
Importance of Tissue Doppler Evaluation in Dilated Cardiomyopathy: The Value of Diastolic Filling Pattern as a Prognostic Predictor

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population, Follow-Up Visits and Data Collection
2.2. Ultrasound Methods, Variables of Interest
2.3. Statistical Analysis
- -
- age > 75 years;
- -
- male gender;
- -
- the presence of a restrictive LVDFP;
- -
- LVES diameter > 55 mm;
- -
- LVES volume > 95 cm3;
- -
- LVEF < 25%;
- -
- the presence of comorbidities (DM, COPD);
- -
- the presence of 2nd-degree mitral regurgitation;
- -
- the presence of pulmonary hypertension (PHT);
- -
- ischemic etiology of DCM;
- -
- paroxysmal atrial fibrillation;
- -
- NYHA class IV;
- -
- NT-proBNP > 10,000 pg/m.
3. Results
Demographic and Clinical Characteristics of the Patients
- -
- Group A—95 patients with non-restrictive LVDFP
- -
- Group B—47 patients with restrictive LVDFP
- -
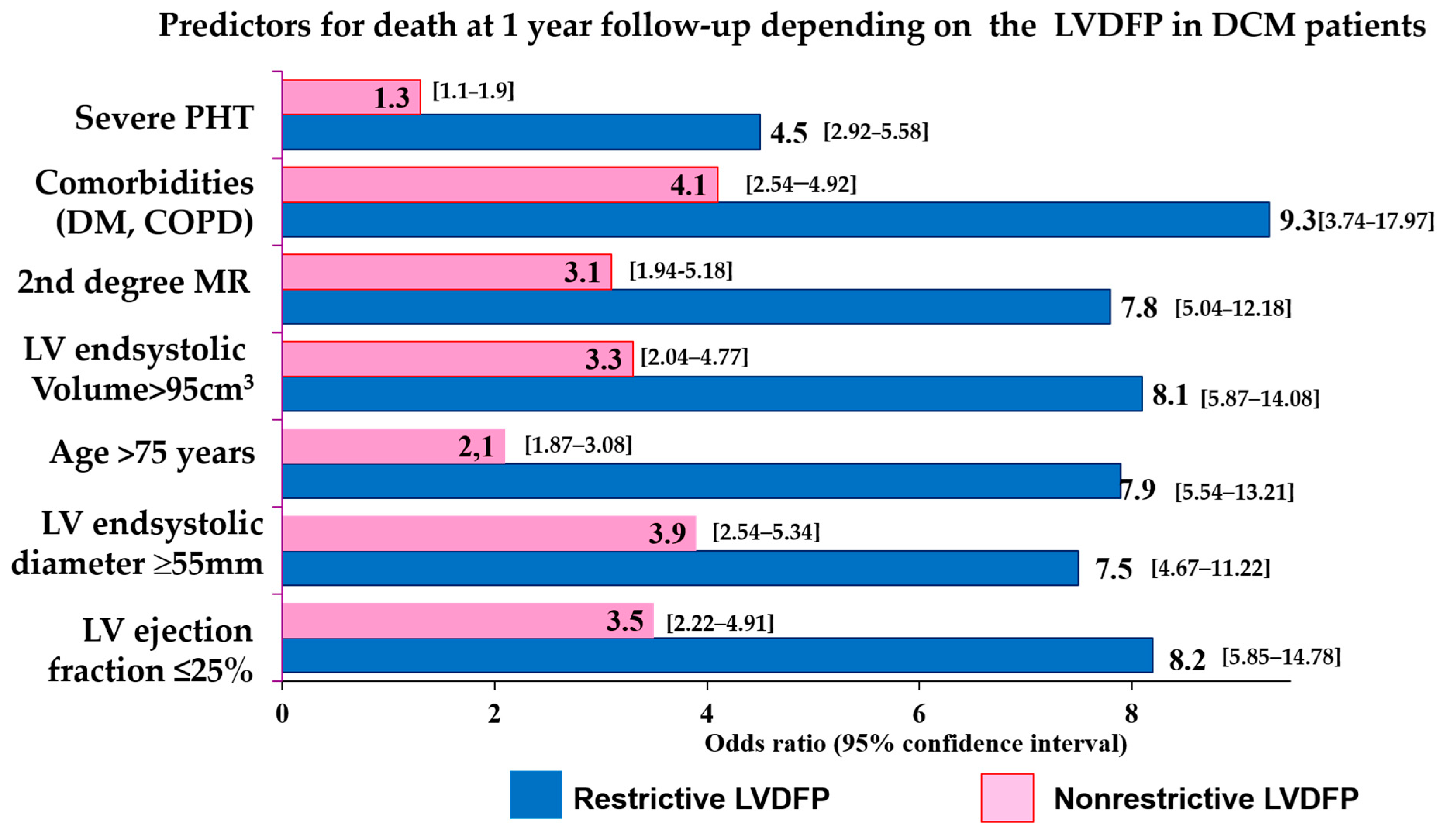
- age > 75 years (OR = 1.75, 95% CI [1.28, 2.78]);
- -
- diabetes mellitus (OR = 4.85, 95% CI [2.79, 8.56]);
- -
- COPD (OR = 4.57, 95% CI [1.45, 12.78]);
- -
- arterial hypertension (OR = 2.03, 95% CI [1.98, 3.92]);
- -
- paroxysmal atrial fibrillation (OR = 3.79, 95% CI [1.76, 7.98]);
- -
- ischemic etiology of DCM (OR= 2. 23, 95% CI [2.78, 4.08]);
- -
- LVEF < 25% (OR = 3.78, 95% CI [2.45, 3.99]);
- -
- NYHA class > III (OR = 4.88, 95% CI [2.58, 8.97]);
- -
- severe PHT (OR = 2.92, 95% CI [1.45, 4.97]).
- -
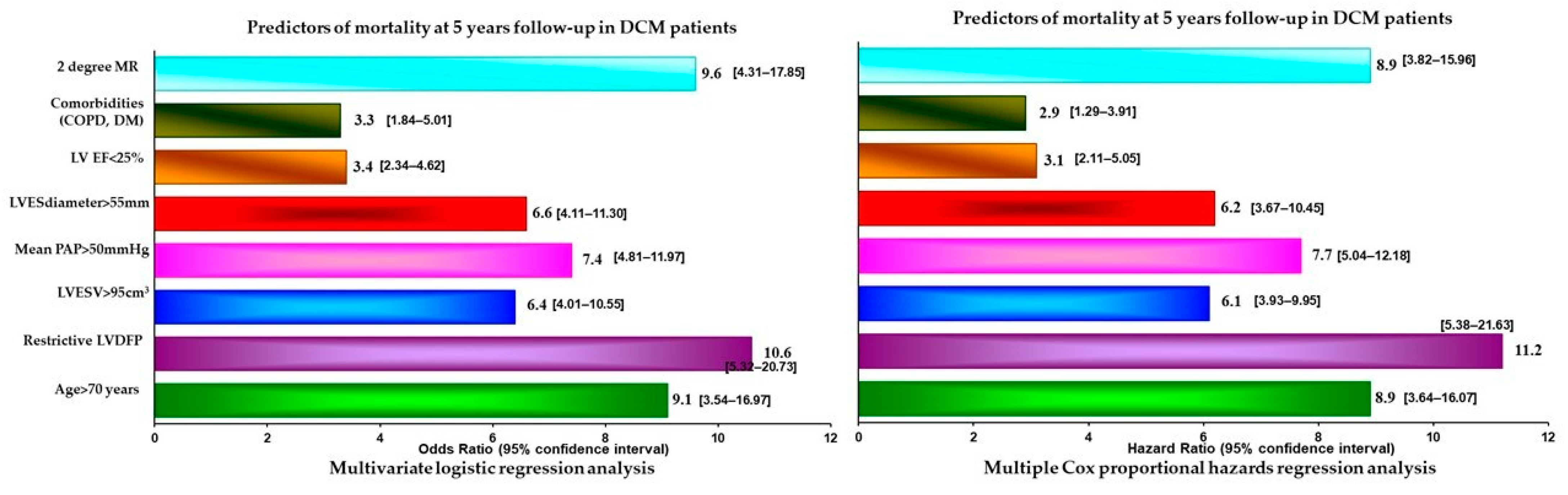
- the presence of a restrictive LVDFP (OR = 6.75, 95% CI [4.64–8.78]);
- -
- age > 75 years (OR = 5.8, 95% CI [3.88–8.12]);
- -
- LVES diameter > 55 mm (OR = 4.52, 95% CI [3.59–6.59]);
- -
- LVES volume > 95 cm3 (OR = 5.32, 95% CI [3.64–7.78]);
- -
- the presence of comorbidities (DM, COPD) (OR = 6.52, 95%CI [3.87–8.33]);
- -
- the presence of 2nd-degree mitral regurgitation (OR = 5.41, 95% CI [3.74–7.89]);
- -
- the presence of pulmonary hypertension (PHT) (OR = 2.8, 95% CI [1.58–3.89]).
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Schultheiss, H.-P.; Fairweather, D.; Caforio, A.L.P.; Escher, F.; Hershberger, R.E.; Lipshultz, S.E.; Liu, P.P.; Matsumori, A.; Mazzanti, A.; McMurray, J.; et al. Dilated cardiomyopathy. Nat. Rev. Dis. Prim. 2019, 5, 32. [Google Scholar] [CrossRef]
- Truby, L.K.; Rogers, J.G. Advanced Heart Failure: Epidemiology, Diagnosis, and Therapeutic Approaches. JACC Heart Fail. 2020, 8, 523–536. [Google Scholar] [CrossRef]
- Japp, A.G.; Gulati, A.; Cook, S.A.; Cowie, M.R.; Prasad, S.K. The Diagnosis and Evaluation of Dilated Cardiomyopathy. J. Am. Coll. Cardiol. 2016, 67, 2996–3010. [Google Scholar] [CrossRef]
- Thomas, D.E.; Wheeler, R.; Yousef, Z.R.; Masani, N.D. The role of echocardiography in guiding management in dilated cardiomyopathy. Eur. J. Echocardiogr. 2009, 10, iii15–iii21. [Google Scholar] [CrossRef]
- Nogueira, M.A.; Ferreira, F.; Raposo, A.F.; Mónica, L.; Dias, S.S.; Vasconcellos, R.; Proença, G. Impact of telemedicine on the management of heart failure patients during coronavirus disease 2019 pandemic. ESC Heart Fail. 2021, 8, 1150–1155. [Google Scholar] [CrossRef]
- Visco, V.; Esposito, C.; Manzo, M.; Fiorentino, A.; Galasso, G.; Vecchione, C.; Ciccarelli, M. A Multistep Approach to Deal with Advanced Heart Failure: A Case Report on the Positive Effect of Cardiac Contractility Modulation Therapy on Pulmonary Pressure Measured by CardioMEMS. Front. Cardiovasc. Med. 2022, 9, 874433. [Google Scholar] [CrossRef]
- Macarie, C.; Iliuta, L.; Savulescu, C.; Moldovan, H.; Vasile, R.; Filipescu, D.; Gherghiceanu, D.P.; Candea, V. The left ventricular diastolic filling pattern as prognostic predictor in patients with idiopathic dilated cardiomyopathy. Eur. Heart J. 2004, 25, 7. [Google Scholar]
- Henein, M.Y.; Lindqvist, P.; Henein, M.M.Y. Diastolic function assessment by echocardiography: A practical manual for clinical use and future applications. Echocardiography 2020, 37, 1908–1918. [Google Scholar] [CrossRef]
- Iliuta, L. Predictors of persistent severe diastolic dysfunction after aortic valve replacement in aortic stenosis compared with aortic regurgitation. Eur. Heart J. 2012, 33, 667–668. [Google Scholar]
- Xu, X.R.; Han, M.M.; Yang, Y.Z.; Wang, X.; Hou, D.Y.; Meng, X.C.; Wang, H.; Zhao, W.-S.; Zhang, L.; Xu, L. Fifteen-year mortality and prognostic factors in patients with dilated cardiomyopathy: Persistent standardized application of drug therapy and strengthened management may bring about encouraging change in an aging society. J. Geriatr. Cardiol. 2022, 19, 335–342. [Google Scholar]
- Iliuta, L.; Rac-Albu, M. Predictors and late incidence of persistent or recurrent heart failure after aortic valve replacement for aortic stenosis compared with aortic regurgitation. Eur. Heart J. 2014, 35, 358. [Google Scholar]
- Iliuta, L. The role of TDI diastolic measurements for prognostic prediction early and late after surgical ventricular reconstruction. Eur. Heart J. 2019, 40, 2798. [Google Scholar] [CrossRef]
- Iliuta, L.; Andronesi, A.G.; Panaitescu, E.; Rac-Albu, M.E.; Scafa-Udriște, A.; Moldovan, H. Challenges for Management of Dilated Cardiomyopathy during COVID-19 Pandemic—A Telemedicine Application. J. Clin. Med. 2022, 11, 7411. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Januzzi, J.L.; van Kimmenade, R.; Lainchbury, J.; Bayes-Genis, A.; Ordonez-Llanos, J.; Santalo-Bel, M.; Pinto, Y.M.; Richards, M. NT-proBNP testing for diagnosis and short-term prognosis in acute destabilized heart failure: An international pooled analysis of 1256 patients: The International Collaborative of NT-proBNP Study. Eur. Heart J. 2006, 27, 330–337. [Google Scholar] [CrossRef]
- Matsumura, Y.; Takata, J.; Kitaoka, H.; Kubo, T.; Baba, Y.; Hoshikawa, E.; Hamada, T.; Okawa, M.; Hitomi, N.; Sato, K.; et al. Long-Term Prognosis of Dilated Cardiomyopathy Revisited: An Improvement in Survival over the Past 20 Years. Circ. J. 2006, 70, 376–383. [Google Scholar] [CrossRef]
- Goldberger, J.J.; Subačius, H.; Patel, T.; Cunnane, R.; Kadish, A.H. Sudden Cardiac Death Risk Stratification in Patients with Nonischemic Dilated Cardiomyopathy. J. Am. Coll. Cardiol. 2014, 63, 1879–1889. [Google Scholar] [CrossRef]
- Cannata, A.; Manca, P.; Nuzzi, V.; Gregorio, C.; Artico, J.; Gentile, P.; Loco, C.P.; Ramani, F.; Barbati, G.; Merlo, M.; et al. Sex-Specific Prognostic Implications in Dilated Cardiomyopathy after Left Ventricular Reverse Remodeling. J. Clin. Med. 2020, 9, 2426. [Google Scholar] [CrossRef]
- Iliuta, L.; Andronesi, A.G.; Diaconu, C.C.; Panaitescu, E.; Camburu, G. Additional Prognostic Value of Tissue Doppler Evaluation in Patients with Aortic Stenosis and Left-Ventricular Systolic Dysfunction Undergoing Aortic Valve Replacement. Medicina 2022, 58, 1410. [Google Scholar] [CrossRef]
- Markman, T.M.; Nazarian, S. Moving toward Improved Risk Stratification in Patients with Dilated Cardiomyopathy. Circ. Cardiovasc. Imaging 2020, 13, e010629. [Google Scholar] [CrossRef] [PubMed]
- Pinamonti, B.; Zecchin, M.; Di Lenarda, A.; Gregori, D.; Sinagra, G.; Camerini, F. Persistence of Restrictive Left Ventricular Filling Pattern in Dilated Cardiomyopathy: An Ominous Prognostic Sign. J. Am. Coll. Cardiol. 1997, 29, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.Z.; Blomström-Lundqvist, C.; Bloom, H.; Cooper, C.; Ellis, C.; Goette, A.; Greenspon, A.J.; Love, C.J.; Johansen, J.B.; Philippon, F.; et al. Use of healthcare claims to validate the Prevention of Arrhythmia Device Infection Trial cardiac implantable electronic device infection risk score. Europace 2021, 23, 1446–1455. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Hartshorne-Evans, N.; Redmond-Lyon, S.; Wilson, J.; Essa, H.; Gray, A.; Clayton, L.; Barton, C.; Ahmed, F.Z.; Cunnington, C.; et al. The impact of COVID-19 on the management of heart failure: A United Kingdom patient questionnaire study. ESC Heart Fail. 2021, 8, 1324–1332. [Google Scholar] [CrossRef]
- Abraham, W.T.; Adamson, P.B.; Bourge, R.C.; Aaron, M.F.; Costanzo, M.R.; Stevenson, L.W.; Strickland, W.; Neelagaru, S.; Raval, N.; Krueger, S.; et al. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: A randomised controlled trial. Lancet 2011, 377, 658–666. [Google Scholar] [CrossRef]
- Jurcut, R.; Savu, O.; Popescu, B.A.; Florian, A.; Herlea, V.; Moldovan, H.; Ginghina, C. Primary cardiac leiomyosarcoma when valvular disease becomes a vascular surgical emergency. Circulation 2010, 121, E415–E418. [Google Scholar] [CrossRef]
- Iliuta, L.; Savulescu, C.; Moldovan, H.; Gherghiceanu, D.P.; Vasile, R.; Filipescu, D. Diastolic versus systolic left ventricular dysfunction as independent predictors for unfavourable postoperative evolution in patients with aortic stenosis undergoing aortic valve replacement. Eur. Heart J. 2005, 26, 193. [Google Scholar]
- Rich, J.D.; Burns, J.; Freed, B.H.; Maurer, M.S.; Burkhoff, D.; Shah, S.J. Meta-Analysis Global Group in Chronic (MAGGIC) Heart Failure Risk Score: Validation of a Simple Tool for the Prediction of Morbidity and Mortality in Heart Failure with Preserved Ejection Fraction. J. Am. Heart Assoc. 2018, 7, e009594. [Google Scholar] [CrossRef]
- Pinamonti, B.; Di Lenarda, A.; Sinagra, G.; Camerini, F. Restrictive left ventricular filling pattern in dilated cardiomyopathy assessed by doppler echocardiography: Clinical, echocardiographic and hemodynamic correlations and prognostic implications. J. Am. Coll. Cardiol. 1993, 22, 808–815. [Google Scholar] [CrossRef]
- Fantini, F.; Toso, A.; Menicanti, L.; Moroni, F.; Castelvecchio, S. Restrictive filling pattern in ischemic cardiomyopathy: Insights after surgical ventricular restoration. J. Thorac. Cardiovasc. Surg. 2021, 161, 651–660. [Google Scholar] [CrossRef]
- Iliuta, L.; Moldovan, H.; Filipescu, D.; Radulescu, B.; Vasilescu, A. Diastolic versus systolic left ventricular dysfunction as independent predictors for unfavourable postoperative evolution in patients with aortic regurgitation undergoing aortic valve replacement. Eur. Heart J. 2009, 30, 865. [Google Scholar]
- Matsumura, Y.; Hoshikawa-Nagai, E.; Kubo, T.; Yamasaki, N.; Furuno, T.; Kitaoka, H.; Takata, J.; Sugiura, T.; Doi, Y. Left Ventricular Reverse Remodeling in Long-Term (>12 Years) Survivors with Idiopathic Dilated Cardiomyopathy. Am. J. Cardiol. 2013, 111, 106–110. [Google Scholar] [CrossRef]
- Boehmer, J.P.; Hariharan, R.; Devecchi, F.G.; Smith, A.L.; Molon, G.; Capucci, A.; An, Q.; Averina, V.; Stolen, C.M.; Thakur, P.H.; et al. A Multisensor Algorithm Predicts Heart Failure Events in Patients with Implanted Devices: Results from the MultiSENSE Study. JACC Heart Fail. 2017, 5, 216–225. [Google Scholar] [CrossRef]
- Ong, M.K.; Romano, P.S.; Edgington, S.; Aronow, H.U.; Auerbach, A.D.; Black, J.T.; De Marco, T.; Escarce, J.J.; Evangelista, L.S.; Hanna, B.; et al. Effectiveness of Remote Patient Monitoring after Discharge of Hospitalized Patients with Heart Failure: The Better Effectiveness after Transition—Heart Failure (BEAT-HF) Randomized Clinical Trial. JAMA Intern. Med. 2016, 176, 310–318. [Google Scholar] [CrossRef]
- Iliuta, L.; Rac-Albu, M.; Rac-Albu, M.-E.; Andronesi, A. Impact of Pulmonary Hypertension on Mortality after Surgery for Aortic Stenosis. Medicina 2022, 58, 1231. [Google Scholar] [CrossRef]
- Marrow, B.A.; Cook, S.A.; Prasad, S.K.; McCann, G.P. Emerging Techniques for Risk Stratification in Nonischemic Dilated Cardiomyopathy: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2020, 75, 1196–1207. [Google Scholar] [CrossRef] [PubMed]
- Iliuta, L. Impact of Severe Pulmonary Hypertension on Outcomes Late after Aortic Valve Replacement for Aortic Stenosis Compared with Aortic Regurgitation. Cardiology 2014, 128, 177. [Google Scholar]
- Brown, P.F.; Miller, C.; Di Marco, A.; Schmitt, M. Towards cardiac MRI based risk stratification in idiopathic dilated cardiomyopathy. Heart 2019, 105, 270–275. [Google Scholar] [CrossRef]
- Buzatu, M.; Geantă, V.; Ştefănoiu, R.; Buţu, M.; Petrescu, M.I.; Buzatu, M.; Antoniac, I.; Iacob, G.; Niculescu, F.; Ghica, Ş.I.; et al. Investigations into Ti-15Mo-W Alloys Developed for Medical Applications. Materials 2019, 12, 147. [Google Scholar] [CrossRef]
- Popma, J.J.; Cigarroa, R.G.; Buja, L.M.; Hillis, L.D. Diagnostic and prognostic utility of right-sided catheterization and endomyocardial biopsy in idiopathic dilated cardiomyopathy. Am. J. Cardiol. 1989, 63, 955–958. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group A—95 pts Non-Restrictive LVDFP | Group B—47 pts Restrictive LVDFP | p-Value | |
|---|---|---|---|
| Mean (SD) age (years) | 59 (11) | 63 (13) | 0.381 1 |
| Women, no. (%) | 41 (43.1%) | 19 (40.4%) | 0.584 2 |
| Medical history, no. (%) | |||
| Arterial hypertension | 49 (51.6%) | 27 (57.4%) | 0.229 2 |
| Diabetes mellitus | 39(41.1%) | 36 (76.6%) | 0.001 2 |
| Paroxysmal atrial fibrillation | 32 (33.7%) | 26 (55.3%) | 0.035 2 |
| Ischemic etiology of DCM | 45 (47.4%) | 24 (51.1%) | 0.059 2 |
| Chronic kidney disease | 32 (33.7) | 15 (31.9%) | 0.338 2 |
| COPD | 11 (11.6%) | 14 (29.8%) | 0.012 2 |
| Mean (SD) LVEF (%) | 32 (5) | 22 (4) | 0.003 1 |
| LVEF ≤ 25%, no. (%) | 19 (20%) | 18 (38.3%) | 0.001 2 |
| Mean (SD) heart rate (b/min) | 75 (17) | 84 (18) | 0.641 1 |
| Mean (SD) systolic blood pressure (mm Hg) | 125 ± 18 | 105 ± 12 | 0.052 1 |
| NYHAa class I/II, no. (%) | 40 (42.1%) | 5 (10.6%) | 0.001 3 |
| NYHAa class III, no. (%) | 39 (41.1%) | 25 (53.2%) | |
| NYHAa class IV, no. (%) | 13 (13.7%) | 20 (42.5%) | |
| Median NT-proBNP (IQR) b (pg/mL) | 1192 (800–2693) | 1929 (800–2693) | 0.034 1 |
| Medications, no. (%) | |||
| ACEi or ARB | 60 (63.2%) | 29 (61.7%) | 0.114 3 |
| Sacubitril/valsartan | 35 (36.8%) | 11 (23.4%) | 0.212 3 |
| Beta-blocker | 88 (92.6%) | 40 (85.1%) | 0.071 3 |
| Mineralocorticoid receptor antagonist | 90 (94.7%) | 44 (93.6%) | 0.511 3 |
| Ivabradine | 10 (10.5%) | 3 (6.38%) | 0.442 3 |
| Digitalis | 55 (57.9%) | 26(55.32%) | 0.125 3 |
| Diuretic | 53 (55.8%) | 37(78.73%) | 0.041 3 |
| Implantable cardioverter defibrillator | 2 (2.1%) | 3 (6.38%) | 0.001 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iliuță, L.; Andronesi, A.G.; Rac-Albu, M.; Rac-Albu, M.-E.; Scafa-Udriște, A.; Moldovan, H.; Furtunescu, F.L.; Rădulescu, B.C.; Panaitescu, E. Importance of Tissue Doppler Evaluation in Dilated Cardiomyopathy: The Value of Diastolic Filling Pattern as a Prognostic Predictor. J. Cardiovasc. Dev. Dis. 2023, 10, 237. https://doi.org/10.3390/jcdd10060237
Iliuță L, Andronesi AG, Rac-Albu M, Rac-Albu M-E, Scafa-Udriște A, Moldovan H, Furtunescu FL, Rădulescu BC, Panaitescu E. Importance of Tissue Doppler Evaluation in Dilated Cardiomyopathy: The Value of Diastolic Filling Pattern as a Prognostic Predictor. Journal of Cardiovascular Development and Disease. 2023; 10(6):237. https://doi.org/10.3390/jcdd10060237
Chicago/Turabian StyleIliuță, Luminita, Andreea Gabriella Andronesi, Marius Rac-Albu, Mădălina-Elena Rac-Albu, Alexandru Scafa-Udriște, Horațiu Moldovan, Florentina Ligia Furtunescu, Bogdan Constantin Rădulescu, and Eugenia Panaitescu. 2023. "Importance of Tissue Doppler Evaluation in Dilated Cardiomyopathy: The Value of Diastolic Filling Pattern as a Prognostic Predictor" Journal of Cardiovascular Development and Disease 10, no. 6: 237. https://doi.org/10.3390/jcdd10060237