
Review of Canine Lymphoma Treated with Chemotherapy—Outcomes and Prognostic Factors

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Treatment Response, Remission Duration, and Survival Definitions
3.2. Outcomes for Chemotherapy Treatment
3.3. Remission Times, Survival Times, and Response Rates for Multicentric/Nodal Lymphoma
3.4. Remission Times, Survival Times, and Response Rates for Other Forms of Lymphoma Treated with Chemotherapy
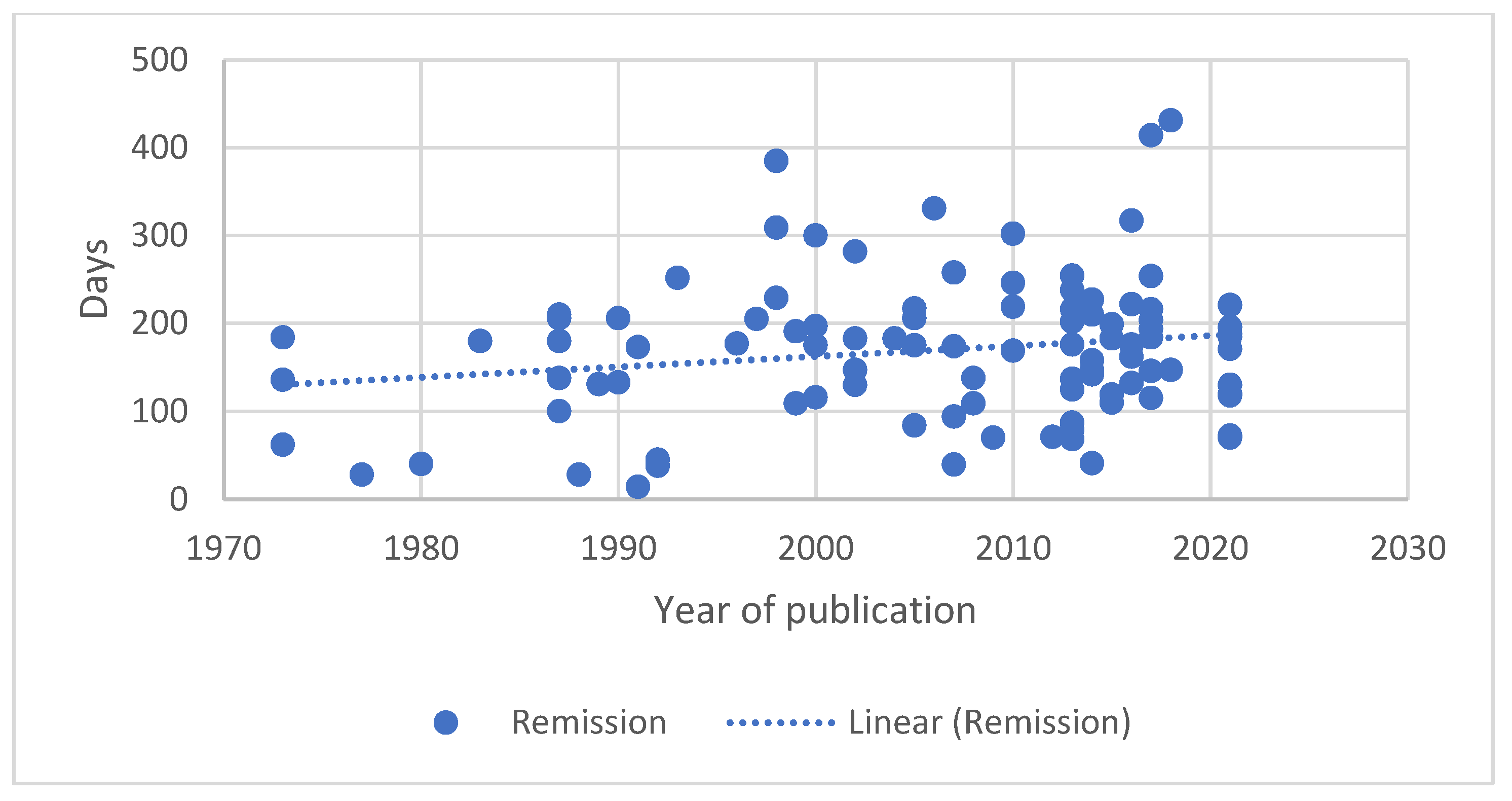
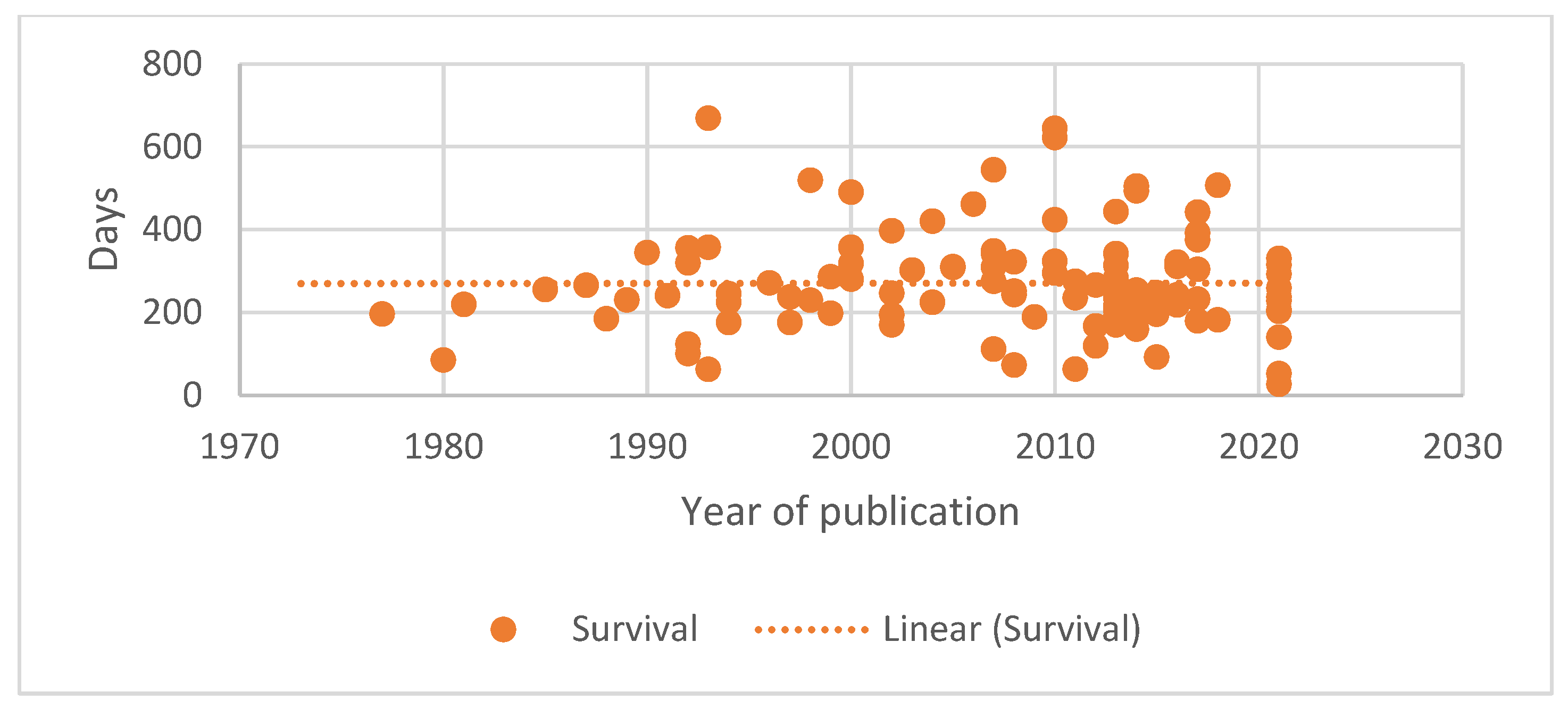
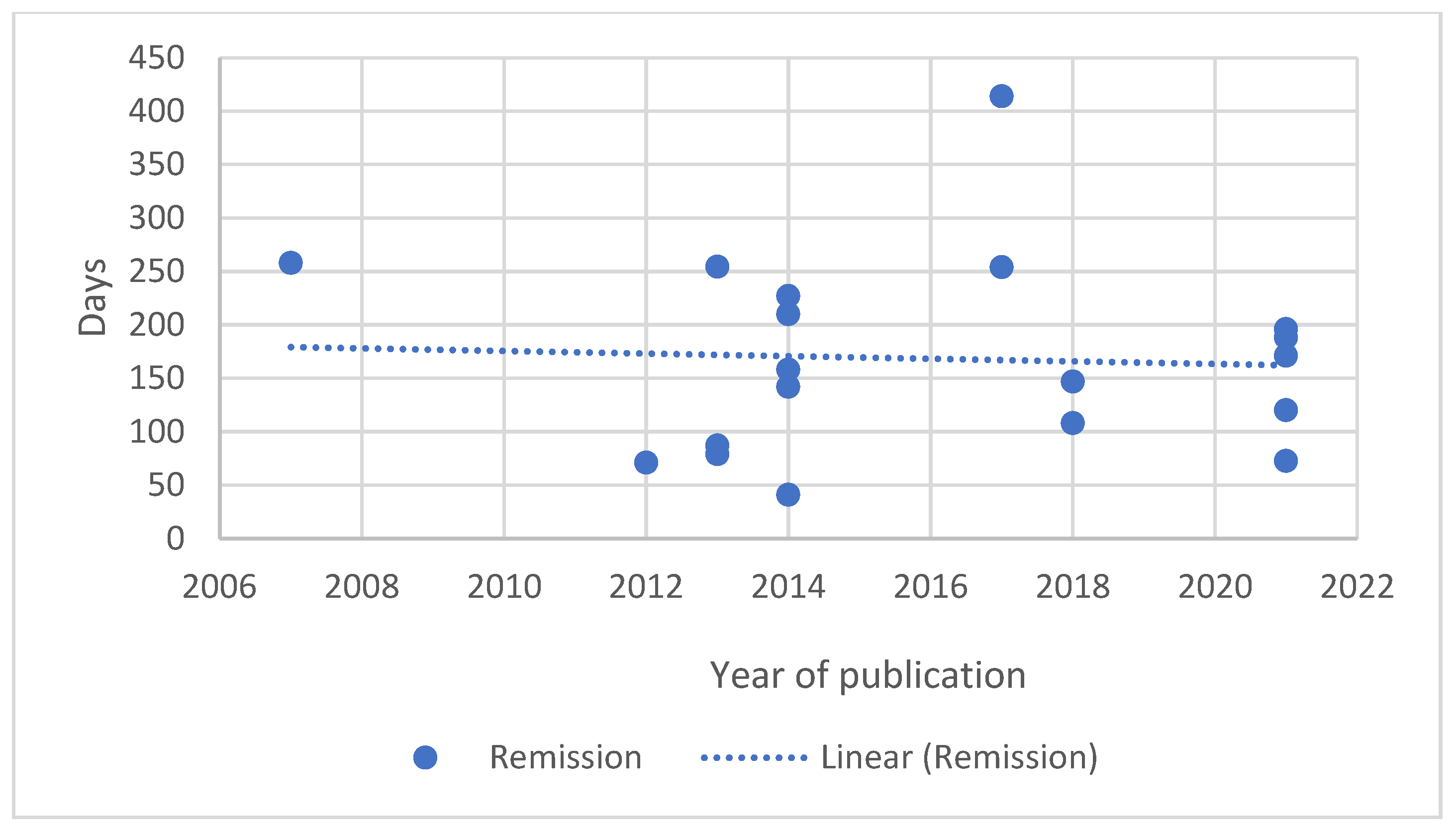
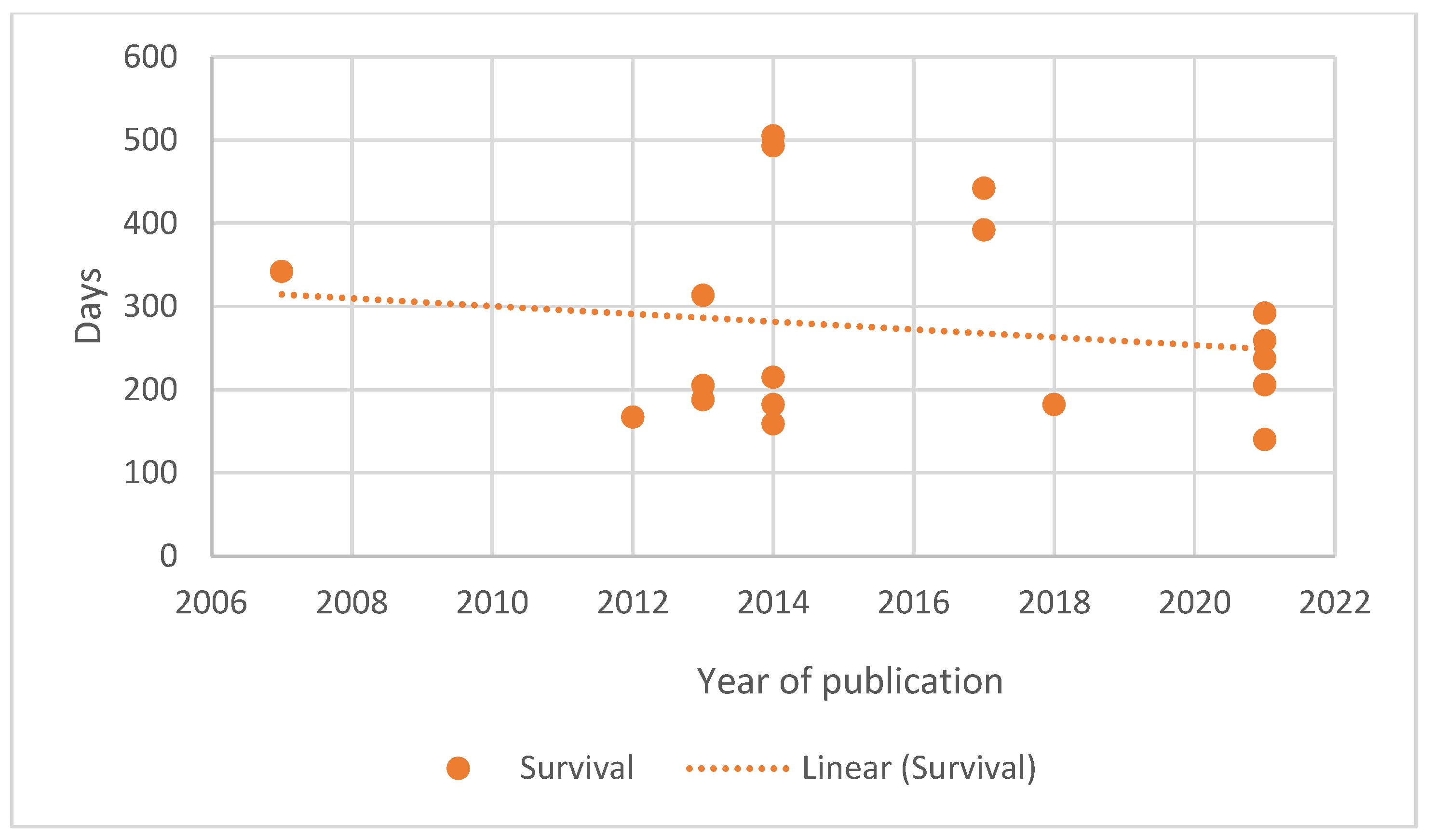
3.5. Changes in Remission and Survival Durations over Time
3.6. Prognostic Factors
3.6.1. Patient Characteristics
3.6.2. Lymphoma Characteristics
3.6.3. Laboratory Findings
3.6.4. Treatment Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Merlo, D.F.; Rossi, L.; Pellegrino, C.; Ceppi, M.; Cardellino, U.; Capurro, C.; Ratto, A.; Sambucco, P.L.; Sestito, V.; Tanara, G.; et al. Cancer Incidence in Pet Dogs: Findings of the Animal Tumor Registry of Genoa, Italy. J. Vet. Intern. Med. 2008, 22, 976–984. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, I.N.; Elgehiny, A.; Ragoonanan, D.; Mahadeo, K.M.; Nieto, Y.; Khazal, S. Management of Aggressive Non-Hodgkin Lymphomas in the Pediatric, Adolescent, and Young Adult Population: An Adult vs. Pediatric Perspective. Cancers 2022, 14, 2912. [Google Scholar] [CrossRef] [PubMed]
- Valli, V.E.; San Myint, M.; Barthel, A.; Bienzle, D.; Caswell, J.; Colbatzky, F.; Durham, A.; Ehrhart, E.J.; Johnson, Y.; Jones, C.; et al. Classification of Canine Malignant Lymphomas According to the World Health Organization Criteria. Vet. Pathol. 2011, 48, 198–211. [Google Scholar] [CrossRef] [PubMed]
- Valli, V.E.; Kass, P.H.; San Myint, M.; Scott, F. Canine Lymphomas: Association of Classification Type, Disease Stage, Tumor Subtype, Mitotic Rate, and Treatment with Survival. Vet. Pathol. 2013, 50, 738–748. [Google Scholar] [CrossRef]
- Hosoya, K.; Kisseberth, W.C.; Lord, L.K.; Alvarez, F.J.; Lara-Garcia, A.; Kosarek, C.E.; London, C.A.; Couto, C.G. Comparison of COAP and UW-19 Protocols for dogs with multicentric lymphoma. J. Vet. Intern. Med. 2007, 21, 1355–1363. [Google Scholar] [CrossRef]
- Marconato, L.; Polton, G.A.; Sabattini, S.; Dacasto, M.; Garden, O.A.; Grant, I.; Hendrickx, T.; Henriques, J.; Lubas, G.; Morello, E.; et al. Conformity and controversies in the diagnosis, staging and follow-up evaluation of canine nodal lymphoma: A systematic review of the last 15 years of published literature. Vet. Comp. Oncol. 2017, 15, 1029–1040. [Google Scholar] [CrossRef] [PubMed]
- Vail, D.M.; Michels, G.M.; Khanna, C.; Selting, K.A.; London, C.A.; Group, V.C.O. Response evaluation criteria for peripheral nodal lymphoma in dogs (v1.0)—A veterinary cooperative oncology group (VCOG) consensus document. Vet. Comp. Oncol. 2010, 8, 28–37. [Google Scholar] [CrossRef]
- Alabdaljabar, M.S.; Durani, U.; Thompson, C.A.; Constine, L.S.; Hashmi, S.K. The forgotten survivor: A comprehensive review on Non-Hodgkin lymphoma survivorship. Am. J. Hematol. 2022, 97, 1627–1637. [Google Scholar] [CrossRef]
- Crow, S.E.; Theilen, G.H.; Benjamini, E.; Torten, M.; Henness, A.M.; Buhles, W.C. Chemoimmunotherapy for canine lymphosarcoma. Cancer 1977, 40, 2102–2108. [Google Scholar] [CrossRef]
- Gavazza, A.; Lubas, G.; Fridman, A.; Peruzzi, D.; Impellizeri, J.A.; Luberto, L.; Marra, E.; Roscilli, G.; Ciliberto, G.; Aurisicchio, L. Safety and Efficacy of a Genetic Vaccine Targeting Telomerase Plus Chemotherapy for the Therapy of Canine B-Cell Lymphoma. Hum. Gene Ther. 2013, 24, 728–738. [Google Scholar] [CrossRef]
- Jeglum, K.A.; Young, K.M.; Barnsley, K.; Whereat, A. Chemotherapy versus chemotherapy with intralymphatic tumor-cell vaccine in canine lymphoma. Cancer 1988, 61, 2042–2050. [Google Scholar] [CrossRef] [PubMed]
- Marconato, L.; Frayssinet, P.; Rouquet, N.; Comazzi, S.; Leone, V.F.; Laganga, P.; Rossi, F.; Vignoli, M.; Pezzoli, L.; Aresu, L. Randomized, Placebo-Controlled, Double-Blinded Chemoimmunotherapy Clinical Trial in a Pet Dog Model of Diffuse Large B-cell Lymphoma. Clin. Cancer Res. 2014, 20, 668–677. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, C.M.; Sheppard, S.; Hartline, C.A.; Huls, H.; Johnson, M.; Palla, S.L.; Maiti, S.; Ma, W.; Davis, R.E.; Craig, S.; et al. Adoptive T-cell therapy improves treatment of canine non-Hodgkin lymphoma post chemotherapy. Sci. Rep. 2012, 2, 249. [Google Scholar] [CrossRef] [PubMed]
- Theilen, G.H.; Worley, M.; Benjamini, E. Chemoimmunotherapy for canine lymphosarcoma. J. Am. Vet. Med. Assoc. 1977, 170, 607–610. [Google Scholar] [PubMed]
- Turek, M.M.; Thamm, D.H.; Mitzey, A.; Kurzman, I.D.; Huelsmeyer, M.K.; Dubielzig, R.R.; Vail, D.M. Human granulocyte-macrophage colony-stimulating factor DNA cationic-lipid complexed autologous tumour cell vaccination in the treatment of canine B-cell multicentric lymphoma. Vet. Comp. Oncol. 2007, 5, 219–231. [Google Scholar] [CrossRef]
- Berlato, D.; Schrempp, D.; Van den Steen, N.; Murphy, S. Radiotherapy in the management of localized mucocutaneous oral lymphoma in dogs: 14 cases. Vet. Comp. Oncol. 2012, 10, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Epstein, R.B.; Graham, T.C.; Storb, R.; Thomas, E.D. Studies of marrow transplantation, chemotherapy and cross-circulation in canine lymphosarcoma. Blood 1971, 37, 349–359. [Google Scholar] [CrossRef]
- George, R.; Smith, A.; Schleis, S.; Brawner, W.; Almond, G.; Kent, M.; Wypij, J.; Borrego, J.; Moore, A.; Keyerleber, M.; et al. Outcome of dogs with intranasal lymphoma treated with various radiation and chemotherapy protocols: 24 cases. Vet. Radiol. Ultrasound 2016, 57, 306–312. [Google Scholar] [CrossRef]
- Gustafson, N.R.; Lana, S.E.; Mayer, M.N.; LaRue, S.M. A preliminary assessment of whole-body radiotherapy interposed within a chemotherapy protocol for canine lymphoma. Vet. Comp. Oncol. 2004, 2, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Lurie, D.M.; Gordon, I.K.; Theon, A.P.; Rodriguez, C.O.; Suter, S.E.; Kent, M.S. Sequential Low-Dose Rate Half-Body Irradiation and Chemotherapy for the Treatment of Canine Multicentric Lymphoma. J. Vet. Intern. Med. 2009, 23, 1064–1070. [Google Scholar] [CrossRef]
- Novotney, C.A.; Page, R.L.; Macy, D.W.; Dewhirst, M.W.; Ogilvie, G.K.; Withrow, S.J.; McEntee, M.C.; Heidner, G.L.; Allen, S.A.; Thrall, D.E.; et al. Phase I evaluation of doxorubicin and whole-body hyperthermia in dogs with lymphoma. J. Vet. Intern. Med. 1992, 6, 245–249. [Google Scholar] [CrossRef]
- Rassnick, K.M.; McEntee, M.C.; Erb, H.N.; Burke, B.P.; Balkman, C.E.; Flory, A.B.; Kiselow, M.A.; Autio, K.; Gieger, T.L. Comparison of 3 protocols for treatment after induction of remission in dogs with lymphoma. J. Vet. Intern. Med. 2007, 21, 1364–1373. [Google Scholar] [CrossRef]
- Vaughan, A.; Johnson, J.L.; Williams, L.E. Impact of chemotherapeutic dose intensity and hematologic toxicity on first remission duration in dogs with lymphoma treated with a chemoradiotherapy protocol. J. Vet. Intern. Med. 2007, 21, 1332–1339. [Google Scholar] [CrossRef] [PubMed]
- Willcox, J.L.; Pruitt, A.; Suter, S.E. Autologous Peripheral Blood Hematopoietic Cell Transplantation in Dogs with B-cell Lymphoma. J. Vet. Intern. Med. 2012, 26, 1155–1163. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.E.; Johnson, J.L.; Hauck, M.L.; Ruslander, D.M.; Price, G.S.; Thrall, D.E. Chemotherapy followed by half-body radiation therapy for canine lymphoma. J. Vet. Intern. Med. 2004, 18, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Frimberger, A.E.; Moore, A.S.; Rassnick, K.M.; Cotter, S.M.; O’Sullivan, J.L.; Quesenberry, P.J. A combination chemotherapy protocol with dose intensification and autologous bone marrow transplant (VELCAP-HDC) for canine lymphoma. J. Vet. Intern. Med. 2006, 20, 355–364. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, D.; Moore, P.F.; Vernau, W.; Peauroi, J.R.; Rebhun, R.B.; Rodriguez, C.O., Jr.; Skorupski, K.A. Clinical Characteristics and Outcome in Dogs with Splenic Marginal Zone Lymphoma. J. Vet. Intern. Med. 2013, 27, 949–954. [Google Scholar] [CrossRef] [PubMed]
- van Stee, L.L.; Boston, S.E.; Singh, A.; Romanelli, G.; Rubio-Guzman, A.; Scase, T.J. Outcome and Prognostic Factors for Canine Splenic Lymphoma Treated by Splenectomy (1995–2011). Vet. Surg. 2015, 44, 976–982. [Google Scholar] [CrossRef]
- Macewen, E.G.; Brown, N.O.; Patnaik, A.K.; Hayes, A.A.; Passe, S. Cyclic combination chemotherapy of canine lymphosarcoma. J. Am. Vet. Med. Assoc. 1981, 178, 1178–1181. [Google Scholar]
- Valerius, K.D.; Olgilvie, G.K.; Fettman, M.J.; Walton, J.A.; Richardson, K.; Powers, B.E.; McNiel, E.A.; Rogers, Q.R. Comparison of the effects of asparinginase administered subcutaneously versus intramuscularly for treatment of multicentric lymphoma in dogs receiving doxorubicin. J. Am. Vet. Med. Assoc. 1999, 214, 353–356. [Google Scholar]
- Kliczkowska-Klarowicz, K.; Jagielski, D.; Czopowicz, M.; Sapierzyński, R. Prognostic role of clinical presentation, cytological picture and response to treatment in canine centroblastic lymphoma. Pol. J. Vet. Sci. 2021, 24, 101–107. [Google Scholar] [PubMed]
- Stone, M.S.; Goldstein, M.A.; Cotter, S.M. Comparison of two protocols for induction of remission in dogs with lymphoma. J. Am. Anim. Hosp. Assoc. 1991, 27, 315–321. [Google Scholar]
- Dervisis, N.G.; Dominguez, P.A.; Sarbu, L.; Newman, R.G.; Cadile, C.D.; Swanson, C.N.; Kitchell, B.E. Efficacy of temozolomide or dacarbazine in combination with an anthracycline for rescue chemotherapy in dogs with lymphoma. J. Am. Vet. Med. Assoc. 2007, 231, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Azuma, K.; Ohmi, A.; Goto-Koshino, Y.; Tomiyasu, H.; Ohno, K.; Chambers, J.K.; Uchida, K.; Namba, H.; Nagata, M.; Nagamine, E.; et al. Outcomes and prognostic factors in canine epitheliotropic and nonepitheliotropic cutaneous T-cell lymphomas. Vet. Comp. Oncol. 2021, 20, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Simon, D.; Moreno, S.N.; Hirschberger, J.; Moritz, A.; Kohn, B.; Neumann, S.; Jurina, K.; Scharvogel, S.; Schwedes, C.; Reinacher, M.; et al. Efficacy of a continuous, multiagent chemotherapeutic protocol versus a short-term single-agent protocol in dogs with lymphoma. J. Am. Vet. Med. Assoc. 2008, 232, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Simon, D.; Nolte, I.; Eberle, N.; Abbrederis, N.; Killich, M.; Hirschberger, J. Treatment of dogs with lymphoma using a 12-week, maintenance-free combination chemotherapy protocol. J. Vet. Intern. Med. 2006, 20, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Smallwood, K.; Tanis, J.B.; Grant, I.A.; Blackwood, L.; Killick, D.R.; Amores-Fuster, I.; Elliott, J.; Mas, A.; Harper, A.; Marrington, M. Evaluation of a multi-agent chemotherapy protocol combining dexamethasone, melphalan, actinomycin D, and cytarabine for the treatment of resistant canine non-Hodgkin high-grade lymphomas: A single centre’s experience. Vet. Comp. Oncol. 2019, 17, 165–173. [Google Scholar] [CrossRef]
- Zemann, B.I.; Moore, A.S.; Rand, W.M.; Mason, G.; Ruslander, D.M.; Frimberger, A.E.; Wood, C.A.; L’Heureux, D.A.; Gliatto, J.; Cotter, S.M. A combination chemotherapy protocol (VELCAP-L) for dogs with lymphoma. J. Vet. Intern. Med. 1998, 12, 465–470. [Google Scholar] [CrossRef]
- Moore, A.S.; London, C.A.; Wood, C.A.; Williams, J.E.; Cotter, S.M.; L’Heureux, D.A.; Frimberger, A.E. Lomustine (CCNU) for the treatment of resistant lymphoma in dogs. J. Vet. Intern. Med. 1999, 13, 395–398. [Google Scholar] [CrossRef]
- Morrison-Collister, K.E.; Rassnick, K.M.; Northrup, N.C.; Kristal, O.; Chretin, J.D.; Williams, L.E.; Cotter, S.M.; Moore, A.S. A combination chemotherapy protocol with MOPP and CCNU consolidation (Tufts VELCAP-SC) for the treatment of canine lymphoma. Vet. Comp. Oncol. 2003, 1, 180–190. [Google Scholar] [CrossRef]
- Rassnick, K.M.; Moore, A.S.; Collister, K.E.; Northrup, N.C.; Kristal, O.; Chretin, J.D.; Bailey, D.B. Efficacy of Combination Chemotherapy for Treatment of Gastrointestinal Lymphoma in Dogs. J. Vet. Intern. Med. 2009, 23, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.E.; Rassnick, K.M.; Power, H.T.; Lana, S.E.; Morrison-Collister, K.E.; Hansen, K.; Johnson, J.L. CCNU in the treatment of canine epitheliotropic lymphoma. J. Vet. Intern. Med. 2006, 20, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Flory, A.B.; Rassnick, K.M.; Erb, H.N.; Garrett, L.D.; Northrup, N.C.; Selting, K.A.; Phillips, B.S.; Locke, J.E.; Chretin, J.D. Evaluation of factors associated with second remission in dogs with lymphoma undergoing retreatment with a cyclophosphamide, doxorubicin, vincristine, and prednisone chemotherapy protocol: 95 cases (2000–2007). J. Am. Vet. Med. Assoc. 2011, 238, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Griessmayr, P.C.; Payne, S.E.; Winter, J.E.; Barber, L.G.; Shofer, F.S. Dacarbazine as single-agent therapy for relapsed lymphoma in dogs. J. Vet. Intern. Med. 2009, 23, 1227–1231. [Google Scholar] [CrossRef]
- Northrup, N.C.; Gieger, T.L.; Kosarek, C.E.; Saba, C.F.; LeRoy, B.E.; Wall, T.M.; Hume, K.R.; Childress, M.O.; Keys, D.A. Mechlorethamine, procarbazine and prednisone for the treatment of resistant lymphoma in dogs. Vet. Comp. Oncol. 2009, 7, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Flory, A.B.; Rassnick, K.M.; Al-Sarraf, R.; Bailey, D.B.; Balkman, C.E.; Kiselow, M.A.; Autio, K. Combination of CCNU and DTIC chemotherapy for treatment of resistant lymphoma in dogs. J. Vet. Intern. Med. 2008, 22, 164–171. [Google Scholar] [CrossRef]
- Back, A.R.; Schleis, S.E.; Smrkovski, O.A.; Lee, J.; Smith, A.N.; Phillips, J.C. Mechlorethamine, vincristine, melphalan and prednisone (MOMP) for the treatment of relapsed lymphoma in dogs. Vet. Comp. Oncol. 2015, 13, 398–408. [Google Scholar] [CrossRef]
- Intile, J.L.; Rassnick, K.M.; Al-Sarraf, R.; Chretin, J.D. Evaluation of the Tolerability of Combination Chemotherapy with Mitoxantrone and Dacarbazine in Dogs with Lymphoma. J. Am. Anim. Hosp. Assoc. 2019, 55, 101–109. [Google Scholar] [CrossRef]
- Al-Nadaf, S.; Rebhun, R.B.; Curran, K.M.; Venable, R.O.; Skorupski, K.A.; Willcox, J.L.; Burton, J.H. Retrospective analysis of doxorubicin and prednisone as first-line therapy for canine B-cell lymphoma. BMC Vet. Res. 2018, 14, 356. [Google Scholar] [CrossRef]
- Tanis, J.B.; Mason, S.; Maddox, T.; Blackwood, L.; Killick, D.; Amores-Fuster, I.; Harper, A.; Finotello, R. Evaluation of a multi-agent chemotherapy protocol combining lomustine, procarbazine and prednisolone (LPP) for the treatment of relapsed canine non-Hodgkin high-grade lymphomas. Vet. Comp. Oncol. 2018, 16, 361–369. [Google Scholar] [CrossRef]
- Hughes, K.L.; Ehrhart, E.; Rout, E.D.; Harris, L.J.; Fernandez, M.; Yoshimoto, J.A.; Dossey, J.; Kuzmik, A.R.; Avery, P.R.; Avery, A.C. Diffuse Small B-Cell Lymphoma: A High-Grade Malignancy. Vet. Pathol. 2021, 58, 912–922. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.; Eberle, N.; Bullerdiek, J.; Nolte, I.; Simon, D. High-mobility group B1 proteins in canine lymphoma: Prognostic value of initial and sequential serum levels in treatment outcome following combination chemotherapy. Vet. Comp. Oncol. 2010, 8, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.S.; Ogilvie, G.K.; Vail, D.M. Actinomycin-D for reinduction of remission in dogs with resistant lymphoma. J. Vet. Intern. Med. 1994, 8, 343–344. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.; Kojima, M.; Ohno, K.; Chambers, J.K.; Uchida, K.; Ohmi, A.; Goto-Koshino, Y.; Tomiyasu, H.; Tsujimoto, H. Efficacy and adverse events of continuous l-asparaginase administration for canine large cell lymphoma of presumed gastrointestinal origin. Vet. Comp. Oncol. 2021, 20, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Marconato, L.; Martini, V.; Aresu, L.; Sampaolo, M.; Valentini, F.; Rinaldi, V.; Comazzi, S. Assessment of bone marrow infiltration diagnosed by flow cytometry in canine large B cell lymphoma: Prognostic significance and proposal of a cut-off value. Vet. J. 2013, 197, 776–781. [Google Scholar] [CrossRef]
- Škor, O.; Bicanová, L.; Wolfesberger, B.; Fuchs-Baumgartinger, A.; Ruetgen, B.; Štěrbová, M.; Schwendenwein, I.; Kleiter, M. Are B-symptoms more reliable prognostic indicators than substage in canine nodal diffuse large B-cell lymphoma. Vet. Comp. Oncol. 2021, 19, 201–208. [Google Scholar] [CrossRef]
- Aresu, L.; Martini, V.; Rossi, F.; Vignoli, M.; Sampaolo, M.; Arico, A.; Laganga, P.; Pierini, A.; Frayssinet, P.; Mantovani, R.; et al. Canine indolent and aggressive lymphoma: Clinical spectrum with histologic correlation. Vet. Comp. Oncol. 2015, 13, 348–362. [Google Scholar] [CrossRef]
- Mortier, F.; Daminet, S.; Vandenabeele, S.; Van de Maele, I. Canine lymphoma: A retrospective study (2009–2010). Vlaams Diergeneeskd. Tijdschr. 2012, 81, 341–351. [Google Scholar] [CrossRef]
- Squire, R.A.; Bush, R.M.; Melby, E.C.; Neeley, L.M.; Yarbrough, B. Clinical and pathologic study of canine lymphoma: Clinical staging, cell classification, and therapy. J. Natl. Cancer Inst. 1973, 51, 565–574. [Google Scholar]
- Lucas, S.R.R.; Coelho, B.M.P.; Marquezi, M.L.; Franchini, M.L.; Miyashiro, S.I.; Pozzi, D.H.D. Carmustine, vincristine, and prednisone in the treatment of canine lymphosarcoma. J. Am. Anim. Hosp. Assoc. 2004, 40, 292–299. [Google Scholar] [CrossRef]
- Price, G.S.; Page, R.L.; Fischer, B.M.; Levine, J.F.; Gerig, T.M. Efficicacy and toxicity of doxorubicin cyclophosphamide maintenance therapy in dogs with multicentric lymphosarcoma. J. Vet. Intern. Med. 1991, 5, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Chun, R.; Garrett, L.D.; Vail, D.M. Evaluation of a high-dose chemotherapy protocol with no maintenance therapy for dogs with lymphosarcoma. J. Vet. Intern. Med. 2000, 14, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Mutsaers, A.J.; Glickman, N.W.; DeNicola, D.B.; Widmer, W.R.; Bonney, P.L.; Hahn, K.A.; Knapp, D.W. Evaluation of treatment with doxorubicin and piroxicam or doxorubicin alone for multicentric lymphoma in dogs. J. Am. Vet. Med. Assoc. 2002, 220, 1813–1817. [Google Scholar] [CrossRef]
- Rassnick, K.M.; Bailey, D.B.; Malone, E.K.; Intile, J.L.; Kiselow, M.A.; Flory, A.B.; Barlow, L.L.; Balkman, C.E.; Barnard, S.M.; Waite, A.H. Comparison between L-CHOP and an L-CHOP protocol with interposed treatments of CCNU and MOPP (L-CHOP-CCNU-MOPP) for lymphoma in dogs. Vet. Comp. Oncol. 2010, 8, 243–253. [Google Scholar] [CrossRef]
- Chan, C.M.; Frimberger, A.E.; Moore, A.S. Clinical outcome and prognosis of dogs with histopathological features consistent with epitheliotropic lymphoma: A retrospective study of 148 cases (2003–2015). Vet. Dermatol. 2018, 29, e154–e159. [Google Scholar] [CrossRef] [PubMed]
- Holtermann, N.; Kiupel, M.; Kessler, M.; Teske, E.; Betz, D.; Hirschberger, J. Masitinib monotherapy in canine epitheliotropic lymphoma. Vet. Comp. Oncol. 2016, 14, 127–135. [Google Scholar] [CrossRef]
- Morges, M.A.; Burton, J.H.; Saba, C.F.; Vail, D.M.; Burgess, K.E.; Thamm, D.H. Phase II Evaluation of VDC-1101 in Canine Cutaneous T-Cell Lymphoma. J. Vet. Intern. Med. 2014, 28, 1569–1574. [Google Scholar] [CrossRef]
- Risbon, R.E.; de Lorimier, L.P.; Skorupski, K.; Burgess, K.E.; Bergman, P.J.; Carreras, J.; Hahn, K.; LeBlanc, A.; Turek, M.; Impellizeri, J.; et al. Response of canine cutaneous epitheliotropic lymphoma to lomustine (CCNU): A retrospective study of 46 cases (1999–2004). J. Vet. Intern. Med. 2006, 20, 1389–1397. [Google Scholar] [CrossRef]
- Desmas, I.; Burton, J.H.; Post, G.; Kristal, O.; Gauthier, M.; Borrego, J.F.; Di Bella, A.; Lara-Garcia, A. Clinical presentation, treatment and outcome in 31 dogs with presumed primary colorectal lymphoma (2001–2013). Vet. Comp. Oncol. 2017, 15, 504–517. [Google Scholar] [CrossRef]
- Sogame, N.; Risbon, R.; Burgess, K.E. Intestinal lymphoma in dogs: 84 cases (1997–2012). J. Am. Vet. Med. Assoc. 2018, 252, 440–447. [Google Scholar] [CrossRef]
- Aresu, L.; Agnoli, C.; Nicoletti, A.; Fanelli, A.; Martini, V.; Bertoni, F.; Marconato, L. Phenotypical Characterization and Clinical Outcome of Canine Burkitt-Like Lymphoma. Front. Vet. Sci. 2021, 8, 647009. [Google Scholar] [CrossRef] [PubMed]
- Aresu, L.; Marconato, L.; Martini, V.; Fanelli, A.; Licenziato, L.; Foiani, G.; Melchiotti, E.; Nicoletti, A.; Vascellari, M. Prognostic Value of PD-L1, PD-1 and CD8A in Canine Diffuse Large B-Cell Lymphoma Detected by RNAscope. Vet. Sci. 2021, 8, 120. [Google Scholar] [CrossRef]
- Avery, P.R.; Burton, J.; Bromberek, J.L.; Seelig, D.M.; Elmslie, R.; Correa, S.; Ehrhart, E.J.; Morley, P.S.; Avery, A.C. Flow Cytometric Characterization and Clinical Outcome of CD4+ T-Cell Lymphoma in Dogs: 67 Cases. J. Vet. Intern. Med. 2014, 28, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Barnard, R.A.; Wittenburg, L.A.; Amaravadi, R.K.; Gustafson, D.L.; Thorburn, A.; Thamm, D.H. Phase I clinical trial and pharmacodynamic evaluation of combination hydroxychloroquine and doxorubicin treatment in pet dogs treated for spontaneously occurring lymphoma. Autophagy 2014, 10, 1415–1425. [Google Scholar] [CrossRef] [PubMed]
- Baskin, C.R.; Couto, C.G.; Wittum, T.E. Factors influencing the first remission and survival in 145 dogs with lymphoma: A retrospective study. J. Am. Anim. Hosp. Assoc. 2000, 36, 404–409. [Google Scholar] [CrossRef]
- Benjamin, S.E.; Sorenmo, K.U.; Krick, E.L.; Salah, P.; Walsh, K.A.; Weinstein, N.M.; Keuler, N.S.; Avery, A.C.; Atherton, M.J.; Lenz, J.A. Response-based modification of CHOP chemotherapy for canine B-cell lymphoma. Vet. Comp. Oncol. 2021, 19, 541–550. [Google Scholar] [CrossRef]
- Bergman, P.J.; Ogilvie, G.K.; Powers, B.E. Monoclonal antibody C219 immunohistochemistry against P-glycoprotein: Sequential analysis and predictive ability in dogs with lymphoma. J. Vet. Intern. Med. 1996, 10, 354–359. [Google Scholar] [CrossRef]
- Bergmann, M.; Sauter-Louis, C.; Hirschberger, J. Chemotherapy in dogs with lymphoma-efficacy and adverse effects from the veterinarian’s and owner’s perspective. Kleintierpraxis 2011, 56, 573–584. [Google Scholar]
- Blaxill, J.; Buzzacott, P.; Finlay, J. Prognostic indicators for naïve canine non-indolent T-cell lymphoma treated with combination lomustine, vincristine, procarbazine and prednisolone chemotherapy. Vet. Comp. Oncol. 2021, 20, 215–226. [Google Scholar] [CrossRef]
- Bowles, C.A.; Lucas, D. Clinical and immunological response of lymphoma dogs following chemotherapy and irradiation. Comp. Immunol. Microbiol. Infect. Dis. 1980, 3, 317–326. [Google Scholar] [CrossRef]
- Boyce, K.L.; Kitchell, B.E. Treatment of canine lymphoma with COPLA/LVP. J. Am. Anim. Hosp. Assoc. 2000, 36, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Buffo de Capua, M.L.; Dela Coleta, F.E.; Massae Nakage Canesin, A.P.; Godoy, A.V.; Calazans, S.G.; Miotto, M.R.; Daleck, C.R.; Santana, A.E. Canine lymphoma: Clinical and hematological aspects and treatment with the Madison-Wisconsin protocol. Cienc. Rural 2011, 41, 1245–1251. [Google Scholar] [CrossRef]
- Burton, J.H.; Garrett-Mayer, E.; Thamm, D.H. Evaluation of a 15-week CHOP protocol for the treatment of canine multicentric lymphoma. Vet. Comp. Oncol. 2013, 11, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-W.; Small, G.W.; Motsinger-Reif, A.; Suter, S.E.; Richards, K.L. VH1-44 gene usage defines a subset of canine B-cell lymphomas associated with better patient survival. Vet. Immunol. Immunopathol. 2014, 157, 125–130. [Google Scholar] [CrossRef]
- Chikazawa, S.; Hori, Y.; Hoshi, F.; Kanai, K.; Ito, N. Hyperferritinemia is associated with short survival time in dogs with multicentric lymphoma. J. Vet. Med. Sci. 2015, 77, 843–846. [Google Scholar] [CrossRef] [PubMed]
- Cotter, S.M.; Goldstein, M.A. Comparison of 2 protocols for maintenance of remission in dogs with lymphoma. J. Am. Anim. Hosp. Assoc. 1987, 23, 495–499. [Google Scholar]
- Curran, K.; Thamm, D.H. Retrospective analysis for treatment of naive canine multicentric lymphoma with a 15-week, maintenance-free CHOP protocol. Vet. Comp. Oncol. 2016, 14, 147–155. [Google Scholar] [CrossRef]
- Curran, K.M.; Schaffer, P.A.; Frank, C.B.; Lana, S.E.; Hamil, L.E.; Burton, J.H.; Labadie, J.; Ehrhart, E.J.; Avery, P.R. BCL2 and MYC are expressed at high levels in canine diffuse large B-cell lymphoma but are not predictive for outcome in dogs treated with CHOP chemotherapy. Vet. Comp. Oncol. 2017, 15, 1269–1279. [Google Scholar] [CrossRef]
- Dank, G.; Rassnick, K.M.; Kristal, O.; Rodriguez, C.O., Jr.; Clifford, C.A.; Ward, R.; Mallett, C.L.; Gieger, T.; Segev, G. Clinical characteristics, treatment, and outcome of dogs with presumed primary hepatic lymphoma: 18 cases (1992–2008). J. Am. Vet. Med. Assoc. 2011, 239, 966–971. [Google Scholar] [CrossRef]
- Daters, A.T.; Mauldin, G.E.; Mauldin, G.N.; Brodsky, E.M.; Post, G.S. Evaluation of a multidrug chemotherapy protocol with mitoxantrone based maintenance (CHOP-MA) for the treatment of canine lymphoma. Vet. Comp. Oncol. 2010, 8, 11–22. [Google Scholar] [CrossRef]
- Deravi, N.; Berke, O.; Woods, J.P.; Bienzle, D. Specific immunotypes of canine T cell lymphoma are associated with different outcomes. Vet. Immunol. Immunopathol. 2017, 191, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Dhaliwal, R.S.; Kitchell, B.E.; Ehrhart, E.J.; Valli, V.E.; Dervisis, N.G. Clinicopathologic Significance of Histologic Grade, Pgp, and P53 Expression in Canine Lymphoma. J. Am. Anim. Hosp. Assoc. 2013, 49, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Dobson, J.M.; Gorman, N.T. Canine multicentric lymphoma-2—Comparison of response to 2 chemotherapeutic protocols. J. Small Anim. Pract. 1994, 35, 9–15. [Google Scholar] [CrossRef]
- Elliott, J.W.; Cripps, P.; Blackwood, L. Thymidine kinase assay in canine lymphoma. Vet. Comp. Oncol. 2013, 11, 1–13. [Google Scholar] [CrossRef]
- Elliott, J.W.; Cripps, P.; Marrington, A.M.; Grant, I.A.; Blackwood, L. Epirubicin as part of a multi-agent chemotherapy protocol for canine lymphoma. Vet. Comp. Oncol. 2013, 11, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Fontaine, S.J.; McCulloch, E.; Eckersall, P.D.; Haining, H.; Patterson Kane, J.C.; Morris, J.S. Evaluation of the modified Glasgow Prognostic Score to predict outcome in dogs with newly diagnosed lymphoma. Vet. Comp. Oncol. 2017, 15, 1513–1526. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara-Igarashi, A.; Goto-Koshino, Y.; Sato, M.; Maeda, S.; Igarashi, H.; Takahashi, M.; Fujino, Y.; Ohno, K.; Tsujimoto, H. Prognostic significance of the expression levels of the p16, p15, and p14 genes in dogs with high-grade lymphoma. Vet. J. 2014, 199, 236–244. [Google Scholar] [CrossRef]
- Garnica, T.K.; Lesbon, J.C.C.; Avila, A.C.F.C.M.; Rochetti, A.L.; Matiz, O.R.S.; Ribeiro, R.C.S.; Zoppa, A.; Nishiya, A.T.; Costa, M.T.; de Nardi, A.B.; et al. Liquid biopsy based on small extracellular vesicles predicts chemotherapy response of canine multicentric lymphomas. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Garrett, L.D.; Thamm, D.H.; Chun, R.; Dudley, R.; Vail, D.M. Evaluation of a 6-month chemotherapy protocol with no maintenance therapy for dogs with lymphoma. J. Vet. Intern. Med. 2002, 16, 704–709. [Google Scholar] [CrossRef]
- Goodman, I.H.; Moore, A.S.; Frimberger, A.E. Treatment of canine non-indolent T cell lymphoma using the VELCAP-TSC protocol: A retrospective evaluation of 70 dogs (2003–2013). Vet. J. 2016, 211, 39–44. [Google Scholar] [CrossRef]
- Greenlee, P.G.; Filippa, D.A.; Quimby, F.W.; Patnaik, A.K.; Calvano, S.E.; Matus, R.E.; Kimmel, M.; Hurvitz, A.I.; Lieberman, P.H. Lymphoma in dogs. A morphologic, immunologic and clinical study. Cancer 1990, 66, 480–490. [Google Scholar] [CrossRef] [PubMed]
- Henriques, J.; Felisberto, R.; Constantino-Casas, F.; Cabecadas, J.; Dobson, J. Peripheral blood cell ratios as prognostic factors in canine diffuse large B-cell lymphoma treated with CHOP protocol. Vet. Comp. Oncol. 2021, 19, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Higginbotham, M.L.; McCaw, D.L.; Roush, J.K.; Nietfeld, J.C.; Wilkerson, M.J.; Reeds, K.; Burr, D. Intermittent Single-Agent Doxorubicin for the Treatment of Canine B-Cell Lymphoma. J. Am. Anim. Hosp. Assoc. 2013, 49, 357–362. [Google Scholar] [CrossRef]
- Keller, E.T.; Macewen, E.G.; Rosenthal, R.C.; Helfand, S.C.; Fox, L.E. Evaluation of prognostic factors and sequential combination chemotherapy with doxorubicin for canine lymphoma. J. Vet. Intern. Med. 1993, 7, 289–295. [Google Scholar] [CrossRef]
- Kessler, M.; Kandel, B. Chemotherapy of malignant lymphoma in dogs. Results and experiences with the “Hofheim”-protocol in 57 cases. Kleintierpraxis 2004, 49, 349–358. [Google Scholar]
- Khanna, C.; Lund, E.M.; Redic, K.A.; Hayden, D.W.; Bell, F.W.; Goulland, E.L.; Klausner, J.S. Randomized controlled trial of doxorubicin versus dactinomycin in a multiagent protocol for treatment of dogs with malignant lymphoma. J. Am. Vet. Med. Assoc. 1998, 213, 985–990. [Google Scholar] [PubMed]
- Lee, J.-J.; Liao, A.T.; Wang, S.-L. L-Asparaginase, Doxorubicin, Vincristine, and Prednisolone (LHOP) Chemotherapy as a First-Line Treatment for Dogs with Multicentric Lymphoma. Animals 2021, 11, 2199. [Google Scholar] [CrossRef]
- Lori, J.C.; Stein, T.J.; Thamm, D.H. Doxorubicin and cyclophosphamide for the treatment of canine lymphoma: A randomized, placebo-controlled study. Vet. Comp. Oncol. 2010, 8, 188–195. [Google Scholar] [CrossRef]
- Lucas, S.R.R.; Maranhao, R.C.; Guerra, J.L.; Coelho, B.M.P.; Barboza, R.; Pozzi, D.H.B. Pilot clinical study of carmustine associated with a lipid nanoemulsion in combination with vincristine and prednisone for the treatment of canine lymphoma. Vet. Comp. Oncol. 2015, 13, 184–193. [Google Scholar] [CrossRef]
- MacDonald, V.S.; Thamm, D.H.; Kurzman, I.D.; Turek, M.M.; Vail, D.M. Does L-asparaginase influence efficacy or toxicity when added to a standard CHOP protocol for dogs with lymphoma? J. Vet. Intern. Med. 2005, 19, 732–736. [Google Scholar] [CrossRef]
- Macewen, E.G.; Hayes, A.A.; Mooney, S.; Patnaik, A.; Kurzman, I.; Hardy, W.D. Levamisole as adjuvant to chemotherapy for canine lymphosarcoma. J. Biol. Response Modif. 1985, 4, 427–433. [Google Scholar]
- Macewen, E.G.; Rosenthal, R.C.; Fox, L.E.; Loar, A.S.; Kurzman, I.D. Evaluation of L-asparaginase:Polyethylene glycol conjugate versus native L-asparaginase combined with chemotherapy. A randomized double-blind study in canine lymphoma. J. Vet. Intern. Med. 1992, 6, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Marconato, L.; Bonfanti, U.; Stefanello, D.; Lorenzo, M.R.; Romanelli, G.; Comazzi, S.; Zini, E. Cytosine arabinoside in addition to VCAA-based protocols for the treatment of canine lymphoma with bone marrow involvement: Does it make the difference? Vet. Comp. Oncol. 2008, 6, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Merlo, A.; Gagliano Rezende, B.C.; Franchini, M.L.; Nunes Simoes, D.M.; Ricci Lucas, S.R. Serum C-reactive protein concentrations in dogs with multicentric lymphoma undergoing chemotherapy. J. Am. Vet. Med. Assoc. 2007, 230, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.S.; Ogilvie, G.K.; Ruslander, D.; Rand, W.S.; Cotter, S.M.; Getzy, D.M.; Lheureux, D.A.; Dennis, R.A. Evaluation of mitoxantrone for the treatment of lymphoma in dogs. J. Am. Vet. Med. Assoc. 1994, 204, 1903–1905. [Google Scholar] [PubMed]
- Morgan, E.; O’Connell, K.; Thomson, M.; Griffin, A. Canine T cell lymphoma treated with lomustine, vincristine, procarbazine, and prednisolone chemotherapy in 35 dogs. Vet. Comp. Oncol. 2018, 16, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.S.; Dunn, J.K.; Dobson, J.M. Canine lymphoid leukaemia and lymphoma with bone marrow involvement: A review of 24 cases. J. Small Anim. Pract. 1993, 34, 72–79. [Google Scholar] [CrossRef]
- Mutz, M.; Boudreaux, B.; Kearney, M.; Stroda, K.; Gaunt, S.; Shiomitsu, K. Prognostic value of baseline absolute lymphocyte concentration and neutrophil/lymphocyte ratio in dogs with newly diagnosed multi-centric lymphoma. Vet. Comp. Oncol. 2015, 13, 337–347. [Google Scholar] [CrossRef]
- Myers, N.C.; Moore, A.S.; Rand, W.M.; Gliatto, J.; Cotter, S.M. Evaluation of a multidrug chemotherapy protocol (ACOPA III) in dogs with lymphoma. J. Vet. Intern. Med. 1997, 11, 333–339. [Google Scholar]
- Nerschbach, V.; Eberle, N.; Joetzke, A.E.; Hoeinghaus, R.; Hungerbuehler, S.; Mischke, R.; Nolte, I.; Betz, D. Splenic and hepatic ultrasound and cytology in canine lymphoma: Effects of findings on stage migration and assessment of prognosis. Vet. Comp. Oncol. 2016, 14, 82–93. [Google Scholar] [CrossRef]
- Ogilvie, G.K.; Atwater, S.W.; Ciekot, P.A.; Bergman, P.J.; Henkel, S.; Walters, L.M. Prevalence of anaphylaxis associated with the intramuscular administration of L-asparaginase to 81 dogs with cancer: 1989–1991. J. Am. Anim. Hosp. Assoc. 1994, 30, 62–65. [Google Scholar]
- Olgilvie, G.K.; Vail, D.M.; Klain, M.K.; Powers, B.E.; Dickinson, K. Weekly adminstration of low-dose doxorubicin for treatment of malignant lymphoma in dogs. J. Am. Vet. Med. Assoc. 1991, 198, 1762–1764. [Google Scholar]
- Ossowska, M.; Teske, E.; Beirens-van Kuijk, L.; Zandvliet, M.; de Vos, J.P. Treatment of multicentric or cranial mediastinal high-grade T-cell lymphoma in dogs with a first-line CCNU-L(-chlorambucil)-CHOP protocol. Vlaams Diergeneeskd. Tijdschr. 2016, 85, 275–284. [Google Scholar] [CrossRef]
- Poggi, A.; Miniscalco, B.; Morello, E.; Gattino, F.; Delaude, A.; Poschetto, L.F.; Aresu, L.; Gelain, M.E.; Martini, V.; Comazzi, S.; et al. Prognostic significance of Ki67 evaluated by flow cytometry in dogs with high-grade B-cell lymphoma. Vet. Comp. Oncol. 2017, 15, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Postorino, N.C.; Susaneck, S.J.; Withrow, S.J.; Macy, D.W.; Harris, C. Single agent therapy with adriamycin for canine lymphosarcoma. J. Am. Anim. Hosp. Assoc. 1989, 25, 221–225. [Google Scholar]
- Rebhun, R.B.; Kent, M.S.; Borrofka, S.A.E.B.; Frazier, S.; Skorupski, K.; Rodriguez, C.O. CHOP chemotherapy for the treatment of canine multicentric T-cell lymphoma. Vet. Comp. Oncol. 2011, 9, 38–44. [Google Scholar] [CrossRef]
- Sauerbrey, M.L.; Mullins, M.N.; Bannink, E.O.; Van Dorp, T.E.R.; Kaneene, J.B.; Obradovich, J.E. Lomustine and prednisone as a first-line treatment for dogs with multicentric lymphoma: 17 cases (2004–2005). J. Am. Vet. Med. Assoc. 2007, 230, 1866–1869. [Google Scholar] [CrossRef]
- Siedlecki, C.T.; Kass, P.H.; Jakubiak, M.J.; Dank, G.; Lyons, J.; Kent, M.S. Evaluation of an actinomycin-D-containing combination chemotherapy protocol with extended maintenance therapy for canine lymphoma. Can. Vet. J. -Rev. Vet. Can. 2006, 47, 52–59. [Google Scholar]
- Teske, E.; Rutteman, G.R.; Vanheerde, P.; Misdorp, W. Polyethylene glycol-L-asparaginase versus native L-asparaginase in canine non-Hodgkins-lymphoma. Eur. J. Cancer 1990, 26, 891–895. [Google Scholar] [CrossRef]
- Thamm, D.H.; Vail, D.M.; Post, G.S.; Fan, T.M.; Phillips, B.S.; Axiak-Bechtel, S.; Elmslie, R.S.; Klein, M.K.; Ruslander, D.A. Alternating Rabacfosadine/Doxorubicin: Efficacy and Tolerability in Naive Canine Multicentric Lymphoma. J. Vet. Intern. Med. 2017, 31, 872–878. [Google Scholar] [CrossRef]
- Todd, J.; Thomas, P.; Nguyen, S. Cyclophosphamide and prednisolone for chemotherapy naive B cell multicentric lymphoma in dogs: 32 cases (2017–2021). J. Small Anim. Pract. 2021, 63, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Valerius, K.D.; Ogilvie, G.K.; Mallinckrodt, C.H.; Getzy, D.M. Doxorubicin alone or in combination with asparaginase, followed by cyclophosphamide, vincristine, and prednisone for treatment of multicentric lymphoma in dogs: 121 cases (1987–1995). J. Am. Vet. Med. Assoc. 1997, 210, 512–516. [Google Scholar] [PubMed]
- Veluvolu, S.; Pellin, M.; Vos, N. Evaluation of neutrophilia as a prognostic factor in dogs with multicentric lymphoma treated with a cyclophosphamide, doxorubicin, vincristine, and prednisone based chemotherapy protocol. J. Am. Vet. Med. Assoc. 2021, 259, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.L.; Lee, J.J.; Liao, A.T. Comparison of efficacy and toxicity of doxorubicin and mitoxantrone in combination chemotherapy for canine lymphoma. Can. Vet. J.-Rev. Vet. Can. 2016, 57, 271–276. [Google Scholar]
- Zandvliet, M.; Rutteman, G.R.; Teske, E. Prednisolone inclusion in a first-line multidrug cytostatic protocol for the treatment of canine lymphoma does not affect therapy results. Vet. J. 2013, 197, 656–661. [Google Scholar] [CrossRef]
- Zenker, I.; Meichner, K.; Steinle, K.; Kessler, M.; Hirschberger, J. Thirteen-week dose-intensifying simultaneous combination chemotherapy protocol for malignant lymphoma in dogs. Vet. Rec. 2010, 167, 744–748. [Google Scholar] [CrossRef]
- Alvarez, F.J.; Kisseberth, W.C.; Gallant, S.L.; Couto, C.G. Dexamethasone, melphalan, actinomycin D, cytosine arabinoside (DMAC) protocol for dogs with relapsed lymphoma. J. Vet. Intern. Med. 2006, 20, 1178–1183. [Google Scholar] [CrossRef]
- Bannink, E.O.; Sauerbrey, M.L.; Mullins, M.N.; Hauptman, J.G.; Obradovich, J.E. Actinomycin D as rescue therapy in dogs with relapsed or resistant lymphoma: 49 cases (1999–2006). J. Am. Vet. Med. Assoc. 2008, 233, 446–451. [Google Scholar] [CrossRef]
- Calvert, C.A.; Leifer, C.E. Doxorubicin for treatment of canine lymphosarcoma after development of resistance to combination chemotherapy. J. Am. Vet. Med. Assoc. 1981, 179, 1011–1012. [Google Scholar]
- Fahey, C.E.; Milner, R.J.; Barabas, K.; Lurie, D.; Kow, K.; Parfitt, S.; Lyles, S.; Clemente, M. Evaluation of the University of Florida lomustine, vincristine, procarbazine, and prednisone chemotherapy protocol for the treatment of relapsed lymphoma in dogs: 33 cases (2003–2009). J. Am. Vet. Med. Assoc. 2011, 239, 209–215. [Google Scholar] [CrossRef]
- Gillem, J.; Giuffrida, M.; Krick, E. Efficacy and toxicity of carboplatin and cytarabine chemotherapy for dogs with relapsed or refractory lymphoma (2000–2013). Vet. Comp. Oncol. 2017, 15, 400–410. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, A.K.; Mauldin, G.E.; Milner, R.J.; LaDue, T.A.; Mauldin, G.N.; Bartges, J.W. Efficacy and toxicity of BOPP and LOPP chemotherapy for the treatment of relapsed canine lymphoma. Vet. Comp. Oncol. 2006, 4, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Lenz, J.A.; Robat, C.S.; Stein, T.J. Vinblastine as a second rescue for the treatment of canine multicentric lymphoma in 39 cases (2005 to 2014). J. Small Anim. Pract. 2016, 57, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Lucroy, M.D.; Phillips, B.S.; Kraegel, S.A.; Simonson, E.R.; Madewell, B.R. Evaluation of single-agent mitoxantrone as chemotherapy for relapsing canine lymphoma. J. Vet. Intern. Med. 1998, 12, 325–329. [Google Scholar] [CrossRef]
- Mastromauro, M.; Suter, S.; Hauck, M.; Hess, P. Oral melphalan for the treatment of relapsed canine lymphoma. Vet. Comp. Oncol. 2018, 16, E123–E129. [Google Scholar] [CrossRef]
- Parsons-Doherty, M.; Poirier, V.J.; Monteith, G. The efficacy and adverse event profile of dexamethasone, melphalan, actinomycin D, and cytosine arabinoside (DMAC) chemotherapy in relapsed canine lymphoma. Can. Vet. J.-Rev. Vet. Can. 2014, 55, 175–180. [Google Scholar]
- Saba, C.; Vickery, K.; Clifford, C.; Burgess, K.; Phillips, B.; Vail, D.; Wright, Z.; Morges, M.; Fan, T.; Thamm, D. Rabacfosadine for relapsed canine B-cell lymphoma: Efficacy and adverse event profiles of 2 different doses. Vet. Comp. Oncol. 2018, 16, E76–E82. [Google Scholar] [CrossRef]
- Saba, C.F.; Hafeman, S.D.; Vail, D.M.; Thamm, D.H. Combination Chemotherapy with Continuous l-Asparaginase, Lomustine, and Prednisone for Relapsed Canine Lymphoma. J. Vet. Intern. Med. 2009, 23, 1058–1063. [Google Scholar] [CrossRef]
- Smith, A.A.; Lejeune, A.; Kow, K.; Milner, R.J.; Souza, C.H.M. Clinical Response and Adverse Event Profile of Bleomycin Chemotherapy for Canine Multicentric Lymphoma. J. Am. Anim. Hosp. Assoc. 2017, 53, 128–134. [Google Scholar] [CrossRef]
- van Vechten, M.; Helfand, S.C.; Jeglum, K.A. Treatment of relapsed canine lymphoma with doxorubicin and dacarbazine. J. Vet. Intern. Med. 1990, 4, 187–191. [Google Scholar] [CrossRef]
- Alexandrakis, I.; Tuli, R.; Ractliffe, S.C.; Tappin, S.W.; Foale, R.D.; Roos, A.; Slater, K.J. Utility of a multiple serum biomarker test to monitor remission status and relapse in dogs with lymphoma undergoing treatment with chemotherapy. Vet. Comp. Oncol. 2017, 15, 6–17. [Google Scholar] [CrossRef] [PubMed]
- Boye, P.; Serres, F.; Marescaux, L.; Hordeaux, J.; Bouchaert, E.; Gomes, B.; Tierny, D. Dose escalation study to evaluate safety, tolerability and efficacy of intravenous etoposide phosphate administration in 27 dogs with multicentric lymphoma. PLoS ONE 2017, 12, e0177486. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, E.M.; Maudlin, G.N.; Lachowicz, J.L.; Post, G.S. Asparaginase and MOPP Treatment of Dogs with Lymphoma. J. Vet. Intern. Med. 2009, 23, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Childress, M.O.; Fulkerson, C.M.; Lahrman, S.A.; Weng, H.Y. Inter- and intra-rater reliability of calliper-based lymph node measurement in dogs with peripheral nodal lymphomas. Vet. Comp. Oncol. 2016, 14, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Hohenhaus, A.E.; Matus, R.E. Etoposide (VP-16). Retrospective analysis of treatment in 13 dogs with lymphoma. J. Vet. Intern. Med. 1990, 4, 239–241. [Google Scholar] [CrossRef]
- Ogilvie, G.K.; Richardson, R.C.; Curtis, C.R.; Withrow, S.J.; Reynolds, H.A.; Norris, A.M.; Henderson, R.A.; Klausner, J.S.; Fowler, J.D.; McCaw, D. Acute and short-term toxicoses associated with the administration of doxorubicin to dogs with malignant tumors. J. Am. Vet. Med. Assoc. 1989, 195, 1584–1587. [Google Scholar] [PubMed]
- Carter, R.F.; Harris, C.K.; Withrow, S.J.; Valli, V.E.O.; Susaneck, S.J. Chemotherapy of canine lymphoma wiht histopathological correlation-doxorubicin alone compared to COP as 1st treatment regimen. J. Am. Anim. Hosp. Assoc. 1987, 23, 587–598. [Google Scholar]
- Cotter, S.M. Treatment of lymphoma and leukemia with cyclophosphamide, vincristine, and prednisone. 1. Treatment of dogs. J. Am. Anim. Hosp. Assoc. 1983, 19, 159–165. [Google Scholar]
- Frankhouse, K.A.; Rout, E.D.; Hughes, K.L.; Labadie, J.D.; Yoshimoto, J.A.; Lana, S.E.; Avery, P.R.; Avery, A.C. An Aggressive CD4−CD8− T-cell Neoplasm in Young English Bulldogs. Vet. Comp. Oncol. 2021, 20, 416–426. [Google Scholar] [CrossRef]
- Gavazza, A.; Sacchini, F.; Lubas, G.; Gugliucci, B.; Valori, E. Clinical, laboratory, diagnostic and prognostic aspects of canine lymphoma: A retrospective study. Comp. Clin. Pathol. 2009, 18, 291–299. [Google Scholar] [CrossRef]
- Gentilini, F.; Turba, M.E.; Forni, M. Retrospective monitoring of minimal residual disease using hairpin-shaped clone specific primers in B-cell lymphoma affected dogs. Vet. Immunol. Immunopathol. 2013, 153, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Gray, K.N.; Raulston, G.L.; Gleiser, C.A.; Jardine, J.H. Histologic classificatoin as an indication of therapeutic response in malignant-lymphoma of dogs. J. Am. Vet. Med. Assoc. 1984, 184, 814–817. [Google Scholar] [PubMed]
- Hahn, K.A.; Richardson, R.C.; Teclaw, R.F.; Cline, J.M.; Carlton, W.W.; Denicola, D.B.; Bonney, P.L. Is maintenance chemotherapy appropriate for the management of canine malignant-lymphoma? J. Vet. Intern. Med. 1992, 6, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Jagielski, D.; Lechowski, R.; Hoffmann-Jagielska, M.; Winiarczyk, S. A Retrospective Study of the Incidence and Prognostic Factors of Multicentric Lymphoma in Dogs (1998–2000). J. Vet. Med. Ser. A 2002, 49, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Jeffreys, A.B.; Knapp, D.W.; Carlton, W.W.; Thomas, R.M.; Bonney, P.L.; Lucroy, M.D. Influence of asparaginase on a combination chemotherapy protocol for canine multicentric lymphoma. J. Am. Anim. Hosp. Assoc. 2005, 41, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Lautscham, E.M.; Kessler, M.; Ernst, T.; Willimzig, L.; Neiger, R. Comparison of a CHOP-LAsp-based protocol with and without maintenance for canine multicentric lymphoma. Vet. Rec. 2017, 180, 303. [Google Scholar] [CrossRef]
- Macewen, E.G.; Hayes, A.A.; Matus, R.E.; Kurzman, I. Evaluation of some prognostic factors for advanced multicentric lymphosarcoma in the dog—147 cases (1978–1981). J. Am. Vet. Med. Assoc. 1987, 190, 564–568. [Google Scholar]
- Maddison, J.E.; Peaston, A.; Church, D.B. Treatment of 42 cases of canine lymphosarcoma with combination chemotherapy—1987–1993. Aust. Vet. Pract. 1994, 24, 94–101. [Google Scholar]
- Romano, F.R.; Heinze, C.R.; Barber, L.G.; Mason, J.B.; Freeman, L.M. Association between Body Condition Score and Cancer Prognosis in Dogs with Lymphoma and Osteosarcoma. J. Vet. Intern. Med. 2016, 30, 1179–1186. [Google Scholar] [CrossRef]
- Rout, E.D.; Labadie, J.D.; Yoshimoto, J.A.; Avery, P.R.; Curran, K.M.; Avery, A.C. Clinical outcome and prognostic factors in dogs with B-cell chronic lymphocytic leukemia: A retrospective study. J. Vet. Intern. Med. 2021, 35, 1918–1928. [Google Scholar] [CrossRef]
- Sorenmo, K.; Overley, B.; Krick, E.; Ferrara, T.; LaBlanc, A.; Shofer, F. Outcome and toxicity associated with a dose-intensified, maintenance-free CHOP-based chemotherapy protocol in canine lymphoma: 130 cases. Vet. Comp. Oncol. 2010, 8, 196–208. [Google Scholar] [CrossRef] [PubMed]
- Wilson-Robles, H.; Budke, C.M.; Miller, T.; Dervisis, N.; Novosad, A.; Wright, Z.; Thamm, D.H.; Vickery, K.; Burgess, K.; Childress, M.; et al. Geographical differences in survival of dogs with non-Hodgkin lymphoma treated with a CHOP based chemotherapy protocol. Vet. Comp. Oncol. 2017, 15, 1564–1571. [Google Scholar] [CrossRef] [PubMed]
- Wolfesberger, B.; Tonar, Z.; Fuchs-Baumgartinger, A.; Walter, I.; Skalicky, M.; Witter, K.; Thalhammer, J.G.; Pagitz, M.; Kleiter, M. Angiogenic markers in canine lymphoma tissues do not predict survival times in chemotherapy treated dogs. Res. Vet. Sci. 2012, 92, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Childress, M.O.; Ramos-Vara, J.A.; Ruple, A. A randomized controlled trial of the effect of prednisone omission from a multidrug chemotherapy protocol on treatment outcome in dogs with peripheral nodal lymphomas. J. Am. Vet. Med. Assoc. 2016, 249, 1067–1078. [Google Scholar] [CrossRef] [PubMed]
- Zandvliet, M.; Teske, E.; Chapuis, T.; Fink-Gremmels, J.; Schrickx, J.A. Masitinib reverses doxorubicin resistance in canine lymphoid cells by inhibiting the function of P-glycoprotein. J. Vet. Pharmacol. Ther. 2013, 36, 583–587. [Google Scholar] [CrossRef]
- Avery, P.R.; Burton, J.; Bromberek, J.L.; Seelig, D.M.; Elmslie, R.; Correa, S.; Ehrhart, E.J.; Morley, P.S.; Avery, A.C. Flow Cytometric Characterization and Clinical Outcome of CD4 T Cell Lymphoma in Dogs. J. Vet. Intern. Med. 2014, 28, 538–546. [Google Scholar] [CrossRef]
- Ogilvie, G.K.; Obradovich, J.E.; Elmslie, R.E.; Vail, D.M.; Moore, A.S.; Straw, R.C.; Dickinson, K.; Cooper, M.F.; Withrow, S.J. Efficacy of mitoxantrone against various neoplasms in dogs. J. Am. Vet. Med. Assoc. 1991, 198, 1618–1621. [Google Scholar] [PubMed]
- Ogilvie, G.K.; A Reynolds, H.; Richardson, R.C.; Withrow, S.J.; Norris, A.M.; Henderson, R.A.; Klausner, J.S.; Fowler, J.D.; McCaw, D. Phase II evaluation of doxorubicin for treatment of various canine neoplasms. J. Am. Vet. Med. Assoc. 1989, 195, 1580–1582. [Google Scholar]
- Chan, C.M.; Frimberger, A.E.; Moore, A.S. Incidence of sterile hemorrhagic cystitis in tumor-bearing dogs concurrently treated with oral metronomic cyclophosphamide chemotherapy and furosemide: 55 cases (2009–2015). J. Am. Vet. Med. Assoc. 2016, 249, 1408–1414. [Google Scholar] [CrossRef]
- Frank, J.D.; Reimer, S.B.; Kass, P.H.; Kiupel, M. Clinical outcomes of 30 cases (1997–2004) of canine gastrointestinal lymphoma. J. Am. Anim. Hosp. Assoc. 2007, 43, 313–321. [Google Scholar] [CrossRef]
- Marconato, L.; Stefanello, D.; Sabattini, S.; Comazzi, S.; Riondato, F.; Laganga, P.; Frayssinet, P.; Pizzoni, S.; Rouquet, N.; Aresu, L. Enhanced therapeutic effect of APAVAC immunotherapy in combination with dose-intense chemotherapy in dogs with advanced indolent B-cell lymphoma. Vaccine 2015, 33, 5080–5086. [Google Scholar] [CrossRef] [PubMed]
- Marconato, L.; Stefanello, D.; Valenti, P.; Bonfanti, U.; Comazzi, S.; Roccabianca, P.; Caniatti, M.; Romanelli, G.; Massari, F.; Zini, E. Predictors of long-term survival in dogs with high-grade multicentric lymphoma. J. Am. Vet. Med. Assoc. 2011, 238, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Marconato, L.; Martini, V.; Stefanello, D.; Moretti, P.; Ferrari, R.; Comazzi, S.; Laganga, P.; Riondato, F.; Aresu, L. Peripheral blood lymphocyte/monocyte ratio as a useful prognostic factor in dogs with diffuse large B-cell lymphoma receiving chemoimmunotherapy. Vet. J. 2015, 206, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Yamzaki, J.; Goto-Koshino, Y.; Takahashi, M.; Fujino, Y.; Ohno, K.; Tsujimoto, H. The prognostic significance of minimal residual disease in the early phases of chemotherapy in dogs with high-grade B-cell lymphoma. Vet. J. 2013, 195, 319–324. [Google Scholar] [CrossRef]
- Hahn, K.A.; Chan, T.C.K.; Morrison, W.B.; Hahn, E.A. High-performance liquid chromatographic analysis of doxorubicin and its metabolites in canine urine. J. Am. Anim. Hosp. Assoc. 1994, 30, 276–280. [Google Scholar]
- Kiupel, M.; Teske, E.; Bostock, D. Prognostic factors for treated canine malignant lymphoma. Vet. Pathol. 1999, 36, 292–300. [Google Scholar] [CrossRef]
- Lee, J.J.; Hughes, C.S.; Fine, R.L.; Page, R.L. P-glycoprotein expression in canine lymphoma—A relevant, intermediate model of multidrug resistance. Cancer 1996, 77, 1892–1898. [Google Scholar] [CrossRef]
- Pinheiro, D.; Chang, Y.-M.; Bryant, H.; Sziadovits, B.; Daiessandri, T.; Davison, L.J.; Yallop, E.; Mills, E.; Leo, C.; Lara, A.; et al. Dissecting the Regulatory Microenvironment of a Large Animal Model of Non-Hodgkin Lymphoma: Evidence of a Negative Prognostic Impact of FOXP3(+) T Cells in Canine B Cell Lymphoma. PLoS ONE 2014, 9, e105027. [Google Scholar] [CrossRef]
- Rao, S.; Lana, S.; Eickhoff, J.; Marcus, E.; Avery, P.R.; Morley, P.S.; Avery, A.C. Class II Major Histocompatibility Complex Expression and Cell Size Independently Predict Survival in Canine B-Cell Lymphoma. J. Vet. Intern. Med. 2011, 25, 1097–1105. [Google Scholar] [CrossRef]
- Vail, D.M.; Kisseberth, W.C.; Obradovich, J.E.; Moore, F.M.; London, C.A.; MacEwen, E.G.; Ritter, M.A. Assessment of potential doubling time (T-pot), argyrophilic nucleolar organizer regions (AgNOR), and proliferating cell nuclear antigen (PCNA) as predictors of therapy response in canine non-Hodgkin’s lymphoma. Exp. Hematol. 1996, 24, 807–815. [Google Scholar]
- von Euler, H.; Einarsson, R.; Olsson, U.; Lagerstedt, A.S.; Eriksson, S. Serum thymidine kinase activity in dogs with malignant lymphoma: A potent marker for prognosis and monitoring the disease. J. Vet. Intern. Med. 2004, 18, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.; Avery, A.; Lana, S.; Hillers, K.; Bachand, A.; Avery, P. Canine lymphoproliferative disease characterized by lymphocytosis: Immunophenotypic markers of prognosis. J. Vet. Intern. Med. 2008, 22, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.H.; Lee, J.J.; Liao, A.T.; Wang, S.L. Paraneoplastic Syndrome as a Prognostic Factor in Dogs with Multicentric Lymphoma. Int. J. Appl. Res. Vet. Med. 2020, 18, 131–141. [Google Scholar]
- Barber, L.G.; Weishaar, K.M. Criteria for designation of clinical substage in canine lymphoma: A survey of veterinary oncologists. Vet. Comp. Oncol. 2016, 14, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Hahn, K.A.; Richardson, R.C.; Hahn, E.A.; Chrisman, C.L. Diagnostic and prognostic importance of chromosomal aberrations identified in 61 dogs with lymphosarcoma. Vet. Pathol. 1994, 31, 528–540. [Google Scholar] [CrossRef]
- Boyé, P.; Serres, F.; Floch, F.; Fournel-Fleury, C.; Tierny, D. Prognostic value of pretreatment plasma D-dimer level in dogs with intermediate to high-grade non-Hodgkin lymphoma. Vet. Comp. Oncol. 2021, 19, 44–52. [Google Scholar] [CrossRef]
- Miller, A.G.; Morley, P.S.; Rao, S.; Avery, A.C.; Lana, S.E.; Olver, C.S. Anemia Is Associated with Decreased Survival Time in Dogs with Lymphoma. J. Vet. Intern. Med. 2009, 23, 116–122. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Response Criteria Reported | Number of Papers | CR Definition (n) | PR Definition (n) | PD Definition (n) |
|---|---|---|---|---|
| CR only | 3 | 100% decrease (2) Not defined (1) | N/A | N/A |
| CR, PR, NR | 38 | 100% decrease (33) 75% decrease (1) 50% decrease (1) Not defined (3) | 50% decrease (39) 25–50% decrease (1) Not defined (8) | Not CR or PR (38) |
| CR, PR, SD, PD | 50 | 100% decrease (50) | 50% decrease (39) 30% decrease (3) Not defined (8) | 50% increase (8) 25% increase (19) 20% increase (4) 10% increase (3) Not defined (16) |
| VCOG or modified RECIST | 30 | 100% decrease (30) | 30% decrease (30) | 20% increase (30) |
| Not stated | 35 | N/A | N/A | N/A |
| Outcome Term | Number of Papers | Variations Included in the Term in This Review |
|---|---|---|
| Remission times | ||
| Progression-free survival | 50 | Disease-free interval Progression-free interval |
| Duration of remission | 30 | Duration of first remission Time of first remission Relapse-free interval Remission time |
| Median response period | 32 | Median duration response Median response time Median response duration |
| Objective response duration | 1 | Objective response time |
| Time to progression | 18 | Time to failure Time to relapse |
| Not available | 25 | |
| Survival times | ||
| Overall survival time | 101 | Median survival time |
| Lymphoma-specific survival | 11 | |
| Length of survival | 1 | |
| Not available | 43 | |
| Outcome | CHOP-like, Multicentric or Nodal Lymphoma (Number of Groups) | CHOP-like, Anatomical Location Not Clearly Defined Lymphoma (n = Number of Groups) | COP-like, Mixed Lymphoma (n = Number of Groups) | CHOP-like, B-Cell Multicentric or Nodal lymphoma (n = Number of Groups) | T-cell Multicentric or Nodal Lymphoma (n = Number of Groups) |
|---|---|---|---|---|---|
| Number of papers | 43 (54) | 26 (33) | 21 (27) | 11 (14) | 8 (9) |
| CR % | 25–100 (45) | 27–100 (24) | 53–90 (23) | 63–100 (5) | 64–92 (4) |
| Mean CR % | 76 | 76 | 71 | 79 | 82 |
| Median CR% | 77 | 78 | 73 | 77 | 86 |
| PR % | 0–33 (34) | 4–21 (19) | 2–40 (21) | 0–15 (3) | 8–11 (3) |
| Mean PR % | 13 | 12 | 18 | 6 | 9 |
| Median PR% | 9 | 12 | 15 | 4.5 | 9 |
| ORR | 64–100 (34) | 27–100 (19) | 56–100 (21) | 64–100 (3) | 73–96 (3) |
| Mean ORR | 86 | 85 | 88 | 83 | 88 |
| Median ORR | 91 | 89 | 90 | 87 | 94 |
| MRT range in days | 41–414 (35) | 28–331 (23) | 28–199 (20) | 41–414 (14) | 118–431 (5) |
| MRT mean in days | 199 | 195 | 125 | 187 | 237 |
| MRT median | 196 | 208 | 128 | 192 | 175 |
| Mean remission in days | 59, 518 (2) | 77, 201 (2) | 31–323 (6) | 59 (1) | NR |
| MRT CR in days | 104–317 (13) | 202–348 (10) | 132–215 (3) | NR | 104–316 (3) |
| MRT PR in days | 43–117 (3) | 41 (1) | 75 (1) | NR | 60 (1) |
| MST range in days | 73–622 (44) | 175–644 (23) | 85–357 (15) | 159–505 (14) | 26–507 (8) |
| MST mean in days | 287 | 333 | 226 | 297 | 200 |
| MST median | 267 | 314 | 224 | 276 | 191 |
| Mean survival in days | 136 (1) | 207–459 (3) | 138–386 (8) | 136 (1) | NR |
| MST CR in days | 244–573 (4) | 309–446 (3) | 266, 290 (2) | NR | 362 (1) |
| MST PR in days | 50–177 (7) | 97–205 (3) | 129, 152 (2) | NR | 177 (1) |
| % Remission at 1 year | 17–46 (6) | 26 (1) | 0–19 (3) | NR | 27, 54 (2) |
| % Remission at 2 years | 12–35 (6) | NR | 0, 5 (2) | NR | 16, 29 (2) |
| % Remission at 3 years | 7–13 (3) | NR | 0 (2) | NR | 12, 13 (2) |
| % Survival at 1 year | 28–70 (10) | 22–57 (7) | 0–40 (6) | NR | 31, 54 (2) |
| % Survival at 2 years | 6–33 (8) | 11–26 (4) | 0–17 (6) | NR | 20, 35 (2) |
| % Survival at 3 years | 12–25 (3) | 4 (1) | 0–15 (5) | NR | 12, 12 (2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bennett, P.; Williamson, P.; Taylor, R. Review of Canine Lymphoma Treated with Chemotherapy—Outcomes and Prognostic Factors. Vet. Sci. 2023, 10, 342. https://doi.org/10.3390/vetsci10050342
Bennett P, Williamson P, Taylor R. Review of Canine Lymphoma Treated with Chemotherapy—Outcomes and Prognostic Factors. Veterinary Sciences. 2023; 10(5):342. https://doi.org/10.3390/vetsci10050342
Chicago/Turabian StyleBennett, Peter, Peter Williamson, and Rosanne Taylor. 2023. "Review of Canine Lymphoma Treated with Chemotherapy—Outcomes and Prognostic Factors" Veterinary Sciences 10, no. 5: 342. https://doi.org/10.3390/vetsci10050342