
Beraprost and Overall Survival in Cats with Chronic Kidney Disease




Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Case Selection
2.2. Study Design
2.3. Data Analysis
3. Results
3.1. Baseline Characteristics of All Cats in Cohort A
3.2. Multivariable Analyses of All Cats in Cohort A
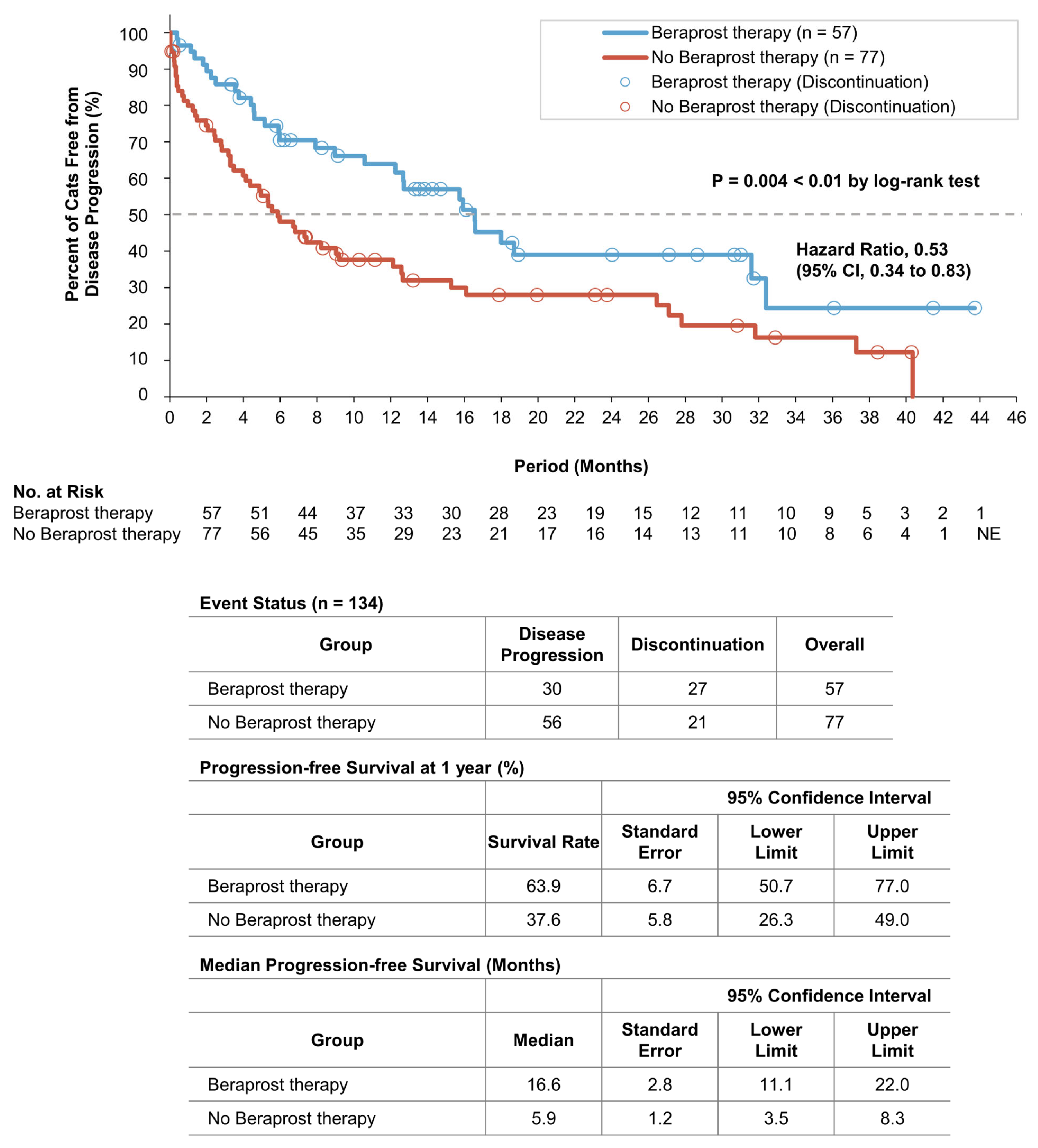
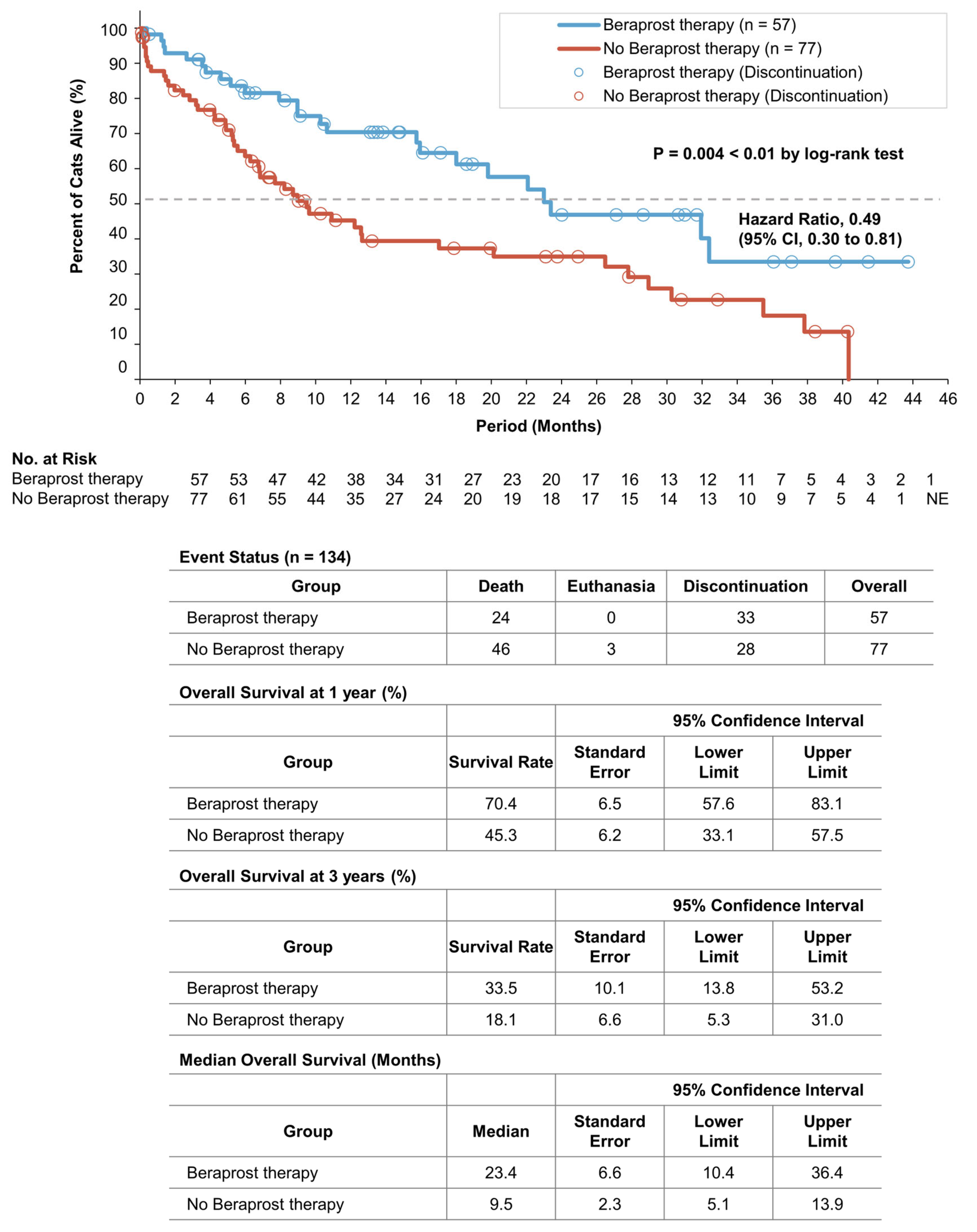
3.3. Survival Analyses of the Two Groups in Cohort A
3.4. Baseline Characteristics of All Cats in Cohort B
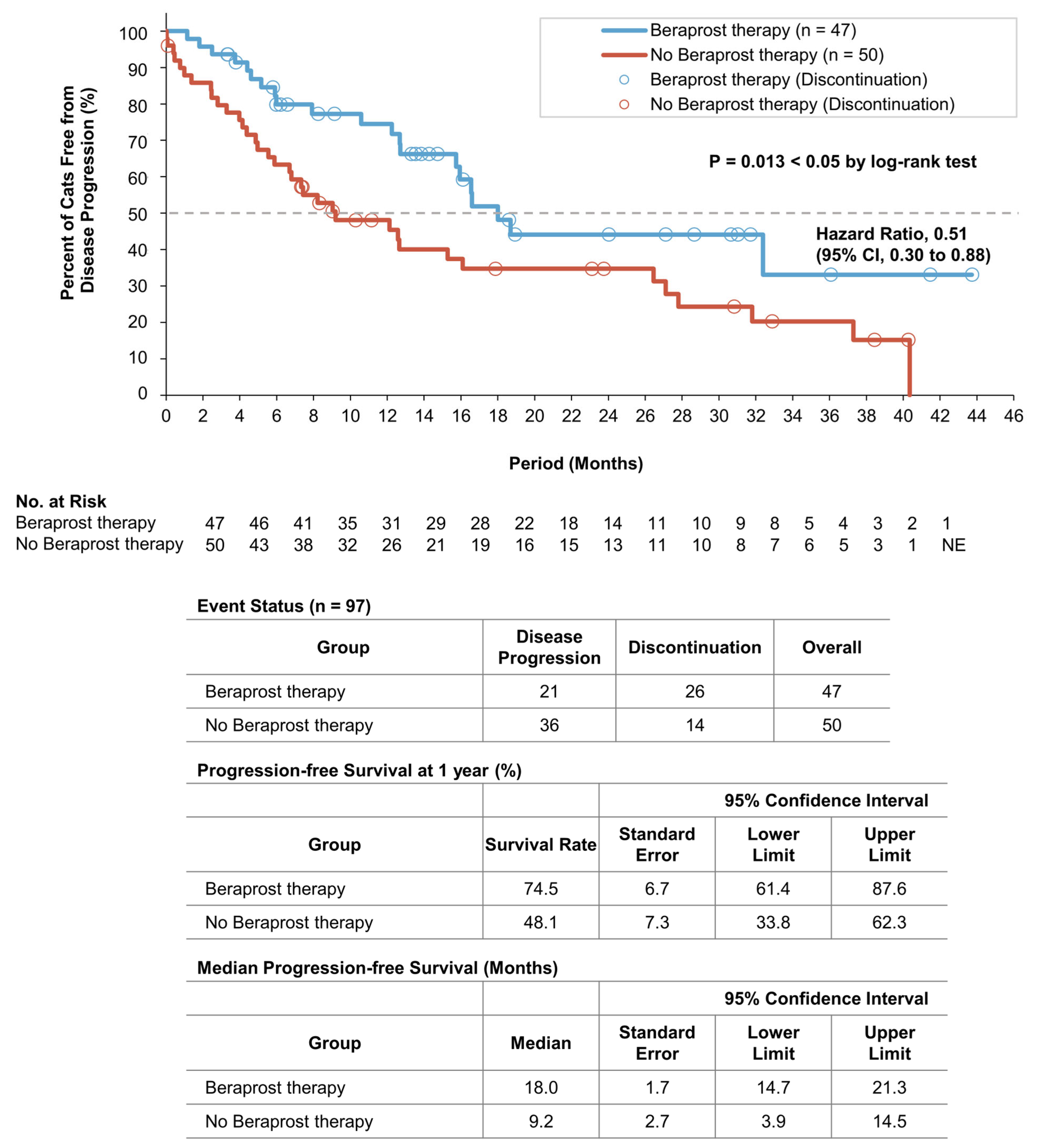
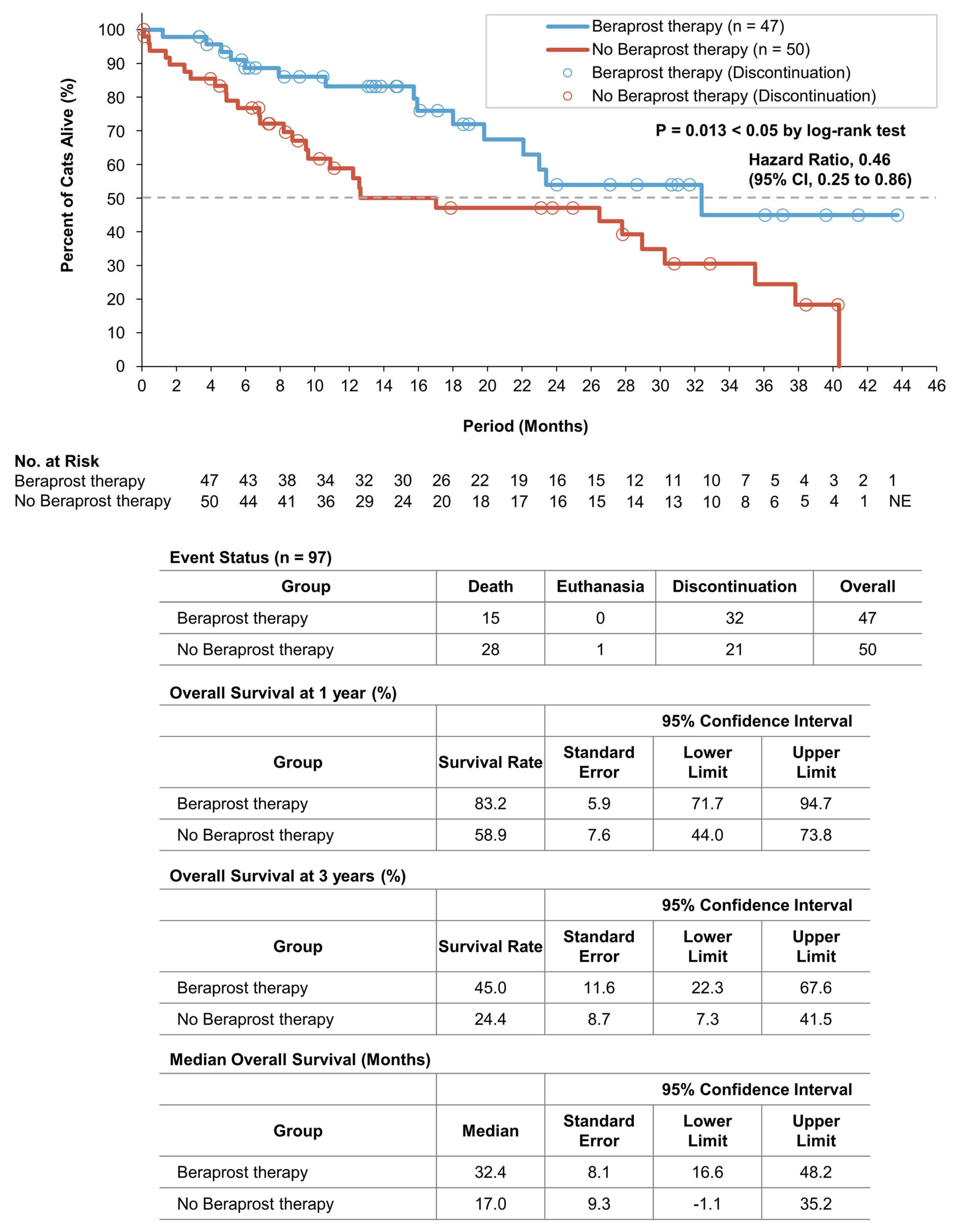
3.5. Survival Analyses of the Two Groups in Cohort B
3.6. Onset of Chronic Disorders of the Two Groups in Cohort A
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sparkes, A.H.; Caney, S.; Chalhoub, S.; Elliott, J.; Finch, N.; Gajanayake, I.; Langston, C.; Lefebvre, H.P.; White, J.; Quimby, J. ISFM Consensus Guidelines on the Diagnosis and Management of Feline Chronic Kidney Disease. J. Feline Med. Surg. 2016, 18, 219–239. [Google Scholar] [CrossRef] [PubMed]
- International Renal Interest Society. IRIS Treatment Recommendations for CKD. 2019. Available online: http://iris-kidney.com/guidelines/recommendations.html (accessed on 28 March 2021).
- Pouchelon, J.L.; Atkins, C.E.; Bussadori, C.; Oyama, M.A.; Vaden, S.L.; Bonagura, J.D.; Chetboul, V.; Cowgill, L.D.; Elliot, J.; Francey, T.; et al. Cardiovascular-renal axis disorders in the domestic dog and cat: A veterinary consensus statement. J. Small Anim. Pract. 2015, 56, 537–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, T.L.; Peak, K.J.; Brodbelt, D.; Elliott, J.; Syme, H.M. Survival and the development of azotemia after treatment of hyperthyroid cats. J. Vet. Intern. Med. 2010, 24, 863–869. [Google Scholar] [CrossRef]
- Perez-Lopez, L.; Boronat, M.; Melian, C.; Saavedra, P.; Brito-Casillas, Y.; Wagner, A.M. Assessment of the association between diabetes mellitus and chronic kidney disease in adult cats. J. Vet. Intern. Med. 2019, 33, 1921–1925. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.-H.; Kanellis, J.; Hugo, C.; Truong, L.; Anderson, S.; Kerjaschki, D.; Schreiner, G.F.; Johnson, R.J. Role of the microvascular endothelium in progressive renal disease. J. Am. Soc. Nephrol. 2002, 13, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Endemann, D.H.; Schiffrin, E.L. Endothelial dysfunction. J. Am. Soc. Nephrol. 2004, 15, 1983–1992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jepson, R.; Syme, H.; Vallance, C.; Elliott, J. Plasma asymmetric dimethylarginine, symmetric dimethylarginine, l-arginine, and nitrite/nitrate concentrations in cats with chronic kidney disease and hypertension. J. Vet. Intern. Med. 2008, 22, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Kainoh, M.N.S.; Nakadate, T. Cytoprotective Action of Beraprost Sodium against Peroxide-Induced Damage in Vascular Endothelial Cells. Pharmacology 1992, 45, 61–70. [Google Scholar] [CrossRef]
- Niwano, K.; Arai, M.; Tomaru, K.; Uchiyama, T.; Ohyama, Y.; Kurabayashi, M. Transcriptional stimulation of the eNOS gene by the stable prostacyclin analogue beraprost is mediated through cAMP-responsive element in vascular endothelial cells: Close link between PGI2 signal and NO pathways. Circ. Res. 2003, 93, 523–530. [Google Scholar] [CrossRef]
- Matsumoto, K.; Morishita, R.; Tomita, N.; Moriguchi, A.; Yamasaki, K.; Aoki, M.; Nakamura, T.; Higaki, J.; Ogihara, T. Impaired endothelial dysfunction in diabetes mellitus rats was restored by oral administration of prostaglandin I2 analogue. J. Endocrinol. 2002, 175, 217–223. [Google Scholar] [CrossRef] [Green Version]
- Goto, Y.; Yamaguchi, S.; Tamura, M.; Mochizuki, H.; Kurumatani, H.; Okano, K.; Miyamoto, M. A prostacyclin analog prevents the regression of renal microvascular network by inhibiting mitochondria-dependent apoptosis in the kidney of rat progressive glomerulonephritis. Prostaglandins Other Lipid Mediat. 2014, 112, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, S.; Inada, C.; Tamura, M.; Sato, N.; Yamada, M.; Itaba, S.; Okazaki, S.; Matsuura, H.; Fujii, S.; Matsuda, F.; et al. Beraprost sodium improves survival rates in anti-glomerular basement membrane glomerulonephritis and 5/6 nephrectomized chronic kidney disease rats. Eur. J. Pharmacol. 2013, 714, 325–331. [Google Scholar] [CrossRef]
- Takenaka, M.; Iio, A.; Sato, R.; Sakamoto, T.; Kurumatani, H.; KT-140 Clinical Study Group. A Double-blind, Placebo-controlled, Multicenter, Prospective, Randomized Study of Beraprost Sodium Treatment for Cats with Chronic Kidney Disease. J. Vet. Intern. Med. 2018, 32, 236–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakrabarti, S.; Syme, H.M.; Elliott, J. Clinicopathological variables predicting progression of azotemia in cats with chronic kidney disease. J. Vet. Intern. Med. 2012, 26, 275–281. [Google Scholar] [CrossRef] [PubMed]
- King, J.N.; Tasker, S.; Gunn-Moore, D.A.; Strehlau, G.; BENRIC (benazepril in renal insufficiency in cats) Study Group. Prognostic factors in cats with chronic kidney disease. J. Vet. Intern. Med. 2007, 21, 906–916. [Google Scholar] [CrossRef]
- Feinstein, A.R. An additional basic science for clinical medicine: II. The limitations of randomized trials. Ann. Intern. Med. 1983, 99, 544–550. [Google Scholar] [CrossRef]
- Black, N. Why we need observational studies to evaluate the effectiveness of health care. BMJ 1996, 312, 1215–1218. [Google Scholar] [CrossRef] [Green Version]
- Elliott, J.; Barber, P.J. Feline CKD: Clinical findings in 80 cases diagnosed between 1992 and 1995. J. Small Anim. Pract. 1998, 39, 78–85. [Google Scholar] [CrossRef]
- Syme, H.M.; Markwell, P.J.; Pfeiffer, D.; Elliott, J. Survival of cats with naturally occurring CKD is related to severity of proteinuria. J. Vet. Intern. Med. 2006, 20, 528–535. [Google Scholar] [CrossRef]
- Freeman, L.M.; Lachaud, M.P.; Matthews, S.; Rhodes, L.; Zollers, B. Evaluation of Weight Loss Over Time in Cats with Chronic Kidney Disease. J. Vet. Intern. Med. 2016, 30, 1661–1666. [Google Scholar] [CrossRef] [Green Version]
- Sassnau, R. Epidemiological investigation on the prevalence of feline hyperthyroidism in an urban population in Germany. Tierärztliche Praxis Kleintiere 2006, 34, 450–457. [Google Scholar]
- Miyamoto, Y.; Miyata, I.; Kurobane, K. Prevalence of feline hyperthyroidism in Osaka and the Chugoku region. J. Jpn. Vet. Med. Assoc. 2002, 55, 289–292. [Google Scholar] [CrossRef]
- Wakeling, J.; Elliott, J.; Syme, H. Evaluation of predictors for the diagnosis of hyperthyroidism in cats. J. Vet. Intern. Med. 2011, 25, 1057–1065. [Google Scholar] [CrossRef] [PubMed]
- Paige, C.F.; Abbott, J.A.; Elvinger, F.; Pyle, R.L. Prevalence of cardiomyopathy in apparently healthy cats. J. Am. Vet. Med. Assoc. 2009, 234, 1398–1403. [Google Scholar] [CrossRef] [Green Version]
- Payne, J.R.; Brodbelt, D.C.; Luis Fuentes, V. Cardiomyopathy prevalence in 780 apparently healthy cats in rehoming centres (the CatScan study). J. Vet. Cardiol. 2015, 17 (Suppl. 1), S244–S257. [Google Scholar] [CrossRef] [Green Version]
- Gouni, V.; Chetboul, V.; Pouchelon, J.L.; Carlos Sampedrano, C.; Maurey, C.; Lefebvre, H.P. Azotemia in cats with feline hypertrophic cardiomyopathy: Prevalence and relationships with echocardiographic variables. J. Vet. Cardiol. 2008, 10, 117–123. [Google Scholar] [CrossRef]
- Wormser, C.; Mariano, A.; Holmes, E.S.; Aronson, L.R.; Volk, S.W. Post-transplant malignant neoplasia associated with cyclosporine-based immunotherapy: Prevalence, risk factors and survival in feline renal transplant recipients. Vet. Comp. Oncol. 2016, 14, e126–e134. [Google Scholar] [CrossRef]
- Owens, J.M.D.F.; Gilbertson, S.R. Pancreatic disease in the cat. JAAHA 1975, 11, 83–89. [Google Scholar]
- Geddes, R.F.; Elliott, J.; Syme, H.M. Relationship between plasma fibroblast growth factor-23 concentration and survival time in cats with chronic kidney disease. J. Vet. Intern. Med. 2015, 29, 1494–1501. [Google Scholar] [CrossRef]
- Boyd, L.M.; Langston, C.; Thompson, K.; Zivin, K.; Imanishi, M. Survival in cats with naturally occurring chronic kidney disease (2000–2002). J. Vet. Intern. Med. 2008, 22, 1111–1117. [Google Scholar] [CrossRef] [Green Version]
- Jepson, R.E.; Elliott, J.; Brodbelt, D.; Syme, H.M. Effect of control of systolic blood pressure on survival in cats with systemic hypertension. J. Vet. Intern. Med. 2007, 21, 402–409. [Google Scholar] [CrossRef]
- Syme, H.M. Proteinuria in cats. Prognostic marker or mediator? J. Feline Med. Surg. 2009, 11, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Mizutani, H.; Koyama, H.; Watanabe, T.; Kitagawa, H.; Nakano, M.; Kajiwara, K.; King, J.N. Evaluation of the clinical efficacy of benazepril in the treatment of chronic renal insufficiency in cats. J. Vet. Intern. Med. 2006, 20, 1074–1079. [Google Scholar] [CrossRef]
- King, J.N.; Gunn-Moore, D.A.; Tasker, S.; Gleadhill, A.; Strehlau, G.; Benazepril in Renal Insufficiency in Cats Study Group. Tolerability and efficacy of benazepril in cats with chronic kidney disease. J. Vet. Intern. Med. 2006, 20, 1054–1064. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Mishina, M. Effects of benazepril hydrochloride in cats with experimentally induced or spontaneously occurring CKD. J. Vet. Med. Sci. 2007, 69, 1015–1023. [Google Scholar] [CrossRef] [Green Version]
- Sent, U.; Gossl, R.; Elliott, J.; Syme, H.M.; Zimmering, T. Comparison of Efficacy of Long-term Oral Treatment with Telmisartan and Benazepril in Cats with Chronic Kidney Disease. J. Vet. Intern. Med. 2015, 29, 1479–1487. [Google Scholar] [CrossRef]
- Kwiatkowska, M.; Hoppe, S.; Pomianowski, A.; Tipold, A. Reactive seizures in cats: A retrospective study of 64 cases. Vet. J. 2019, 244, 1–6. [Google Scholar] [CrossRef]
- Hatamizadeh, P.; Fonarow, G.C.; Budoff, M.J.; Darabian, S.; Kovesdy, C.P.; Kalantar-Zadeh, K. Cardiorenal syndrome: Pathophysiology and potential targets for clinical management. Nat. Rev. Nephrol. 2013, 9, 99–111. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 730) | Beraprost Prescription | ||||
|---|---|---|---|---|---|
| Yes (n = 124) | No (n = 606) | ||||
| IRIS | Stage 1 | number | 143 | 13 | 130 |
| Stage 2 | number | 369 | 37 | 332 | |
| Stage 3 | number | 134 | 57 | 77 | |
| Stage 4 | number | 84 | 17 | 67 | |
| Total (n = 134) | Beraprost Therapy (n = 57) | No Beraprost Therapy (n = 77) | p Value | ||
|---|---|---|---|---|---|
| Age (years) | median (25th, 75th percentile) | 15.3 (10.5, 17.3) | 15.9 (13.0, 17.3) | 15.1 (8.6, 17.4) | 0.254 |
| Weight (kg) | median (25th, 75th percentile) | 3.6 (3.0, 4.4) | 3.8 (3.1, 4.4) | 3.4 (2.8, 4.4) | 0.142 |
| Sex | |||||
| Female | number (%) | 62 (46.3) | 30 (52.6) | 32 (41.6) | 0.224 |
| Male | number (%) | 72 (53.7) | 27 (47.4) | 45 (58.4) | |
| Neutered | number (%) | 115 (85.8) | 46 (80.7) | 69 (89.6) | 0.210 |
| Breeds | |||||
| Domestic Shorthair | number (%) | 91 (67.9) | 37 (64.9) | 54 (70.1) | 0.577 |
| Japanese Bobtail | number (%) | 7 (5.2) | 3 (5.3) | 4 (5.2) | |
| American Shorthair | number (%) | 6 (4.5) | 3 (5.3) | 3 (3.9) | |
| Other | number (%) | 30 (22.4) | 14 (24.5) | 16 (20.8) | |
| Biochemistry | |||||
| Creatinine (mg/dL) | median (25th, 75th percentile) | 3.3 (3.0, 3.7) | 3.3 (3.0, 3.7) | 3.3 (3.0, 3.7) | 0.767 |
| Urea (mg/dL) | median (25th, 75th percentile) | 42.0 (35.0, 60.0) | 38.0 (31.0, 52.5) | 46.0 (37.0, 70.0) ** | 0.001 |
| Phosphate (mg/dL) | median (25th, 75th percentile) | 4.9 (4.0, 6.1) | 4.6 (3.9, 5.3) | 5.3 (4.2, 6.8) ** | 0.006 |
| Calcium (mg/dL) | median (25th, 75th percentile) | 9.7 (9.2, 10.1) | 9.8 (9.4, 10.4) * | 9.6 (9.0, 10.0) | 0.016 |
| Potassium (mmol/L) | median (25th, 75th percentile) | 3.9 (3.5, 4.2) | 3.9 (3.6, 4.2) | 3.9 (3.5, 4.3) | 0.445 |
| Hematology | |||||
| Packed cell volume (%) | median (25th, 75th percentile) | 35.0 (30.0, 40.0) | 36.0 (31.0, 41.0) | 33.5 (29.5, 40.0) | 0.075 |
| Urinalysis | |||||
| Urine specific gravity | median (25th, 75th percentile) | 1.014 (1.012, 1.018) | 1.014 (1.012, 1.018) | 1.014 (1.012, 1.018) | 0.800 |
| Urine protein (mg/dL) | mean (SD) | 59.6 (167.9) | 27.5 (60.1) | 90.0 (223.6) * | 0.048 |
| Blood pressure measurement | |||||
| Systolic blood pressure (mmHg) | median (25th, 75th percentile) | 153.0 (132.0, 165.0) | 153.0 (132.0, 165.0) | 151.5 (132.8, 160.3) | 0.976 |
| Treatment | |||||
| Beraprost (RAPROS) | number (%) | 57 (42.5%) | 57 (100.0%) ** | 0 (0.0%) | <0.001 |
| Dose (μg/kg twice daily) | mean (SD, range) | 15.0 (4.0, 7.1–26.2) | 15.0 (4.0, 7.1–26.2) ** | 0 (0, 0–0) | <0.001 |
| Subcutaneous fluid therapy (total) | number (%) | 106 (79.1%) | 42 (73.7%) | 64 (83.1%) | 0.203 |
| At clinic | number (%) | 87 (64.9%) | 32 (56.1%) | 55 (71.4%) | 0.071 |
| At home | number (%) | 72 (53.7%) | 28 (49.1%) | 44 (57.1%) | 0.385 |
| Kidney Diet (total) | number (%) | 75 (56.0%) | 35 (61.4%) | 40 (51.9%) | 0.296 |
| Royal Canin (Renal Support) | number (%) | 53 (39.6%) | 22 (38.6%) | 31 (40.3%) | 0.860 |
| Hill’s (k/d) | number (%) | 34 (25.4%) | 16 (28.1%) | 18 (23.4%) | 0.553 |
| Other | number (%) | 33 (24.6%) | 20 (35.1%) * | 13 (16.9%) | 0.025 |
| Phosphate binder | number (%) | 40 (29.9%) | 16 (28.1%) | 24 (31.2%) | 0.849 |
| Ferric chloride (Lenziaren) | |||||
| Oral activated charcoal | number (%) | 37 (27.6%) | 15 (26.3%) | 22 (28.6%) | 0.846 |
| ACEI/ARB (total) | number (%) | 34 (25.4%) | 15 (26.3%) | 19 (24.7%) | 0.843 |
| Benazepril (Fortekor) | number (%) | 27 (20.1%) | 10 (17.5%) | 17 (22.1%) | 0.664 |
| Telmisartan (Semintra) | number (%) | 10 (7.5%) | 5 (8.8%) | 5 (6.5%) | 0.743 |
| Calcium channel blocker | number (%) | 11 (8.2%) | 7 (12.3%) | 4 (5.2%) | 0.203 |
| Amlodipine | |||||
| Erythrocyte-stimulating agents | number (%) | 34 (25.4%) | 11 (19.3%) | 23 (29.9%) | 0.228 |
| Darbepoetin alfa | |||||
| Managing inappetence, nausea and vomiting (total) | number (%) | 102 (76.1%) | 41 (71.9%) | 61 (79.2%) | 0.413 |
| Maropitant (Cerenia) | number (%) | 88 (65.7%) | 34 (59.6%) | 54 (70.1%) | 0.270 |
| Mirtazapine | number (%) | 44 (32.8%) | 21 (36.8%) | 23 (29.9%) | 0.458 |
| Famotidine | number (%) | 27 (20.1%) | 16 (28.1%) | 11 (14.3%) | 0.054 |
| Omeprazole | number (%) | 8 (6.0%) | 2 (3.5%) | 6 (7.8%) | 0.466 |
| Metoclopramide | number (%) | 11 (8.2%) | 5 (8.8%) | 6 (7.8%) | 1.000 |
| Coexisting Disorders | |||||
| Any | number (%) | 38 (28.4%) | 18 (31.6%) | 20 (26.0%) | 0.562 |
| Hyperthyroidism | number (%) | 13 (9.7%) | 7 (12.3%) | 6 (7.8%) | 0.395 |
| Congestive heart failure | number (%) | 10 (7.5%) | 2 (3.5%) | 8 (10.4%) | 0.189 |
| Neoplasia † | number (%) | 8 (6.0%) | 4 (7.0%) | 4 (5.2%) | 0.723 |
| Diabetes mellitus | number (%) | 4 (3.0%) | 3 (5.3%) | 1 (1.3%) | 0.312 |
| Pancreatitis | number (%) | 3 (2.2%) | 2 (3.5%) | 1 (1.3%) | 0.575 |
| Progression-Free Survival | ||||||
| Covariate | Coefficient | Standard Error | Hazard Ratio for Disease Progression | 95% Confidence Interval | p Value | |
| Lower Limit | Upper Limit | |||||
| Beraprost | −0.52 | 0.24 | 0.59 | 0.37 | 0.96 | 0.032 * |
| Urea (mg/dL) ≥ 60.0 | 1.06 | 0.27 | 2.90 | 1.72 | 4.89 | <0.001 ** |
| Overall Survival | ||||||
| Covariate | Coefficient | Standard Error | Hazard Ratio for Death | 95% Confidence Interval | p Value | |
| Lower Limit | Upper Limit | |||||
| Beraprost | −0.54 | 0.27 | 0.58 | 0.34 | 0.99 | 0.047 * |
| Urea (mg/dL) ≥ 60.0 | 0.96 | 0.34 | 2.61 | 1.35 | 5.06 | 0.004 ** |
| Phosphate (mg/dL) ≥ 7.0 | 0.88 | 0.46 | 2.41 | 0.98 | 5.94 | 0.056 |
| Progression-Free Survival | |||||
| Beraprost Therapy versus No Beraprost Therapy | |||||
| Subgroups | Number of Cats | Hazard Ratio for Disease Progression | 95% Confidence Interval | p Value | |
| Lower Limit | Upper Limit | ||||
| All | 134 | 0.53 | 0.34 | 0.83 | 0.005 ** |
| Age (years) ≤ 15.0 | 61 | 0.39 | 0.18 | 0.83 | 0.015 * |
| Weight (kg) ≥ 3.0 | 99 | 0.53 | 0.31 | 0.90 | 0.018 * |
| Creatinine (mg/dL) < 4.0 | 109 | 0.53 | 0.32 | 0.88 | 0.015 * |
| Urea (mg/dL) < 120.0 | 129 | 0.57 | 0.36 | 0.89 | 0.014 * |
| Phosphate (mg/dL) < 6.0 | 97 | 0.51 | 0.30 | 0.88 | 0.015 * |
| Calcium (mg/dL) < 10.6 | 116 | 0.48 | 0.30 | 0.78 | 0.003 ** |
| Potassium (mmol/L) ≥ 3.5 | 104 | 0.59 | 0.35 | 0.98 | 0.042 * |
| Packed cell volume (%) ≥ 30.0 | 105 | 0.47 | 0.28 | 0.79 | 0.005 ** |
| Urine protein (mg/dL) ≤ 300 | 112 | 0.60 | 0.37 | 0.97 | 0.037 * |
| Overall Survival | |||||
| Beraprost Therapy versus No Beraprost Therapy | |||||
| Subgroups | Number of Cats | Hazard Ratio for Death | 95% Confidence Interval | p Value | |
| Lower Limit | Upper Limit | ||||
| All | 134 | 0.49 | 0.30 | 0.81 | 0.005 ** |
| Age (years) ≤ 15.0 | 61 | 0.25 | 0.10 | 0.67 | 0.006 ** |
| Weight (kg) ≥ 3.0 | 99 | 0.45 | 0.24 | 0.81 | 0.008 ** |
| Creatinine (mg/dL) < 4.0 | 109 | 0.45 | 0.25 | 0.80 | 0.007 ** |
| Urea (mg/dL) < 120.0 | 129 | 0.53 | 0.32 | 0.88 | 0.014 * |
| Phosphate (mg/dL) < 6.0 | 97 | 0.46 | 0.25 | 0.86 | 0.015 * |
| Calcium (mg/dL) < 10.6 | 116 | 0.44 | 0.26 | 0.76 | 0.003 ** |
| Potassium (mmol/L) ≥ 3.5 | 104 | 0.55 | 0.31 | 0.97 | 0.039 * |
| Packed cell volume (%) ≥ 30.0 | 105 | 0.42 | 0.23 | 0.75 | 0.004 ** |
| Urine protein (mg/dL) ≤ 300 | 112 | 0.54 | 0.32 | 0.92 | 0.023 * |
| Total (n = 97) | Beraprost Therapy (n = 47) | No Beraprost Therapy (n = 50) | p Value | ||
|---|---|---|---|---|---|
| Age (years) | median (25th, 75th percentile) | 15.6 (12.0, 17.1) | 15.9 (13.8, 17.1) | 15.1 (9.5, 17.3) | 0.302 |
| Weight (kg) | median (25th, 75th percentile) | 3.7 (3.0, 4.7) | 3.9 (3.4, 4.7) | 3.7 (2.9, 4.8) | 0.337 |
| Sex | |||||
| Female | number (%) | 53 (54.6%) | 27 (57.4%) | 26 (52.0%) | 0.684 |
| Male | number (%) | 44 (45.4%) | 20 (42.6%) | 24 (48.0%) | |
| Neutered | number (%) | 85 (87.6%) | 38 (80.9%) | 47 (94.0%) | 0.066 |
| Breeds | |||||
| Domestic Shorthair | number (%) | 66 (68.0%) | 33 (70.2%) | 33 (66.0%) | 0.670 |
| Japanese Bobtail | number (%) | 5 (5.2%) | 3 (6.4%) | 2 (4.0%) | |
| American Shorthair | number (%) | 6 (6.2%) | 3 (6.4%) | 3 (6.0%) | |
| Other | number (%) | 20 (20.6%) | 8 (17.0%) | 12 (24.0%) | |
| Biochemistry | |||||
| Creatinine (mg/dL) | median (25th, 75th percentile) | 3.2 (3.0, 3.5) | 3.2 (3.0, 3.6) | 3.2 (3.0, 3.4) | 0.335 |
| Urea (mg/dL) | median (25th, 75th percentile) | 38.0 (32.0, 48.0) | 36.0 (30.5, 44.0) | 40.5 (35.3, 48.8) * | 0.045 |
| Phosphate (mg/dL) | median (25th, 75th percentile) | 4.3 (3.8, 5.1) | 4.3 (3.8, 5.0) | 4.4 (3.9, 5.2) | 0.280 |
| Calcium (mg/dL) | median (25th, 75th percentile) | 9.7 (9.2, 10.1) | 9.8 (9.4, 10.4) * | 9.5 (9.0, 10.0) | 0.032 |
| Potassium (mmol/L) | median (25th, 75th percentile) | 3.9 (3.5, 4.2) | 4.0 (3.7, 4.2) | 3.9 (3.5, 4.2) | 0.119 |
| Hematology | |||||
| Packed cell volume (%) | median (25th, 75th percentile) | 36.5 (32.0, 40.0) | 37.0 (32.5, 41.0) | 35.0 (31.0, 40.0) | 0.146 |
| Urinalysis | |||||
| Urine specific gravity | median (25th, 75th percentile) | 1.014 (1.013, 1.017) | 1.014 (1.013, 1.017) | 1.014 (1.012, 1.018) | 0.837 |
| Urine protein (mg/dL) | mean (SD) | 36.7 (116.6) | 22.8 (51.5) | 52.7 (161.3) | 0.141 |
| Blood pressure measurement | |||||
| Systolic blood pressure (mmHg) | median (25th, 75th percentile) | 155.0 (139.0, 165.0) | 158.0 (140.0, 166.0) | 155.0 (137.5, 160.5) | 0.456 |
| Treatment | |||||
| Beraprost (RAPROS) | number (%) | 47 (48.5%) | 47 (100.0%) ** | 0 (0.0%) | <0.001 |
| Dose (μg/kg twice daily) | mean (SD, range) | 14.4 (3.6, 7.1–22.2) | 14.4 (3.6, 7.1–22.2) ** | 0 (0, 0–0) | <0.001 |
| Subcutaneous fluid therapy (total) | number (%) | 76 (78.4%) | 33 (70.2%) | 43 (86.0%) | 0.084 |
| At clinic | number (%) | 65 (67.0%) | 27 (57.4%) | 38 (76.0%) | 0.083 |
| At home | number (%) | 48 (49.5%) | 20 (42.6%) | 28 (56.0%) | 0.225 |
| Kidney Diet (total) | number (%) | 53 (54.6%) | 28 (59.6%) | 25 (50.0%) | 0.416 |
| Royal Canin (Renal Support) | number (%) | 37 (38.1%) | 17 (36.2%) | 20 (40.0%) | 0.835 |
| Hill’s (k/d) | number (%) | 24 (24.7%) | 13 (27.7%) | 11 (22.0%) | 0.639 |
| Other | number (%) | 28 (28.9%) | 19 (40.4%) * | 9 (18.0%) | 0.024 |
| Phosphate binder | number (%) | 24 (24.7%) | 9 (19.1%) | 13 (26.0%) | 0.474 |
| Ferric chloride (Lenziaren) | |||||
| Oral activated charcoal | number (%) | 26 (26.8%) | 13 (27.7%) | 13 (26.0%) | 1.000 |
| ACEI/ARB (total) | number (%) | 26 (26.8%) | 12 (25.5%) | 14 (28.0%) | 0.822 |
| Benazepril (Fortekor) | number (%) | 19 (19.6%) | 7 (14.9%) | 12 (24.0%) | 0.312 |
| Telmisartan (Semintra) | number (%) | 10 (10.3%) | 5 (10.6%) | 5 (10.0%) | 1.000 |
| Calcium channel blocker | number (%) | 9 (9.3%) | 7 (14.9%) | 2 (4.0%) | 0.085 |
| Amlodipine | |||||
| Erythrocyte-stimulating agents | number (%) | 21 (21.6%) | 8 (17.0%) | 13 (26.0%) | 0.330 |
| Darbepoetin alfa | |||||
| Managing inappetence, nausea and vomiting (total) | number (%) | 77 (79.4%) | 36 (76.6%) | 41 (82.0%) | 0.618 |
| Maropitant (Cerenia) | number (%) | 66 (68.0%) | 29 (61.7%) | 37 (74.0%) | 0.276 |
| Mirtazapine | number (%) | 31 (32.0%) | 18 (38.3%) | 13 (26.0%) | 0.276 |
| Famotidine | number (%) | 22 (22.7%) | 14 (29.8%) | 8 (16.0%) | 0.146 |
| Omeprazole | number (%) | 6 (6.2%) | 2 (4.3%) | 4 (8.0%) | 0.678 |
| Metoclopramide | number (%) | 10 (10.3%) | 4 (8.5%) | 6 (12.0%) | 0.742 |
| Coexisting Disorders | |||||
| Any | number (%) | 24 (24.7%) | 11 (23.4%) | 13 (26.0%) | 0.817 |
| Hyperthyroidism | number (%) | 10 (10.3%) | 6 (12.8%) | 4 (8.0%) | 0.516 |
| Congestive heart failure | number (%) | 4 (4.1%) | 0 (0.0%) | 4 (8.0%) | 0.118 |
| Neoplasia † | number (%) | 6 (6.2%) | 3 (6.4%) | 3 (6.0%) | 1.000 |
| Diabetes mellitus | number (%) | 2 (2.1%) | 1 (2.1%) | 1 (2.0%) | 1.000 |
| Pancreatitis | number (%) | 2 (2.1%) | 1 (2.1%) | 1 (2.0%) | 1.000 |
| Total (n = 134) | Beraprost Therapy (n = 57) | No Beraprost Therapy (n = 77) | ||
|---|---|---|---|---|
| Any | number (%) | 21 (15.7%) | 5 (8.8%) | 16 (20.8%) |
| Cardiovascular disorders (total) | number (%) | 10 (7.5%) | 2 (3.5%) | 8 (10.4%) |
| Congestive heart failure | number (%) | 4 (3.0%) | 0 (0.0%) | 4 (5.2%) |
| Cardiomyopathy | number (%) | 6 (4.5%) | 2 (3.5%) | 4 (5.2%) |
| Endocrine disorders (total) | number (%) | 2 (1.5%) | 0 (0.0%) | 2 (2.6%) |
| Hyperthyroidism | number (%) | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) |
| Diabetes mellitus | number (%) | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) |
| Neuromuscular disorders (total) | number (%) | 3 (2.2%) | 0 (0.0%) | 3 (3.9%) |
| Epilepsy & Seizures | number (%) | 3 (2.2%) | 0 (0.0%) | 3 (3.9%) |
| Neoplasia (total) | number (%) | 6 (4.5%) | 3 (5.3%) | 3 (3.9%) |
| Mast cell tumor | number (%) | 1 (0.7%) | 1 (1.8%) | 0 (0.0%) |
| Lymphoma | number (%) | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) |
| Squamous cell carcinoma | number (%) | 1 (0.7%) | 1 (1.8%) | 0 (0.0%) |
| Fibrosarcoma | number (%) | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) |
| Pulmonary adenocarcinoma | number (%) | 1 (0.7%) | 1 (1.8%) | 0 (0.0%) |
| Mesothelioma | number (%) | 1 (0.7%) | 0 (0.0%) | 1 (1.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, H.; Matsuura, T.; Sano, T. Beraprost and Overall Survival in Cats with Chronic Kidney Disease. Vet. Sci. 2023, 10, 459. https://doi.org/10.3390/vetsci10070459
Ito H, Matsuura T, Sano T. Beraprost and Overall Survival in Cats with Chronic Kidney Disease. Veterinary Sciences. 2023; 10(7):459. https://doi.org/10.3390/vetsci10070459
Chicago/Turabian StyleIto, Hiroyuki, Takumi Matsuura, and Tadashi Sano. 2023. "Beraprost and Overall Survival in Cats with Chronic Kidney Disease" Veterinary Sciences 10, no. 7: 459. https://doi.org/10.3390/vetsci10070459