
Quantitative SPECT/CT Parameters in the Assessment of Transthyretin Cardiac Amyloidosis—A New Dimension of Molecular Imaging
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Aims of Review
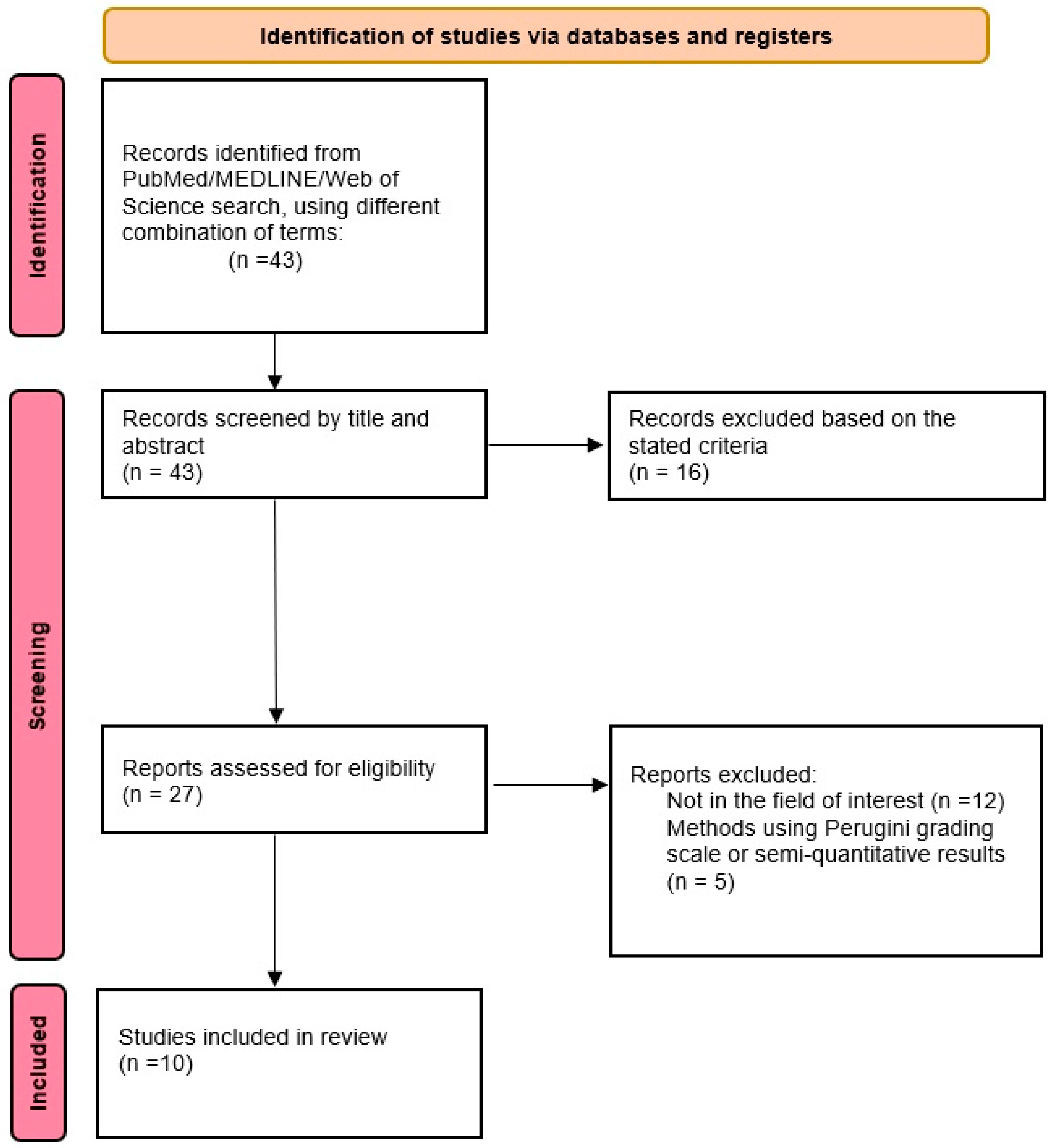
2.2. Search Algorithm
2.3. Data Extraction and Synthesis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Muchtar, E.; Dispenzieri, A.; Magen, H.; Grogan, M.; Mauermann, M.; McPhail, E.D.; Kurtin, P.J.; Leung, N.; Buadi, F.K.; Dingli, D.; et al. Systemic Amyloidosis from A (AA) to T (ATTR): A Review. J. Intern. Med. 2021, 289, 268–292. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.P.; Damy, T.; Eriksson, U.; et al. Diagnosis and Treatment of Cardiac Amyloidosis: A Position Statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2021, 42, 1554–1568. [Google Scholar] [CrossRef]
- Maurer, M.S.; Elliott, P.; Comenzo, R.; Semigran, M.; Rapezzi, C. Addressing Common Questions Encountered in the Diagnosis and Management of Cardiac Amyloidosis. Circulation 2017, 135, 1357–1377. [Google Scholar] [CrossRef] [PubMed]
- Bistola, V.; Parissis, J.; Foukarakis, E.; Valsamaki, P.N.; Anastasakis, A.; Koutsis, G.; Efthimiadis, G.; Kastritis, E. Practical Recommendations for the Diagnosis and Management of Transthyretin Cardiac Amyloidosis. Heart Fail. Rev. 2021, 26, 861–879. [Google Scholar] [CrossRef]
- Saad, J.M.; Ahmed, A.I.; Han, Y.; Saeed, S.; Pournazari, P.; Al-Mallah, M.H. 99mTechnetium-Labeled Cardiac Scintigraphy for Suspected Amyloidosis: A Review of Current and Future Directions. Heart Fail. Rev. 2022, 27, 1493–1503. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.D.; Coriu, D.; Jercan, A.; Bădeliţă, S.; Popescu, B.A.; Damy, T.; Jurcuţ, R. Progress and Challenges in the Treatment of Cardiac Amyloidosis: A Review of the Literature. ESC Heart Fail. 2021, 8, 2380–2396. [Google Scholar] [CrossRef]
- Siddiqi, O.K.; Ruberg, F.L. Cardiac Amyloidosis: An Update on Pathophysiology, Diagnosis, and Treatment. Trends Cardiovasc. Med. 2018, 28, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Alexander, K.M.; Witteles, R.M. Bone Scintigraphy Imaging for Transthyretin Cardiac Amyloidosis: Still Much to Learn*. JACC Cardiovasc. Imaging 2020, 13, 1322–1324. [Google Scholar] [CrossRef]
- Falk, R.H.; Alexander, K.M.; Liao, R.; Dorbala, S. AL (Light-Chain) Cardiac Amyloidosis: A Review of Diagnosis and Therapy. J. Am. Coll. Cardiol. 2016, 68, 1323–1341. [Google Scholar] [CrossRef]
- Yamamoto, H.; Yokochi, T. Transthyretin Cardiac Amyloidosis: An Update on Diagnosis and Treatment. ESC Heart Fail. 2019, 6, 1128–1139. [Google Scholar] [CrossRef]
- Dorbala, S.; Ando, Y.; Bokhari, S.; Dispenzieri, A.; Falk, R.H.; Ferrari, V.A.; Fontana, M.; Gheysens, O.; Gillmore, J.D.; Glaudemans, A.W.J.M.; et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI Expert Consensus Recommendations for Multimodality Imaging in Cardiac Amyloidosis: Part 2 of 2—Diagnostic Criteria and Appropriate Utilization. J. Nucl. Cardiol. 2020, 27, 659–673. [Google Scholar] [CrossRef] [PubMed]
- Paeng, J.C.; Choi, J.Y. Nuclear Imaging for Cardiac Amyloidosis: Bone Scan, SPECT/CT, and Amyloid-Targeting PET. Nucl. Med. Mol. Imaging 2021, 55, 61–70. [Google Scholar] [CrossRef]
- Jurcuţ, R.; Onciul, S.; Adam, R.; Stan, C.; Coriu, D.; Rapezzi, C.; Popescu, B.A. Multimodality Imaging in Cardiac Amyloidosis: A Primer for Cardiologists. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 833–844. [Google Scholar] [CrossRef]
- Velaga, J.; Liew, C.; Poh, A.C.C.; Lee, P.T.; Lath, N.; Low, S.C.; Bharadwaj, P. Multimodality Imaging in the Diagnosis and Assessment of Cardiac Amyloidosis. World J. Nucl. Med. 2022, 21, 173–183. [Google Scholar] [CrossRef]
- Martinez-Naharro, A.; Baksi, A.J.; Hawkins, P.N.; Fontana, M. Diagnostic Imaging of Cardiac Amyloidosis. Nat. Rev. Cardiol. 2020, 17, 413–426. [Google Scholar] [CrossRef]
- Fontana, M.; Chung, R.; Hawkins, P.N.; Moon, J.C. Cardiovascular Magnetic Resonance for Amyloidosis. Heart Fail. Rev. 2015, 20, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Slart, R.H.J.A.; Glaudemans, A.W.J.M.; Noordzij, W.; Bijzet, J.; Hazenberg, B.P.C.; Nienhuis, H.L.A. Time for New Imaging and Therapeutic Approaches in Cardiac Amyloidosis. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1402–1406. [Google Scholar] [CrossRef]
- Hawkins, P.N.; Lavender, J.P.; Pepys, M.B. Evaluation of Systemic Amyloidosis by Scintigraphy with 123I-Labeled Serum Amyloid P Component. N. Engl. J. Med. 1990, 323, 508–513. [Google Scholar] [CrossRef]
- Glaudemans, A.W.J.M.; Slart, R.H.J.A.; Zeebregts, C.J.; Veltman, N.C.; Tio, R.A.; Hazenberg, B.P.C.; Dierckx, R.A.J.O. Nuclear Imaging in Cardiac Amyloidosis. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 702–714. [Google Scholar] [CrossRef]
- Ross, J.C.; Hutt, D.F.; Burniston, M.; Page, J.; Steeden, J.A.; Gillmore, J.D.; Wechalekar, A.D.; Hawkins, P.N.; Fontana, M. Quantitation of 99mTc-DPD Uptake in Patients with Transthyretin-Related Cardiac Amyloidosis. Amyloid 2018, 25, 203–210. [Google Scholar] [CrossRef]
- Dorbala, S.; Ando, Y.; Bokhari, S.; Dispenzieri, A.; Falk, R.H.; Ferrari, V.A.; Fontana, M.; Gheysens, O.; Gillmore, J.D.; Glaudemans, A.W.J.M.; et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI Expert Consensus Recommendations for Multimodality Imaging in Cardiac Amyloidosis: Part 1 of 2—Evidence Base and Standardized Methods of Imaging. J. Nucl. Cardiol. 2019, 26, 2065–2123. [Google Scholar] [CrossRef] [PubMed]
- Gallegos, C.; Miller, E.J. Advances in PET-Based Cardiac Amyloid Radiotracers. Curr. Cardiol. Rep. 2020, 22, 40. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Uppal, D.; Wang, Y.C.; Xu, X.; Kokkinidis, D.G.; Travin, M.I.; Tauras, J.M. Nuclear Imaging for the Diagnosis of Cardiac Amyloidosis in 2021. Diagnostics 2021, 11, 996. [Google Scholar] [CrossRef]
- Wolk, D.A.; Zhang, Z.; Boudhar, S.; Clark, C.M.; Pontecorvo, M.J.; Arnold, S.E. Amyloid Imaging in Alzheimer’s Disease: Comparison of Florbetapir and Pittsburgh Compound-B Positron Emission Tomography. J. Neurol. Neurosurg. Psychiatry 2012, 83, 923–926. [Google Scholar] [CrossRef]
- Aimo, A.; Merlo, M.; Porcari, A.; Georgiopoulos, G.; Pagura, L.; Vergaro, G.; Sinagra, G.; Emdin, M.; Rapezzi, C. Redefining the Epidemiology of Cardiac Amyloidosis. A Systematic Review and Meta-Analysis of Screening Studies. Eur. J. Heart Fail. 2022, 24, 2342–2351. [Google Scholar] [CrossRef] [PubMed]
- Perugini, E.; Guidalotti, P.L.; Salvi, F.; Cooke, R.M.T.; Pettinato, C.; Riva, L.; Leone, O.; Farsad, M.; Ciliberti, P.; Bacchi-Reggiani, L.; et al. Noninvasive Etiologic Diagnosis of Cardiac Amyloidosis Using 99mTc-3,3-Diphosphono-1,2-Propanodicarboxylic Acid Scintigraphy. J. Am. Coll. Cardiol. 2005, 46, 1076–1084. [Google Scholar] [CrossRef]
- Ramsay, S.C.; Cuscaden, C. The Current Status of Quantitative SPECT/CT in the Assessment of Transthyretin Cardiac Amyloidosis. J. Nucl. Cardiol. 2020, 27, 1464–1468. [Google Scholar] [CrossRef]
- Dickson, J.C.; Armstrong, I.S.; Gabiña, P.M.; Denis-Bacelar, A.M.; Krizsan, A.K.; Gear, J.M.; Van den Wyngaert, T.; de Geus-Oei, L.-F.; Herrmann, K. EANM Practice Guideline for Quantitative SPECT-CT. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 980–995. [Google Scholar] [CrossRef]
- Gherghe, M.; Mutuleanu, M.-D.; Stanciu, A.E.; Irimescu, I.; Lazar, A.; Bacinschi, X.; Anghel, R.M. Quantitative Analysis of SPECT-CT Data in Metastatic Breast Cancer Patients—The Clinical Significance. Cancers 2022, 14, 273. [Google Scholar] [CrossRef]
- Qi, N.; Meng, Q.; You, Z.; Chen, H.; Shou, Y.; Zhao, J. Standardized Uptake Values of 99mTc-MDP in Normal Vertebrae Assessed Using Quantitative SPECT/CT for Differentiation Diagnosis of Benign and Malignant Bone Lesions. BMC Med. Imaging 2021, 21, 39. [Google Scholar] [CrossRef]
- Gherghe, M.; Lazar, A.M.; Simion, L.; Irimescu, I.-N.; Sterea, M.-C.; Mutuleanu, M.-D.; Anghel, R.M. Standardized Uptake Values on SPECT/CT: A Promising Alternative Tool for Treatment Evaluation and Prognosis of Metastatic Neuroendocrine Tumours. Diagnostics 2023, 13, 318. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Ramsay, S.C.; Lindsay, K.; Fong, W.; Patford, S.; Younger, J.; Atherton, J. Tc-HDP Quantitative SPECT/CT in Transthyretin Cardiac Amyloid and the Development of a Reference Interval for Myocardial Uptake in the Non-Affected Population. Eur. J. Hybrid Imaging 2018, 2, 17. [Google Scholar] [CrossRef] [PubMed]
- Caobelli, F.; Braun, M.; Haaf, P.; Wild, D.; Zellweger, M.J. Quantitative 99mTc-DPD SPECT/CT in Patients with Suspected ATTR Cardiac Amyloidosis: Feasibility and Correlation with Visual Scores. J. Nucl. Cardiol. 2020, 27, 1456–1463. [Google Scholar] [CrossRef]
- Bellevre, D.; Bailliez, A.; Delelis, F.; Blaire, T.; Agostini, D.; Mouquet, F.; Maréchaux, S.; Manrique, A. Quantitation of Myocardial 99mTc-HMDP Uptake with New SPECT/CT Cadmium Zinc Telluride (CZT) Camera in Patients with Transthyretin-Related Cardiac Amyloidosis: Ready for Clinical Use? J. Nucl. Cardiol. 2022, 29, 506–514. [Google Scholar] [CrossRef]
- Scully, P.R.; Morris, E.; Patel, K.P.; Treibel, T.A.; Burniston, M.; Klotz, E.; Newton, J.D.; Sabharwal, N.; Kelion, A.; Manisty, C.; et al. DPD Quantification in Cardiac Amyloidosis: A Novel Imaging Biomarker. JACC Cardiovasc. Imaging 2020, 13, 1353–1363. [Google Scholar] [CrossRef] [PubMed]
- Wollenweber, T.; Rettl, R.; Kretschmer-Chott, E.; Rasul, S.; Kulterer, O.; Rainer, E.; Raidl, M.; Schaffarich, M.P.; Matschitsch, S.; Stadler, M.; et al. In Vivo Quantification of Myocardial Amyloid Deposits in Patients with Suspected Transthyretin-Related Amyloidosis (ATTR). J. Clin. Med. 2020, 9, 3446. [Google Scholar] [CrossRef] [PubMed]
- Ren, C.; Ren, J.; Tian, Z.; Du, Y.; Hao, Z.; Zhang, Z.; Fang, W.; Li, F.; Zhang, S.; Hsu, B.; et al. Assessment of Cardiac Amyloidosis with 99mTc-Pyrophosphate (PYP) Quantitative SPECT. EJNMMI Phys. 2021, 8, 3. [Google Scholar] [CrossRef] [PubMed]
- Dorbala, S.; Park, M.-A.; Cuddy, S.; Singh, V.; Sullivan, K.; Kim, S.; Falk, R.H.; Taqueti, V.R.; Skali, H.; Blankstein, R.; et al. Absolute Quantitation of Cardiac 99mTc-Pyrophosphate Using Cadmium-Zinc-Telluride–Based SPECT/CT. J. Nucl. Med. 2021, 62, 716–722. [Google Scholar] [CrossRef]
- Ben-Haim, S.; Chicheportiche, A.; Goshen, E.; Arad, M.; Smekhov, M.; Menezes, L.J.; Elliott, P.M.; O’Mahoney, E.; Stern, E.; Yuzefovich, B.; et al. Quantitative SPECT/CT Parameters of Myocardial 99mTechnetium-3,3-Diphosphono-1,2-Propanodicarboxylic Acid (DPD) Uptake in Suspected Cardiac Transthyretin Amyloidosis. EJNMMI Res. 2021, 11, 86. [Google Scholar] [CrossRef]
- Kessler, L.; Fragoso Costa, P.; Kersting, D.; Jentzen, W.; Weber, M.; Lüdike, P.; Carpinteiro, A.; Oubari, S.; Hagenacker, T.; Thimm, A.; et al. Quantitative 99mTc-DPD-SPECT/CT Assessment of Cardiac Amyloidosis. J. Nucl. Cardiol. 2023, 30, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Avalon, J.C.; Fuqua, J.; Deskins, S.; Miller, T.; Conte, J.; Martin, D.; Marano, G.; Yanamala, N.; Mills, J.; Bianco, C.; et al. Quantitative Single Photon Emission Computed Tomography Derived Standardized Uptake Values on 99mTc-PYP Scan in Patients with Suspected ATTR Cardiac Amyloidosis. J. Nucl. Cardiol. 2023, 30, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.S.; Bokhari, S.; Damy, T.; Dorbala, S.; Drachman, B.M.; Fontana, M.; Grogan, M.; Kristen, A.V.; Lousada, I.; Nativi-Nicolau, J.; et al. Expert Consensus Recommendations for the Suspicion and Diagnosis of Transthyretin Cardiac Amyloidosis. Circ. Heart Fail. 2019, 12, e006075. [Google Scholar] [CrossRef] [PubMed]
- Gillmore, J.D.; Maurer, M.S.; Falk, R.H.; Merlini, G.; Damy, T.; Dispenzieri, A.; Wechalekar, A.D.; Berk, J.L.; Quarta, C.C.; Grogan, M.; et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation 2016, 133, 2404–2412. [Google Scholar] [CrossRef] [PubMed]
- Acampa, W.; Buechel, R.R.; Gimelli, A. Low Dose in Nuclear Cardiology: State of the Art in the Era of New Cadmium–Zinc–Telluride Cameras. Eur. Heart J.–Cardiovasc. Imaging 2016, 17, 591–595. [Google Scholar] [CrossRef]
- Panjer, M.; Dobrolinska, M.; Wagenaar, N.R.L.; Slart, R.H.J.A. Diagnostic Accuracy of Dynamic CZT-SPECT in Coronary Artery Disease. A Systematic Review and Meta-Analysis. J. Nucl. Cardiol. 2022, 29, 1686–1697. [Google Scholar] [CrossRef]
- Khor, Y.M.; Cuddy, S.A.M.; Singh, V.; Falk, R.H.; Di Carli, M.F.; Dorbala, S. 99mTc Bone-Avid Tracer Cardiac Scintigraphy: Role in Noninvasive Diagnosis of Transthyretin Cardiac Amyloidosis. Radiology 2023, 306, e221082. [Google Scholar] [CrossRef]
- Musumeci, M.B.; Cappelli, F.; Russo, D.; Tini, G.; Canepa, M.; Milandri, A.; Bonfiglioli, R.; Di Bella, G.; My, F.; Luigetti, M.; et al. Low Sensitivity of Bone Scintigraphy in Detecting Phe64Leu Mutation-Related Transthyretin Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2020, 13, 1314–1321. [Google Scholar] [CrossRef]
- Cuddy, S.A.M.; Dorbala, S.; Falk, R.H. Complexities and Pitfalls in Cardiac Amyloidosis. Circulation 2020, 142, 409–415. [Google Scholar] [CrossRef]
- Möckelind, S.; Axelsson, J.; Pilebro, B.; Lindqvist, P.; Suhr, O.B.; Sundström, T. Quantification of Cardiac Amyloid with [18F]Flutemetamol in Patients with V30M Hereditary Transthyretin Amyloidosis. Amyloid 2020, 27, 191–199. [Google Scholar] [CrossRef]
- Rauf, M.U.; Hawkins, P.N.; Cappelli, F.; Perfetto, F.; Zampieri, M.; Argiro, A.; Petrie, A.; Law, S.; Porcari, A.; Razvi, Y.; et al. Tc-99m Labelled Bone Scintigraphy in Suspected Cardiac Amyloidosis. Eur. Heart J. 2023. In press. [Google Scholar] [CrossRef]
- Oerlemans, M.I.F.J.; Rutten, K.H.G.; Minnema, M.C.; Raymakers, R.A.P.; Asselbergs, F.W.; de Jonge, N. Cardiac Amyloidosis: The Need for Early Diagnosis. Neth. Heart J. 2019, 27, 525–536. [Google Scholar] [CrossRef]
- Griffin, J.M.; Rosenthal, J.L.; Grodin, J.L.; Maurer, M.S.; Grogan, M.; Cheng, R.K. ATTR Amyloidosis: Current and Emerging Management Strategies: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncol. 2021, 3, 488–505. [Google Scholar] [CrossRef] [PubMed]
- Bellevre, D.; Bailliez, A.; Maréchaux, S.; Manrique, A.; Mouquet, F. First Follow-Up of Cardiac Amyloidosis Treated by Tafamidis, Evaluated by Absolute Quantification in Bone Scintigraphy. JACC Case Rep. 2021, 3, 133–135. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Calabretta, R.; Yu, J.; Binder, P.; Hu, S.; Hacker, M.; Li, X. Nuclear Molecular Imaging of Disease Burden and Response to Treatment for Cardiac Amyloidosis. Biology 2022, 11, 1395. [Google Scholar] [CrossRef] [PubMed]
- Schindler, T.H.; Sharma, M.; Valenta, I.; Imperiale, A.; Dilsizian, V. Potential Cardiac Amyloid PET/CT Imaging Targets for Differentiating Immunoglobulin Light Chain From Transthyretin Amyloidosis. Curr. Cardiol. Rep. 2021, 23, 76. [Google Scholar] [CrossRef] [PubMed]
- Genovesi, D.; Vergaro, G.; Giorgetti, A.; Marzullo, P.; Scipioni, M.; Santarelli, M.F.; Pucci, A.; Buda, G.; Volpi, E.; Emdin, M. [18F]-Florbetaben PET/CT for Differential Diagnosis Among Cardiac Immunoglobulin Light Chain, Transthyretin Amyloidosis, and Mimicking Conditions. JACC Cardiovasc. Imaging 2021, 14, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Cuddy, S.A.M.; Bravo, P.E.; Falk, R.H.; El-Sady, S.; Kijewski, M.F.; Park, M.-A.; Ruberg, F.L.; Sanchorawala, V.; Landau, H.; Yee, A.J.; et al. Improved Quantification of Cardiac Amyloid Burden in Systemic Light Chain Amyloidosis: Redefining Early Disease? JACC Cardiovasc. Imaging 2020, 13, 1325–1336. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | No. Patients | 99mTc-Labelled Radiopharmaceutical | Time from Injection to SPECT | Phantom Study | Segmentation Software | SPECT/CT Parameters | Planar Indices |
|---|---|---|---|---|---|---|---|
| Ramsay et al. [33] | 29 | HDP | 3 h | No | Syngo.via (Siemens) | SUVmax | Perugini score |
| Caobelli et al. [34] | 13 | DPD | 3.5–4 h | No | Syngo.via (Siemens) | SUVmax, SUVpeak, nSUVmax, nSUVpeak, | Perugini score |
| Bellevre et al. [35] | 30 | HMDP | 167 ± 25 min | Yes | Q.Metrix (General Electric Healthcare) | SUVmax, ID, HLR, MBR | Perugini score |
| Scully et al. [36] | 100 | DPD | 3 h | No | Hybrid Recon (Hermes Medical Solutions) | SUVpeak, Cardiac SUV retention index | Perugini score, H/WB, H/CL |
| Wollenweber et al. [37] | 32 | DPD | 2.5 h | Yes | Hermes Hybrid 3D (Hermes Medical Solutions) | SUVpeak, nSUVpeak, wSUVpeak | Perugini score, H/WB, H/CL |
| Ren et al. [38] | 37 | PYP | 1 h | Yes | MyoFlowQ | SUVmax, SUVmean, SUVmedian | Perugini score, H/CL |
| Dorbala et al. [39] | 72 | PYP | 2.5–3 h | Yes | MIM | SUVmax, SUVmean, CAA, ID | NA |
| Ben-Haim et al. [40] | 28 | DPD | 3 h | No | Q.Volumetrix MI | SUVmax, SMaT20, SMaT40, SMaT60 | Perugini score |
| Kessler et al. [41] | 136 | DPD | 3 h | Yes | Pmod v3.2 | SUVmax, MBR*, MVR | Perugini score |
| Avalon et al. [42] | 77 | PYP | 1 h and 3 h | No | NA | SUVmax, SUVmin, SUVmean, Cardiac SUV retention index | Perugini score, H/CL |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gherghe, M.; Lazar, A.M.; Sterea, M.-C.; Spiridon, P.M.; Motas, N.; Gales, L.N.; Coriu, D.; Badelita, S.N.; Mutuleanu, M.-D. Quantitative SPECT/CT Parameters in the Assessment of Transthyretin Cardiac Amyloidosis—A New Dimension of Molecular Imaging. J. Cardiovasc. Dev. Dis. 2023, 10, 242. https://doi.org/10.3390/jcdd10060242
Gherghe M, Lazar AM, Sterea M-C, Spiridon PM, Motas N, Gales LN, Coriu D, Badelita SN, Mutuleanu M-D. Quantitative SPECT/CT Parameters in the Assessment of Transthyretin Cardiac Amyloidosis—A New Dimension of Molecular Imaging. Journal of Cardiovascular Development and Disease. 2023; 10(6):242. https://doi.org/10.3390/jcdd10060242
Chicago/Turabian StyleGherghe, Mirela, Alexandra Maria Lazar, Maria-Carla Sterea, Paula Monica Spiridon, Natalia Motas, Laurentia Nicoleta Gales, Daniel Coriu, Sorina Nicoleta Badelita, and Mario-Demian Mutuleanu. 2023. "Quantitative SPECT/CT Parameters in the Assessment of Transthyretin Cardiac Amyloidosis—A New Dimension of Molecular Imaging" Journal of Cardiovascular Development and Disease 10, no. 6: 242. https://doi.org/10.3390/jcdd10060242