
Short-Term Mortality in Hospitalized Patients with Congestive Heart Failure: Markers of Thrombo-Inflammation Are Independent Risk Factors and Only Weakly Associated with Renal Insufficiency and Co-Morbidity Burden
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Definition of CHF
2.3. Data Selection
2.4. Statistical Analysis
3. Results
3.1. Univariate Analysis of Factors Associated with 28-Day Mortality
3.2. Bivariate Relationship between Charlson Co-Morbidity Index, eGFR, and Thrombo-Inflammatory Biomarkers
3.3. Multivariate Analysis of Factors Independently Associated with 28-Day Mortality
4. Discussion
Study Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yan, T.; Zhu, S.; Yin, X.; Xie, C.; Xue, J.; Zhu, M.; Weng, F.; Zhu, S.; Xiang, B.; Zhou, X.; et al. Burden, Trends, and Inequalities of Heart Failure Globally, 1990 to 2019: A Secondary Analysis Based on the Global Burden of Disease 2019 Study. J. Am. Heart Assoc. 2023, 12, e027852. [Google Scholar] [CrossRef]
- Cunningham, L.C.; Fonarow, G.C.; Yancy, C.W.; Sheng, S.; Matsouaka, R.A.; Devore, A.D.; Jneid, H.; Deswal, A. Regional variations in heart failure quality and outcomes: Get with the guidelines—Heart failure registry. J. Am. Heart Assoc. 2021, 10, e018696. [Google Scholar] [CrossRef]
- Ambrosy, A.P.; Fonarow, G.C.; Butler, J.; Chioncel, O.; Greene, S.J.; Vaduganathan, M.; Nodari, S.; Lam, C.S.P.; Sato, N.; Shah, A.N. The global health and economic burden of hospitalizations for heart failure: Lessons learned from hospitalized heart failure registries. J. Am. Coll. Cardiol. 2014, 63, 1123–1133. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Savarese, G.; Becher, P.M.; Lund, L.H.; Seferovic, P.; Rosano, G.M.C.; Coats, A.J.S. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc. Res. 2022, 118, 3272–3287. [Google Scholar] [CrossRef] [PubMed]
- Chioncel, O.; Lainscak, M.; Seferovic, P.M.; Anker, S.D.; Crespo-Leiro, M.G.; Harjola, V.-P.; Parissis, J.; Laroche, C.; Piepoli, M.F.; Fonseca, C.; et al. Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: An analysis of the ESC Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2017, 19, 1574–1585. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/ejhf.813 (accessed on 27 January 2024). [CrossRef] [PubMed]
- Minhas, A.M.K.; Ijaz, S.H.; Jamal, S.; Dani, S.S.; Khan, M.S.; Greene, S.J.; Fudim, M.; Warraich, H.J.; Shapiro, M.D.; Virani, S.S. Trends in characteristics and outcomes in primary heart failure hospitalizations among older population in the United States, 2004 to 2018. Circ. Heart Fail. 2022, 15, e008943. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Gupta, A.; Sharma, T.; Gupta, R. New horizons in the management of heart failure. J. Evid. Based Med. Healthc. 2016, 3, 1604–1607. [Google Scholar] [CrossRef] [PubMed]
- Norhammar, A.; Bodegard, J.; Vanderheyden, M.; Tangri, N.; Karasik, A.; Maggioni, A.P.; Sveen, K.A.; Taveira-Gomes, T.; Botana, M.; Hunziker, L.; et al. Prevalence, outcomes and costs of a contemporary, multinational population with heart failure. Heart 2023, 109, 548. [Google Scholar] [CrossRef] [PubMed]
- Havranek, E.P.; Wolfe, P.; Masoudi, F.A.; Rathore, S.S.; Krumholz, H.M.; Ordin, D.L. Provider and hospital characteristics associated with geographic variation in the evaluation and management of elderly patients with heart failure. Arch. Intern. Med. 2004, 164, 1186–1191. Available online: https://www.semanticscholar.org/paper/Provider-and-hospital-characteristics-associated-in-Havranek-Wolfe/5fae66ace47a73cfe1335da73fd3b2bc373d1f05 (accessed on 27 January 2024). [CrossRef] [PubMed]
- Yu, Y.; Gupta, A.; Wu, C.; Masoudi, F.A.; Du, X.; Zhang, J.; Krumholz, H.M.; Li, J. Characteristics, Management, and Outcomes of Patients Hospitalized for Heart Failure in China: The China PEACE Retrospective Heart Failure Study. J. Am. Heart Assoc. 2019, 8, e012884. [Google Scholar] [CrossRef]
- Crespo-Leiro, M.G.; Anker, S.D.; Maggioni, A.P.; Coats, A.J.; Filippatos, G.; Ruschitzka, F.; Ferrari, R.; Piepoli, M.F.; Delgado Jimenez, J.F.; Metra, M.; et al. European Society of Cardiology Heart Failure Long-Term Registry (ESC-HF-LT): 1-year follow-up outcomes and differences across regions. Eur. J. Heart Fail. 2016, 18, 613–625. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Adams, K.F.; Abraham, W.T.; Yancy, C.W.; Boscardin, W.J.; ADHERE Scientific Advisory Committee, Study Group, and Investigators. The Risk Stratification for In-Hospital Risk Stratification for In-Hospital Mortality in Acutely Decompensated Heart FailureClassification and Regression Tree Analysis. JAMA 2005, 293, 572–580. [Google Scholar] [CrossRef]
- Heywood, J.T. The cardiorenal syndrome: Lessons from the ADHERE database and treatment options. Heart Fail. Rev. 2004, 9, 195–201. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Filippatos, G. Reassessing treatment of acute heart failure syndromes: The ADHERE Registry. Eur. Heart J. Suppl. 2005, 7 (Suppl. B), B13–B19. [Google Scholar] [CrossRef]
- Fonarow, G.C. Epidemiology and risk stratification in acute heart failure. Am. Heart J. 2008, 155, 200–207. Available online: https://www.sciencedirect.com/science/article/pii/S0002870307008241 (accessed on 27 January 2024). [CrossRef]
- Gregg, C.; Fonarow, T.B.H. Combining Natriuretic Peptides and Necrosis Markers in Determining Prognosis in Heart Failure. Rev. Cardiovasc. Med. 2003, 4, 20–28. [Google Scholar]
- Fonarow, G.C.; Peacock, W.F.; Phillips, C.O.; Givertz, M.M.; Lopatin, M. Admission B-type natriuretic peptide levels and in-hospital mortality in acute decompensated heart failure. J. Am. Coll. Cardiol. 2007, 49, 1943–1950. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W.; Lopatin, M.; Stevenson, L.W.; De Marco, T.; Fonarow, G.C. Clinical presentation, management, and in-hospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: A report from the Acute Decompensated Heart Failure National Registry (ADHERE) Database. J. Am. Coll. Cardiol. 2006, 47, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Adams, K.F.; Fonarow, G.C.; Emerman, C.L.; LeJemtel, T.H.; Costanzo, M.R.; Abraham, W.T.; Berkowitz, R.L.; Galvao, M.; Horton, D.P. Characteristics and outcomes of patients hospitalized for heart failure in the United States: Rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am. Heart J. 2005, 149, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Gheorghiade, M.; Abraham, W.T.; Albert, N.M.; Gattis Stough, W.; Greenberg, B.H.; O’Connor, C.M.; She, L.; Yancy, C.W.; Young, J.; Fonarow, G.C.; et al. Relationship between admission serum sodium concentration and clinical outcomes in patients hospitalized for heart failure: An analysis from the OPTIMIZE-HF registry. Eur. Heart J. 2007, 28, 980–988. [Google Scholar] [CrossRef]
- Patel, R.B.; Fonarow, G.C.; Greene, S.J.; Zhang, S.; Alhanti, B.; DeVore, A.D.; Butler, J.; Heidenreich, P.A.; Huang, J.C.; Kittleson, M.M.; et al. Kidney Function and Outcomes in Patients Hospitalized with Heart Failure. J. Am. Coll. Cardiol. 2021, 78, 330–343. [Google Scholar] [CrossRef] [PubMed]
- Sartipy, U.; Dahlström, U.; Edner, M.; Lund, L.H. Predicting Survival in Heart Failure: Validation of the MAGGIC Heart Failure Risk Score in 51043 Patients From the Swedish Heart Failure Registry. Eur. J. Heart Fail. 2014, 16, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Sarraf, M.; Masoumi, A.; Schrier, R.W. Cardiorenal Syndrome in Acute Decompensated Heart Failure. Clin. J. Am. Soc. Nephrol. 2009, 4, 2013–2026. [Google Scholar] [CrossRef] [PubMed]
- Dahlen, B.; Schulz, A.; Göbel, S.; Tröbs, S.-O.; Schwuchow-Thonke, S.; Spronk, H.M.; Prochaska, J.H.; Arnold, N.; Lackner, K.J.; Gori, T.; et al. The impact of platelet indices on clinical outcome in heart failure: Results from the MyoVasc study. ESC Heart Fail. 2021, 8, 2991–3001. [Google Scholar] [CrossRef] [PubMed]
- Çakır, M.O. The Prognostic Significance of Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio for Long-Term Survival in Patients with Severe Left Ventricular Dysfunction and Implantable Cardioverter Defibrillator. Cureus 2023, 15, e47441. [Google Scholar] [CrossRef]
- Colombo, P.C.; Ganda, A.; Lin, J.; Onat, D.; Harxhi, A.; Iyasere, J.E.; Uriel, N.; Cotter, G. Inflammatory Activation: Cardiac, Renal, and Cardio-Renal Interactions in Patients with the Cardiorenal Syndrome. Heart Fail. Rev. 2012, 17, 177–190. [Google Scholar] [CrossRef]
- von Haehling, S.; Schefold, J.C.; Lainščak, M.; Doehner, W.; Anker, S.D. Inflammatory Biomarkers in Heart Failure Revisited: Much More Than Innocent Bystanders. Heart Fail Clin. 2009, 5, 549–560. [Google Scholar] [CrossRef]
- Yasemin, K.A.Y.A.; Ahmet, K.A.Y.A.; Akkaya, F.; Filiz, M. The Relationship between Recurrent Hospitalization and Inflammation in Heart Failure Patients. ODÜ Tıp Derg. 2023, 10, 1–7. [Google Scholar]
- Zorlu, A.; Yilmaz, M.B.; Yucel, H.; Bektasoglu, G.; Refiker Ege, M.; Tandogan, I. Increased d-dimer levels predict cardiovascular mortality in patients with systolic heart failure. J. Thromb. Thrombolysis 2012, 33, 322–328. [Google Scholar] [CrossRef]
- Huang, B.; Li, Y.J.; Shen, J.; Yang, Y.; Liu, G.; Luo, S.X. D-dimer level and long-term outcome in patients with end-stage heart failure secondary to idiopathic dilated cardiomyopathy. J. Geriatr. Cardiol. 2019, 16, 621–629. [Google Scholar] [CrossRef]
- Zhang, Z.; Cao, L.; Chen, R.; Zhao, Y.; Lv, L.; Xu, Z.; Xu, P. Electronic healthcare records and external outcome data for hospitalized patients with heart failure. Sci. Data 2021, 8, 46. [Google Scholar] [CrossRef]
- Douma, R.A.; Le Gal, G.; Söhne, M.; Righini, M.; Kamphuisen, P.W.; Perrier, A.; Kruip, M.J.; Bounameaux, H.; Büller, H.R.; Roy, P.M. Potential of an age adjusted D-dimer cut-off value to improve the exclusion of pulmonary embolism in older patients: A retrospective analysis of three large cohorts. BMJ 2010, 340, c1475. [Google Scholar] [CrossRef]
- Shebeshi, D.S.; Dolja-Gore, X.; Byles, J. Charlson Co-morbidity Index as a predictor of repeated hospital admission and mortality among older women diagnosed with cardiovascular disease. Aging Clin. Exp. Res. 2021, 33, 2873–2878. [Google Scholar] [CrossRef]
- Li, C. Little’s Test of Missing Completely at Random. Stata J. 2013, 13, 795–809. [Google Scholar] [CrossRef]
- Kalogeropoulos, A.; Georgiopoulou, V.; Psaty, B.M.; Rodondi, N.; Smith, A.L.; Harrison, D.G.; Liu, Y.; Hoffmann, U.; Bauer, D.C.; Newman, A.B.; et al. Inflammatory Markers and Incident Heart Failure Risk in Older Adults. J. Am. Coll. Cardiol. 2010, 55, 2129–2137. [Google Scholar] [CrossRef]
- Taube, A.; Schlich, R.; Sell, H.; Eckardt, K.; Eckel, J. Inflammation and metabolic dysfunction: Links to cardiovascular diseases. Am. J. Physiol. -Heart Circ. Physiol. 2012, 302, H2148–H2165. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.S.; Lyass, A.; Kraigher-Krainer, E.; Massaro, J.M.; Lee, D.S.; Ho, J.E.; Levy, D.; Redfield, M.M.; Pieske, B.M.; Benjamin, E.J.; et al. Cardiac dysfunction and noncardiac dysfunction as precursors of heart failure with reduced and preserved ejection fraction in the community. Circulation 2011, 124, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Paulus, W.J.; Tschöpe, C. A Novel Paradigm for Heart Failure with Preserved Ejection Fraction: Co-morbidities Drive Myocardial Dysfunction and Remodeling through Coronary Microvascular Endothelial Inflammation. J. Am. Coll. Cardiol. 2013, 62, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Libby, P. Inflammation in atherosclerosis. Nature 2002, 420, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Arnold, N.; Lechner, K.; Waldeyer, C.; Shapiro, M.D.; Koenig, W. Inflammation and Cardiovascular Disease: The Future. Eur. Cardiol. Rev. 2021, 16, e20. [Google Scholar] [CrossRef]
- Murphy, S.P.; Kakkar, R.; McCarthy, C.P.; Januzzi, J.L. Inflammation in Heart Failure: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 1324–1340. [Google Scholar] [CrossRef]
- Cugno, M.; Mari, D.; Meroni, P.L.; Gronda, E.; Vicari, F.; Frigerio, M.; Coppola, R.; Bottasso, B.; Borghi, M.O.; Gregorini, L. Haemostatic and Inflammatory Biomarkers in Advanced Chronic Heart Failure: Role of Oral Anticoagulants and Successful Heart Transplantation. Br. J. Haematol. 2004, 126, 85–92. [Google Scholar] [CrossRef]
- Suetomi, T.; Miyamoto, S.; Brown, J.H. Inflammation in nonischemic heart disease: Initiation by cardiomyocyte CaMKII and NLRP3 inflammasome signaling. Am. J. Physiol.-Heart Circ. Physiol. 2019, 317, H877–H890. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, E.A.; Ponikowski, P.; Piepoli, M.F.; Banasiak, W.; Anker, S.D.; Poole-Wilson, P.A. Autonomic imbalance and immune activation in chronic heart failure–pathophysiological links. Cardiovasc. Res. 2006, 70, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Tromp, J.; Westenbrink, B.D.; Ouwerkerk, W.; van Veldhuisen, D.J.; Samani, N.J.; Ponikowski, P.; Metra, M.; Anker, S.D.; Cleland, J.G.; Dickstein, K.; et al. Identifying Pathophysiological Mechanisms in Heart Failure with Reduced Versus Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2018, 72, 1081–1090. [Google Scholar] [CrossRef] [PubMed]
- Higashikuni, Y.; Liu, W.; Numata, G.; Tanaka, K.; Fukuda, D.; Tanaka, Y.; Hirata, Y.; Imamura, T.; Takimoto, E.; Komuro, I. NLRP3 inflammasome activation through heart-brain interaction initiates cardiac inflammation and hypertrophy during pressure overload. Circulation 2023, 147, 338–355. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F. Immune activation and inflammatory system in chronic heart failure: Novel pathophysiological hypotheses generate new therapeutic options. Int. J. Clin. Pract. 2007, 61, 536–538. [Google Scholar] [CrossRef]
- Getawa, S.; Bayleyegn, B. Platelet, Neutrophil and Lymphocyte Quantitative Abnormalities in Patients with Heart Failure: A Retrospective Study. Vasc. Health Risk Manag. 2023, 19, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Majmundar, M.; Kansara, T.; Park, H.; Ibarra, G.; Marta Lenik, J.; Shah, P.; Kumar, A.; Doshi, R.; Zala, H.; Chaudhari, S.; et al. Absolute lymphocyte count as a predictor of mortality and readmission in heart failure hospitalization. Int. J. Cardiol. Heart Vasc. 2022, 39, 100981. [Google Scholar] [CrossRef]
- Wu, C.C.; Wu, C.H.; Lee, C.H.; Cheng, C.I. Association between neutrophil percentage-to-albumin ratio (NPAR), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and long-term mortality in community-dwelling adults with heart failure: Evidence from US NHANES 2005–2016. BMC Cardiovasc. Disord. 2023, 23, 312. [Google Scholar] [CrossRef]
- Haybar, H.; Pezeshki, S.M.S.; Saki, N. Evaluation of complete blood count parameters in cardiovascular diseases: An early indicator of prognosis? Exp. Mol. Pathol. 2019, 110, 104267. [Google Scholar] [CrossRef]
- Huang, W.; Cheng, H.; Huang, C.C.; Guo, C.-Y.; Lu, D.Y.; Lee, C.-W.; Hsu, P.; Yu, W.C.; Chen, C.H.; Sung, S.H. Hemographic Indices Are Associated with Mortality in Acute Heart Failure. Sci. Rep. 2017, 7, 17828. [Google Scholar] [CrossRef] [PubMed]
- Jablonska, E.; Jablonski, J.; Holownia, A. Role of neutrophils in release of some cytokines and their soluble receptors. Immunol. Lett. 2000, 70, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Nijm, J.; Wikby, A.; Tompa, A.; Olsson, A.G.; Jonasson, L. Circulating levels of pro-inflammatory cytokines and neutrophil-platelet aggregates in patients with coronary artery disease. Am. J. Cardiol. 2005, 95, 452–456. [Google Scholar] [CrossRef]
- Garraud, O.; Hamzeh-Cognasse, H.; Cognasse, F. Platelets and cytokines: How and why? Transfus. Clin. Biol. 2012, 19, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Pennings, G.J.; Reddel, C.J.; Traini, M.; Lam, M.; Kockx, M.; Chen, V.; Kritharides, L. Rapid Release of Interleukin-1β From Human Platelets Is Independent of NLRP3 and Caspase. Thromb. Haemost. 2022, 122, 517–528. [Google Scholar] [CrossRef]
- Lindemann, S.; Tolley, N.D.; Dixon, D.A.; McIntyre, T.M.; Prescott, S.M.; Zimmerman, G.A.; Weyrich, A.S. Activated Platelets Mediate Inflammatory Signaling by Regulated Interleukin 1β Synthesis. J. Cell Biol. 2001, 154, 485–490. [Google Scholar] [CrossRef]
- Intan, R.E.; Alkaff, F.F.; Oktaviono, Y.H.; Nugraha, R.A.; Octora, T.N.; Jonatan, M.; Balti, D.R.; Hasibuan, F.S.; Radi, B.; Santoso, A. Retrospective Study of the Association between Platelet-to-Lymphocyte Ratio in Patients with Acute Coronary Syndrome on Admission to a Rural Referral Center in East Java, Indonesia, and the Incidence of New Symptomatic Heart Failure at 6 Months. Med. Sci. Monit. 2022, 28, e935002. [Google Scholar] [CrossRef]
- Benites-Zapata, V.A.; Hernandez, A.V.; Nagarajan, V.; Cauthen, C.A.; Starling, R.C.; Tang, W.H.W. Usefulness of neutrophil-to-lymphocyte ratio in risk stratification of patients with advanced heart failure. Am. J. Cardiol. 2015, 115, 57–61. [Google Scholar] [CrossRef]
- Pourafkari, L.; Wang, C.K.; Tajlil, A.; Afshar, A.H.; Schwartz, M.; Nader, N.D. Platelet-lymphocyte ratio in prediction of outcome of acute heart failure. Biomark. Med. 2018, 12, 63–70. [Google Scholar] [CrossRef]
- Heidarpour, M.; Bashiri, S.; Vakhshoori, M.; Heshmat-Ghahdarijani, K.; Khanizadeh, F.; Ferdowsian, S.; Shafie, D. The Association between Platelet-to-Lymphocyte Ratio with Mortality among Patients Suffering from Acute Decompensated Heart Failure. BMC Cardiovasc. Disord. 2021, 21, 454. [Google Scholar] [CrossRef]
- Ye, G.; Chen, Q.; Chen, X.; Liu, Y.; Yin, T.; Meng, Q.; Liu, Y.; Wei, H.; Zhou, Q. The Prognostic Role of Platelet-to-Lymphocyte Ratio in Patients with Acute Heart Failure: A Cohort Study. Sci Rep. 2019, 9, 10639. [Google Scholar] [CrossRef] [PubMed]
- Durmus, E.; Kivrak, T.; Gerin, F.; Sunbul, M.; Sari, I.; Erdogan, O. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio are Predictors of Heart Failure. Arq. Bras. Cardiol. 2015, 105, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Delcea, C.; Buzea, C.A.; Vîjan, A.E.; Bădilă, E.; Dan, G.A. The Platelet to Lymphocyte Ratio in Heart Failure: A Comprehensive Review. Rom. J. Intern. Med. 2023, 61, 84–97. [Google Scholar] [CrossRef] [PubMed]
- Demir, M.; Duyuler, P.T.; Guray, U.; Celik, M.C. Platelet to Lymphocyte Ratio on Admission and Prognosis in Patients with Acute Cardiogenic Pulmonary Edema. J. Emerg. Med. 2018, 55, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.; Qu, W.; Zhang, L.; Liu, M.; Gao, X.; Gao, Y.; Cheng, X.; Xu, W.; Liu, Y. Role of blood urea nitrogen in predicting the post-discharge prognosis in elderly patients with acute decompensated heart failure. Sci. Rep. 2018, 8, 13507. [Google Scholar] [CrossRef]
- Brisco, M.A.; Zile, M.R.; Hanberg, J.S.; Wilson, F.P.; Parikh, C.R.; Coca, S.G.; Tang, W.H.W.; Testani, J.M. Relevance of Changes in Serum Creatinine During a Heart Failure Trial of Decongestive Strategies: Insights from the DOSE Trial. J. Card. Fail. 2016, 22, 753–760. [Google Scholar] [CrossRef]
- Xanthopoulos, A.; Starling, R.C.; Kitai, T.; Triposkiadis, F. Heart Failure and Liver Disease: Cardiohepatic Interactions. JACC Heart Fail. 2019, 7, 87–97. [Google Scholar] [CrossRef]
- Fortea, J.I.; Puente, Á.; Cuadrado, A.; Huelin, P.; Pellón, R.; González Sánchez, F.J.; Mayorga, M.; Cagigal, M.L.; García Carrera, I.; Cobreros, M.; et al. Congestive Hepatopathy. Int. J. Mol. Sci. 2020, 21, 9420. [Google Scholar] [CrossRef]
- Nikolaou, M.; Mebazaa, A. Cardiohepatic interactions in heart failure: Clinical and therapeutic implications. Contin. Cardiol. Educ. 2017, 3, 117–120. [Google Scholar] [CrossRef]


{kind=link}
| Survivors (N = 1971) | Non-Survivors (N = 37) | p-Value | |
|---|---|---|---|
| Clinical variables | |||
| PULSE (beat/min) | 82 (70, 98) | 88 (70, 102) | 0.28 |
| SBP (mm Hg) | 130 (114, 147) | 126 (100, 141) | 0.15 |
| DBP (mm Hg) | 76 (66, 85) | 72 (60,84) | 0.13 |
| MAP | 93 (83, 104) | 90 (75, 99) | 0.1 |
| BMI | 21 (18.5, 23) | 21 (18, 23) | 0.7 |
| CHARLSON INDEX | 2 (1, 2) | 2 (1, 3) | 0.1 |
| Laboratory variables | |||
| URIC ACID (mg/dL) | 7.7 (6.0, 9.6) | 10 (7.0, 13) | 0.00001 |
| eGFR (mL/min) | 65 (42, 90) | 34 (16–65) | 0.00001 |
| CYSTATIN C (mg/L) | 1.5 (1.2, 2.2) | 2.4 (1.6, 4.3) | 0.00001 |
| WBC COUNT (109/L) | 6.5 (5, 8.6) | 9.2 (6.3, 11.3) | 0.001 |
| HEMATOCRIT (%) | 36 (32, 40) | 35 (24–40) | 0.2 |
| LYMPHOCYTE COUNT (109/L) | 0.9 (0.6, 1.3) | 0.83 (0.4, 1.2) | 0.1 |
| HEMOGLOBIN (g/dL) | 11.7 (10, 13) | 11 (7.8, 13.3) | 0.12 |
| PLATELET COUNT (109/L) | 134 (101, 176) | 178 (114, 239) | 0.005 |
| NEUTROPHIL COUNT (109/L) | 4.9 (3.6, 6.7) | 7.3 (5, 10) | 0.00001 |
| THROMBIN TIME | 17 (16, 18) | 18 (17, 18) | 0.003 |
| FIBRINOGEN (mg/dL) | 300 (250, 370) | 360 (270, 450) | 0.04 |
| HIGH-SENSITIVITY TROPONIN (pg/mL) | 0.05 (0.023, 0.12) | 0.13 (0.08, 0.23) | 0.00001 |
| CALCIUM (mg/dL) | 9.2 (8.8, 9.6) | 8.8 (8.4, 9.2) | 0.003 |
| POTASSIUM (mEq/L) | 3.9 (3.5, 4.3) | 4.5 (3.8, 5.3) | 0.00001 |
| SODIUM (mEq/L) | 139 (136, 141) | 136 (133, 139) | 0.001 |
| BNP (pg/mL) | 744 (300, 1726) | 1448 (741, 3387) | 0.001 |
| CRP (mg/L) | 9.2 (3.9, 29) | 43 (8, 77) | 0.004 |
| ALBUMIN (g/dL) | 3.7 (3.3, 4.0) | 3.4 (3.2, 3.7) | 0.004 |
| CREATININE (mg/dL) | 0.98 (0.73, 1.4) | 1.8 (1.0, 3.2) | 0.00001 |
| BUN (mg/dL) | 48 (35, 68) | 94 (55, 139) | 0.00001 |
| D-DIMER (ng/mL) | 1200 (790, 2130) | 3055 (1385, 10,142) | 0.00001 |
| AGE-ADJUSTED D-DIMER (ng/mL) | 753 (500, 1355) | 1853 (1045, 5698) | 0.00001 |
| NEUTROPHIL/LYMPHOCYTE RATIO (NLR) | 5.1 (3.2, 8.5) | 8.3 (5.6–19.4) | 0.57 |
| PLATELET/LYMPHOCYTE RATIO (PLR) | 145 (96, 223) | 235 (132, 379) | 0.0001 |
| Survivors (N = 1971) | Non-Survivors (N = 37) | p-Value | Odds Ratio | 95% CI | |
|---|---|---|---|---|---|
| AGE ≥ 69 | 1434 (73%) | 28 (76%) | 0.69 | 1.16 | 0.55–2.5 |
| GENDER (M) | 824 (42%) | 21 (57%) | 0.07 | 1.83 | 0.95–3.52 |
| NYHA > 2 | 1619 (82%) | 36 (%) | 0.014 | 7.82 | 1.07–57 |
| BIVENTRICULAR HEART FAILURE | 1453 (74%) | 27 (73%) | 0.57 | ||
| LEFT HEART FAILURE | 467 (24%) | 10 (27%) | 0.57 | ||
| RIGHT HEART FAILURE | 51 (2.6%) | 0 | 0.57 | ||
| HYPERTENSION (SBP ≥ 140 mm Hg) | 743 (38) | 13 (35%) | 0.75 | 0.89 | 0.45–1.8 |
| ACUTE MI | 140 (7.1%) | 3 (8%) | 0.74 | 1.15 | 0.35–3.8 |
| NEW DIAGNOSIS OF CHF | 132 (7%) | 4 (11%) | 0.32 | 1.66 | 0.6–4.6 |
| PVD | 99 (5%) | 2 (5%) | 0.71 | 1.1 | 0.26–4.5 |
| CEREBROVASCULAR DISEASE | 145 (7.4%) | 5 (13.5%) | 0.19 | 1.97 | 0.75–5.13 |
| COPD | 231 (12%) | 2 (5.4%) | 0.31 | 0.43 | 0.10–1.80 |
| CAD (Surrogate) | 715 (36%) | 15 (40%) | 0.59 | 1.2 | 0.61–2.3 |
| DIABETES | 458 (23%) | 8 (22%) | 1 | 0.91 | 0.41–2.0 |
| MODERATE-TO-SEVERE CKD | 455 (23%) | 19 (51%) | 0.00001 | 3.5 | 1.8–6.7 |
| CHRONIC LIVER DISEASE | 78 (4%) | 6 (16%) | 0.004 | 4.7 | 1.9–11.6 |
| ACUTE RENAL FAILURE | 5 (0.3%) | 2 (5.4) | 0.007 | 22.5 | 4.2–120 |
| Pearson Correlation Coefficient | p | |
|---|---|---|
| Charlson co-morbidity index | 1 | |
| Lymphocyte count | −0.040 | 0.078 |
| Platelet count | −0.010 | 0.66 |
| Neutrophil count | 0.106 | 0.001 |
| Thrombin time | 0.036 | 0.173 |
| Fibrinogen | 0.072 | 0.001 |
| D-dimer | 0.036 | 0.127 |
| NLR | 0.10 | 0.00001 |
| CRP | 0.10 | 0.00001 |
| PLR | 0.072 | 0.001 |
| Pearson Correlation Coefficient | p | |
|---|---|---|
| eGFR | 1 | |
| Lymphocyte count | 0.12 | 0.00001 |
| Platelet count | 0.04 | 0.10 |
| Neutrophil count | −0.10 | 0.00001 |
| Thrombin time | −0.01 | 0.60 |
| Fibrinogen | −0.04 | 0.07 |
| D-dimer | −0.12 | 0.00001 |
| NLR | 0.14 | 0.00001 |
| CRP | −0.07 | 0.001 |
| PLR | −0.07 | 0.00001 |
| Beta | SE | Sig. | HR | 95% CI | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Thrombin time (s) | 0.024 | 0.006 | 0.0001 | 1.02 | 1.012 | 1.038 |
| Creatinine (mg/dL) | 0.277 | 0.112 | 0.0131 | 1.32 | 1.060 | 1.642 |
| D-dimer (ng/mL) * | 0.000 | 0.000 | 0.0012 | 1.00 | 1.000 | 1.000 |
| Urea (mg/dL) | 0.012 | 0.004 | 0.0018 | 1.01 | 1.004 | 1.020 |
| Platelet/lymphocyte ratio | 0.003 | 0.001 | 0.0001 | 1.003 | 1.001 | 1.004 |
| Liver disease | 1.654 | 0.471 | 0.0004 | 5.23 | 2.078 | 13.166 |
| NYHA > 2 | 2.413 | 1.057 | 0.0224 | 11.17 | 1.408 | 88.579 |
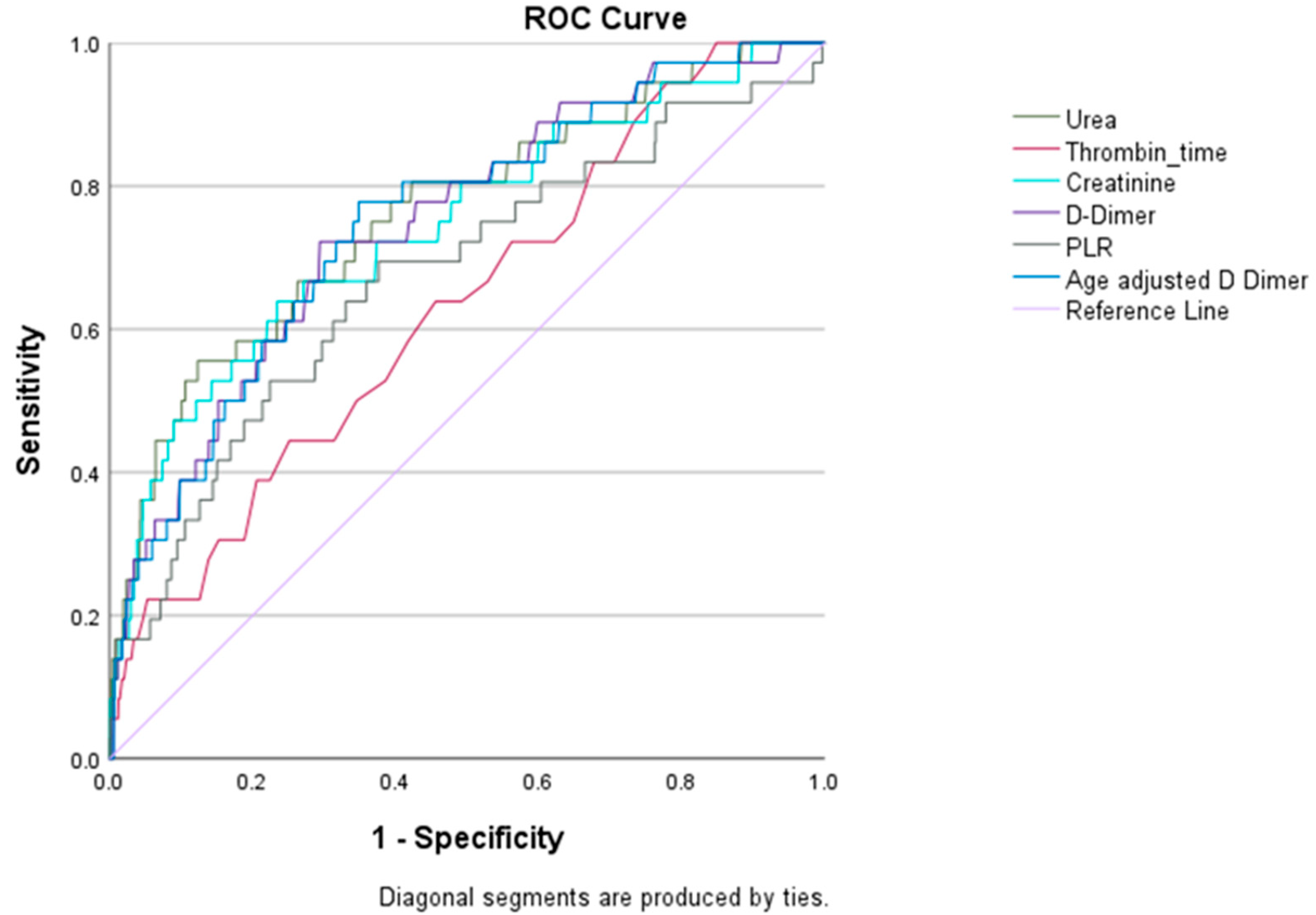
| Variables | Sensitivity | Specificity |
|---|---|---|
| Urea | 0.56 | 0.87 |
| Thrombin time | 0.46 | 0.75 |
| Creatinine | 0.68 | 0.72 |
| D-dimer | 0.72 | 0.71 |
| Platelet/lymphocyte ratio | 0.68 | 0.62 |
| Age-adjusted D-dimer | 0.72 | 0.66 |
| NYHA class > 2 | 0.97 | 0.18 |
| Liver disease | 0.16 | 0.97 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iglesias, J.; Okoh, N.; Ang, S.P.; Rodriguez, C.A.; Chia, J.E.; Levine, J.S. Short-Term Mortality in Hospitalized Patients with Congestive Heart Failure: Markers of Thrombo-Inflammation Are Independent Risk Factors and Only Weakly Associated with Renal Insufficiency and Co-Morbidity Burden. J. Cardiovasc. Dev. Dis. 2024, 11, 93. https://doi.org/10.3390/jcdd11030093
Iglesias J, Okoh N, Ang SP, Rodriguez CA, Chia JE, Levine JS. Short-Term Mortality in Hospitalized Patients with Congestive Heart Failure: Markers of Thrombo-Inflammation Are Independent Risk Factors and Only Weakly Associated with Renal Insufficiency and Co-Morbidity Burden. Journal of Cardiovascular Development and Disease. 2024; 11(3):93. https://doi.org/10.3390/jcdd11030093
Chicago/Turabian StyleIglesias, Jose, Nelson Okoh, Song Peng Ang, Cristina A. Rodriguez, Jia Ee Chia, and Jerrold S. Levine. 2024. "Short-Term Mortality in Hospitalized Patients with Congestive Heart Failure: Markers of Thrombo-Inflammation Are Independent Risk Factors and Only Weakly Associated with Renal Insufficiency and Co-Morbidity Burden" Journal of Cardiovascular Development and Disease 11, no. 3: 93. https://doi.org/10.3390/jcdd11030093