
Intracoronary Administration of Microencapsulated HGF in a Reperfused Myocardial Infarction Swine Model
 , , , ,
, , , ,
Abstract
:1. Introduction
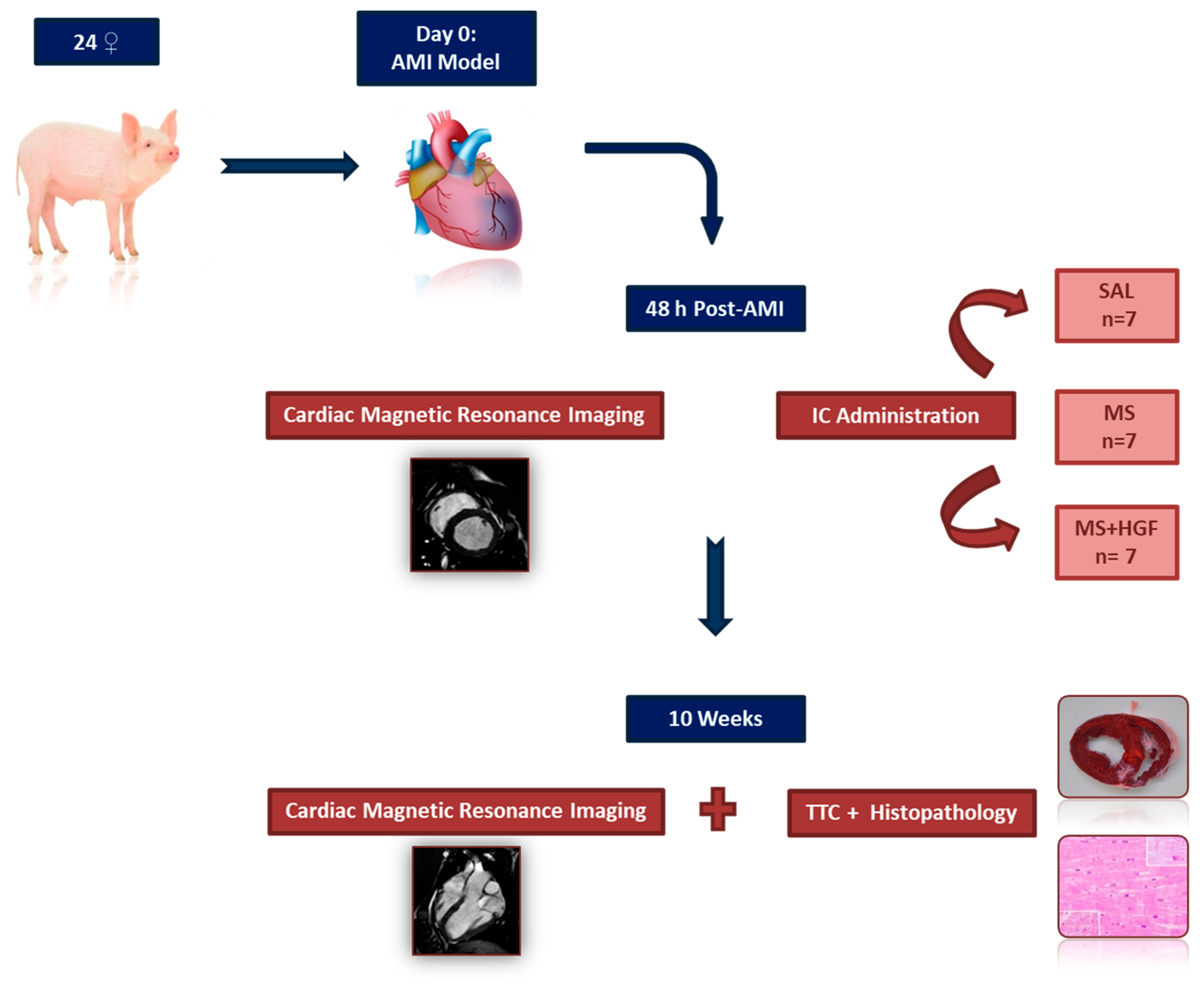
2. Materials and Methods
2.1. Anesthesia and Analgesia
2.2. Myocardial Infarction Induction
2.3. Cardiac Magnetic Resonance Imaging (cMR)
2.4. Treatment
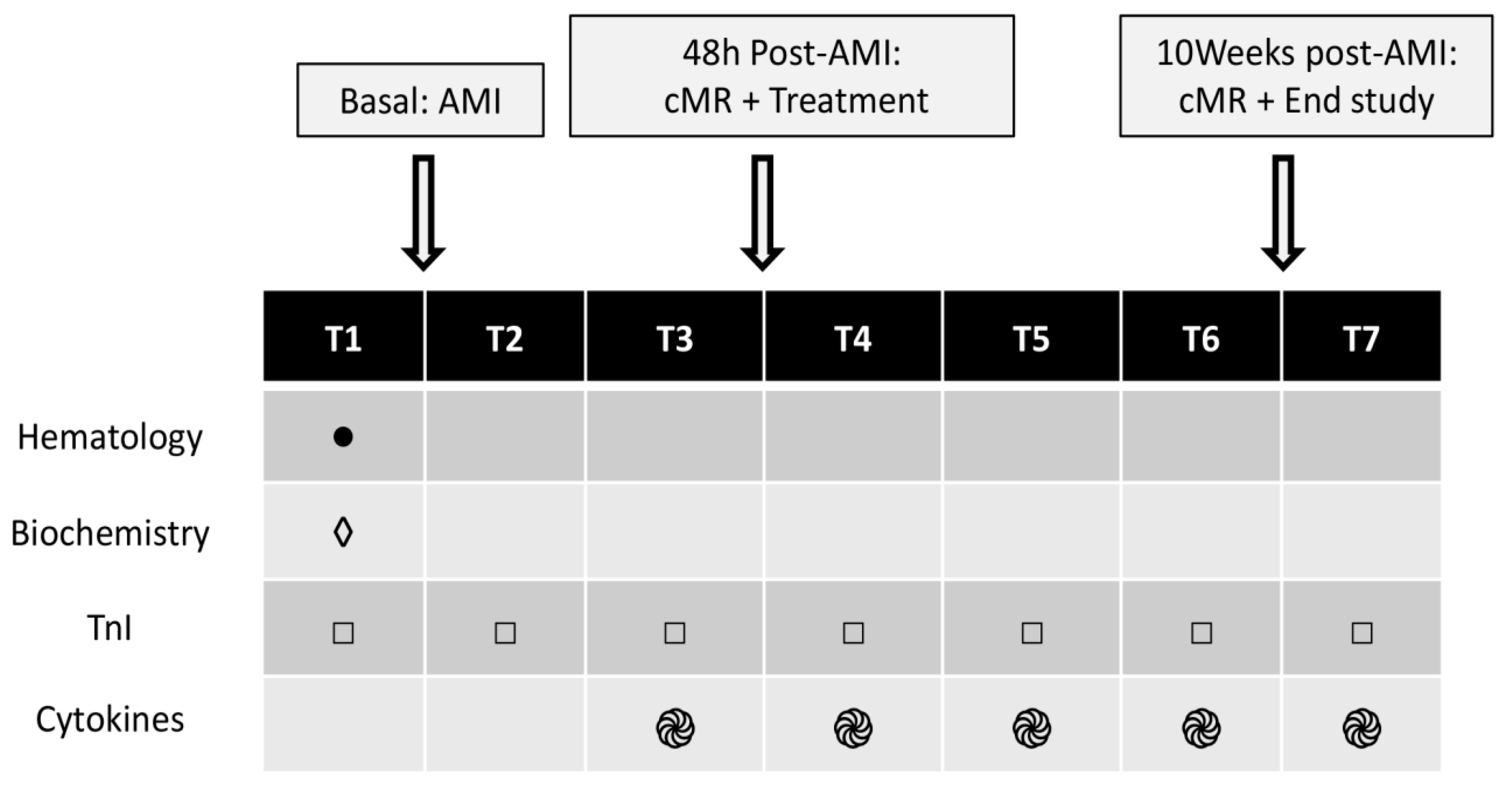
2.5. Blood Tests
2.6. End of Study: cMR2 and Histology
2.7. Statistical Analysis
3. Results
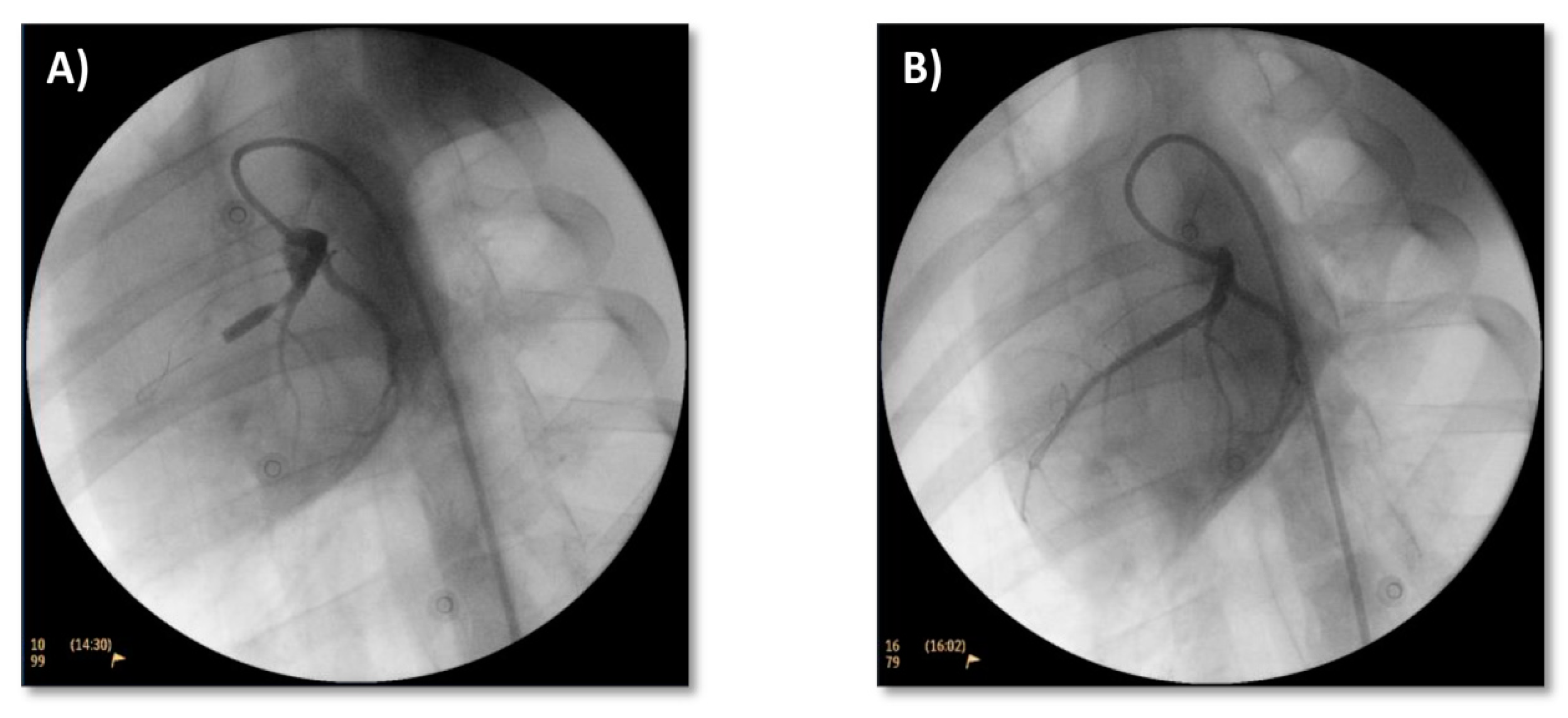
3.1. Model Induction
3.2. Treatment
3.2.1. Coronary Flow and ECG
3.2.2. Cardiac Enzymes
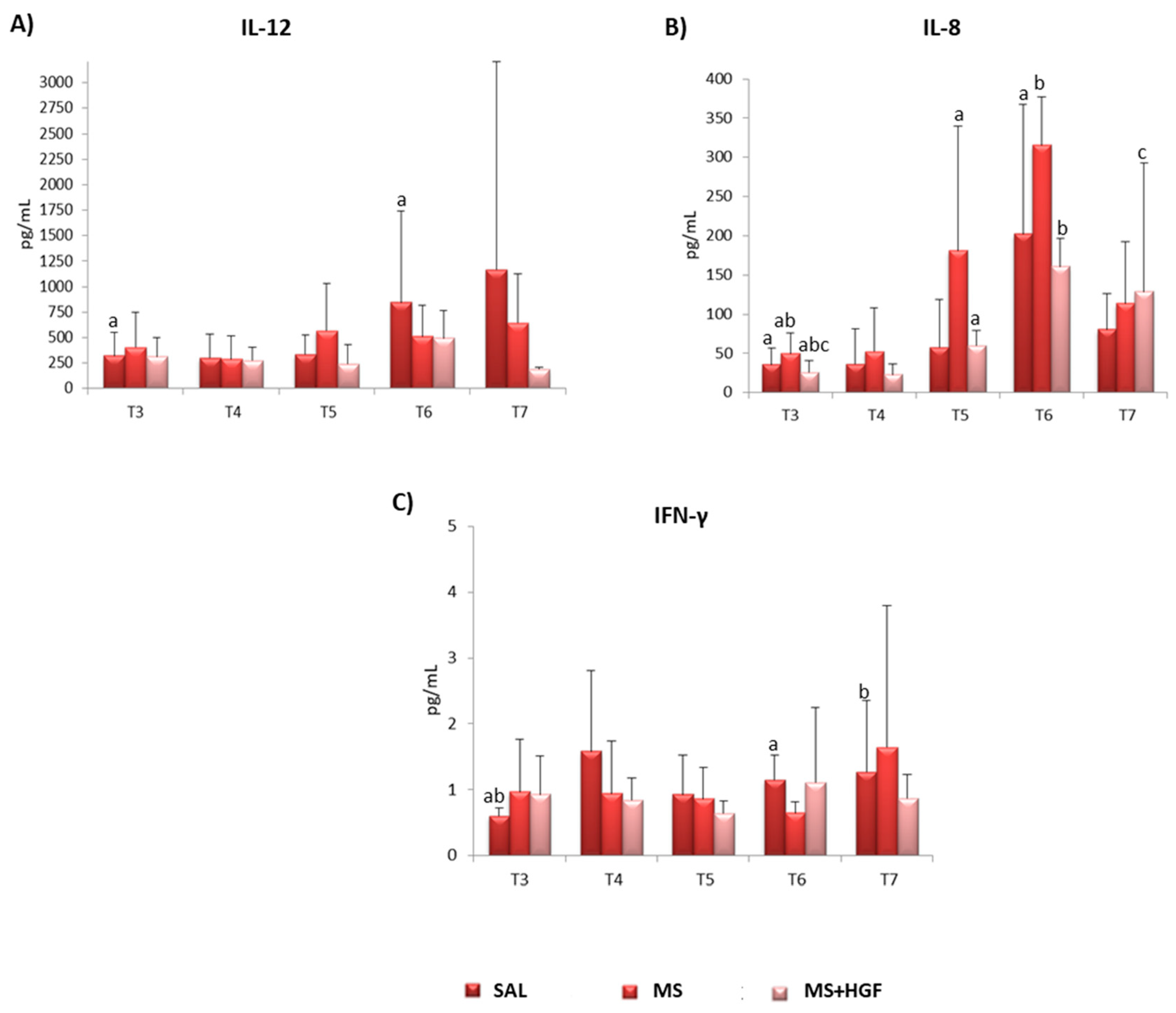
3.2.3. Cytokines
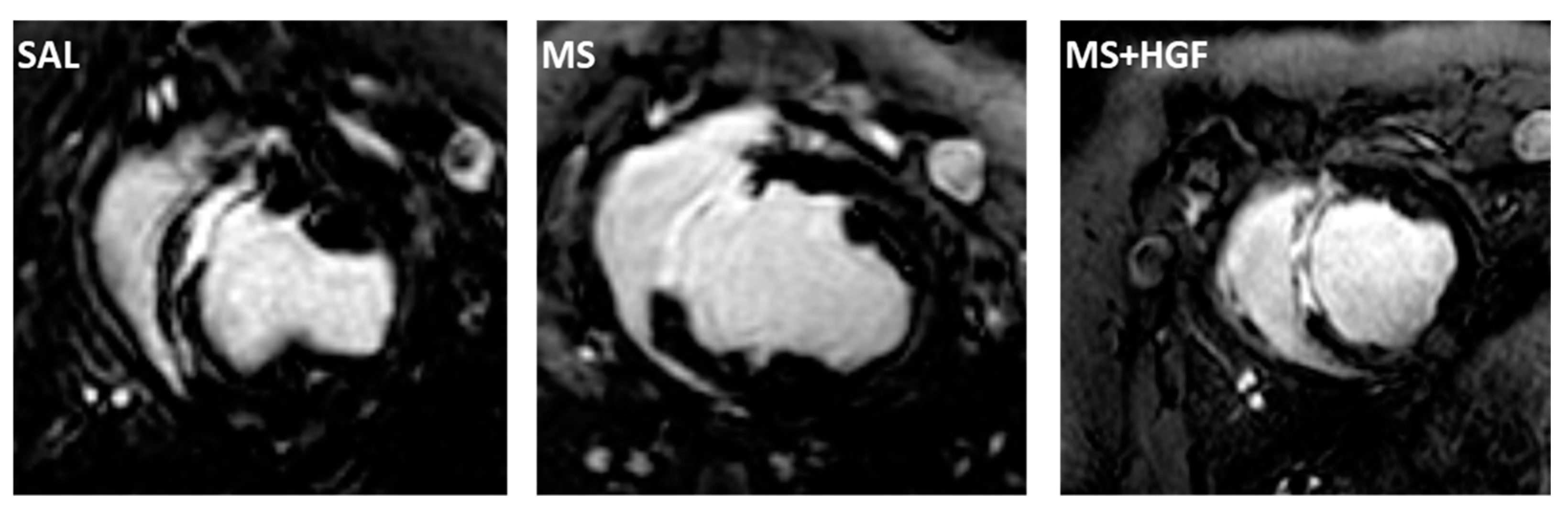
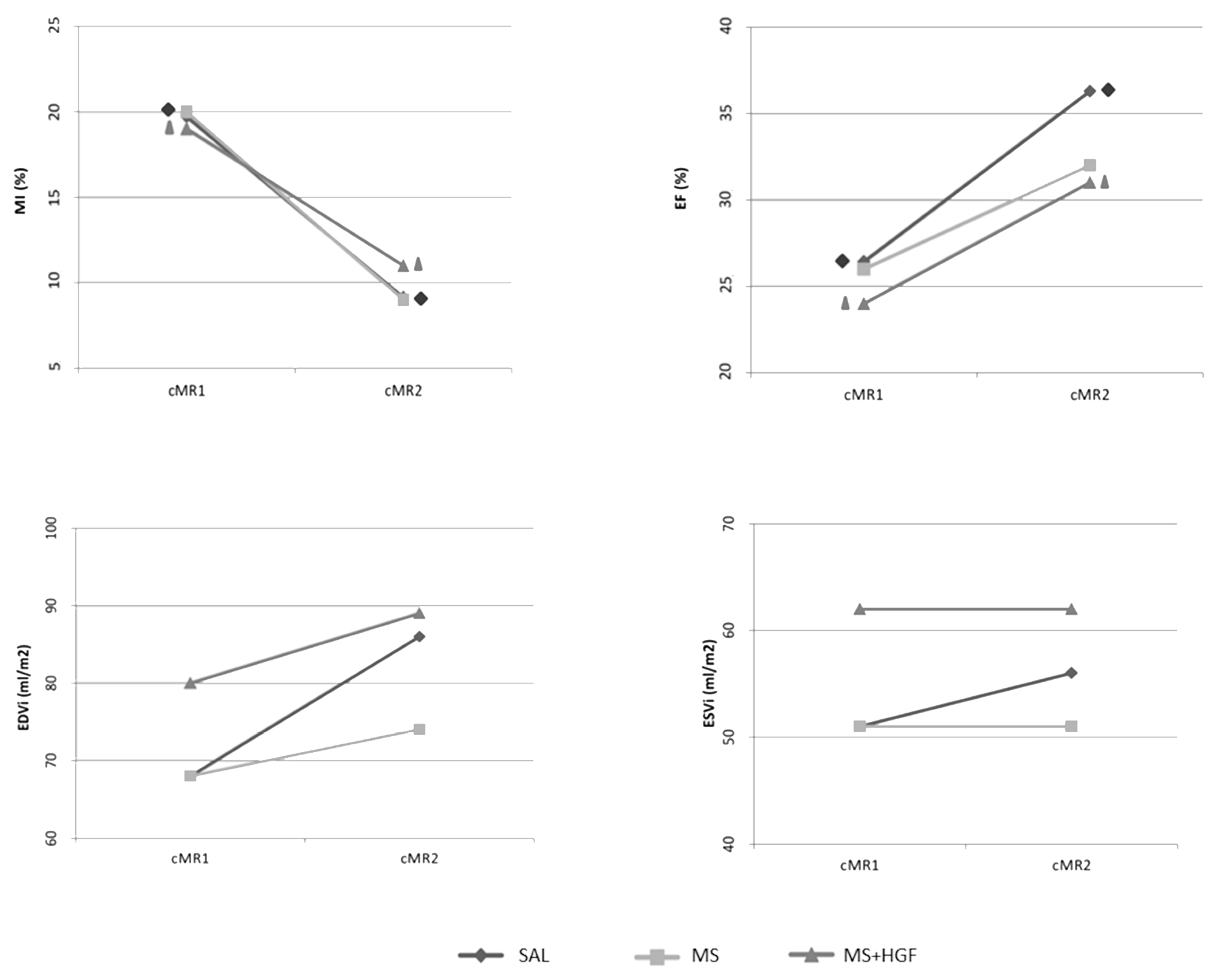
3.3. cMR
3.4. End of Study
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics—2018 Update: A Report from the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [PubMed]
- Rossello, X.; Lobo-Gonzalez, M.; Ibanez, B. Pathophysiology and therapy of myocardial ischaemia/reperfusion syndrome. Eur. Heart J. Acute Cardiovasc. Care 2019, 8, 443–456. [Google Scholar] [CrossRef] [PubMed]
- Chamuleau, S.A.; Van Der Naald, M.; Climent, A.M.; Kraaijeveld, A.O.; Wever, K.E.; Duncker, D.J.; Fernández-Avilés, F.; Bolli, R. Translational research in cardiovascular repair: A call for a paradigm shift. Circ. Res. 2018, 122, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Tompkins, B.A.; Balkan, W.; Winkler, J.; Gyöngyösi, M.; Goliasch, G.; Fernández-Avilés, F.; Hare, J.M. Preclinical Studies of Stem Cell Therapy for Heart Disease. Circ. Res. 2018, 122, 1006–1020. [Google Scholar] [CrossRef] [PubMed]
- Eschenhagen, T.; Bolli, R.; Braun, T.; Field, L.J.; Fleischmann, B.K.; Frisén, J.; Giacca, M.; Hare, J.M.; Houser, S.; Lee, R.T.; et al. Cardiomyocyte Regeneration: A Consensus Statement. Circulation 2017, 136, 680–686. [Google Scholar] [CrossRef]
- Lewis, F.C.; Kumar, S.D.; Ellison-Hughes, G.M. Non-invasive strategies for stimulating endogenous repair and regenerative mechanisms in the damaged heart. Pharmacol. Res. 2018, 127, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Gallo, S.; Sala, V.; Gatti, S.; Crepaldi, T. HGF/Met Axis in Heart Function and Cardioprotection. Biomedicines 2014, 2, 247–262. [Google Scholar] [CrossRef] [Green Version]
- Gallo, S.; Sala, V.; Gatti, S.; Crepaldi, T. Cellular and molecular mechanisms of HGF/Met in the cardiovascular system. Clin. Sci. 2015, 129, 1173–1193. [Google Scholar] [CrossRef]
- Rong, S.L.; Wang, X.L.; Wang, Y.C.; Wu, H.; Zhou, X.D.; Wang, Z.K.; Wang, Y.C.; Xue, C.S.; Li, B.; Gao, D.L. Anti-inflammatory activities of hepatocyte growth factor in post-ischemic heart failure. Acta Pharmacol. Sin. 2018, 39, 1613–1621. [Google Scholar] [CrossRef] [Green Version]
- Fan, Z.; Guan, J. Antifibrotic therapies to control cardiac fibrosis. Biomater. Res. 2016, 20, 13. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.S.; Wang, H.; Zhang, Q.L.; Yang, Z.J.; Kong, F.X.; Wu, C.T. Hepatocyte Growth Factor Gene Therapy for Ischemic Diseases. Hum. Gene Ther. 2018, 29, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Koudstaal, S.; Bastings, M.M.; Feyen, D.A.; Waring, C.D.; Van Slochteren, F.J.; Dankers, P.Y.; Torella, D.; Sluijter, J.P.; Nadal-Ginard, B.; Doevendans, P.A.; et al. Sustained delivery of insulin-like growth factor-1/hepatocyte growth factor stimulates endogenous cardiac repair in the chronic infarcted pig heart. J. Cardiovasc. Transl. Res. 2014, 7, 232–241. [Google Scholar] [CrossRef] [Green Version]
- Ellison, G.M.; Torella, D.; Dellegrottaglie, S.; Perez-Martinez, C.; Perez de Prado, A.; Vicinanza, C.; Purushothaman, S.; Galuppo, V.; Iaconetti, C.; Waring, C.D.; et al. Endogenous cardiac stem cell activation by insulin-like growth factor-1/hepatocyte growth factor intracoronary injection fosters survival and regeneration of the infarcted pig heart. J. Am. Coll. Cardiol. 2011, 58, 977–986. [Google Scholar]
- Ylä-Herttuala, S.; Bridges, C.; Katz, M.G.; Korpisalo, P. Angiogenic gene therapy in cardiovascular diseases: Dream or vision? Eur. Heart J. 2017, 38, 1365–1371. [Google Scholar] [PubMed] [Green Version]
- Fernández-Jiménez, R.; Sánchez-González, J.; Agüero, J.; García-Prieto, J.; López-Martín, G.J.; García-Ruiz, J.M.; Molina-Iracheta, A.; Rosselló, X.; Fernández-Friera, L.; Pizarro, G.; et al. Myocardial edema after ischemia/reperfusion is not stable and follows a bimodal pattern: Imaging and histological tissue characterization. J. Am. Coll. Cardiol. 2015, 65, 315–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piek, A.; de Boer, R.A.; Silljé, H.H. The fibrosis-cell death axis in heart failure. Heart Fail Rev. 2016, 21, 199–211. [Google Scholar] [CrossRef] [Green Version]
- Baez-Diaz, C.; Blanco-Blazquez, V.; Sanchez-Margallo, F.M.; Bayes-Genis, A.; Gonzalez, I.; Abad, A.; Steendam, R.; Franssen, O.; Palacios, I.; Sanchez, B.; et al. Microencapsulated Insulin-Like Growth Factor-1 therapy improves cardiac function and reduces fibrosis in a porcine acute myocardial infarction model. Sci. Rep. 2020, 10, 7166. [Google Scholar] [CrossRef] [PubMed]
- Suarez, S.L.; Muñoz, A.; Mitchell, A.; Braden, R.L.; Luo, C.; Cochran, J.R.; Almutairi, A.; Christman, K.L. Degradable acetalated dextran microparticles for tunable release of an engineered hepatocyte growth factor fragment. ACS Biomater. Sci. Eng. 2016, 2, 197–204. [Google Scholar] [CrossRef] [Green Version]
- Crisostomo, V.; Baez-Diaz, C.; Maestre, J.; Garcia-Lindo, M.; Sun, F.; Casado, J.G.; Blazquez, R.; Abad, J.L.; Palacios, I.; Rodriguez-Borlado, L. Delayed administration of allogeneic cardiac stem cell therapy for acute myocardial infarction could ameliorate adverse remodeling: Experimental study in swine. J. Transl. Med. 2015, 13, 156. [Google Scholar]
- Fishbein, M.C.; Maclean, D.; Maroko, P.R. The histopathologic evolution of myocardial infarction. Chest 1978, 73, 843–849. [Google Scholar] [CrossRef] [Green Version]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Socie. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed] [Green Version]
- Crisostomo, V.; Sun, F.; Maynar, M.; Baez-Diaz, C.; Blanco, V.; Garcia-Lindo, M.; Uson-Gargallo, J.; Sánchez-Margallo, F.M. Common swine models of cardiovascular disease for research and training. Lab Anim. 2016, 45, 67–74. [Google Scholar]
- de Prado, A.P.; Cuellas-Ramón, C.; Regueiro-Purriños, M.; Gonzalo-Orden, J.M.; Pérez-Martínez, C.; Altónaga, J.R.; García-Iglesias, M.J.; Orden-Recio, M.A.; García-Marín, J.F.; Fernández-Vázquez, F. Closed-chest experimental porcine model of acute myocardial infarction-reperfusion. J. Pharmacol. Toxicol. Methods 2009, 60, 301–306. [Google Scholar]
- Chen, Y.; Shao, D.B.; Zhang, F.X.; Zhang, J.; Yuan, W.; Man, Y.L.; Du, W.; Liu, B.X.; Wang, D.W.; Li, X.R.; et al. Establishment and evaluation of a swine model of acute myocardial infarction and reperfusion-ventricular fibrillation-cardiac arrest using the interventional technique. J. Chin. Med. Assoc. 2013, 76, 491–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuellas-Ramón, C.; de Prado, A.P.; Pérez-Martínez, C.; Diego-Nieto, A.; Gonzalo-Orden, J.M.; Fernández-Vázquez, F. Investigación traslacional en isquemia, infarto de miocardio y reperfusión. Rev. Esp. Cardiol. Supl. 2013, 13, 57–63. [Google Scholar]
- Sun, R.; Li, X.; Liu, M.; Zeng, Y.; Chen, S.; Zhang, P. Advances in stem cell therapy for cardiovascular disease (Review). Int. J. Mol. Med. 2016, 38, 23–29. [Google Scholar]
- Janssens, S.; Dubois, C.; Bogaert, J.; Theunissen, K.; Deroose, C.; Desmet, W.; Kalantzi, M.; Herbots, L.; Sinnaeve, P.; Dens, J.; et al. Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevation myocardial infarction: Double-blind, randomised controlled trial. Lancet 2006, 367, 113–121. [Google Scholar]
- Dib, N.; Khawaja, H.; Varner, S.; McCarthy, M.; Campbell, A. Cell therapy for cardiovascular disease: A comparison of methods of delivery. J. Cardiovasc. Transl. Res. 2011, 4, 177–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, B.; Kemp, B.J.; Chareonthaitawee, P.; Reed, C.; Schmeckpeper, J.; Sorajja, P.; Russell, S.; Araoz, P.; Riederer, S.J.; Caplice, N.M. Dynamic Tracking During Intracoronary Injection of 18F-FDG-Labeled Progenitor Cell Therapy for Acute Myocardial Infarction. J. Nucl. Med. 2007, 48, 1708–1714. [Google Scholar] [CrossRef] [Green Version]
- Díez-Delhoyo, F.; Gutiérrez-Ibañes, E.; Loughlin, G.; Sanz-Ruiz, R.; Vázquez-Álvarez, M.E.; Sarnago-Cebada, F.; Angulo-Llanos, R.; Casado-Plasencia, A.; Elízaga, J.; Diáz, F.F.A. Coronary physiology assessment in the catheterization laboratory. World J. Cardiol. 2015, 7, 525–538. [Google Scholar] [CrossRef]
- de Jong, R.; van Hout, G.P.; Houtgraaf, J.H.; Kazemi, K.; Wallrapp, C.; Lewis, A.; Pasterkamp, G.; Hoefer, I.E.; Duckers, H.J. Intracoronary infusion of encapsulated glucagon-like peptide-1-eluting mesenchymal stem cells preserves left ventricular function in a porcine model of acute myocardial infarction. Circ. Cardiovasc. Interv. 2014, 7, 673–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez de Prado, A.; Fernández-Vázquez, F.; Cuellas-Ramón, J.C.; Gibson, C. Coronariografía: Más allá de la antomía coronaria. Rev. Esp. Cardiol. 2006, 59, 596–608. [Google Scholar] [PubMed]
- Konijnenberg, L.S.F.; Damman, P.; Duncker, D.J.; Robert, A. Pathophysiology and diagnosis of coronary microvascular dysfunction in ST-elevation myocardial infarction. Cardiovasc. Res. 2020, 116, 787–805. [Google Scholar] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2019, 40, 237–269. [Google Scholar]
- Davidson, S.M.; Arjun, S.; Basalay, M.V.; Bell, R.M.; Bromage, D.I.; Bøtker, H.E.; Carr, R.D.; Cunningham, J.; Ghosh, A.K.; Heusch, G.; et al. The 10th Biennial Hatter Cardiovascular Institute workshop: Cellular protection—Evaluating new directions in the setting of myocardial infarction, ischaemic stroke, and cardio-oncology. Basic Res. Cardiol. 2018, 113, 43. [Google Scholar] [PubMed] [Green Version]
- Bulluck, H.; Hammond-Haley, M.; Weinmann, S.; Martinez-Macias, R.; Hausenloy, D.J. Myocardial Infarct Size by CMR in Clinical Cardioprotection Studies: Insights From Randomized Controlled Trials. JACC Cardiovasc. Imaging 2017, 10, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Jablonowski, R.; Engblom, H.; Kanski, M.; Nordlund, D.; Koul, S.; van der Pals, J.; Englund, E.; Heiberg, E.; Erlinge, D.; Carlsson, M.; et al. Contrast-Enhanced CMR Overestimates Early Myocardial Infarct Size: Mechanistic Insights Using ECV Measurements on Day 1 and Day 7. JACC Cardiovasc. Imaging 2015, 8, 1379–1389. [Google Scholar] [CrossRef] [Green Version]
- Khan, J.N.; McCann, G.P. Cardiovascular magnetic resonance imaging assessment of outcomes in acute myocardial infarction. World J. Cardiol. 2017, 9, 109–133. [Google Scholar] [CrossRef] [Green Version]
- Prabhu, S.D.; Frangogiannis, N.G. The biological basis for cardiac repair after myocardial infarction. Circ. Res. 2016, 119, 91–112. [Google Scholar]
- Ghugre, N.R.; Pop, M.; Thomas, R.; Newbigging, S.; Qi, X.; Barry, J.; Strauss, B.H.; Wright, G.A. Hemorrhage promotes inflammation and myocardial damage following acute myocardial infarction: Insights from a novel preclinical model and cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2017, 19, 50. [Google Scholar]
- Ibanez, B.; Aletras, A.H.; Arai, A.E.; Arheden, H.; Bax, J.; Berry, C.; Bucciarelli-Ducci, C.; Croisille, P.; Dall’Armellina, E.; Dharmakumar, R.; et al. Cardiac MRI Endpoints in Myocardial Infarction Experimental and Clinical Trials: JACC Scientific Expert Panel. J. Am. Coll. Cardiol. 2019, 74, 238–256. [Google Scholar] [CrossRef]
- Rodriguez-Palomares, J.F.; Gavara, J.; Ferreira-González, I.; Valente, F.; Rios, C.; Rodríguez-García, J.; Bonanad, C.; Garcia del Blanco, B.; Miñana, G.; Mutuberria, M.; et al. Prognostic Value of Initial Left Ventricular Remodeling in Patients with Reperfused STEMI. JACC Cardiovasc. Imaging 2019, 12, 2445–2456. [Google Scholar]
- Ibáñez, B.; Rossello, X. Left Ventricular Remodeling Is No Longer a Relevant Outcome After Myocardial Infarction. JACC Cardiovasc. Imaging 2019, 12, 2457–2459. [Google Scholar] [CrossRef]
- Revilla, A.; López, J.; Arnold, R.; Sanchez, P.L.; Villa, A.; Pinedo, M.; Fernandez-Aviles, F.; San Román, J.A. Evolución a largo plazo de la función ventricular tras la terapia celular intracoronaria en el infarto agudo de miocardio. Rev. Esp. Cardiol. 2011, 64, 334–337. [Google Scholar] [PubMed]
- Prat-Vidal, C.; Crisóstomo, V.; Moscoso, I.; Báez-Díaz, C.; Blanco-Blázquez, V.; Gómez-Mauricio, G.; Albericio, G.; Aguilar, S.; Fernández-Santos, M.E.; Fernández-Avilés, F.; et al. Intracoronary Delivery of Porcine Cardiac Progenitor Cells Overexpressing IGF-1 and HGF in a Pig Model of Sub-Acute Myocardial Infarction. Cells 2021, 10, 2571. [Google Scholar] [PubMed]
- Bartekova, M.; Radosinska, J.; Jelemensky, M. Role of cytokines and inflammation in heart function during health and disease. Heart Fail Rev. 2018, 23, 733–758. [Google Scholar]
- Frangogiannis, N.G. Cell biological mechanisms in regulation of the post-infarction inflammatory response. Curr. Opin. Physiol. 2018, 1, 7–13. [Google Scholar] [PubMed]
- Frangogiannis, N.G.; Entman, M.L. Chemokines in myocardial ischemia. Trends Cardiovasc. Med. 2005, 15, 163–169. [Google Scholar] [CrossRef]
- Crisostomo, V.; Baez, C.; Abad, J.L.; Sanchez, B.; Alvarez, V.; Rosado, R.; Gómez-Mauricio, G.; Gheysens, O.; Blanco-Blazquez, V.; Blazquez, R.; et al. Dose-dependent improvement of cardiac function in a swine model of acute myocardial infarction after intracoronary administration of allogeneic heart-derived cells. Stem Cell Res. Ther. 2019, 10, 152. [Google Scholar]
- Wang, W.; Wang, M.Q.; Wang, H.; Gao, W.; Zhang, Z.; Zhao, S.; Xu, H.Z.; Chen, B.; Zhu, M.X.; Wu, Z.Z.; et al. Effects of Adenovirus-Mediated Hepatocyte Growth Factor Gene Therapy on Postinfarct Heart Function: Comparison of Single and Repeated Injections. Hum. Gene Ther. 2016, 27, 643–651. [Google Scholar] [CrossRef]
- Kim, J.S.; Hwang, H.Y.; Cho, K.R.; Park, E.A.; Lee, W.; Paeng, J.C.; Lee, D.S.; Kim, H.K.; Sohn, D.W.; Kim, K.B. Intramyocardial transfer of hepatocyte growth factor as an adjunct to CABG: Phase I clinical study. Gene Ther. 2013, 20, 717–722. [Google Scholar] [PubMed] [Green Version]
- Meng, H.; Chen, B.; Tao, Z.; Xu, Z.; Wang, L.; Weizhu, J.; Hong, Y.; Liu, X.; Wang, H.; Wang, L.; et al. Safety and Efficacy of Adenovirus Carrying Hepatocyte Growth Factor Gene by Percutaneous Endocardial Injection for Treating Post-infarct Heart Failure: A Phase IIa Clinical Trial. Curr. Gene Ther. 2018, 18, 125–130. [Google Scholar] [PubMed]
- Gómez-Mauricio, G.; Moscoso, I.; Martín-Cancho, M.F.; Crisóstomo, V.; Prat-Vidal, C.; Báez-Díaz, C.; Sánchez-Margallo, F.M.; Bernad, A. Combined administration of mesenchymal stem cells overexpressing IGF-1 and HGF enhances neovascularization but moderately improves cardiac regeneration in a porcine model. Stem Cell Res. Ther. 2016, 7, 94. [Google Scholar] [PubMed] [Green Version]
- Lindsey, M.L.; Bolli, R.; Canty Jr, J.M.; Du, X.J.; Frangogiannis, N.G.; Frantz, S.; Gourdie, R.G.; Holmes, J.W.; Jones, S.P.; Kloner, R.A.; et al. Guidelines for experimental models of myocardial ischemia and infarction. Am. J. Physiol. Heart Circ. Physiol. 2018, 314, H812–H838. [Google Scholar]
- Zwetsloot, P.P.; Kouwenberg, L.H.J.A.; Sena, E.S.; Eding, J.E.; Den Ruijter, H.M.; Sluijter, J.P.G.; Pasterkamp, G.; Doevendans, P.A.; Hoefer, I.E.; Chamuleau, S.A.J.; et al. Optimization of large animal MI models; A systematic analysis of control groups from preclinical studies. Sci. Rep. 2017, 7, 1–11. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DRUG | PRESENTATION | DOSAGE |
|---|---|---|
| Amiodarone | 200 mg tablets | 400 mg/24 h, p. o. From 1 week before AMI and up to 3 days after treatment |
| Acetylsalicylic acid | 500 mg tablets | 500 mg/24 h p. o. from one day before AMI until end of study. |
| Sucralfate | 1 g oral suspension | 1 sachet/24 h p. o. from beginning to end of study. |
| Group | Pre-Treatment TIMI Flow | Post-Treatment TIMI Flow | End of Study TIMI Flow |
|---|---|---|---|
| SAL | 3 (n = 2) | 3 (n = 2) | 3 (n = 6) |
| 2 (n = 5) | 2 (n = 5) | 2 (n = 1) | |
| MS | 3 (n = 4) | 3 (n = 1) | 3 (n = 4) |
| 2 (n = 3) | 2 (n = 5) | 2 (n = 1) | |
| MS+HGF | 3 (n = 3) | 3 (n = 2) | 3 (n = 5) |
| 2 (n = 4) | 2 (n = 4) | 2 (n = 2) | |
| 1 (n = 1) |
| Group | TnI T3 (μg/L) | TnI T4 (μg/L) | TnI T5 (μg/L) | TnI T6(μg/L) |
|---|---|---|---|---|
| SAL | 11.65 ± 6.45 | 10.57 ± 5.11 a | 7 ± 4.17 ab | 0.18 ± 0.24 b |
| MS | 12.97 ± 12.92 | 7.98 ± 4.03 a | 3.59 ± 2.87 ab | 0.08 ± 0.06 b |
| MS+HGF | 12.6 ± 5.58 | 12.43 ± 5.96 a | 7.7 ± 3.09 ab | 0.17 ± 0.16 b |
| Group | T3 | T4 | T5 | T6 | T7 |
|---|---|---|---|---|---|
| SAL | 322.1 ± 227.8 a | 300.8 ± 235.5 | 332.6 ± 193.5 | 845.3 ± 900.3 a | 1164 ± 2044.8 |
| MS | 403.6 ± 342.9 | 285.7 ± 230.1 | 568 ± 460.3 | 510.5 ± 305.7 | 644.9 ± 476.4 |
| MS+HGF | 312 ± 188.5 | 272.6 ± 136.8 | 242.3 ± 185.9 | 495 ± 266.9 | 190.8 ± 17.8 |
| Group | T3 | T4 | T5 | T6 | T7 |
|---|---|---|---|---|---|
| SAL | 35.9 ± 21.6 a | 36.2 ± 45.1 | 57.9 ± 61.1 | 202.6 ± 164.8 a | 80.5 ± 45.5 |
| MS | 49.7 ± 25.9 ab | 52.6 ± 55.9 | 181.1 ± 158.6 a | 315.5 ± 61.9 b | 113.5 ± 79 |
| MS+HGF | 25.9 ± 14.6 abc | 23.2 ± 14 | 59.9 ± 19.1 a | 160.5 ± 36.6 b | 128.5 ± 164.2 c |
| Group | T3 | T4 | T5 | T6 | T7 |
|---|---|---|---|---|---|
| SAL | 0.6 ± 0.1 ab | 1.6 ± 1.2 | 0.9 ± 0.6 | 1.2 ± 0.4 a | 1.3 ± 1.1 b |
| MS | 1 ± 0.8 | 0.9 ± 0.8 | 0.9 ± 0.4 | 0.7 ± 0.2 | 1.6 ± 2.2 |
| MS+HGF | 0.9 ± 0.6 | 0.8 ± 0.3 | 0.6 ± 0.2 | 1.1± 1.1 | 0.9± 0.4 |
| cMR Parameter | SAL | MS | MS+HGF |
|---|---|---|---|
| %MI cMR1 | 20 ± 8 a | 20 ± 5 | 19 ± 3 a |
| %MI cMR2 | 9 ± 4 a | 9 ± 3 | 11 ± 2 a |
| ∆MI (%) | −11 ± 6 | −15 ± 7 | −9 ± 4 |
| EF (%) cMR1 | 26 ± 9 a | 26 ± 5 | 24 ± 8 a |
| EF (%) cMR2 | 36 ± 8 a | 32 ± 10 | 31 ± 5 a |
| ∆EF (%) | 10 ± 9 | 6 ±9 | 7 ±7 |
| EDVi (mL/m2) cMR1 | 68 ± 16 | 68 ± 10 | 80 ± 14 |
| EDVi (mL/m2) cMR2 | 86 ± 22 | 74 ± 13 | 89 ± 16 |
| ∆EDVi (mL/m2) | 18 ± 27 | 7 ±13 | 9 ± 19 |
| ESVi (mL/m2) cMR1 | 51 ± 17 | 51 ± 9 | 62 ± 15 |
| ESVi (mL/m2) cMR2 | 56 ± 21 | 51 ± 12 | 62 ± 14 |
| ∆ESVi (mL/m2) | 5 ± 26 | 1 ± 11 | 0.5 ± 18 |
| Group | Infarction | Necrosis- Apoptosis | Fibrosis | Angiogenesis | Inflammation | Calcification |
|---|---|---|---|---|---|---|
| SAL | 1 | 0 | 1 | 1 | 1 | 3 |
| 1 | 0 | 1 | 1 | 2 | 1 | |
| 1 | 0 | 1 | 1 | 2 | 1 | |
| 1 | 0 | 1 | 1 | 1 | 1 | |
| 1 | 0 | 1 | 1 | 1 | 0 | |
| MS | 1 | 0 | 1 | 1 | 1 | 3 |
| 1 | 0 | 1 | 1 | 3 | 1 | |
| 1 | 1 | 1 | 1 | 1 | 2 | |
| MS+HGF | 1 | 0 | 1 | 1 | 1 | 0 |
| 1 | 0 | 1 | 1 | 1 | 0 | |
| 1 | 1 | 1 | 1 | 0 | 3 | |
| 1 | 0 | 1 | 1 | 1 | 1 | |
| 1 | 0 | 1 | 1 | 1 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanco-Blázquez, V.; Báez-Díaz, C.; Sánchez-Margallo, F.M.; González-Bueno, I.; Martín, H.; Blázquez, R.; Casado, J.G.; Usón, A.; Solares, J.; Palacios, I.; et al. Intracoronary Administration of Microencapsulated HGF in a Reperfused Myocardial Infarction Swine Model. J. Cardiovasc. Dev. Dis. 2023, 10, 86. https://doi.org/10.3390/jcdd10020086
Blanco-Blázquez V, Báez-Díaz C, Sánchez-Margallo FM, González-Bueno I, Martín H, Blázquez R, Casado JG, Usón A, Solares J, Palacios I, et al. Intracoronary Administration of Microencapsulated HGF in a Reperfused Myocardial Infarction Swine Model. Journal of Cardiovascular Development and Disease. 2023; 10(2):86. https://doi.org/10.3390/jcdd10020086
Chicago/Turabian StyleBlanco-Blázquez, Virginia, Claudia Báez-Díaz, Francisco Miguel Sánchez-Margallo, Irene González-Bueno, Helena Martín, Rebeca Blázquez, Javier G. Casado, Alejandra Usón, Julia Solares, Itziar Palacios, and et al. 2023. "Intracoronary Administration of Microencapsulated HGF in a Reperfused Myocardial Infarction Swine Model" Journal of Cardiovascular Development and Disease 10, no. 2: 86. https://doi.org/10.3390/jcdd10020086