
Early Atherosclerosis in Familial Hypercholesterolemia Patients: Significance of Vascular Markers for Risk Stratification
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
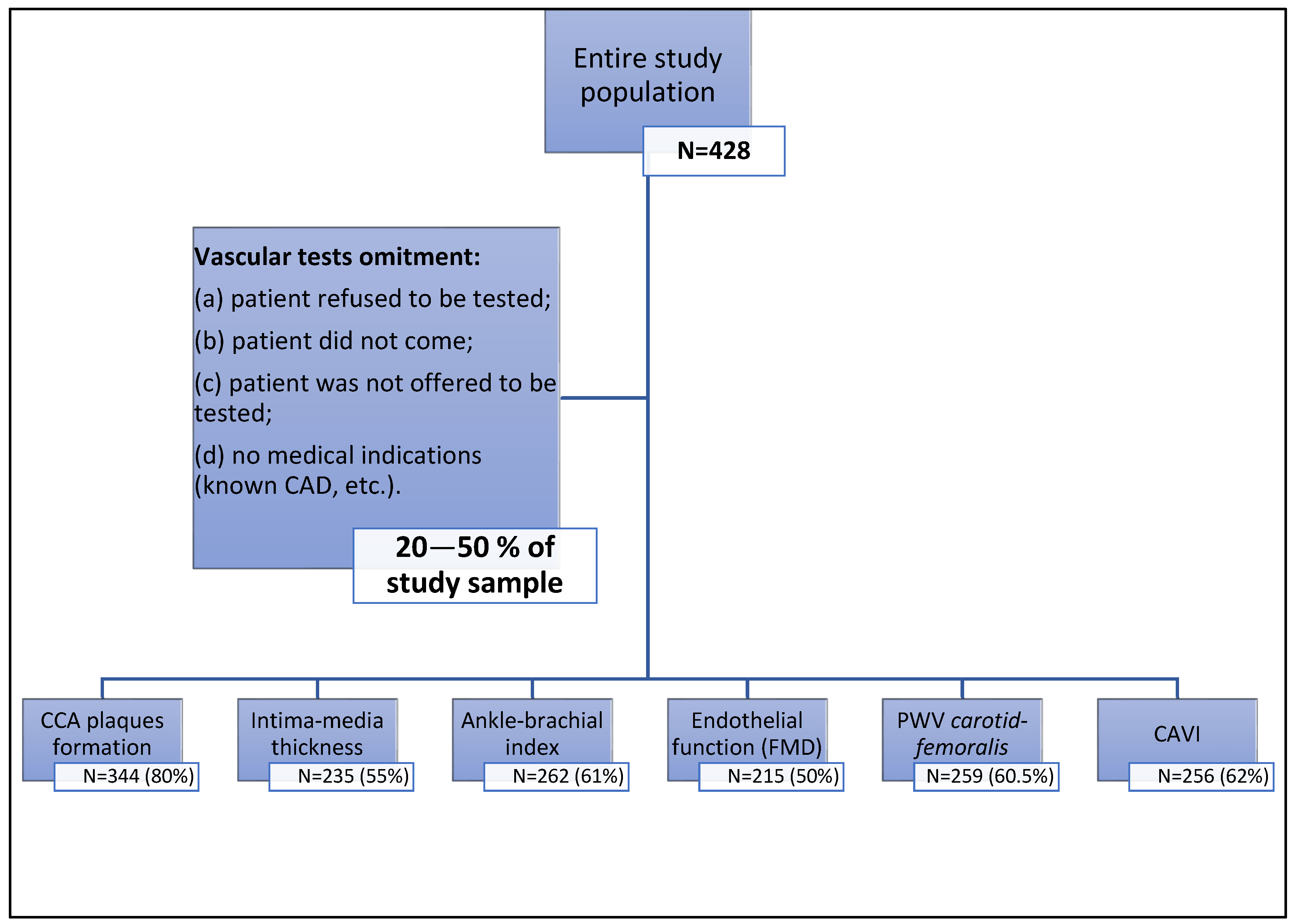
2.1. Study Design
2.2. Measurement Methods
3. Statistical Analysis
4. Results
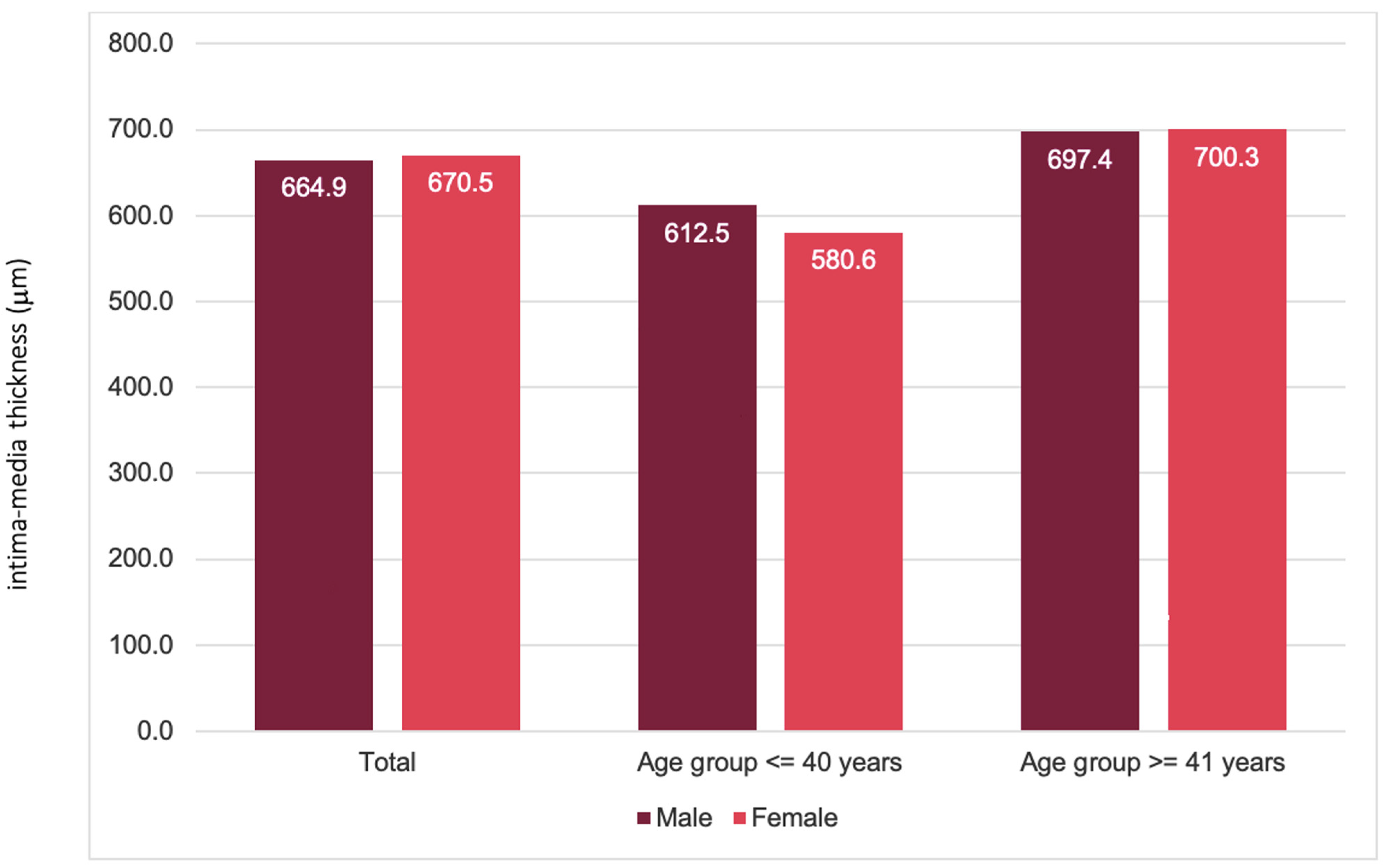
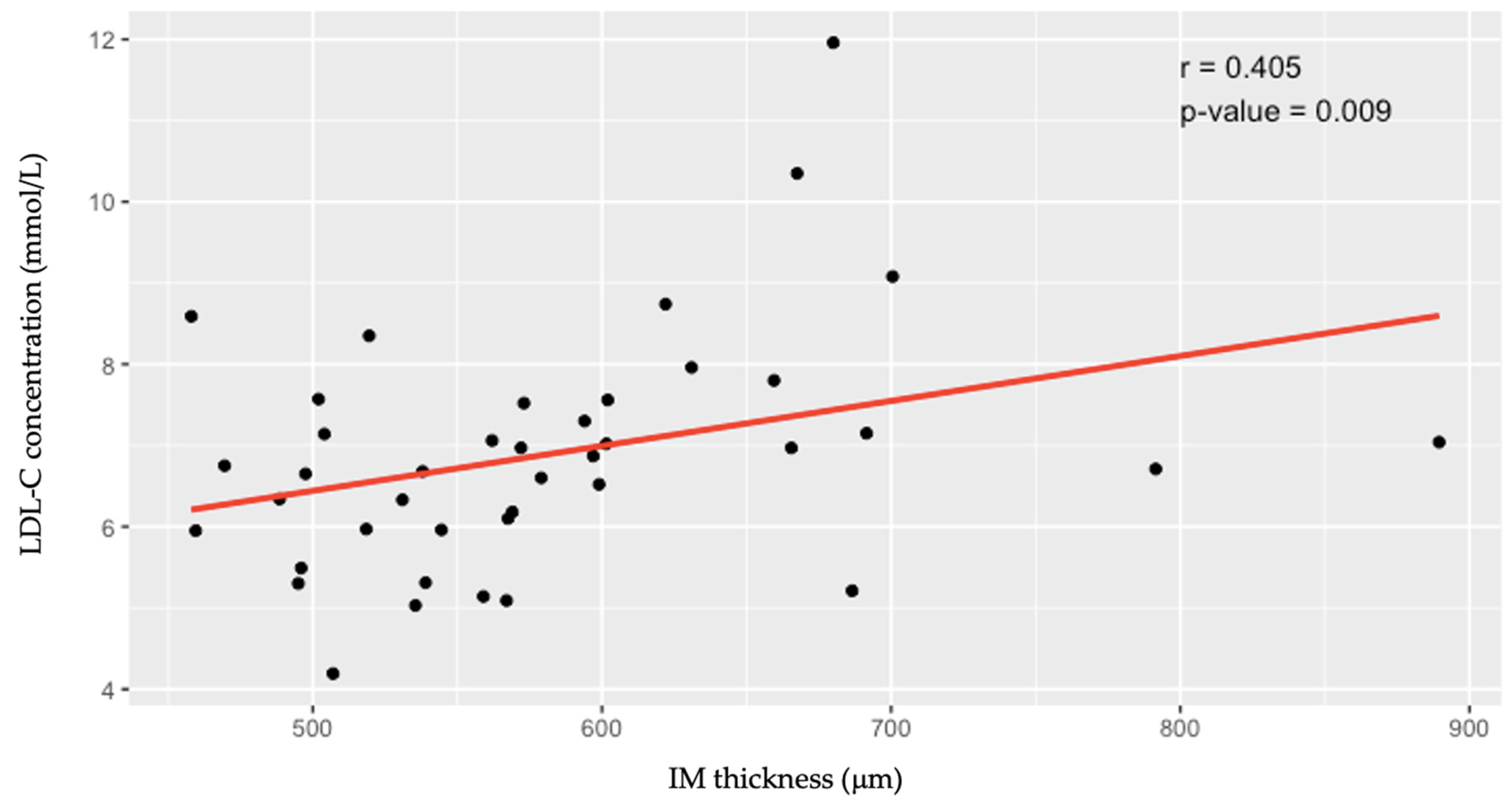
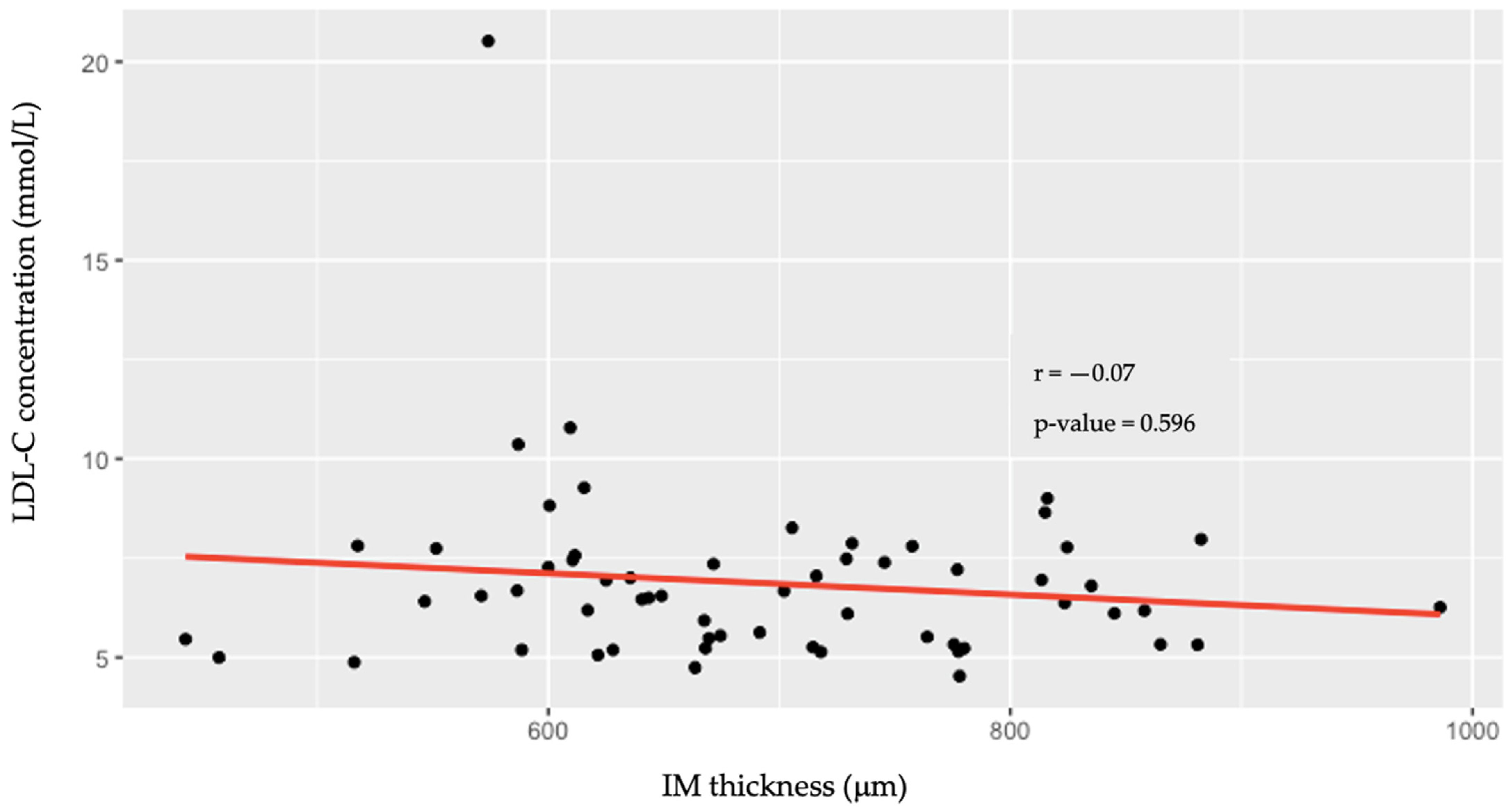
4.1. Intima–Media Thickness (IMT) of the Common Carotid Arteries
4.2. Common Carotid Artery (CCA) Plaque Formation
4.3. The Value of the Ankle–Brachial Index (ABI) for Detecting Peripheral Artery Disease (PAD)
4.4. Endothelial Function Assessed by Flow-Mediated Dilation (FMD)
4.5. Measurements of Arterial Stiffness
4.5.1. Aortic Stiffness, Measured as Aortic Pulse Wave Velocity (PWV Carotid-Femoralis (cfPWV))
4.5.2. Arterial Stiffness, Assessed by the Cardio-Ankle Vascular Index (CAVI)
5. Discussion
6. Conclusions
7. Study Strengths and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABI | ankle–brachial index |
| ANOVA | one-way analysis of variance |
| CAVI | cardio-vascular index |
| CCA | common carotid artery |
| cfPWV | carotid femoralis pulse wave velocity |
| CHD | coronary heart disease |
| CI | confidence interval |
| CVD | cardiovascular disease |
| DLCN | Dutch Lipid Clinic Network |
| DM | diabetes mellitus |
| DNA | deoxyribonucleic acid |
| EAS FHSC | European Atherosclerosis Society Familial Hypercholesterolemia Studies Collaboration |
| FH | Familial hypercholesterolemia |
| FMD | flow-mediated dilation |
| IMT | intima media thickness |
| LDL-C | low-density lipoprotein cholesterol |
| LitHir | Lithuanian High Cardiovascular Risk Primary Prevention Program |
| OR | odds ratio |
| PAD | peripheral artery disease |
| PCSK9 | pro-protein convertase subtilisin/kexin 9 |
| PWV | pulse wave velocity |
| SD | standard deviation |
| μm | micrometer |
References
- Vallejo-Vaz, A.J.; Stevens, C.A.T.; Lyons, A.R.M.; Dharmayat, K.I.; Freiberger, T.; Hovingh, G.K.; Mata, P.; Raal, F.J.; Santos, R.D.; Soran, H.; et al. Global perspective of familial hypercholesterolaemia: A cross-sectional study from the EAS Familial Hypercholesterolaemia Studies Collaboration (FHSC). Lancet 2021, 398, 1713–1725. [Google Scholar] [CrossRef]
- Nordestgaard, B.G.; Chapman, M.J.; Humphries, S.E.; Ginsberg, H.N.; Masana, L.; Descamps, O.S.; Wiklund, O.; Hegele, R.A.; Raal, F.J.; Defesche, J.C.; et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: Guidance for clinicians to prevent coronary heart disease Consensus Statement of the European Atherosclerosis Society. Eur. Heart J. 2013, 34, 3478–3490. [Google Scholar] [CrossRef]
- Knowles, J.W.; O’Brien, E.C.; Greendale, K.; Wilemon, K.; Genest, J.; Sperling, L.S.; Neal, W.A.; Rader, D.J.; Khoury, M.J. Reducing the burden of disease and death from familial hypercholesterolemia: A call to action. Am. Heart J. 2014, 168, 807–811. [Google Scholar] [CrossRef]
- Zamora, A.; Masana, L.; Comas-Cufí, M.; Vila, À.; Plana, N.; García-Gil, M.; Alves-Cabratosa, L.; Marrugat, J.; Roman, I.; Ramos, R. Familial hypercholesterolemia in a European Mediterranean population—Prevalence and clinical data from 2.5 million primary care patients. J. Clin. Lipidol. 2017, 11, 1013–1022. [Google Scholar] [CrossRef]
- Shibayama, J.; Tada, H.; Sakata, K.; Usui, S.; Takamura, M.; Kawashiri, M.A. The Assessment of Carotid Atherosclerotic Plaque among Young Patients with Familial Hypercholesterolemia. Intern. Med. 2022, 61, 3165. [Google Scholar] [CrossRef] [PubMed]
- Jebari-Benslaiman, S.; Galicia-García, U.; Larrea-Sebal, A.; Olaetxea, J.R.; Alloza, I.; Vandenbroeck, K.; Benito-Vicente, A.; Martín, C. Pathophysiology of Atherosclerosis. Int. J. Mol. Sci. 2022, 23, 3346. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Sorensen, K.E.; Gooch, V.M.; Spiegelhalter, D.J.; Miller, O.I.; Sullivan, I.D.; Lloyd, J.K.; Deanfield, J.E.; Spiegelhalter, D.J. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet 1992, 340, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Paquette, M.; Baass, A. Predicting cardiovascular disease in familial hypercholesterolemia. Curr. Opin. Lipidol. 2018, 29, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Trinder, M.; Li, X.; DeCastro, M.L.; Cermakova, L.; Sadananda, S.; Jackson, L.M.; Azizi, H.; Mancini, G.B.J.; Francis, G.A.; Frohlich, J.; et al. Risk of Premature Atherosclerotic Disease in Patients With Monogenic Versus Polygenic Familial Hypercholesterolemia. J. Am. Coll. Cardiol. 2019, 74, 512–522. [Google Scholar] [CrossRef]
- Lewek, J.; Konopka, A.; Starostecka, E.; Penson, P.E.; Maciejewski, M.; Banach, M. Clinical features of familial hypercholesterolemia in children and adults in eas-fhsc regional center for rare diseases in Poland. J. Clin. Med. 2021, 10, 4302. [Google Scholar] [CrossRef] [PubMed]
- Ogura, M.; Harada-Shiba, M.; Masuda, D.; Arai, H.; Bujo, H.; Ishibashi, S.; Daida, H.; Koga, N.; Oikawa, S.; Yamashita, S. Factors Associated with Carotid Atherosclerosis and Achilles Tendon Thickness in Japanese Patients with Familial Hypercholesterolemia: A Subanalysis of the Familial Hypercholesterolemia Expert Forum (FAME) Study. J. Atheroscler. Thromb. 2022, 29, 906–922. [Google Scholar] [CrossRef] [PubMed]
- Gałąska, R.; Kulawiak-Gałąska, D.; Chmara, M.; Chlebus, K.; Mickiewicz, A.; Rynkiewicz, A.; Wasąg, B.; Studniarek, M.; Fijałkowski, M.; Gruchała, M. Carotid intima-media thickness (IMT) in patients with severe familial and non-familial hypercholesterolemia: The effect of measurement site on the IMT correlation with traditional cardiovascular risk factors and calcium scores. Cardiol. J. 2021, 28, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Oren, A.; Vos, L.E.; Uiterwaal, C.S.P.M.; Grobbee, D.E.; Bots, M.L. Cardiovascular risk factors and increased carotid intima-media thickness in healthy young adults: The atherosclerosis risk in young adults (ARYA) study. Arch. Intern. Med. 2003, 163, 1787–1792. [Google Scholar] [CrossRef] [PubMed]
- Qu, B.; Qu, T. Causes of changes in carotid intima-media thickness: A literature review. Cardiovasc. Ultrasound 2015, 13, 46. [Google Scholar] [CrossRef] [PubMed]
- Karapostolakis, G.; Vakaki, M.; Attilakos, A.; Marmarinos, A.; Papadaki, M.; Koumanidou, C.; Alexopoulou, E.; Gourgiotis, D.; Garoufi, A. The Effect of Long-Term Atorvastatin Therapy on Carotid Intima-Media Thickness of Children With Dyslipidemia. Angiology 2021, 72, 322–331. [Google Scholar] [CrossRef] [PubMed]
- Narverud, I.; Retterstøl, K.; Iversen, P.O.; Halvorsen, B.; Ueland, T.; Ulven, S.M.; Ose, L.; Aukrust, P.; Veierød, M.B.; Holven, K.B. Markers of atherosclerotic development in children with familial hypercholesterolemia: A literature review. Atherosclerosis 2014, 235, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Luirink, I.K.; Wiegman, A.; Kusters, D.M.; Hof, M.H.; Groothoff, J.W.; de Groot, E.; Kastelein, J.J.P.; Hutten, B.A. 20-Year Follow-up of Statins in Children with Familial Hypercholesterolemia. N. Engl. J. Med. 2019, 381, 1547–1556. [Google Scholar] [CrossRef]
- Waluś-Miarka, M.; Czarnecka, D.; Kloch-Badełek, M.; Wojciechowska, W.; Kapusta, M.; Malecki, M.T. Carotid artery plaques—Are risk factors the same in men and women with familial hypercholesterolemia? Int. J. Cardiol. 2017, 244, 290–295. [Google Scholar] [CrossRef]
- Maruhashi, T.; Soga, J.; Fujimura, N.; Idei, N.; Mikami, S.; Iwamoto, Y.; Kajikawa, M.; Matsumoto, T.; Hidaka, T.; Kihara, Y.; et al. Relationship between flow-mediated vasodilation and cardiovascular risk factors in a large community-based study. Heart 2013, 99, 1837–1842. [Google Scholar] [CrossRef]
- Vlahos, A.P.; Naka, K.K.; Bechlioulis, A.; Theoharis, P.; Vakalis, K.; Moutzouri, E.; Miltiadous, G.; Michalis, L.K.; Siamopoulou-Mavridou, A.; Elisaf, M.; et al. Endothelial dysfunction, but not structural atherosclerosis, is evident early in children with heterozygous familial hypercholesterolemia. Pediatr. Cardiol. 2014, 35, 63–70. [Google Scholar] [CrossRef]
- Masoura, C.; Pitsavos, C.; Aznaouridis, K.; Skoumas, I.; Vlachopoulos, C.; Stefanadis, C. Arterial endothelial function and wall thickness in familial hypercholesterolemia and familial combined hyperlipidemia and the effect of statins. A systematic review and meta-analysis. Atherosclerosis 2011, 214, 129–138. [Google Scholar] [CrossRef]
- Heiss, C.; Rodriguez-Mateos, A.; Bapir, M.; Skene, S.S.; Sies, H.; Kelm, M. Flow-mediated dilation reference values for evaluation of endothelial function and cardiovascular health. Cardiovasc. Res. 2023, 119, 283–293. [Google Scholar] [CrossRef]
- Kaczmarczyk, P.; Maga, P.; Niżankowski, R.; Januszek, R.; Frołow, M.; Maga, M.; Kościelniak, J.; Belowski, A. The relationship between pulse waveform analysis indices, endothelial function and clinical outcomes in patients with peripheral artery disease treated using percutaneous transluminal angioplasty during a one-year follow-up period. Cardiol. J. 2020, 27, 142–151. [Google Scholar] [CrossRef]
- Pereira, C.; Miname, M.H.; Makdisse, M.R.P.; Watanabe, C.; Pesaro, A.E.; Jannes, C.E.; Kalil Filho, R.; Pereira, A.C.; Santos, R.D. Peripheral arterial disease in heterozygous familial hypercholesterolemia. Atherosclerosis 2015, 242, 174–178. [Google Scholar] [CrossRef]
- Mundal, L.J.; Hovland, A.; Igland, J.; Vetrhus, M.; Veierød, M.B.; Holven, K.B.; Bogsrud, M.P.; Tell, G.S.; Leren, T.P.; Retterstøl, K. Increased risk of peripheral artery disease in persons with familial hypercholesterolaemia: A prospective registry study. Eur. J. Prev. Cardiol. 2021, 28, E11–E13. [Google Scholar] [CrossRef] [PubMed]
- Akioyamen, L.E.; Tu, J.V.; Genest, J.; Ko, D.T.; Coutin, A.J.S.; Shan, S.D.; Chu, A. Risk of Ischemic Stroke and Peripheral Arterial Disease in Heterozygous Familial Hypercholesterolemia: A Meta-Analysis. Angiology 2019, 70, 726–736. [Google Scholar] [CrossRef] [PubMed]
- Horváth, L.; Németh, N.; Fehér, G.; Kívés, Z.; Endrei, D.; Boncz, I. Epidemiology of Peripheral Artery Disease: Narrative Review. Life 2022, 12, 1041. [Google Scholar] [CrossRef] [PubMed]
- Emanuelsson, F.; Nordestgaard, B.G.; Benn, M. Familial Hypercholesterolemia and Risk of Peripheral Arterial Disease and Chronic Kidney Disease. J. Clin. Endocrinol. Metab. 2018, 103, 4491–4500. [Google Scholar] [CrossRef] [PubMed]
- Armas-Padrón, A.M.; Sicilia-Sosvilla, M.; Rodríguez-Bello, S.; López-Carmona, M.D.; Ruiz-Esteban, P.; Hernández, D. Abnormal ankle-brachial index, cardiovascular risk factors and healthy lifestyle factors in hypertensive patients: Prospective cohort study from a primary care urban population. BMC Prim. Care 2022, 23, 232. [Google Scholar] [CrossRef] [PubMed]
- Ershova, A.I.; Meshkov, A.N.; Rozhkova, T.A.; Kalinina, M.V.; Deev, A.D.; Rogoza, A.N.; Balakhonova, T.V.; Boytsov, S.A. Carotid and Aortic Stiffness in Patients with Heterozygous Familial Hypercholesterolemia. PLoS ONE 2016, 11, e0158964. [Google Scholar] [CrossRef] [PubMed]
- Choo, J.; Shin, C.; Barinas-Mitchell, E.; Masaki, K.; Willcox, B.J.; Seto, T.B.; Ueshima, H.; Lee, S.; Miura, K.; Venkitachalam, L.; et al. Regional pulse wave velocities and their cardiovascular risk factors among healthy middle-aged men: A cross-sectional population-based study. BMC Cardiovasc. Disord. 2014, 14, 5. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.; Dharmarajan, A.; Swain, P.K.; Das, D.; Verma, P.; Tripathy, P.R. Impact of Cardiovascular Factors on Pulse Wave Velocity and Total Vascular Resistance in Different Age Group Patients with Cardiovascular Disorders. Curr. Aging Sci. 2019, 11, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Saiki, A.; Ohira, M.; Yamaguchi, T.; Nagayama, D.; Shimizu, N.; Shirai, K.; Tatsuno, I. New horizons of arterial stiffness developed using Cardio-Ankle Vascular Index (CAVI). J. Atheroscler. Thromb. 2020, 27, 732–748. [Google Scholar] [CrossRef] [PubMed]
- Shirai, K.; Hiruta, N.; Song, M.; Kurosu, T.; Suzuki, J.; Tomaru, T.; Miyashita, Y.; Saiki, A.; Takahashi, M.; Suzuki, K.; et al. Cardio-ankle vascular index (CAVI) as a novel indicator of arterial stiffness: Theory, evidence and perspectives. J. Atheroscler. Thromb. 2011, 18, 924–938. [Google Scholar] [CrossRef]
- Choi, S.Y.; Oh, B.H.; Park, J.B.; Choi, D.J.; Rhee, M.Y.; Park, S. Age-associated increase in arterial stiffness measured according to the cardio-ankle vascular index without blood pressure changes in healthy adults. J. Atheroscler. Thromb. 2013, 20, 911–923. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | ≤40 | ≥41 | p Value | |
|---|---|---|---|---|
| N (%) | 428 | 126 (29%) | 292 (68%) | - |
| Median Age (years) | 47 | - | - | - |
| Median LDL-C (mmol/L ± SD) | 6.37 ± 1.63 | 6.71 ± 1.7 | 6.23 ± 1.6 | 0.034 |
| Definite FH (N) | 83 | 46 (55.4%) | 35 (42.2%) | - |
| Probable FH (N) | 97 | 23 (23.7%) | 72 (74.2%) | - |
| Possible FH (N) | 224 | 49 (21.9%) | 170 (75.9%) | - |
| Unlikely FH (N) | 24 | 8 (33.3%) | 15 (62.5%) | - |
| Hypertension (N) | 221 | 36 (16.3%) | 181 (81.9%) | <0.001 |
| Diabetes mellitus (N) | 44 | 4 (9.1%) | 39 (88.6%) | 0.002 |
| Smoking (N) | 128 | 35 (27.3%) | 91 (71.1%) | 0.686 |
| FH mutation (N) | 49 | 25 (51%) | 23 (46.9%) | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aliosaitiene, U.; Petrulioniene, Z.; Rinkuniene, E.; Mainelis, A.; Barysiene, J.; Smailyte, U.; Sileikiene, V.; Laucevicius, A. Early Atherosclerosis in Familial Hypercholesterolemia Patients: Significance of Vascular Markers for Risk Stratification. J. Cardiovasc. Dev. Dis. 2024, 11, 91. https://doi.org/10.3390/jcdd11030091
Aliosaitiene U, Petrulioniene Z, Rinkuniene E, Mainelis A, Barysiene J, Smailyte U, Sileikiene V, Laucevicius A. Early Atherosclerosis in Familial Hypercholesterolemia Patients: Significance of Vascular Markers for Risk Stratification. Journal of Cardiovascular Development and Disease. 2024; 11(3):91. https://doi.org/10.3390/jcdd11030091
Chicago/Turabian StyleAliosaitiene, Urte, Zaneta Petrulioniene, Egidija Rinkuniene, Antanas Mainelis, Jurate Barysiene, Urte Smailyte, Vaida Sileikiene, and Aleksandras Laucevicius. 2024. "Early Atherosclerosis in Familial Hypercholesterolemia Patients: Significance of Vascular Markers for Risk Stratification" Journal of Cardiovascular Development and Disease 11, no. 3: 91. https://doi.org/10.3390/jcdd11030091