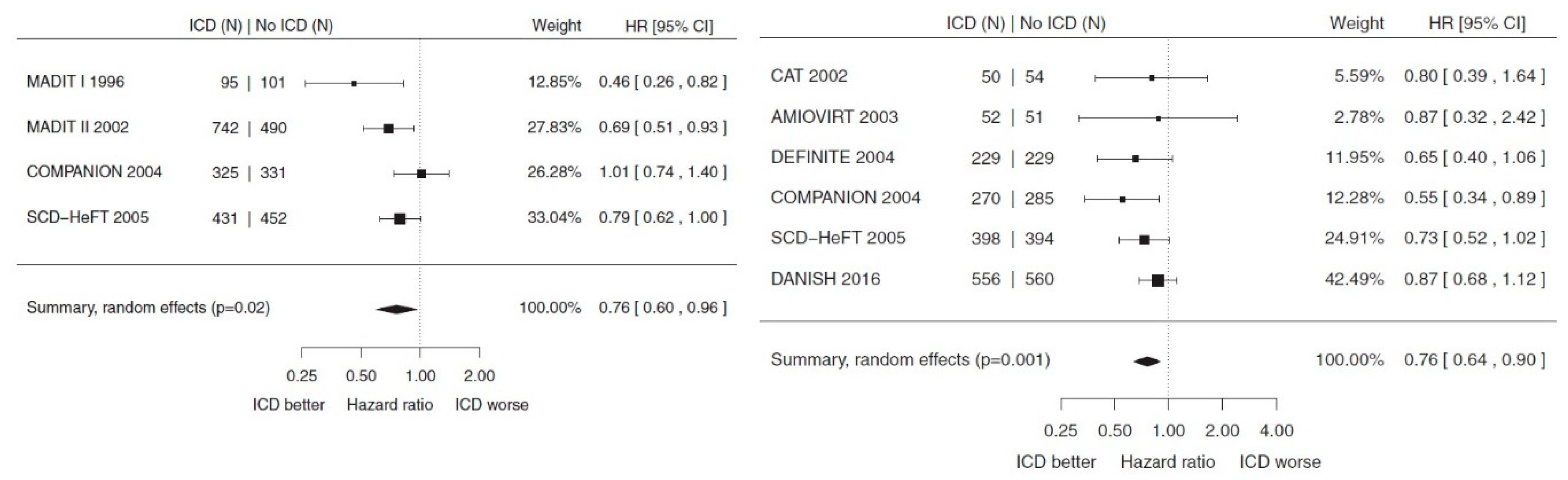
2.2. Primary Prevention in Ischaemic Cardiomyopathy (ICMP)
2.3. Primary Prevention in Non-Ischaemic Cardiomyopathy (NICMP)
2.4. ICD Use in Other Clinical Settings
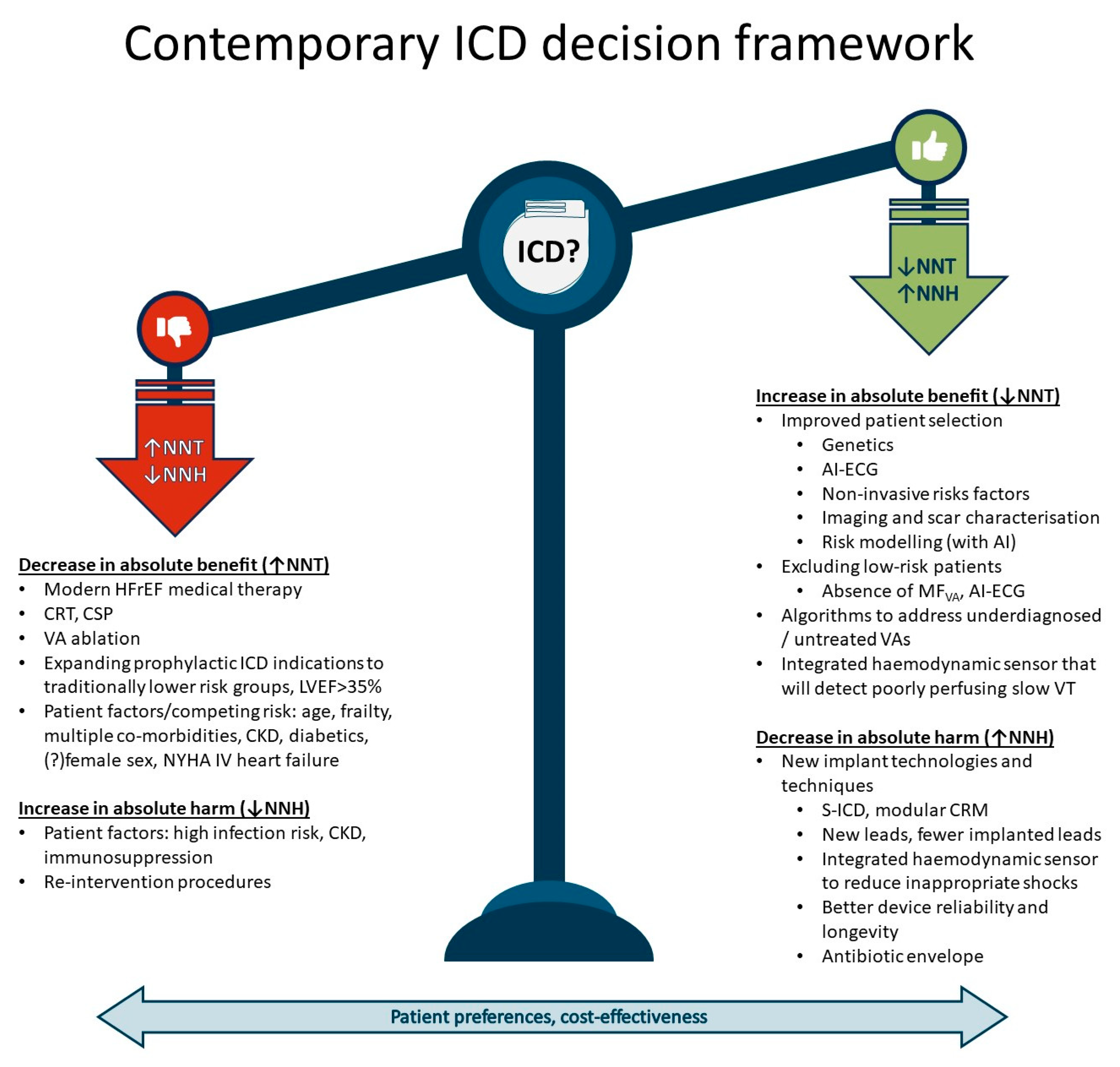
3. Risk vs. Benefit of ICDs
3.1. Patient Selection
3.2. Competing Risk
3.3. Contemporary HFrEF Therapy
4. ICD Cost Reduction
4.1. Shock Reduction
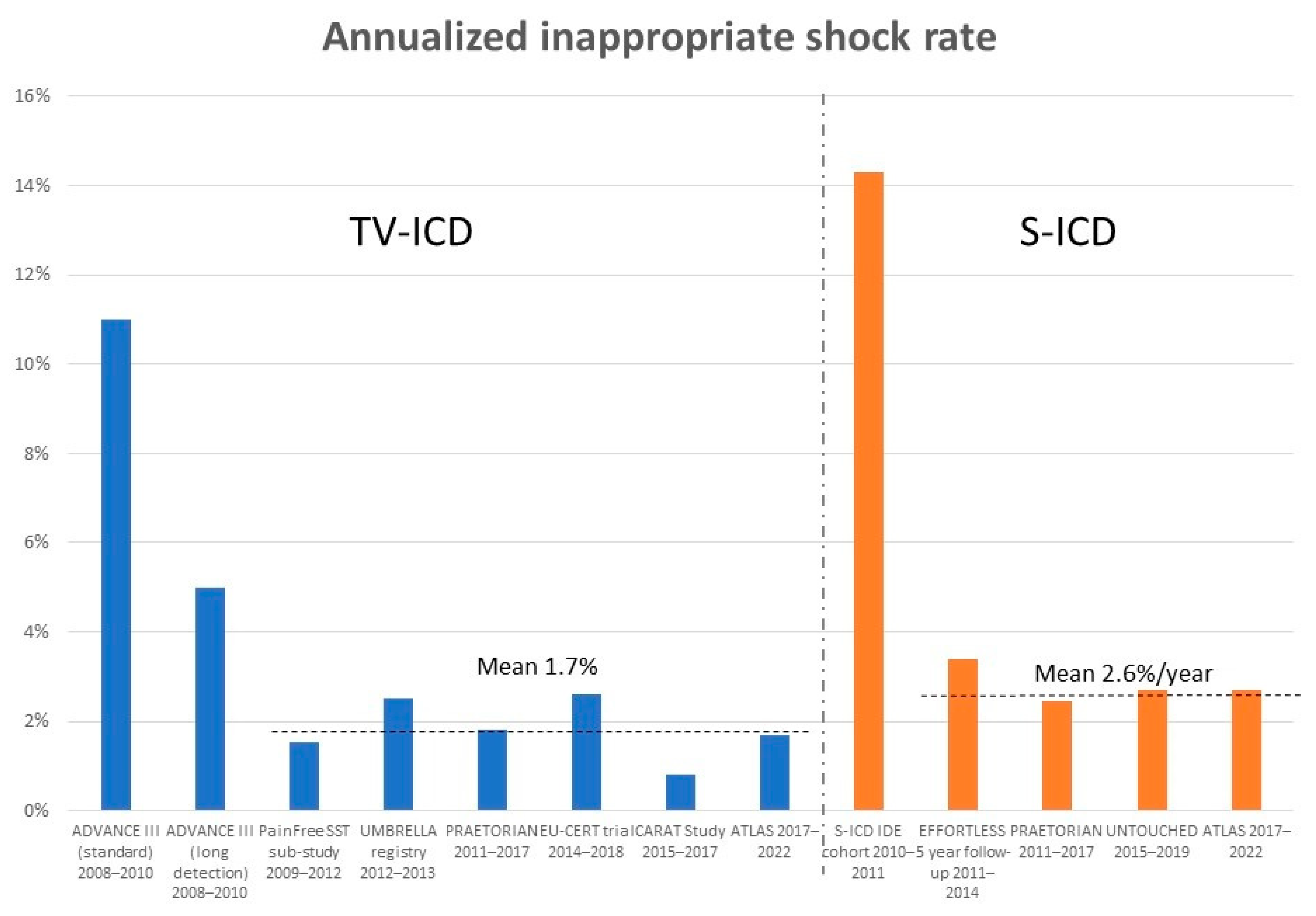
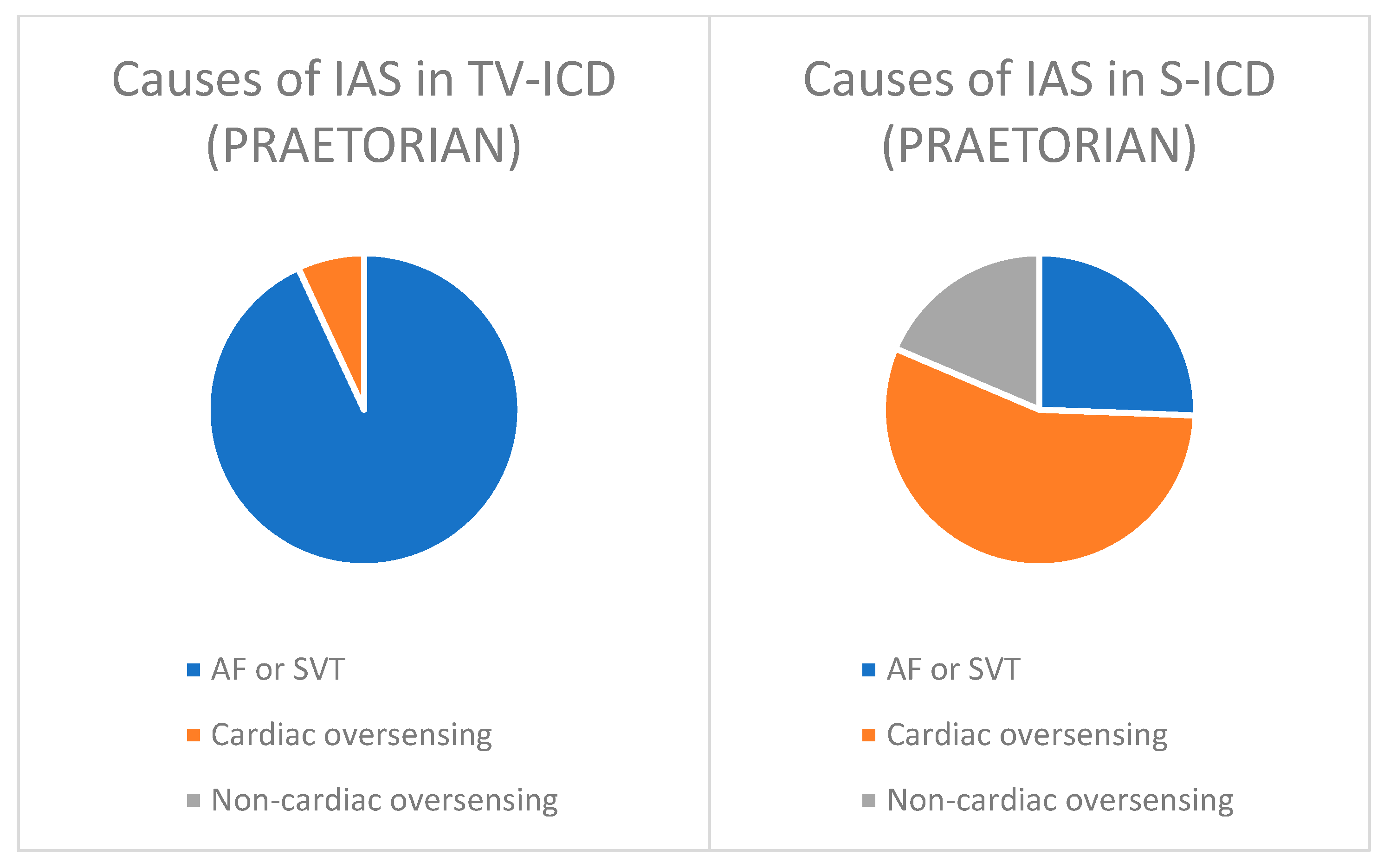
4.1.1. Inappropriate Shocks
4.1.2. Delaying Therapies
4.1.3. ATP
4.1.4. Other Considerations for Reducing Therapies and VAs
4.1.5. Failure to Treat Life-Threatening VAs
4.2. S-ICD
5. The Future
5.1. Reducing Inappropriate and Unnecessary Therapies
5.2. New Delivery Technology
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mirowski, M.; Mower, M.M.; Staewen, W.S.; Tabatznik, B.; Mendeloff, A.I. Standby automatic defibrillator. An approach to prevention of sudden coronary death. Arch. Intern. Med. 1970, 126, 158–161. [Google Scholar] [CrossRef]
- Mirowski, M.; Mower, M.M.; Staewen, W.S.; Denniston, R.H.; Mendeloff, A.I. The development of the tranvenous automatic defibrillator. Arch. Intern. Med. 1972, 129, 773–779. [Google Scholar] [CrossRef]
- Mirowski, M.; Mower, M.M.; Gott, V.L.; Brawley, R.K. Feasibility and effectiveness of low-energy catheter defibrillation in man. Circulation 1973, 47, 79–85. [Google Scholar] [CrossRef]
- Mirowski, M.; Reid, P.R.; Mower, M.M.; Watkins, L.; Gott, V.L.; Schauble, J.F.; Langer, A.; Heilman, M.S.; Kolenik, S.A.; Fischell, R.E.; et al. Termination of malignant ventricular ar-rhythmias with an implanted automatic defibrillator in human beings. N. Engl. J. Med. 1980, 303, 322–324. [Google Scholar] [CrossRef]
- Lindsay, B.D.; Saksena, S.; Rothbart, S.T.; Wasty, N.; Pantopoulos, D. Prospective evaluation of a sequential pacing and high-energy bidirectional shock algorithm for transvenous cardioversion in patients with ventricular tachycardia. Circulation 1987, 76, 601–609. [Google Scholar] [CrossRef]
- Winkle, R.A.; Mead, R.H.; Ruder, M.A.; Gaudiani, V.A.; Smith, N.A.; Buch, W.S.; Schmidt, P.; Shipman, T. Long-term outcome with the automatic implantable cardioverter-defibrillator. J. Am. Coll. Cardiol. 1989, 13, 1353–1361. [Google Scholar] [CrossRef] [PubMed]
- Klein, H.U.; Nisam, S. Michel Mirowski and the beginning of a new era of fighting sudden arrhythmic death. Herzschrittmachertherapie Elektrophysiologie 2015, 26, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. N. Engl. J. Med. 1997, 337, 1576–1583. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Gent, M.; Roberts, R.S.; Dorian, P.; Roy, D.; Sheldon, R.S.; Mitchell, L.B.; Green, M.S.; Klein, G.K.; O’Brien, B. Canadian implantable defibrillator study (CIDS): A randomized trial of the implantable cardioverter defibrillator against amiodarone. Circulation 2000, 101, 1297–1302. [Google Scholar] [CrossRef] [PubMed]
- Kuck, K.H.; Cappato, R.; Siebels, J.; Rüppel, R. Randomized comparison of antiarrhythmic drug therapy with implantable defib-rillators in patients resuscitated from cardiac arrest: The Cardiac Arrest Study Hamburg (CASH). Circulation 2000, 102, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Hallstrom, A.P.; Cappato, R.; Schron, E.B.; Kuck, K.-H.; Zipes, D.P.; Greene, H.L.; Boczor, S.; Domanski, M.; Follmann, D.; et al. Meta-analysis of the implantable cardioverter defibrillator secondary prevention trials. AVID, CASH and CIDS studies. Antiarrhythmics vs Implantable Defibrillator study. Cardiac Arrest Study Hamburg. Canadian Implantable Defibrillator Study. Eur. Heart J. 2000, 21, 2071–2078. [Google Scholar] [CrossRef] [PubMed]
- Moss, A.J.; Hall, W.J.; Cannom, D.S.; Daubert, J.P.; Higgins, S.L.; Klein, H.; Levine, J.H.; Saksena, S.; Waldo, A.L.; Wilber, D.; et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. N. Engl. J. Med. 1996, 335, 1933–1940. [Google Scholar] [CrossRef]
- Buxton, A.E.; Lee, K.L.; Fisher, J.D.; Josephson, M.E.; Prystowsky, E.N.; Hafley, G. A randomized study of the prevention of sudden death in patients with coronary artery disease. N. Engl. J. Med. 1999, 341, 1882–1890, Erratum in N. Engl. J. Med. 2000, 342, 1300. [Google Scholar] [CrossRef]
- Buxton, A.E.; Lee, K.L.; Hafley, G.E.; Wyse, D.G.; Fisher, J.D.; Lehmann, M.H.; Pires, L.A.; Gold, M.R.; Packer, D.L.; Josephson, M.E.; et al. Relation of ejection fraction and inducible ventricular tachycardia to mode of death in patients with coronary artery disease: An analysis of patients enrolled in the multicenter unsustained tachycardia trial. Circulation 2002, 106, 2466–2472. [Google Scholar] [CrossRef] [PubMed]
- Moss, A.J.; Zareba, W.; Hall, W.J.; Klein, H.; Wilber, D.J.; Cannom, D.S.; Daubert, J.P.; Higgins, S.L.; Brown, M.W.; Andrews, M.L. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N. Engl. J. Med. 2002, 346, 877–883. [Google Scholar] [CrossRef]
- Bardy, G.H.; Lee, K.L.; Mark, D.B.; Poole, J.E.; Packer, D.L.; Boineau, R.; Domanski, M.; Troutman, C.; Anderson, J.; Johnson, G.; et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N. Engl. J. Med. 2005, 352, 225–237, Erratum in N. Engl. J. Med. 2005, 352, 2146. [Google Scholar] [CrossRef] [PubMed]
- Poole, J.E.; Olshansky, B.; Mark, D.B.; Anderson, J.; Johnson, G.; Hellkamp, A.S.; Davidson-Ray, L.; Fishbein, D.P.; Boineau, R.E.; Anstrom, K.J.; et al. Long-Term Outcomes of Implantable Cardioverter-Defibrillator Therapy in the SCD-HeFT. J. Am. Coll. Cardiol. 2020, 76, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Hohnloser, S.H.; Kuck, K.H.; Dorian, P.; Roberts, R.S.; Hampton, J.R.; Hatala, R.; Fain, E.; Gent, M.; Connolly, S.J. Prophylactic use of an implantable cardioverter-defibrillator after acute myocardial infarction. N. Engl. J. Med. 2004, 351, 2481–2488. [Google Scholar] [CrossRef]
- Steinbeck, G.; Andresen, D.; Seidl, K.; Brachmann, J.; Hoffmann, E.; Wojciechowski, D.; Kornacewicz-Jach, Z.; Sredniawa, B.; Lupkovics, G.; Hofgärtner, F.; et al. Defibrillator implantation early after myocardial infarction. N. Engl. J. Med. 2009, 361, 1427–1436. [Google Scholar] [CrossRef]
- Zabel, M.; Willems, R.; Lubinski, A.; Bauer, A.; Brugada, J.; Conen, D.; Flevari, P.; Hasenfuß, G.; Svetlosak, M.; Huikuri, H.V.; et al. Clinical effectiveness of primary prevention implantable cardioverter-defibrillators: Results of the EU-CERT-ICD controlled multicentre cohort study. Eur. Heart J. 2020, 41, 3437–3447. [Google Scholar] [CrossRef]
- Schrage, B.; Uijl, A.; Benson, L.; Westermann, D.; Ståhlberg, M.; Stolfo, D.; Dahlström, U.; Linde, C.; Braunschweig, F.; Savarese, G. Association between use of primary-prevention implantable cardioverterdefibrillators and mortality in patients with heart failure: A prospective propensity score-matched analysis from the Swedish Heart Failure Registry. Circulation 2019, 140, 1530–1539. [Google Scholar] [CrossRef] [PubMed]
- Køber, L.; Thune, J.J.; Nielsen, J.C.; Haarbo, J.; Videbæk, L.; Korup, E.; Jensen, G.; Hildebrandt, P.; Steffensen, F.H.; Bruun, N.E.; et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N. Engl. J. Med. 2016, 375, 1221–1230. [Google Scholar] [CrossRef] [PubMed]
- Strickberger, S.; Hummel, J.D.; Bartlett, T.G.; IFrumin, H.; Schuger, C.D.; Beau, S.L.; Bitar, C.; Morady, F. Amiodarone versus implantable cardioverter-defibrillator: Randomized trial in patients with nonischemicdilated cardiomyopathy and asymptomaticnonsustained ventricular tachycardia—AMIOVIRT. J. Am. Coll. Cardiol. 2003, 41, 1707–1712. [Google Scholar] [CrossRef] [PubMed]
- Bänsch, D.; Antz, M.; Boczor, S.; Volkmer, M.; Tebbenjohanns, J.; Seidl, K.; Block, M.; Gietzen, F.; Berger, J.; Kuck, K.H.; et al. Primary prevention of sudden cardiac death in idiopathic dilated cardiomyopathy: The Cardiomyopathy Trial (CAT). Circulation 2002, 105, 1453–1458. [Google Scholar] [CrossRef] [PubMed]
- Kadish, A.; Dyer, A.; Daubert, J.P.; Quigg, R.; Estes, N.M.; Anderson, K.P.; Calkins, H.; Hoch, D.; Goldberger, J.; Shalaby, A.; et al. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N. Engl. J. Med. 2004, 350, 2151–2158. [Google Scholar] [CrossRef] [PubMed]
- Bristow, M.R.; Saxon, L.A.; Boehmer, J.; Krueger, S.; Kass, D.A.; De Marco, T.; Carson, P.; DiCarlo, L.; DeMets, D.; White, B.G.; et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N. Engl. J. Med. 2004, 350, 2140–2150. [Google Scholar] [CrossRef] [PubMed]
- Yafasova, A.; Butt, J.H.; Elming, M.B.; Nielsen, J.C.; Haarbo, J.; Videbæk, L.; Olesen, L.L.; Steffensen, F.H.; Bruun, N.E.; Eiskjær, H.; et al. Long-Term Follow-Up of DANISH (the Danish Study to Assess the Efficacy of ICDs in Patients with Nonischemic Systolic Heart Failure on Mortality). Circulation 2022, 145, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Shun-Shin, M.J.; Zheng, S.L.; Cole, G.D.; Howard, J.P.; Whinnett, Z.I.; Francis, D.P. Implantable cardioverter defibrillators for primary prevention of death in left ventricular dysfunction with and without ischaemic heart disease: A meta-analysis of 8567 patients in the 11 trials. Eur. Heart. J. 2017, 38, 1738–1746. [Google Scholar] [CrossRef]
- Golwala, H.; Bajaj, N.S.; Arora, G.; Arora, P. Implantable Cardioverter-Defibrillator for Nonischemic Cardiomyopathy. Circulation 2017, 135, 201–203. [Google Scholar] [CrossRef]
- Beggs, S.A.S.; Jhund, P.S.; EJackson, C.; McMurray, J.J.V.; Gardner, R.S. Non-ischaemic cardiomyopathy, sudden death and implantable defibrillators: A review and meta-analysis. Heart 2018, 104, 144–150. [Google Scholar] [CrossRef]
- Narayanan, M.A.; Vakil, K.; Reddy, Y.N.; Baskaran, J.; Deshmukh, A.; Benditt, D.G.; Adabag, S. Efficacy of Implantable Cardioverter-Defibrillator Therapy in Patients with Nonischemic Cardiomyopathy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. JACC Clin. Electrophysiol. 2017, 3, 962–970. [Google Scholar] [CrossRef]
- Stavrakis, S.; Asad, Z.; Reynolds, D. Implantable Cardioverter Defibrillators for Primary Prevention of Mortality in Patients with Nonischemic Cardiomyopathy: A Meta-Analysis of Randomized Controlled Trials. J. Cardiovasc. Electrophysiol. 2017, 28, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, P.J.; Ackerman, M.J.; Antzelevitch, C.; Bezzina, C.R.; Borggrefe, M.; Cuneo, B.F.; Wilde, A.A.M. Inherited cardiac arrhythmias. Nat. Rev. Dis. Prim. 2020, 6, 58. [Google Scholar] [CrossRef] [PubMed]
- Corrado, D.; Wichter, T.; Link, M.S.; Hauer, R.N.; Marchlinski, F.E.; Anastasakis, A.; Bauce, B.; Basso, C.; Brunckhorst, C.; Tsatsopoulou, A.; et al. Treatment of arrhythmogenic right ventricular cardiomyopathy/dysplasia: An international task force consensus statement. Circulation 2015, 132, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Priori, S.G.; Blomström-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European society of cardiology (ESC). Endorsed by: Association for European paediatric and congenital cardiology (AEPC). Eur. Heart J. 2015, 2015, 2793–2867. [Google Scholar]
- Task, A.; Elliott, P.M.; Uk, C.; Anastasakis, A.; Germany, M.A.; Germany, M.B.; Cecchi, F.; France, P.C.; Alain, A.; France, H.; et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar] [CrossRef]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; A Blom, N.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur. Heart. J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef] [PubMed]
- Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; Kantor, P.; et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients with Hypertrophic Cardiomyopathy: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2020, 142, e558–e631, Erratum in Circulation 2020, 142, e633. [Google Scholar] [CrossRef] [PubMed]
- Corrado, D.; Link, M.S.; Schwartz, P.J. Implantable defibrillators in primary prevention of genetic arrhythmias. A shocking choice? Eur. Heart J. 2022, 43, 3029–3040. [Google Scholar] [CrossRef]
- Ho, C.Y.; Day, S.M.; Ashley, E.A.; Michels, M.; Pereira, A.C.; Jacoby, D.; Lakdawala, N.K.; Ware, J.S.; Helms, A.S.; Colan, S.D.; et al. Genotype and lifetime burden of disease in hypertrophic cardiomyopathy: Insights from the sarcomeric human cardiomyopathy registry (SHaRe). Circulation 2018, 138, 1387–1398. [Google Scholar] [CrossRef]
- Arbelo, E.; Protonotarios, A.; Gimeno, J.R.; Arbustini, E.; Barriales-Villa, R.; Basso, C.; Bezzina, C.R.; Biagini, E.; A Blom, N.; A de Boer, R.; et al. 2023 ESC Guidelines for the management of cardiomyopathies. Eur. Heart. J. 2023, 44, 3503–3626. [Google Scholar] [CrossRef] [PubMed]
- Cadrin-Tourigny, J.; Bosman, L.P.; Nozza, A.; Wang, W.; Tadros, R.; Bhonsale, A.; Bourfiss, M.; Fortier, A.; Lie, Ø.H.; Saguner, A.M.; et al. A new prediction model for ventricular arrhythmias in arrhythmogenic right ventricular cardiomyopathy. Eur. Heart J. 2019, 40, 1850–1858, Erratum in Eur. Heart J. 2022, 43, 2712. [Google Scholar] [CrossRef] [PubMed]
- Casella, M.; Gasperetti, A.; Gaetano, F.; Busana, M.; Sommariva, E.; Catto, V.; Sicuso, R.; Rizzo, S.; Conte, E.; Mushtaq, S.; et al. Long-term follow-up analysis of a highly characterized arrhythmogenic cardiomyopathy cohort with classical and non-classical phenotypes–a real-world assessment of a novel prediction model: Does the subtype really matter. Europace 2020, 22, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Aquaro, G.D.; De Luca, A.; Cappelletto, C.; Raimondi, F.; Bianco, F.; Botto, N.; Lesizza, P.; Grigoratos, C.; Minati, M.; Dell’omodarme, M.; et al. Prognostic Value of Magnetic Resonance Phenotype in Patients with Arrhythmogenic Right Ventricular Cardiomyopathy. J. Am. Coll. Cardiol. 2020, 75, 2753–2765. [Google Scholar] [CrossRef]
- Baudinaud, P.; Laredo, M.; Badenco, N.; Rouanet, S.; Waintraub, X.; Duthoit, G.; Hidden-Lucet, F.; Redheuil, A.; Maupain, C.; Gandjbakhch, E. External Validation of a Risk Prediction Model for Ventricular Arrhythmias in Arrhythmogenic Right Ventricular Cardiomyopathy. Can. J. Cardiol. 2021, 37, 1263–1266. [Google Scholar] [CrossRef]
- Zhang, N.; Wang, C.; Gasperetti, A.; Song, Y.; Niu, H.; Gu, M.; Duru, F.; Chen, L.; Zhang, S.; Hua, W. Validation of an Arrhythmogenic Right Ventricular Cardiomyopathy Risk-Prediction Model in a Chinese Cohort. J. Clin. Med. 2022, 11, 1973. [Google Scholar] [CrossRef]
- Jordà, P.; Bosman, L.P.; Gasperetti, A.; Mazzanti, A.; Gourraud, J.B.; Davies, B.; Frederiksen, T.C.; Weidmann, Z.M.; Di Marco, A.; Roberts, J.D.; et al. Arrhythmic risk prediction in arrhythmogenic right ventricular cardiomyopathy: External validation of the arrhythmogenic right ventricular cardiomyopathy risk calculator. Eur. Heart J. 2022, 43, 3041–3052. [Google Scholar] [CrossRef] [PubMed]
- Protonotarios, A.; Bariani, R.; Cappelletto, C.; Pavlou, M.; García-García, A.; Cipriani, A.; Protonotarios, I.; Rivas, A.; Wittenberg, R.; Graziosi, M.; et al. Importance of genotype for risk stratification in arrhythmogenic right ventricular cardiomyopathy using the 2019 ARVC risk calculator. Eur. Heart J. 2022, 43, 3053–3067, Erratum in Eur. Heart J. 2022, 43, 3053–3067. [Google Scholar] [CrossRef]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS Guideline for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2018, 72, e91–e220, Erratum in J. Am. Coll. Cardiol. 2018, 72, 1760. [Google Scholar] [CrossRef]
- Mazzanti, A.; Trancuccio, A.; Kukavica, D.; Pagan, E.; Wang, M.; Mohsin, M.; Peterson, D.; Bagnardi, V.; Zareba, W.; Priori, S.G. Independent validation and clinical implications of the risk prediction model for long QT syndrome (1-2-3-LQTS-Risk). Europace 2022, 24, 614–619. [Google Scholar] [CrossRef]
- Tan, N.Y.; Roger, V.L.; Killian, J.M.; Cha, Y.; Noseworthy, P.A.; Dunlay, S.M. Ventricular Arrhythmias Among Patients with Advanced Heart Failure: A Population-Based Study. J. Am. Heart Assoc. 2022, 11, e023377. [Google Scholar] [CrossRef]
- Fröhlich, G.M.; Holzmeister, J.; Hübler, M.; Hübler, S.; Wolfrum, M.; Enseleit, F.; Seifert, B.; Hürlimann, D.; Lehmkuhl, H.B.; Noll, G.; et al. Prophylactic implantable cardioverter defibrillator treatment in patients with end-stage heart failure awaiting heart transplantation. Heart 2013, 99, 1158–1165. [Google Scholar] [CrossRef] [PubMed]
- Clerkin, K.J.; Topkara, V.K.; Demmer, R.T.; Dizon, J.M.; Yuzefpolskaya, M.; Fried, J.A.; Mai, X.; Mancini, D.M.; Takeda, K.; Takayama, H.; et al. Implantable cardioverter-defibrillators in patients with a continuous-flow left ventricular assist device: An analysis of the INTERMACS registry. JACC Heart Fail. 2017, 5, 916–926. [Google Scholar] [CrossRef] [PubMed]
- Vakil, K.; Kazmirczak, F.; Sathnur, N.; Adabag, S.; Cantillon, D.J.; Kiehl, E.L.; Koene, R.; Cogswell, R.; Anand, I.; Roukoz, H. Implantable cardioverter-defibrillator use in patients with left ventricular assist devices: A systematic review and meta-analysis. JACC Heart Fail. 2016, 4, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Refaat, M.M.; Tanaka, T.; Kormos, R.L.; Mcnamara, D.; Teuteberg, J.; Winowich, S.; London, B.; Simon, M.A. Survival benefit of implantable cardio-verter-defibrillators in left ventricular assist device-supported heart failure patients. J. Card. Fail. 2012, 18, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Cantillon, D.J.; Tarakji, K.G.; Kumbhani, D.J.; Smedira, N.G.; Starling, R.C.; Wilkoff, B.L. Improved survival among ventricular assist device recipients with a concomitant implantable cardioverter-defibrillator. Heart Rhythm 2010, 7, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Galand, V.; Flécher, E.; Auffret, V.; Boulé, S.; Vincentelli, A.; Dambrin, C.; Mondoly, P.; Sacher, F.; Nubret, K.; Kindo, M.; et al. Predictors and Clinical Impact of Late Ventricular Arrhythmias in Patients with Continuous-Flow Left Ventricular Assist Devices. JACC Clin. Electrophysiol. 2018, 4, 1166–1175. [Google Scholar] [CrossRef] [PubMed]
- Gulletta, S.; Scandroglio, A.M.; Pannone, L.; Falasconi, G.; Melisurgo, G.; Ajello, S.; D’Angelo, G.; Gigli, L.; Lipartiti, F.; Agricola, E.; et al. Clinical characteristics and outcomes of patients with ventricular arrhythmias after continuous-flow left ventricular assist device implant. Artif. Organs 2022, 46, 1608–1615. [Google Scholar] [CrossRef] [PubMed]
- Pausch, J.; Mersmann, J.; Bhadra, O.D.; Barten, M.J.; Tönnis, T.; Yildirim, Y.; Pecha, S.; Reichenspurner, H.; Bernhardt, A.M. Prognostic impact of implantable cardioverter defibrillators and associated adverse events in patients with continuous flow left ventricular assist devices. Front. Cardiovasc. Med. 2023, 10, 1158248. [Google Scholar] [CrossRef]
- Becker, M.A.; Cornel, J.H.; van de Ven, P.M.; van Rossum, A.C.; Allaart, C.P.; Germans, T. The Prognostic Value of Late Gadolinium-Enhanced Cardiac Magnetic Resonance Imaging in Nonischemic Dilated Cardiomyopathy. JACC Cardiovasc. Imaging 2018, 11, 1274–1284. [Google Scholar] [CrossRef]
- Zegard, A.; Okafor, O.; de Bono, J.; Kalla, M.; Lencioni, M.; Marshall, H.; Hudsmith, L.; Qiu, T.; Steeds, R.; Stegemann, B.; et al. Myocardial Fibrosis as a Predictor of Sudden Death in Patients with Coronary Artery Disease. J. Am. Coll. Cardiol. 2021, 77, 29–41. [Google Scholar] [CrossRef]
- Leyva, F.; Zegard, A.; Okafor, O.; Foley, P.; Umar, F.; Taylor, R.J.; Marshall, H.; Stegemann, B.; Moody, W.; Steeds, R.P.; et al. Myocardial Fibrosis Predicts Ventricular Arrhythmias and Sudden Death after Cardiac Electronic Device Implantation. J. Am. Coll. Cardiol. 2022, 79, 665–678. [Google Scholar] [CrossRef]
- Paddock, S.; Tsampasian, V.; Assadi, H.; Mota, B.C.; Swift, A.J.; Chowdhary, A.; Swoboda, P.; Levelt, E.; Sammut, E.; Dastidar, A.; et al. Clinical Translation of Three-Dimensional Scar, Diffusion Tensor Imaging, Four-Dimensional Flow, and Quantitative Perfusion in Cardiac MRI: A Comprehensive Review. Front. Cardiovasc. Med. 2021, 8, 682027. [Google Scholar] [CrossRef]
- ID NCT01918215. Available online: https://clinicaltrials.gov/ (accessed on 1 January 2024).
- ID NCT04246450. Available online: https://clinicaltrials.gov/ (accessed on 1 January 2024).
- Linde, C. CRT-P or CRT-D in heart failure patients: The RESET-CRT project—A prelude to the randomized controlled RESET-CRT study. Eur. Heart J. 2022, 43, 2600–2602. [Google Scholar] [CrossRef] [PubMed]
- Taborsky, M.; Skala, T.; Aiglova, R.; Fedorco, M.; Kautzner, J.; Jandik, T.; Vancura, V.; Linhart, A.; Valek, M.; Novak, M.; et al. Cardiac Resynchronization and Defibrillator Therapy (CRT-D) or CRT Alone (CRT-P) in patients with dilated cardiomyopathy and heart failure without late gadolinium enhancement (LGE) cardiac magnetic resonance imaging (CMRI) high-risk markers—CRT-REALITY study—Study design and rationale. Biomed. Pap. 2022, 166, 173–179. [Google Scholar] [CrossRef]
- Saleh, K.; Varnava, A.; Shun-Shin, M.J.; Ali, N.; Mohal, J.; Chiew, K.; A Hanif, M.; Merzah, A.J.; Howard, J.P.; Jurak, P.; et al. Ultra-high-frequency ECG assessment of QRS fragmentation predicts sudden cardiac death risk in inherited arrhythmia syndromes. Eur. Heart J. 2022, 43, ehac544.678. [Google Scholar] [CrossRef]
- Nicolson, W.B.; Smith, M.I.; Vali, Z.; Samani, N.J.; Ng, G.A. Application of two novel electrical restitution-based ECG markers of ventricular arrhythmia to patients with nonischemic cardiomyopathy. Pacing Clin. Electrophysiol. 2020, 44, 284–292. [Google Scholar] [CrossRef]
- Attia, Z.I.; Noseworthy, P.A.; Lopez-Jimenez, F.; Asirvatham, S.J.; Deshmukh, A.J.; Gersh, B.J.; Carter, R.E.; Yao, X.; Rabinstein, A.A.; Erickson, B.J.; et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: A retrospective analysis of outcome prediction. Lancet 2019, 394, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Kolk, M.Z.; Deb, B.; Ruipérez-Campillo, S.; Bhatia, N.K.; Clopton, P.; Wilde, A.A.; Narayan, S.M.; Knops, R.E.; Tjong, F.V. Machine learning of electrophysiological signals for the prediction of ventricular arrhythmias: Systematic review and examination of heterogeneity between studies. EBioMedicine 2023, 89, 104462. [Google Scholar] [CrossRef]
- Shiraishi, Y.; Goto, S.; Niimi, N.; Katsumata, Y.; Goda, A.; Takei, M.; Saji, M.; Sano, M.; Fukuda, K.; Kohno, T.; et al. Improved prediction of sudden cardiac death in patients with heart failure through digital processing of electrocardiography. Europace 2023, 25, 922–930. [Google Scholar] [CrossRef] [PubMed]
- Kolk, M.Z.H.; Ruipérez-Campillo, S.; Deb, B.; Bekkers, E.J.; Allaart, C.P.; Rogers, A.J.; Van Der Lingen, A.-L.C.J.; Florez, L.A.; Isgum, I.; De Vos, B.D.; et al. Optimizing patient selection for primary prevention implantable cardioverter-defibrillator implantation: Utilizing multimodal machine learning to assess risk of implantable cardioverter-defibrillator non-benefit. Europace 2023, 25, euad271. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, H.A.; Jones, R.E.; Hammersley, D.J.; Hatipoglu, S.; Balaban, G.; Mach, L.; Halliday, B.P.; Lamata, P.; Prasad, S.K.; Bishop, M.J. Machine learning analysis of complex late gadolinium enhancement patterns to improve risk prediction of major arrhythmic events. Front. Cardiovasc. Med. 2023, 10, 1082778. [Google Scholar] [CrossRef]
- ID NCT05373940. Available online: https://clinicaltrials.gov/ (accessed on 1 January 2024).
- Pun, P.H.; Hellkamp, A.S.; Sanders, G.D.; Middleton, J.P.; Hammill, S.C.; Al-Khalidi, H.R.; Curtis, L.H.; Fonarow, G.C.; Al-Khatib, S.M. Primary prevention implantable cardioverter defibrillators in end-stage kidney disease patients on dialysis: A matched cohort study. Nephrol. Dial. Transplant. 2015, 30, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, I.; Kutyifa, V.; Zareba, W.; Huang, D.T.-C.; Rosero, S.Z.; Younis, A.; Schuger, C.; Gao, A.; McNitt, S.; Polonsky, B.; et al. Primary prevention implantable cardioverter defibrillator in cardiac resynchronization therapy recipients with advanced chronic kidney disease. Front. Cardiovasc. Med. 2023, 10, 1237118. [Google Scholar] [CrossRef]
- Junttila, M.J.; Pelli, A.; Kenttä, T.V.; Friede, T.; Willems, R.; Bergau, L.; Malik, M.; Vandenberk, B.; Vos, M.A.; Merkely, B.; et al. Appropriate Shocks and Mortality in Patients with Versus without Diabetes with Prophylactic Implantable Cardioverter Defibrillators. Diabetes Care 2020, 43, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Hu, J.; Zhuo, W.; Wan, R.; Hong, K. Influence of diabetes on mortality and ICD therapies in ICD recipients: A systematic review and meta-analysis of 162,780 patients. Cardiovasc. Diabetol. 2022, 21, 143. [Google Scholar] [CrossRef]
- Postigo, A.; Martínez-Sellés, M. Sex Influence on Heart Failure Prognosis. Front. Cardiovasc. Med. 2020, 7, 616273. [Google Scholar] [CrossRef]
- Rho, R.W.; Patton, K.K.; Poole, J.E.; Cleland, J.G.; Shadman, R.; Anand, I.; Maggioni, A.P.; Carson, P.E.; Swedberg, K.; Levy, W.C. Important differences in mode of death between men and women with heart failure who would qualify for a primary prevention implantable cardioverter-defibrillator. Circulation 2012, 126, 2402–2407, Erratum in Circulation 2013, 127, E541. [Google Scholar] [CrossRef]
- Martínez-Solano, J.; Martínez-Sellés, M. Sudden Death in Men Versus Women with Heart Failure. Curr. Heart Fail. Rep. 2023, 20, 129–137. [Google Scholar] [CrossRef]
- Barra, S.; Providência, R.; Boveda, S.; Narayanan, K.; Virdee, M.; Marijon, E.; Agarwal, S. Do women benefit equally as men from the primary prevention implantable cardioverter-defibrillator? Europace 2018, 20, 897–901. [Google Scholar] [CrossRef]
- Shadman, R.; Poole, J.E.; Mozaffarian, D.; Cleland, J.G.; Swedberg, K.; Maggioni, A.P.; Anand, I.S.; Carson, P.; Levy, W. Predicting the Proportional Risk of Sudden Cardiac Death in a Multicenter Cohort (abstr). Circulation 2011, 124, A17819. [Google Scholar]
- Bilchick, K.C.; Wang, Y.; Cheng, A.; Curtis, J.P.; Dharmarajan, K.; Stukenborg, G.J.; Shadman, R.; Anand, I.; Lund, L.H.; Dahlström, U.; et al. Seattle Heart Failure and Proportional Risk Models Predict Benefit From Implantable Cardioverter-Defibrillators. J. Am. Coll. Cardiol. 2017, 69, 2606–2618. [Google Scholar] [CrossRef] [PubMed]
- Younis, A.; Goldberger, J.J.; Kutyifa, V.; Zareba, W.; Polonsky, B.; Klein, H.; Aktas, M.K.; Huang, D.; Daubert, J.; Estes, M.; et al. Predicted benefit of an implantable cardioverter-defibrillator: The MADIT-ICD benefit score. Eur. Heart J. 2021, 42, 1676–1684, Erratum in Eur. Heart J. 2021, 42, 1441. [Google Scholar] [CrossRef] [PubMed]
- Lincoff, A.M.; Brown-Frandsen, K.; Colhoun, H.M.; Deanfield, J.; Emerson, S.S.; Esbjerg, S.; Hardt-Lindberg, S.; Hovingh, G.K.; Kahn, S.E.; Kushner, R.F.; et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N. Engl. J. Med. 2023, 389, 2221–2232. [Google Scholar] [CrossRef]
- Kosiborod, M.N.; Abildstrøm, S.Z.; Borlaug, B.A.; Butler, J.; Rasmussen, S.; Davies, M.; Hovingh, G.K.; Kitzman, D.W.; Lindegaard, M.L.; Møller, D.V. Semaglutide in Patients with Heart Failure with Preserved Ejection Fraction and Obesity. N. Engl. J. Med. 2023, 389, 1069–1084. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.; Abildstrøm, S.Z.; Borlaug, B.A.; Davies, M.J.; Kitzman, D.W.; Petrie, M.C.; Shah, S.J.; Verma, S.; Abhayaratna, W.P.; Chopra, V.; et al. Semaglutide in Patients with Obesity and Heart Failure Across Mildly Reduced or Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2023, 82, 2087–2096. [Google Scholar] [CrossRef] [PubMed]
- Mcmurray, J.J.V.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef]
- Martens, P.; Nuyens, D.; Rivero-Ayerza, M.; Van Herendael, H.; Vercammen, J.; Ceyssens, W.; Luwel, E.; Dupont, M.; Mullens, W. Sacubitril/valsartan reduces ventricular arrhythmias in parallel with left ventricular reverse remodeling in heart failure with reduced ejection fraction. Clin. Res. Cardiol. 2019, 108, 1074–1082. [Google Scholar] [CrossRef]
- Pozzi, A.; Abete, R.; Tavano, E.; Kristensen, S.L.; Rea, F.; Iorio, A.; Iacovoni, A.; Corrado, G.; Wong, C. Sacubitril/valsartan and arrhythmic burden in patients with heart failure and reduced ejection fraction: A systematic review and meta-analysis. Heart Fail. Rev. 2023, 28, 1395–1403. [Google Scholar] [CrossRef]
- Fernandes, G.C.; Fernandes, A.; Cardoso, R.; Penalver, J.; Knijnik, L.; Mitrani, R.D.; Myerburg, R.J.; Goldberger, J.J. Association of SGLT2 inhibitors with arrhythmias and sudden cardiac death in patients with type 2 diabetes or heart failure: A meta-analysis of 34 randomized controlled trials. Heart Rhythm 2021, 18, 1098–1105. [Google Scholar] [CrossRef]
- Sfairopoulos, D.; Zhang, N.; Wang, Y.; Chen, Z.; Letsas, K.P.; Tse, G.; Li, G.; Lip, G.Y.H.; Liu, T.; Korantzopoulos, P. Association between sodium–glucose cotransporter-2 inhibitors and risk of sudden cardiac death or ventricular arrhythmias: A meta-analysis of randomized controlled trials. Europace 2022, 24, 20–30. [Google Scholar] [CrossRef]
- Kolben, Y.; Raccah, B.H.; Koev, I.; Luria, D.; Amir, O.; Biton, Y. Implantable cardioverter defibrillator for primary prevention in patients with non-ischemic cardiomyopathy in the era of novel therapeutic agents-meta-analysis. Front. Cardiovasc. Med. 2023, 10, 1192101. [Google Scholar] [CrossRef]
- Januzzi, J.L., Jr.; Prescott, M.F.; Butler, J.; Felker, G.M.; Maisel, A.S.; McCague, K.; Camacho, A.; Piña, I.L.; Rocha, R.A.; Shah, A.M.; et al. Association of change in N-terminal pro-B-type natriuretic peptide following initiation of sacubitril-valsartan treatment with cardiac structure and function in patients with heart failure with reduced ejection fraction. JAMA 2019, 322, 1085–1095. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, R.; Lu, C.; Chen, Q.; Xu, T.; Li, D. Effects of the angiotensin-receptor neprilysin inhibitor on cardiac reverse remodeling: Metaanalysis. J. Am. Heart Assoc. 2019, 8, e012272. [Google Scholar] [CrossRef] [PubMed]
- Felker, G.M.; Butler, J.; Ibrahim, N.E.; Piña, I.L.; Maisel, A.; Bapat, D.; Camacho, A.; Ward, J.H.; Williamson, K.M.; Solomon, S.D.; et al. Implantable Cardioverter-Defibrillator Eligibility after Initiation of Sacubitril/Valsartan in Chronic Heart Failure: Insights from PROVE-HF. Circulation 2021, 144, 180–182. [Google Scholar] [CrossRef] [PubMed]
- Yehya, A.; Davis, J.D.; Sauer, A.J.; Ibrahim, N.E. Is it time to revisit ICD indications? Heart Fail. Rev. 2022, 27, 2177–2179, Erratum in Heart Fail. Rev. 2022, 27, 991. [Google Scholar] [CrossRef]
- Flett, A.; Cebula, A.; Nicholas, Z.; Adam, R.; Ewings, S.; Prasad, S.; Cleland, J.G.; Eminton, Z.; Curzen, N. Rationale and study protocol for the BRITISH randomized trial (Using cardiovascular magnetic resonance identified scar as the benchmark risk indication tool for implantable cardioverter defibrillators in patients with nonischemic cardiomyopathy and severe systolic heart failure). Am. Heart J. 2023, 266, 149–158. [Google Scholar] [CrossRef]
- ID NCT04558723. Available online: https://clinicaltrials.gov/ (accessed on 1 January 2024).
- ID NCT06055504. Available online: https://clinicaltrials.gov/ (accessed on 1 January 2024).
- ID NCT05665608. Available online: https://clinicaltrials.gov/ (accessed on 1 January 2024).
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 ACC/AHA/HFSA Guideline for the Management of Heart Failure. J. Card. Fail. 2022, 28, e1–e167. [Google Scholar] [CrossRef] [PubMed]
- Hauser, R.G.; Casey, S.A.; Gitter, C.B.; Tang, C.Y.; Abdelhadi, R.H.; Gornick, C.C.; Stanberry, L.; Sengupta, J.D. Reliability and longevity of implantable defibrillators. J. Interv. Card. Electrophysiol. 2021, 62, 507–518. [Google Scholar] [CrossRef]
- Jordan, J.; Titscher, G.; Peregrinova, L.; Kirsch, H. Manual for the psychotherapeutic treatment of acute and post-traumatic stress disorders following multiple shocks from implantable cardioverter defibrillator (ICD). Psychosoc. Med. 2013, 10, Doc09. [Google Scholar] [CrossRef]
- Dichtl, W.; Wolber, T.; Paoli, U.; Brüllmann, S.; Stühlinger, M.; Berger, T.; Spuller, K.; Strasak, A.; Pachinger, O.; Haegeli, L.M.; et al. Appropriate therapy but not inappropriate shocks predict survival in implantable cardioverter defibrillator patients. Clin. Cardiol. 2011, 34, 433–436. [Google Scholar] [CrossRef]
- Daubert, J.P.; Zareba, W.; Cannom, D.S.; McNitt, S.; Rosero, S.Z.; Wang, P.; Schuger, C.; Steinberg, J.S.; Higgins, S.L.; Wilber, D.J.; et al. Inappropriate implantable cardioverter-defibrillator shocks in MADIT II: Frequency, mechanisms, predictors, and survival impact. J. Am. Coll. Cardiol. 2008, 51, 1357–1365. [Google Scholar] [CrossRef]
- Saxon, L.A.; Hayes, D.L.; Gilliam, F.R.; Heidenreich, P.A.; Day, J.; Seth, M.; Meyer, T.E.; Jones, P.W.; Boehmer, J.P. Long-term outcome after ICD and CRT implantation and influence of remote device follow-up: The ALTITUDE survival study. Circulation 2010, 122, 2359–2367. [Google Scholar] [CrossRef] [PubMed]
- van Rees, J.B.; Borleffs, C.J.W.; de Bie, M.K.; Stijnen, T.; van Erven, L.; Bax, J.J.; Schalij, M.J. Inappropriate implantable cardioverter-defibrillator shocks: Incidence, predictors, and impact on mortality. J. Am. Coll. Cardiol. 2011, 57, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Aktaş, M.K.; Younis, A.; Zareba, W.; Kutyifa, V.; Klein, H.; Daubert, J.P.; Estes, M.; McNitt, S.; Polonsky, B.; Goldenberg, I. Survival after Implantable Cardioverter-Defibrillator Shocks. J. Am. Coll. Cardiol. 2021, 77, 2453–2462. [Google Scholar] [CrossRef] [PubMed]
- Deo, R.; Pothineni, N.V.K. The “Shocking” Reality of ICD Therapies. J. Am. Coll. Cardiol. 2021, 77, 2463–2465. [Google Scholar] [CrossRef] [PubMed]
- Dichtl, W.; De Sousa, J.; Lopez, J.M.R.; Campo, E.G.; Gutleben, K.-J.; Poezevara, Y.; Probst, V. Low rates of inappropriate shocks in contemporary real-world implantable cardioverter defibrillator patients: The CARAT observational study. Europace 2023, 25, euad186, Erratum in Europace 2023, 25, euad26. [Google Scholar] [CrossRef] [PubMed]
- Knops, R.E.; Nordkamp, L.R.O.; Delnoy, P.-P.H.; Boersma, L.V.; Kuschyk, J.; El-Chami, M.F.; Bonnemeier, H.; Behr, E.R.; Brouwer, T.F.; Kääb, S.; et al. Subcutaneous or Transvenous Defibrillator Therapy. N. Engl. J. Med. 2020, 383, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Kleemann, T.; Becker, T.; Doenges, K.; Vater, M.; Senges, J.; Schneider, S.; Saggau, W.; Weisse, U.; Seidl, K. Annual rate of transvenous defibrillation lead defects in implantable cardioverter-defibrillators over a period of >10 years. Circulation 2007, 115, 2474–2480. [Google Scholar] [CrossRef]
- Koneru, J.N.; Jones, P.W.; Hammill, E.F.; Wold, N.; Ellenbogen, K.A. Risk Factors and Temporal Trends of Complications Associated with Transvenous Implantable Cardiac Defibrillator Leads. J. Am. Heart. Assoc. 2018, 7, e007691. [Google Scholar] [CrossRef]
- Khattak, F.; Gupta, A.; Alluri, K.; Shariff, N.; Saba, S. Rate and predictors of electrical failure in non-recalled defibrillator leads. Indian Pacing Electrophysiol. J. 2019, 19, 100–103. [Google Scholar] [CrossRef]
- Goldenberg, I.; Moss, A.J.; Hall, W.J.; McNitt, S.; Zareba, W.; Andrews, M.L.; Cannom, D.S. Causes and consequences of heart failure after prophylactic implantation of a defibrillator in the multicenter automatic defibrillator implantation trial II. Circulation 2006, 113, 2810–2817. [Google Scholar] [CrossRef] [PubMed]
- Poole, J.E.; Johnson, G.W.; Hellkamp, A.S.; Anderson, J.; Callans, D.J.; Raitt, M.H.; Reddy, R.K.; Marchlinski, F.E.; Yee, R.; Guarnieri, T.; et al. Prognostic importance of defibrillator shocks in patients with heart failure. N. Engl. J. Med. 2008, 359, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.O.; Sherfesee, L.; DeGroot, P.J.; Wathen, M.S.; Wilkoff, B.L. Differences in effects of electrical therapy type for ventricular arrhythmias on mortality in implantable cardioverter-defibrillator patients. Heart Rhythm 2010, 7, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Wilkoff, B.L.; Williamson, B.D.; Stern, R.S.; Moore, S.L.; Lu, F.; Lee, S.W.; Birgersdotter-Green, U.M.; Wathen, M.S.; Van Gelder, I.C.; Heubner, B.M.; et al. Strategic programming of detection and therapy parameters in implantable cardioverter-defibrillators reduces shocks in primary prevention patients: Results from the PREPARE (Primary Prevention Parameters Evaluation) study. J. Am. Coll. Cardiol. 2008, 52, 541–550. [Google Scholar] [CrossRef]
- Gasparini, M.; Menozzi, C.; Proclemer, A.; Landolina, M.; Iacopino, S.; Carboni, A.; Lombardo, E.; Regoli, F.; Biffi, M.; Burrone, V.; et al. A simplified biventricular defibrillator with fixed long detection intervals reduces implantable cardioverter defibrillator (ICD) interventions and heart failure hospitalizations in patients with non-ischaemic cardiomyopathy implanted for primary prevention: The RELEVANT [Role of long dEtection window programming in patients with LEft VentriculAr dysfunction, Non-ischemic eTiology in primary prevention treated with a biventricular ICD] study. Eur. Heart J. 2009, 30, 2758–2767. [Google Scholar] [CrossRef]
- Moss, A.J.; Schuger, C.; Beck, C.A.; Brown, M.W.; Cannom, D.S.; Daubert, J.P.; Estes, N.M.I.; Greenberg, H.; Hall, W.J.; Huang, D.T.; et al. Reduction in inappropriate therapy and mortality through ICD programming. N. Engl. J. Med. 2012, 367, 2275–2283. [Google Scholar] [CrossRef]
- Gasparini, M.; Proclemer, A.; Klersy, C.; Kloppe, A.; Lunati, M.; Ferrer, J.B.M.; Hersi, A.; Gulaj, M.; Wijfels, M.C.E.F.; Santi, E.; et al. Effect of long-detection interval vs standard-detection interval for implantable cardioverter-defibrillators on antitachycardia pacing and shock delivery: The ADVANCE III randomized clinical trial. JAMA 2013, 309, 1903–1911, Erratum in JAMA 2013, 309, 2552. [Google Scholar] [CrossRef]
- Saeed, M.; Hanna, I.; Robotis, D.; Styperek, R.; Polosajian, L.; Khan, A.; Alonso, J.; Nabutovsky, Y.; Neason, C. Programming implantable cardioverter-defibrillators in patients with primary prevention indication to prolong time to first shock: Results from the PROVIDE study. J. Cardiovasc. Electrophysiol. 2014, 25, 52–59. [Google Scholar] [CrossRef]
- Tan, V.H.; Wilton, S.B.; Kuriachan, V.; Sumner, G.L.; Exner, D.V. Impact of programming strategies aimed at reducing nonessential implantable cardioverter defibrillator therapies on mortality: A systematic review and meta-analysis. Circ. Arrhythmia Electrophysiol. 2014, 7, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Scott, P.A.; Silberbauer, J.; McDonagh, T.A.; Murgatroyd, F.D. Impact of prolonged implantable cardioverter-defibrillator arrhythmia detection times on outcomes: A meta-analysis. Heart Rhythm 2014, 11, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, Y.; Takagi, M.; Kakihara, J.; Sakamoto, S.; Doi, A.; Sugioka, K.; Hanatani, A.; Yoshiyama, M. Safety and efficacy of high-rate cutoff and long detection interval ICD programming in secondary prevention patients. Heart Vessel. 2017, 32, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Vargas, N.; Tibullo, L.; Landi, C.A.; Carifi, G.; Landi, E.; Salsano, E.; Di Grezia, F.; Candelmo, F. Slow ventricular tachycardia in a 91-year-old man with implantable cardioverter-defibrillator and acute respiratory failure. Am. J. Emerg. Med. 2017, 35, 1213.e5–1213.e8. [Google Scholar] [CrossRef]
- Wannhoff, A.; Nusshag, C.; Stremmel, W.; Merle, U. Slow ventricular tachycardia presenting with acute liver failure. SAGE Open Med. Case Rep. 2017, 5, 2050313X17718100. [Google Scholar] [CrossRef] [PubMed]
- Lüsebrink, U.; Duncker, D.; Hess, M.; Heinrichs, I.; Gardiwal, A.; Oswald, H.; König, T.; Klein, G. Clinical relevance of slow ventricular tachycardia in heart failure patients with primary prophylactic implantable cardioverter defibrillator indication. Europace 2013, 15, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Garner, J.B.; Miller, J.M.; Fellow, C.E. Wide Complex Tachycardia—Ventricular Tachycardia or Not Ventricular Tachycardia, that Remains the Question. Arrhythmia Electrophysiol. Rev. 2013, 2, 23–29. [Google Scholar] [CrossRef]
- Almendral, J.; Arenal, A.; Villacastin, J.P.; Román, D.S.; Bueno, H.; Alday, J.M.; Pastor, A.; Delcan, J.L. The importance of antitachycardia pacing for patients presenting with ventricular tachycardia. Pacing Clin. Electrophysiol. 1993, 16 Pt 2, 535–539. [Google Scholar] [CrossRef]
- Wathen, M.S.; Sweeney, M.O.; DeGroot, P.J.; Stark, A.J.; Koehler, J.L.; Chisner, M.B.; Machado, C.; Adkisson, W.O.; PainFREE ℞ Investigators. Shock reduction using antitachycardia pacing for spontaneous rapid ventricular tachycardia in patients with coronary artery disease. Circulation 2001, 104, 796–801. [Google Scholar] [CrossRef]
- Cheng, A.; Joung, B.; Brown, M.L.; Koehler, J.; Lexcen, D.R.; Sanders, P.; Ellenbogen, K.A. Characteristics of ventricular tachyarrhythmias and their susceptibility to antitachycardia pacing termination in patients with ischemic and nonischemic cardiomyopathy: A patient-level meta-analysis of three large clinical trials. J. Cardiovasc. Electrophysiol. 2020, 31, 2720–2726. [Google Scholar] [CrossRef]
- Swenson, D.J.; Taepke, R.T.; Blauer, J.J.; Kwan, E.; Ghafoori, E.; Plank, G.; Vigmond, E.; MacLeod, R.S.; DeGroot, P.; Ranjan, R. Direct comparison of a novel antitachycardia pacing algorithm against present methods using virtual patient modeling. Heart Rhythm 2020, 17, 1602–1608. [Google Scholar] [CrossRef]
- Yee, R.; Fisher, J.D.; Birgersdotter-Green, U.; Smith, T.W.; Kenigsberg, D.N.; Canby, R.; Jackson, T.; Taepke, R.; DeGroot, P. Initial Clinical Experience with a New Automated Antitachycardia Pacing Algorithm: Feasibility and Safety in an Ambulatory Patient Cohort. Circ. Arrhythmia Electrophysiol. 2017, 10, e004823. [Google Scholar] [CrossRef] [PubMed]
- Morishima, I.; Kanzaki, Y.; Morita, Y.; Tsuji, Y. Successful termination of ventricular tachycardia with intrinsic anti-tachycardia pacing. Indian Pacing Electrophysiol. J. 2021, 21, 394–396. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, H.; Watanabe, M.; Kamada, R.; Anzai, T. Intrinsic anti-tachycardia pacing terminated ventricular tachycardia resistant to traditional anti-tachycardia pacing. Indian Pacing Electrophysiol. J. 2022, 22, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, R.; Gubran, C.; Jeavons, C. Automatic adjustment of ventricular antitachycardia pacing and individualized device therapy. Heart Case Rep. 2021, 8, 171–175. [Google Scholar] [CrossRef]
- Varma, N.; Love, C.J.; Schweikert, R.; Moll, P.; Michalski, J.; Epstein, A.E.; TRUST Investigators. Automatic remote monitoring utilizing daily transmissions: Transmission reliability and implantable cardioverter defibrillator battery longevity in the TRUST trial. Europace 2018, 20, 622–628. [Google Scholar] [CrossRef]
- Guédon-Moreau, L.; Kouakam, C.; Klug, D.; Marquié, C.; Brigadeau, F.; Boulé, S.; Blangy, H.; Lacroix, D.; Clémenty, J.; Sadoul, N.; et al. Decreased delivery of inappropriate shocks achieved by remote monitoring of ICD: A substudy of the ECOST trial. J. Cardiovasc. Electrophysiol. 2014, 25, 763–770. [Google Scholar] [CrossRef]
- Ruwald, M.H.; Abu-Zeitone, A.; Jons, C.; Ruwald, A.-C.; McNitt, S.; Kutyifa, V.; Zareba, W.; Moss, A.J. Impact of carvedilol and metoprolol on inappropriate implantable cardioverter-defibrillator therapy: The MADIT-CRT trial (Multicenter Automatic Defibrillator Implantation with Cardiac Resynchronization Therapy). J. Am. Coll. Cardiol. 2013, 62, 1343–1350. [Google Scholar] [CrossRef]
- Strik, M.; Ploux, S.; Eschalier, R.; Mondoly, P.; Fontagne, L.; Ramirez, F.D.; Haïssaguerre, M.; Bordachar, P. T-Wave Oversensing with Contemporary Implantable Cardioverter–Defibrillators. J. Cardiovasc. Dev. Dis. 2023, 10, 430. [Google Scholar] [CrossRef]
- Swerdlow, C.D.; Gunderson, B.D.; Ousdigian, K.T.; Abeyratne, A.; Stadler, R.W.; Gillberg, J.M.; Patel, A.S.; Ellenbogen, K.A. Downloadable algorithm to reduce inappropriate shocks caused by fractures of implantable cardioverter-defibrillator leads. Circulation 2008, 118, 2122–2129. [Google Scholar] [CrossRef]
- Swerdlow, C.D.; Gunderson, B.D.; Ousdigian, K.T.; Abeyratne, A.; Sachanandani, H.; Ellenbogen, K.A. Downloadable software algorithm reduces inappropriate shocks caused by implantable cardioverter-defibrillator lead fractures: A prospective study. Circulation 2010, 122, 1449–1455. [Google Scholar] [CrossRef]
- Welte, N.; Strik, M.; Eschalier, R.; Mondoly, P.; Defaye, P.; Frontera, A.; Ritter, P.; Haïssaguerre, M.; Ploux, S.; Koneru, J.; et al. Multicenter investigation of an implantable cardioverter-defibrillator algorithm to detect oversensing. Heart Rhythm 2017, 14, 1008–1015. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, N.A.; Roka, A.; Lubitz, S.A.; Gold, M.R.; Daubert, C.; Linde, C.; Steffel, J.; Singh, J.P.; Mela, T. Reduced appropriate implantable cardioverter-defibrillator therapy after cardiac resynchronization therapy-induced left ventricular function recovery: A meta-analysis and systematic review. Eur. Heart J. 2015, 36, 2780–2789. [Google Scholar] [CrossRef]
- Saini, A.; Kannabhiran, M.; Reddy, P.; Gopinathannair, R.; Olshansky, B.; Dominic, P. Cardiac Resynchronization Therapy May Be Antiarrhythmic Particularly in Responders: A Systematic Review and Meta-Analysis. JACC Clin. Electrophysiol. 2016, 2, 307–316. [Google Scholar] [CrossRef]
- Deif, B.; Ballantyne, B.; Almehmadi, F.; Mikhail, M.; McIntyre, W.F.; Manlucu, J.; Yee, R.; Sapp, J.L.; Roberts, J.D.; Healey, J.S.; et al. Cardiac resynchronization is pro-arrhythmic in the absence of reverse ventricular remodelling: A systematic review and meta-analysis. Cardiovasc. Res. 2018, 114, 1435–1444. [Google Scholar] [CrossRef] [PubMed]
- Herweg, B.; Sharma, P.S.; Cano, O.; Ponnusamy, S.S.; Zanon, F.; Jastrzebski, M.; Zou, J.; Chelu, M.G.; Vernooy, K.; Whinnett, Z.I.; et al. Arrhythmic Risk in Biventricular Pacing Compared with Left Bundle Branch Area Pacing: The International LBBAP Collaborative Study (I-CLAS). Circulation 2024, 149, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Pavri, B.B. Conduction system pacing versus biventricular pacing: Reduced repolarization heterogeneity in addition to improved depolarization. J. Cardiovasc. Electrophysiol. 2022, 33, 287–295. [Google Scholar] [CrossRef]
- Thøgersen, A.M.; Larsen, J.M.; Johansen, J.B.; Abedin, M.; Swerdlow, C.D. Failure to Treat Life-Threatening Ventricular Tachyarrhythmias in Contemporary Implantable Cardioverter–Defibrillators: Implications for Strategic Programming. Circ. Arrhythmia Electrophysiol. 2017, 10, e005305. [Google Scholar] [CrossRef]
- Tseng, Z.H.; Hayward, R.M.; Clark, N.M.; Mulvanny, C.G.; Colburn, B.J.; Ursell, P.C.; Olgin, J.E.; Hart, A.P.; Moffatt, E. Sudden Death in Patients with Cardiac Implantable Electronic Devices. JAMA Intern. Med. 2015, 175, 1342–1350. [Google Scholar] [CrossRef]
- Wilkoff, B.L.; Sterns, L.D.; Katcher, M.S.; Upadhyay, G.; Seizer, P.; Kang, C.; Rhude, J.; Davis, K.J.; Fischer, A. Novel ventricular tachyarrhythmia detection enhancement detects undertreated life-threatening arrhythmias. Heart Rhythm O2 2021, 3, 70–78. [Google Scholar] [CrossRef]
- Lakkireddy, D.R.; Segar, D.S.; Sood, A.; Wu, M.; Rao, A.; Sohail, M.R.; Pokorney, S.D.; Blomström-Lundqvist, C.; Piccini, J.P.; Granger, C.B. Early Lead Extraction for Infected Implanted Cardiac Electronic Devices: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2023, 81, 1283–1295. [Google Scholar] [CrossRef]
- Bongiorni, M.G.; Kennergren, C.; Butter, C.; Deharo, J.C.; Kutarski, A.; Rinaldi, C.; Romano, S.L.; Maggioni, A.P.; Andarala, M.; Auricchio, A.; et al. The European Lead Extraction ConTRolled (ELECTRa) study: A European Heart Rhythm Association (EHRA) Registry of Transvenous Lead Extraction Outcomes. Eur. Heart J. 2017, 38, 2995–3005. [Google Scholar] [CrossRef] [PubMed]
- Rordorf, R.; Casula, M.; Pezza, L.; Fortuni, F.; Sanzo, A.; Savastano, S.; Vicentini, A. Subcutaneous versus transvenous implantable defibrillator: An updated meta-analysis. Heart Rhythm 2021, 18, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Rordorf, R. The ATLAS Randomised Clinical Trial: What do the Superiority Results Mean for Subcutaneous ICD Therapy and Sudden Cardiac Death Prevention as a Whole? Arrhythmia Electrophysiol. Rev. 2022, 11 (Suppl. S1). [Google Scholar] [CrossRef] [PubMed]
- Bettin, M.; Rath, B.; Ellermann, C.; Leitz, P.; Reinke, F.; Köbe, J.; Eckardt, L.; Frommeyer, G. Follow-up of the first patients with a totally subcutaneous ICD in Germany from implantation till battery depletion. Clin. Res. Cardiol. 2019, 108, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Quast, A.B.E.; van Dijk, V.F.; Yap, S.; Maass, A.H.; Boersma, L.V.A.; Theuns, D.A.; Knops, R.E. Six-year follow-up of the initial Dutch subcutaneous implantable cardioverter-defibrillator cohort: Long-term complications, replacements, and battery longevity. J. Cardiovasc. Electrophysiol. 2018, 29, 1010–1016. [Google Scholar] [CrossRef]
- Crozier, I.; Haqqani, H.; Kotschet, E.; Shaw, D.; Prabhu, A.; Roubos, N.; Alison, J.; Melton, I.; Denman, R.; Lin, T.; et al. First-in-Human Chronic Implant Experience of the Substernal Extravascular Implantable Cardioverter-Defibrillator. JACC Clin. Electrophysiol. 2020, 6, 1525–1536. [Google Scholar] [CrossRef]
- Sears, S.F.; Harrell, R.; Crozier, I.; Murgatroyd, F.; Boersma, L.V.A.; Manlucu, J.; Knight, B.P.; Leclercq, C.; Birgersdotter-Green, U.M.; Wiggenhorn, C.; et al. Patient-reported quality of life and acceptance of the extravascular implantable cardioverter-defibrillator: Results from pivotal study. J. Cardiovasc. Electrophysiol. 2024, 35, 240–246. [Google Scholar] [CrossRef]
- Friedman, P.; Murgatroyd, F.; Boersma, L.V.; Manlucu, J.; O’donnell, D.; Knight, B.P.; Clémenty, N.; Leclercq, C.; Amin, A.; Merkely, B.P.; et al. Efficacy and Safety of an Extravascular Implantable Cardioverter–Defibrillator. N. Engl. J. Med. 2022, 387, 1292–1302. [Google Scholar] [CrossRef]
- Lloyd, M.S.; Brisben, A.J.; Reddy, V.Y.; Blomström-Lundqvist, C.; Boersma, L.V.; Bongiorni, M.G.; Burke, M.C.; Cantillon, D.J.; Doshi, R.; Friedman, P.A.; et al. Design and rationale of the MODULAR ATP global clinical trial: A novel intercommunicative leadless pacing system and the subcutaneous implantable cardioverter-defibrillator. Heart Rhythm O2 2023, 4, 448–456. [Google Scholar] [CrossRef]
- Breeman, K.T.; Swackhamer, B.; Brisben, A.J.; Quast, A.-F.B.; Carter, N.; Shuros, A.; Soltis, B.; Koop, B.E.; Burke, M.C.; Wilde, A.A.; et al. Long-term performance of a novel communicating antitachycardia pacing–enabled leadless pacemaker and subcutaneous implantable cardioverter-defibrillator system: A comprehensive preclinical study. Heart Rhythm 2022, 19, 837–846. [Google Scholar] [CrossRef]
- ID NCT04798768. Available online: https://clinicaltrials.gov/ (accessed on 1 January 2024).
- Keene, D.; Shun-Shin, M.J.; Arnold, A.D.; Howard, J.P.; Lefroy, D.; Davies, D.W.; Lim, P.B.; Ng, F.S.; Koa-Wing, M.; Qureshi, N.A.; et al. Quantification of Electromechanical Coupling to Prevent Inappropriate Implantable Cardioverter-Defibrillator Shocks. JACC Clin. Electrophysiol. 2019, 5, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Noordman, A.B.; Rienstra, M.; Blaauw, Y.; Tieleman, R.; Maass, A.H. Reducing inappropriate and unnecessary implantable cardioverter-defibrillator therapy: Is patient confirmation via a mobile application the solution? Heart Rhythm. 2023, 4, 815–819. [Google Scholar] [CrossRef] [PubMed]
- Boulé, S.; Brigadeau, F.; Marquié, C.; Salleron, J.; Klug, D.; Kouakam, C.; Guédon-Moreau, L.; Duhamel, A.; Acheré, C.; Wissocque, L.; et al. Basal exit site of clinical ventricular tachycardia is an independent predictor of antitachycardia pacing failure in implantable cardioverter-defibrillators recipients. Pacing Clin. Electrophysiol. 2012, 35, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
- Qian, S.; Connolly, A.; Mendonca-Costa, C.; Campos, F.; Rodero, C.; Whitaker, J.; ARinaldi, C.; Bishop, M.J. Optimization of anti-tachycardia pacing efficacy through scar-specific delivery and minimization of re-initiation: A virtual study on a cohort of infarcted porcine hearts. Europace 2023, 25, 716–725. [Google Scholar] [CrossRef]
- Hirahara, A.M.; Khan, M.S.; Gharbia, O.A.; Lange, M.; Ishidoya, Y.; Smego, D.; Ranjan, R.; Stoddard, G.J.; Selzman, C.H.; Dosdall, D.J. Antitachycardia pacing at the His bundle is safer than conventional right ventricular antitachycardia pacing in a canine myocardial ischemic injury model. J. Cardiovasc. Electrophysiol. 2023, 34, 1249–1256. [Google Scholar] [CrossRef]
- Miyazawa, A. Conduction system pacing as a novel therapeutic approach in ventricular tachycardia: Improving hemodynamics and terminating VT. In Proceedings of the Heart Rhythm Congress, New Orleans, LA, USA, 19–21 May 2023. Abstract 56. [Google Scholar]
- Crossley, G.H.; Sanders, P.; De Filippo, P.; Tarakji, K.G.; Hansky, B.; Shah, M.; Mason, P.; Maus, B.; Holloman, K. Rationale and design of the Lead Evaluation for Defibrillation and Reliability study: Safety and efficacy of a novel ICD lead design. J. Cardiovasc. Electrophysiol. 2023, 34, 257–267, Erratum in J. Cardiovasc. Electrophysiol. 2023, 34, 2011. [Google Scholar] [CrossRef]
- Huybrechts, W.L.; Bergonti, M.; Saenen, J.B.; Miljoen, H.; Van Leuven, O.; Van Assche, L.; Van Herck, P.; Wittock, A.; De Cleen, D.; Sarkozy, A.; et al. Left Bundle Branch Area Defibrillator (LBBAD): A First-in-Human Feasibility Study. JACC Clin. Electrophysiol. 2023, 9, 620–627. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leong, A.M.; Arnold, A.D.; Whinnett, Z.I. Implantable Cardioverter Defibrillator Tachycardia Therapies: Past, Present and Future Directions. J. Cardiovasc. Dev. Dis. 2024, 11, 92. https://doi.org/10.3390/jcdd11030092
Leong AM, Arnold AD, Whinnett ZI. Implantable Cardioverter Defibrillator Tachycardia Therapies: Past, Present and Future Directions. Journal of Cardiovascular Development and Disease. 2024; 11(3):92. https://doi.org/10.3390/jcdd11030092
Chicago/Turabian StyleLeong, Andrew M., Ahran D. Arnold, and Zachary I. Whinnett. 2024. "Implantable Cardioverter Defibrillator Tachycardia Therapies: Past, Present and Future Directions" Journal of Cardiovascular Development and Disease 11, no. 3: 92. https://doi.org/10.3390/jcdd11030092