
Retinal Fundus Multi-Disease Image Dataset (RFMiD) 2.0: A Dataset of Frequently and Rarely Identified Diseases

 ,
,  , , ,
, , ,
Abstract
:1. Summary
2. Data Description
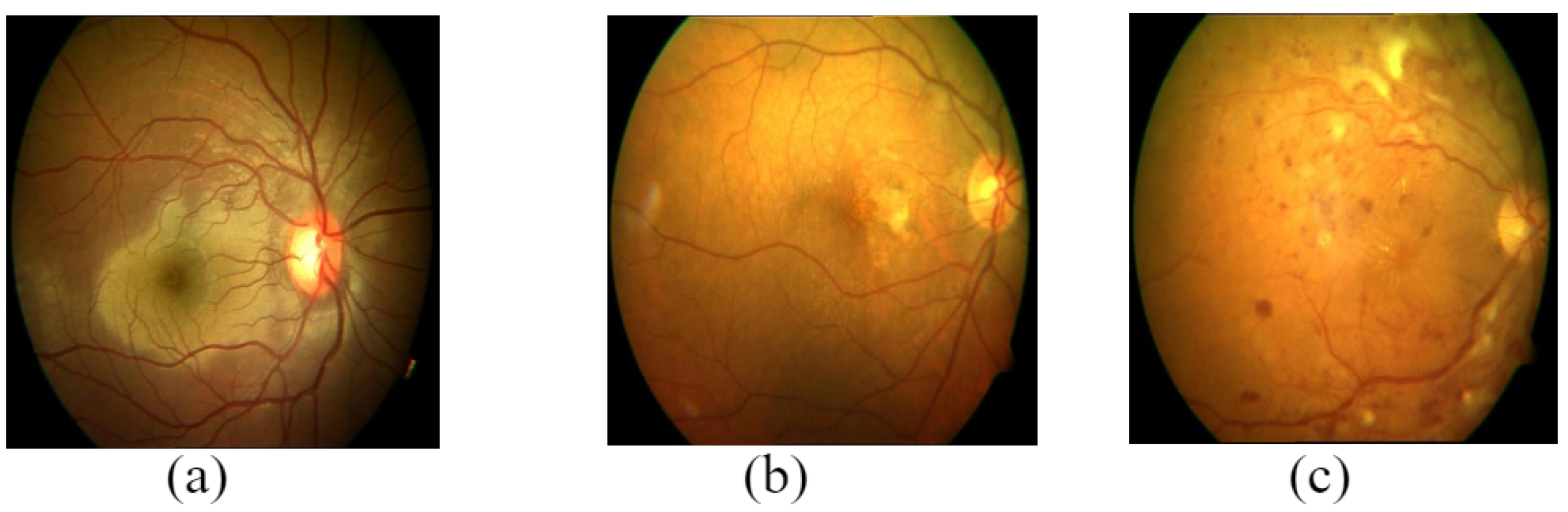
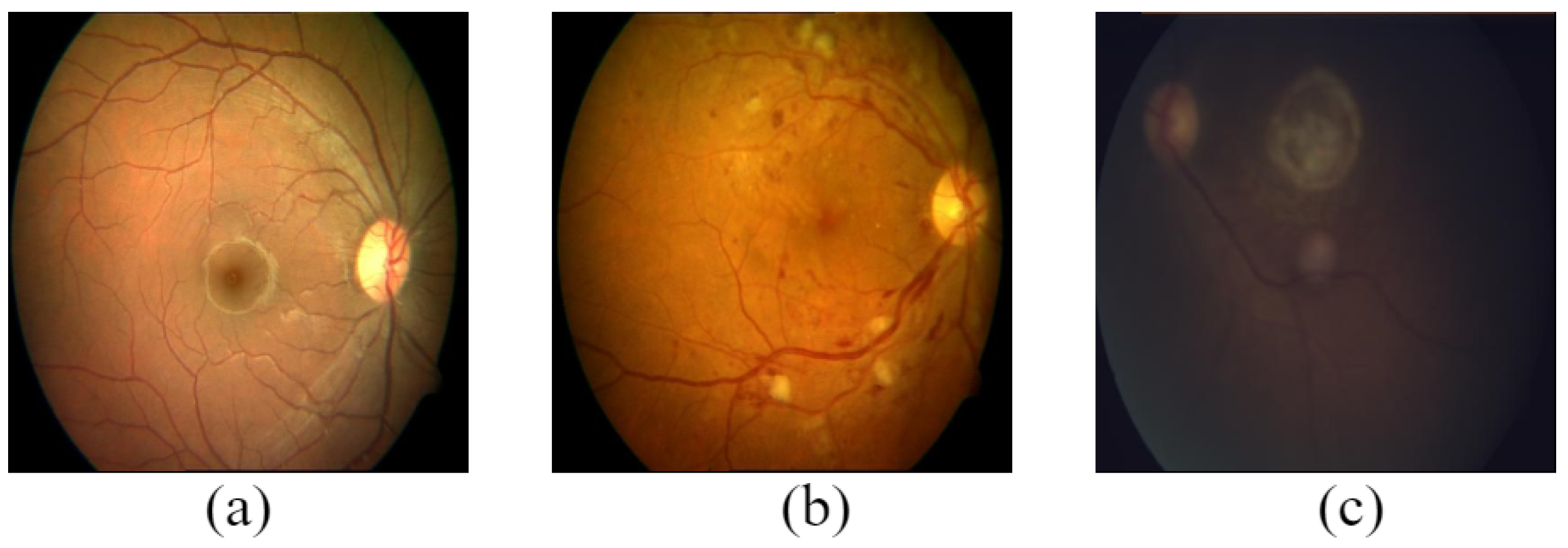
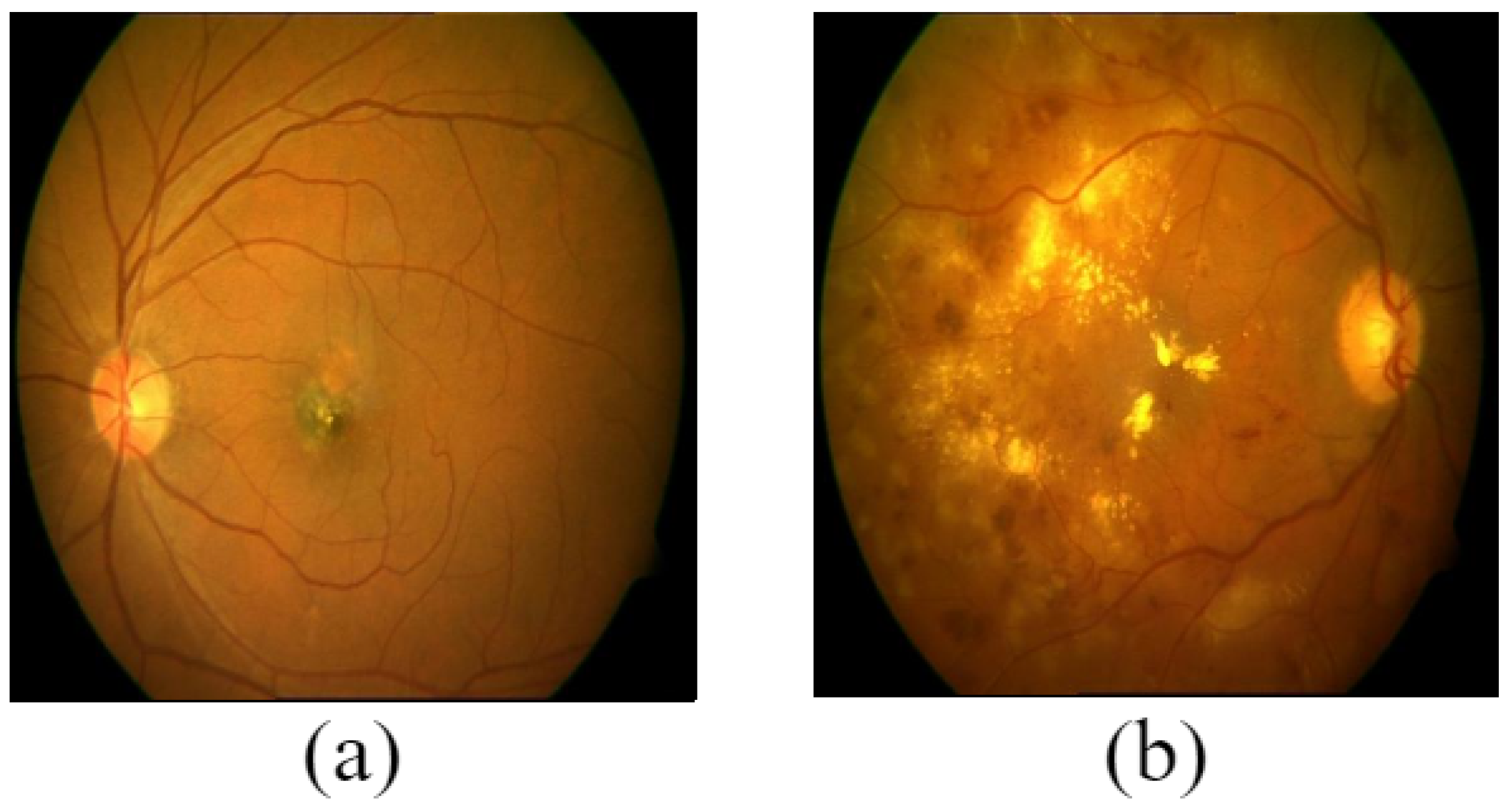
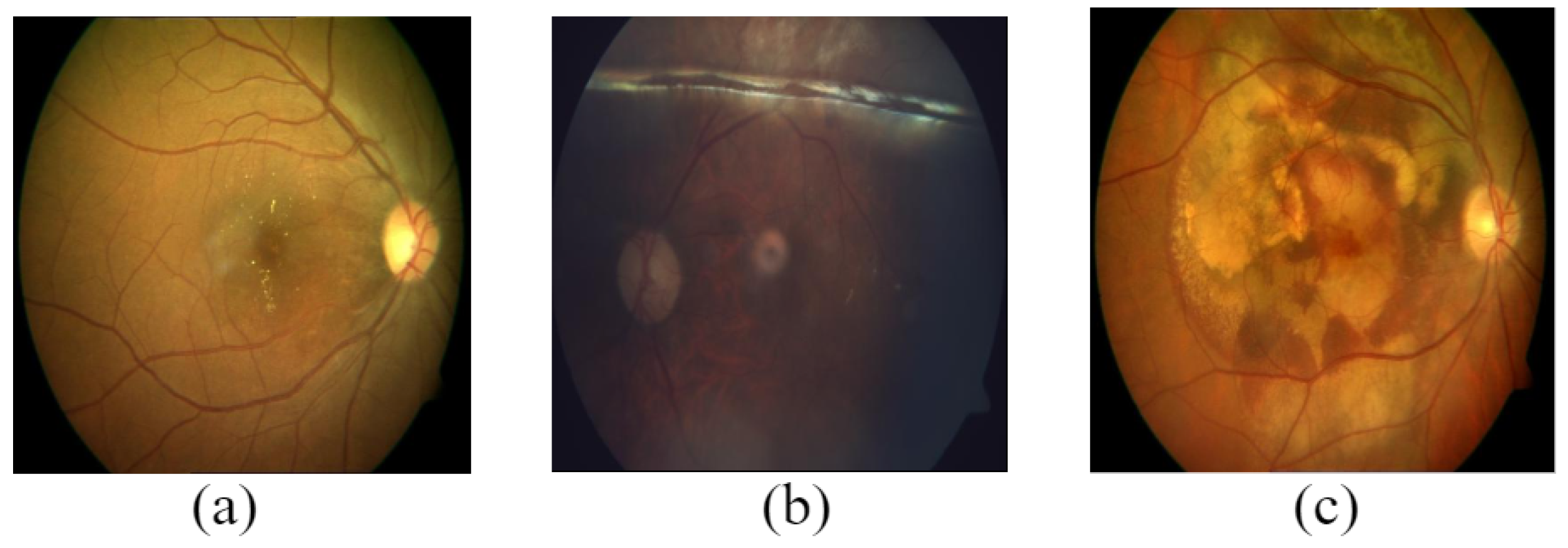
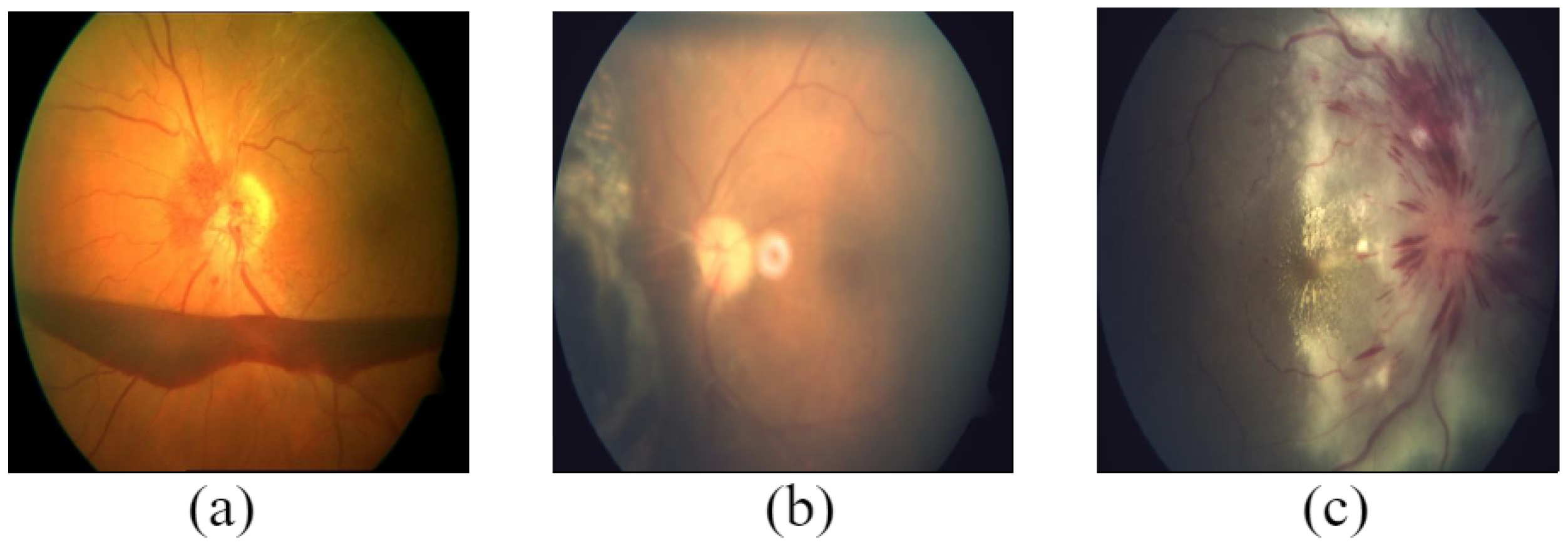
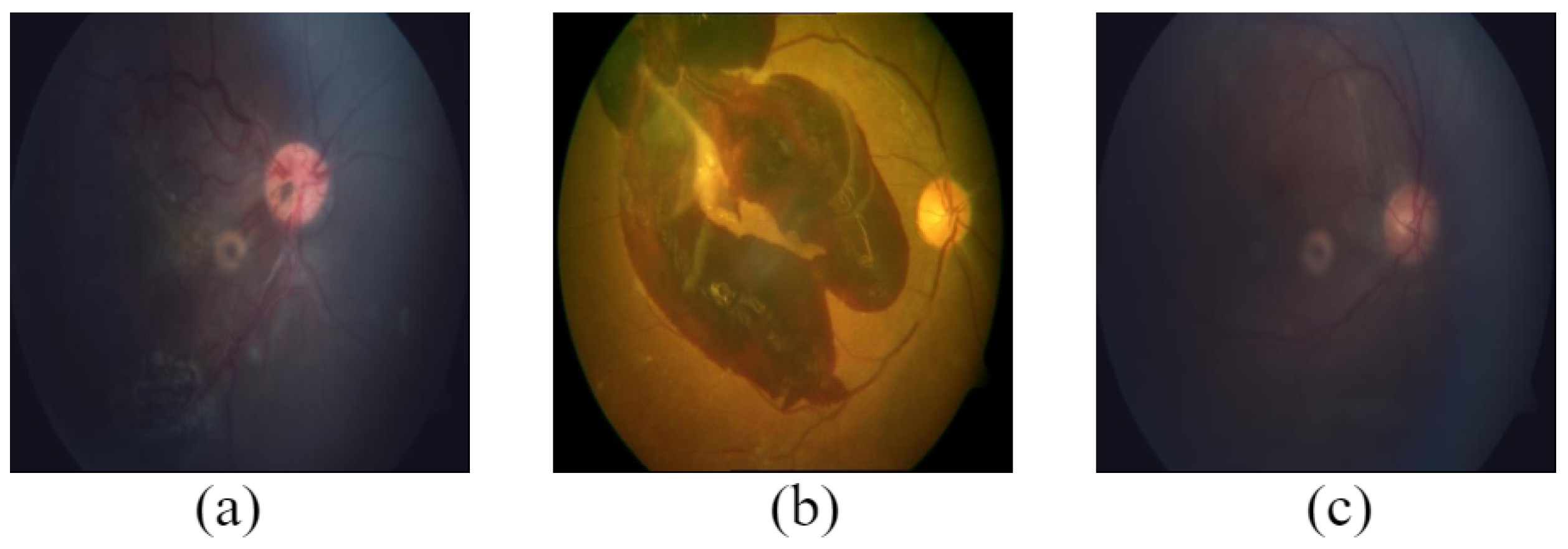
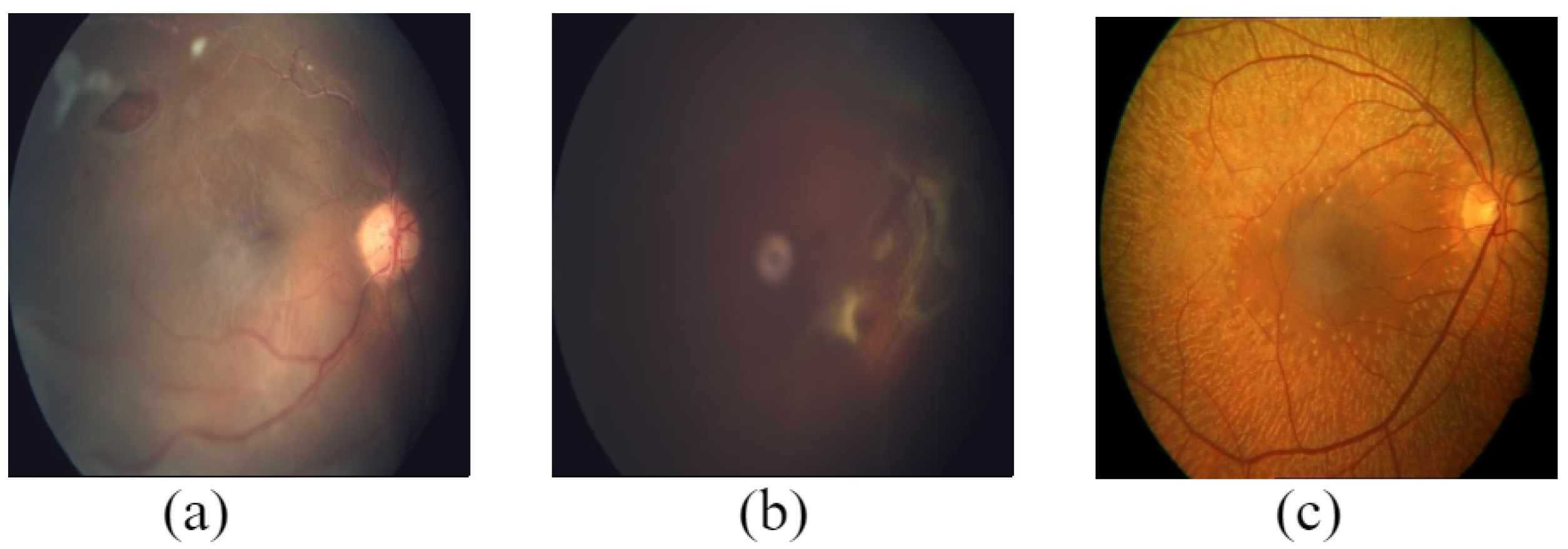
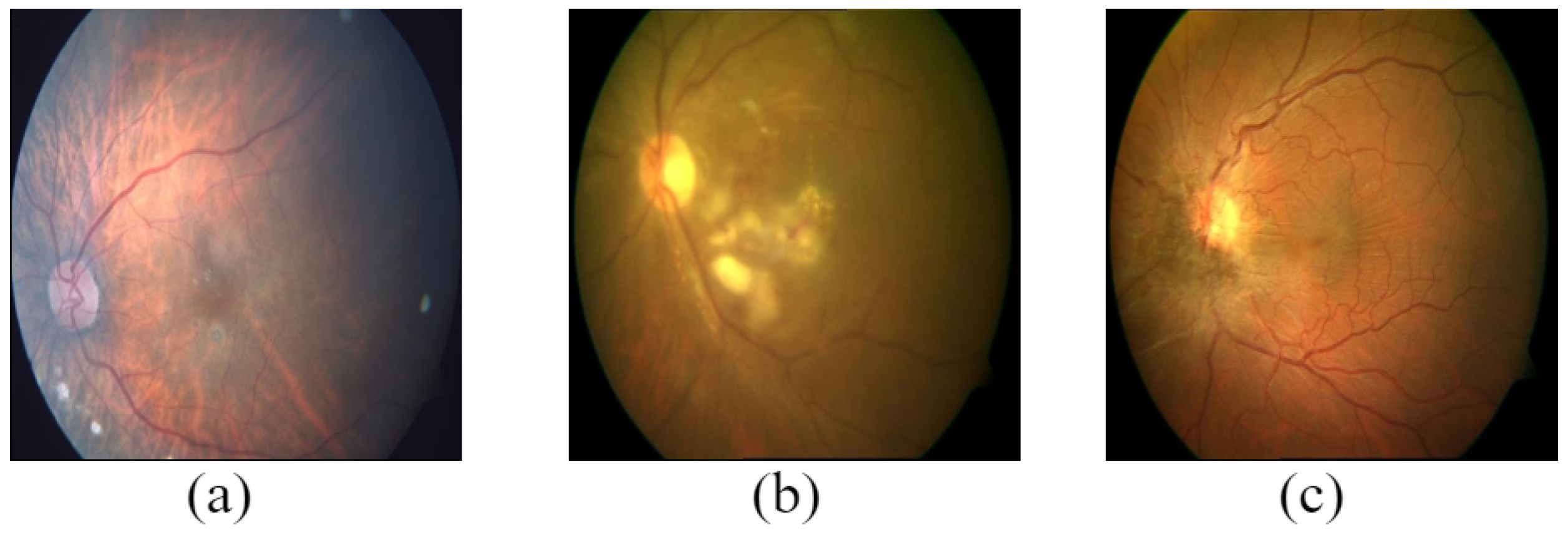
- Firstly, retinal fundus images were screened into healthy and disease-risk categories.
- Further, the disease-risk category was classified into 49 different sub-classes.
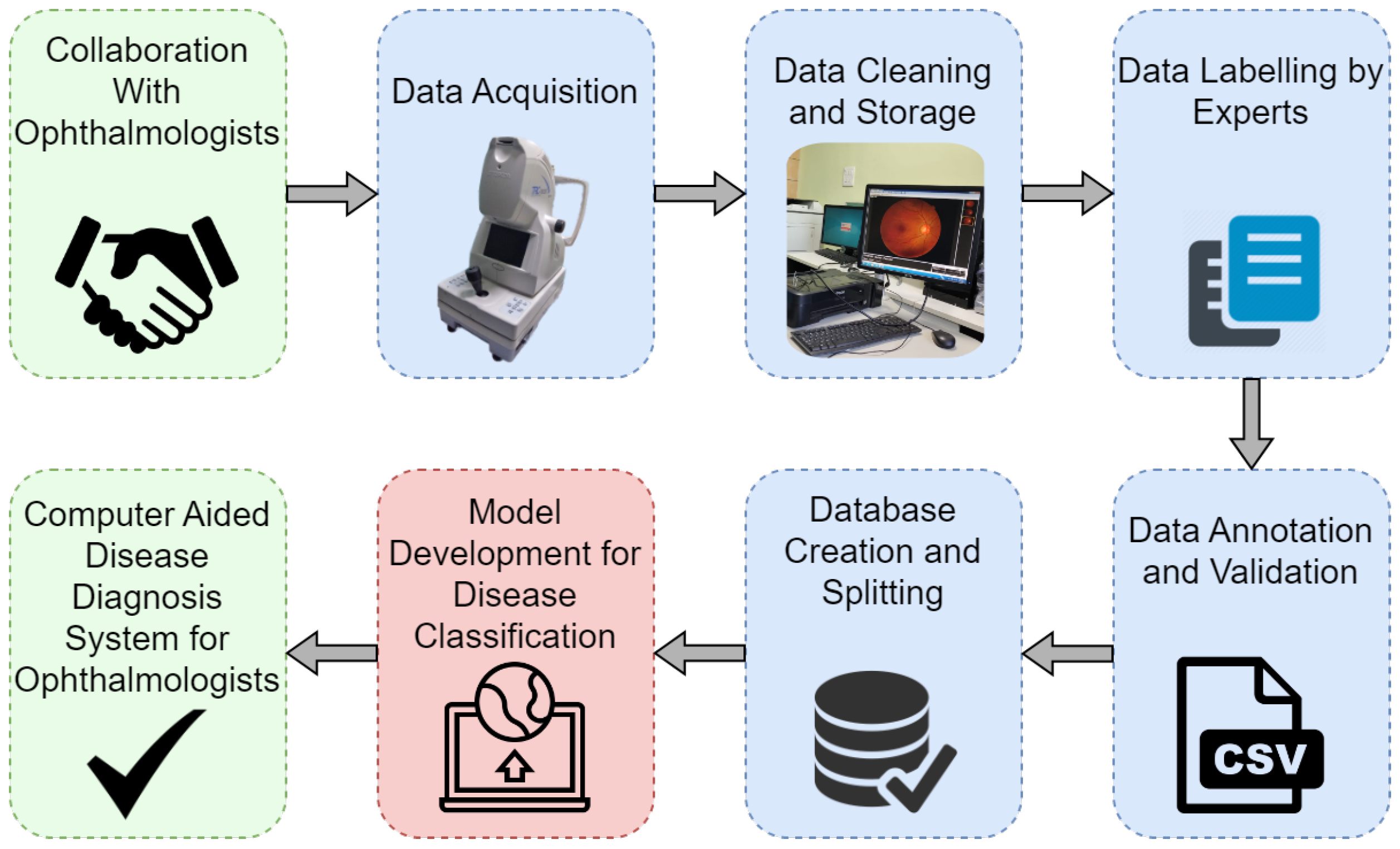
3. Experimental Design, Materials, and Methods
3.1. Ethics Statement
3.2. Data Acquisition
3.2.1. Preparation before Taking Samples
3.2.2. Quality of Image
3.2.3. Camera Specifications
- Eight-megapixel, high-quality images were produced by the integrated digital CCD camera. The angle of view was 45°.
- Fundus camera type: non-Mydriatic
- Auto-focus, auto-exposure, and auto-shoot are vital camera features.
- FF 450plus Fundus Camera and VISUPAC Digital Imaging System are seamlessly integrated for exceptional image quality, operation, and diagnostic adaptability.
- Through reciprocal calibration, the VISUPAC system and the FF 450plus Fundus Camera continuously deliver a distinct level of precision.
- For the fine detail of the macula and optic nerve, the Zeiss FF450 plus Fundus Camera offers three field angles: 50°, 30°, and the smaller 20° field.
3.3. Annotation of Images
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vision Impairment and Blindness. Available online: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment (accessed on 13 October 2022).
- Jelinek, H.; Cree, M.J. Automated Image Detection of Retinal Pathology; CRC Press: Boca Raton, FL, USA, 2009. [Google Scholar]
- Cen, L.P.; Ji, J.; Lin, J.W.; Ju, S.T.; Lin, H.J.; Li, T.P.; Wang, Y.; Yang, J.F.; Liu, Y.F.; Tan, S.; et al. Automatic detection of 39 fundus diseases and conditions in retinal photographs using Deep Neural Networks. Nat. Commun. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.C.; Brown, M.M.; Hiller, T.; Fischer, D.; Benson, W.E.; Magargal, L.E. Cotton-wool spots. Retina 1985, 5, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Shabbir, A.; Rasheed, A.; Shehraz, H.; Saleem, A.; Zafar, B.; Sajid, M.; Ali, N.; Dar, S.H.; Shehryar, T. Detection of glaucoma using retinal fundus images: A comprehensive review. Math. Biosci. Eng. 2021, 18, 2033–2076. [Google Scholar] [CrossRef] [PubMed]
- Mary, V.S.; Rajsingh, E.B.; Naik, G.R. Retinal fundus image analysis for diagnosis of glaucoma: A comprehensive survey. IEEE Access 2016, 4, 4327–4354. [Google Scholar] [CrossRef]
- Catania, C.A.; Bromberg, F.; Garino, C.G. An autonomous labeling approach to support vector machines algorithms for network traffic anomaly detection. Expert Syst. Appl. 2012, 39, 1822–1829. [Google Scholar] [CrossRef]
- Huang, Y.M.; Hung, C.M.; Jiau, H.C. Evaluation of neural networks and data mining methods on a credit assessment task for class imbalance problem. Nonlinear Anal. Real World Appl. 2006, 7, 720–747. [Google Scholar] [CrossRef]
- Jain, A.; Ratnoo, S.; Kumar, D. Addressing class imbalance problem in medical diagnosis: A genetic algorithm approach. In Proceedings of the 2017 International Conference on Information, Communication, Instrumentation and Control (ICICIC), Indore, India, 17–19 August 2017; pp. 1–8. [Google Scholar] [CrossRef]
- Tarekegn, A.; Ricceri, F.; Costa, G.; Ferracin, E.; Giacobini, M. Predictive modeling for frailty conditions in elderly people: Machine learning approaches. JMIR Med. Inform. 2020, 8, e16678. [Google Scholar] [CrossRef]
- Bullock, J.; Luccioni, A.; Pham, K.H.; Lam, C.S.N.; Luengo-Oroz, M. Mapping the landscape of artificial intelligence applications against COVID-19. J. Artif. Intell. Res. 2020, 69, 807–845. [Google Scholar] [CrossRef]
- Topcon TRC NW300—Topcon Europe Medical—PDF Catalogs|Technical Documentation. Available online: https://pdf.medicalexpo.com/pdf/topcon-europe-medical/topcon-trc-nw300/77876-75596.html (accessed on 23 October 2022).
- Zeiss FF450plus Fundus Camera with VISUPAC|Technical Brochure. Available online: https://www.zeiss.com/content/dam/Meditec/us/brochures/ff450plus-visupac-cap-en-us-31-020-0025i.pdf (accessed on 23 October 2022).
- Paulus, J.; Meier, J.; Bock, R.; Hornegger, J.; Michelson, G. Automated quality assessment of retinal fundus photos. Int. J. Comput. Assist. Radiol. Surg. 2010, 5, 557–564. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Smith, L.E. Retinal vasculature in development and diseases. Annu. Rev. Vis. Sci. 2018, 4, 101. [Google Scholar] [CrossRef]
- Tripathy, K. Asteroid hyalosis. N. Engl. J. Med. 2018, 379, e12. [Google Scholar] [CrossRef]
- Fontal, M.R.; Kerrison, J.B.; Garcia, R.; Oria, V. Ischemic optic neuropathy. Semin. Neurol. 2007, 27, 221–232. [Google Scholar] [CrossRef]
- Hayreh, S.S. Ischemic optic neuropathy. Prog. Retin. Eye Res. 2009, 28, 34–62. [Google Scholar] [CrossRef]
- Nowak, J.Z. Age-related macular degeneration (AMD): Pathogenesis and therapy. Pharmacol. Rep. 2006, 58, 353. [Google Scholar]
- DeAngelis, M.M.; Owen, L.A.; Morrison, M.A.; Morgan, D.J.; Li, M.; Shakoor, A.; Vitale, A.; Iyengar, S.; Stambolian, D.; Kim, I.K.; et al. Genetics of age-related macular degeneration (AMD). Hum. Mol. Genet. 2017, 26, R45–R50. [Google Scholar] [CrossRef] [Green Version]
- Kösea, C.; Sevika, U.; Gençalioglub, O. Automatic segmentation of age-related macular degeneration in retinal fundus images. Comput. Biol. Med. 2008, 38, 611–619. [Google Scholar] [CrossRef]
- Jager, R.D.; Mieler, W.F.; Miller, J.W. Age-Related Macular Degeneration. N. Engl. J. Med. 2008, 358, 2606–2617. [Google Scholar] [CrossRef] [Green Version]
- Rogers, S.; McIntosh, R.; Cheung, N.; Lim, L.; Wang, J.; Mitchell, P.; Kowalski, J.; Nguyen, H.; Wong, T. International Eye Disease Consortium: The prevalence of retinal vein occlusion: Pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010, 117, 313–319. [Google Scholar] [CrossRef] [Green Version]
- Gopal, L.; Badrinath, S.S.; Kumar, K.; Doshi, G.; Biswas, N. Optic Disc in Fundus Colobama. Ophthalmology 1996, 103, 2120–2127. [Google Scholar] [CrossRef]
- Grosso, D.; Borrelli, E.; Sacconi, R.; Bandello, F.; Querques, G. Recognition, diagnosis and treatment of chorioretinal folds: Current perspectives. Clin. Ophthalmol. 2020, 14, 3403. [Google Scholar] [CrossRef]
- Henkind, P.; Wise, G.N. Retinal neovascularization, collaterals, and vascular shunts. Br. J. Ophthalmol. 1974, 58, 413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotsos, T.G.; Moschos, M.M. Cystoid macular edema. Clin. Ophthalmol. 2008, 2, 919–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, M.C.S.; Teoh, S.S.; Ibrahim, H.; Embong, Z. Neovascularization detection and localization in fundus images using deep learning. Sensors 2021, 21, 5327. [Google Scholar] [CrossRef] [PubMed]
- Hayreh, S. Central retinal artery occlusion. Indian J. Ophthalmol. 2018, 66, 1684. [Google Scholar] [CrossRef]
- Chorioretinitis—Statpearls—NCBI Bookshelf. Available online: https://www.ncbi.nlm.nih.gov/books/NBK551705/ (accessed on 28 October 2022).
- Cheung, N.; Klein, R.; Wang, J.J.; Cotch, M.F.; Islam, A.F.; Klein, B.E.; Cushman, M.; Wong, T.Y. Traditional and novel cardiovascular risk factors for retinal vein occlusion: The multiethnic study of atherosclerosis. Investig. Ophthalmol. Vis. Sci. 2008, 49, 4297–4302. [Google Scholar] [CrossRef]
- Rebika, D.; Saranya, D.; Kavitha, D.; Parijat, C.; Murugesan, V.; Radhika, T.; Sen, S. Cysticercosis of the eye. Int. J. Ophthalmol. 2017, 10, 1319–1324. [Google Scholar] [CrossRef]
- Optic Disc Pallor: Ophthalmoscopic Abnormalities: The Eyes Have It. Available online: http://kellogg.umich.edu/theeyeshaveit/opticfundus/disc_pallor.html (accessed on 28 October 2022).
- Schmidt, D. The mystery of cotton-wool spots-a review of recent and historical descriptions. Eur. J. Med. Res. 2008, 13, 231. [Google Scholar]
- Mittal, D.; Kumari, K. Automated detection and segmentation of drusen in retinal fundus images. Comput. Electr. Eng. 2015, 47, 82–95. [Google Scholar] [CrossRef]
- Wang, W.; Lo, A.C. Diabetic retinopathy: Pathophysiology and treatments. Int. J. Mol. Sci. 2018, 19, 1816. [Google Scholar] [CrossRef] [Green Version]
- Kempen, J.H.; O’Colmain, B.J.; Leske, M.C.; Haffner, S.M.; Klein, R.; Moss, S.E.; Taylor, H.R.; Hamman, R.F. The prevalence of diabetic retinopathy among adults in the United States. Arch. Ophthalmol. 2004, 122, 552–563. [Google Scholar] [CrossRef] [Green Version]
- Panchal, S.; Kokare, M. A Comprehensive Survey on the Detection of Diabetic Retinopathy. IETE J. Res. 2022. [Google Scholar] [CrossRef]
- American Society of Retina Specialists, Epiretinal Membranes. Available online: https://www.asrs.org/patients/retinal-diseases/19/epiretinal-membranes (accessed on 22 November 2022).
- Berrocal, M.; Chenworth, M.; Acaba, L. Management of giant retinal tear detachments. J. Ophthalmic Vis. Res. 2017, 12, 93. [Google Scholar] [CrossRef]
- Kim, L.A.; Lee, S.Y.; Thorell, M.R.; Tripathy, K.; Barros, N.; Hacopian, A.; Kiernan, D.F.; Bhagat, N.; Lim, J.I.; Jung, E.E. Pigment Epithelial Detachment. Available online: https://eyewiki.aao.org/Pigment_Epithelial_Detachment (accessed on 22 November 2022).
- Sargues, L.R.; Sanchis, M.I.S.; Adsuara, C.M.; Villanueva, C.G.; Salvador, B.L.; Taulet, E.C. Incidental idiopathic intracranial hypertension. Rom. J. Ophthalmol. 2021, 65, 187. [Google Scholar] [CrossRef]
- Modi, P.; Arsiwalla, T. Hypertensive retinopathy. In StatPearls [Internet]; StatPearls Publishing: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Kaur, N.; Chatterjee, S.; Acharyya, M.; Kaur, J.; Kapoor, N.; Gupta, S. A supervised approach for automated detection of hemorrhages in retinal fundus images. In Proceedings of the 2016 5th International Conference on Wireless Networks and Embedded Systems (WECON), Rajpura, India, 14–16 October 2016; pp. 1–5. [Google Scholar] [CrossRef]
- Tang, L.; Niemeijer, M.; Reinhardt, J.M.; Garvin, M.K.; Abramoff, M.D. Splat feature classification with application to retinal hemorrhage detection in fundus images. IEEE Trans. Med. Imaging 2012, 32, 364–375. [Google Scholar] [CrossRef]
- Aziz, T.; Ilesanmi, A.E.; Charoenlarpnopparut, C. Efficient and Accurate Hemorrhages Detection in Retinal Fundus Images Using Smart Window Features. Appl. Sci. 2021, 11, 6391. [Google Scholar] [CrossRef]
- Wei, Q.; Li, X.; Wang, H.; Ding, D.; Yu, W.; Chen, Y. Laser scar detection in fundus images using convolutional neural networks. In Computer Vision—ACCV 2018; Springer: Cham, Switzerland, 2018; pp. 191–206. [Google Scholar] [CrossRef]
- Benzamin, A.; Chakraborty, C. Detection of hard exudates in retinal fundus images using deep learning. In Proceedings of the 2018 Joint 7th International Conference on Informatics, Electronics & Vision (ICIEV) and 2018 2nd International Conference on Imaging, Vision & Pattern Recognition (icIVPR), Kitakyushu, Japan, 25–29 June 2018; pp. 465–469. [Google Scholar] [CrossRef] [Green Version]
- Sengar, N.; Joshi, R.C.; Dutta, M.K. An Efficient Artificial Intelligence-based approach for Diagnosis of Media Haze Disease. In Proceedings of the 2021 12th International Conference on Computing Communication and Networking Technologies (ICCCNT), Kharagpur, India, 6–8 July 2021; pp. 1–6. [Google Scholar] [CrossRef]
- Kim, K.M.; Heo, T.Y.; Kim, A.; Kim, J.; Han, K.J.; Yun, J.; Min, J.K. Development of a fundus image-based deep learning diagnostic tool for various retinal diseases. J. Pers. Med. 2021, 11, 321. [Google Scholar] [CrossRef]
- Bahia-Oliveira, L.M.; Rangel, A.L.; Boechat, M.S.; Mangiavacchi, B.M.; Martins, L.M.; Ferraz, F.B.; Almeida, M.B.; Peixoto, E.M.W.; Vieira, F.P.; Peixe, R.G. Immunological and immunogenetic parameters on the diversity of ocular toxoplasmosis: Evidence to support morphological criteria to classify retinal/retinochoroidal scar lesions in epidemiologic surveys. In Toxoplasmosis-Recent Advances; IntechOpen: London, UK, 2012. [Google Scholar] [CrossRef] [Green Version]
- Devda, J.; Eswari, R. Pathological myopia image analysis using deep learning. Procedia Comput. Sci. 2019, 165, 239–244. [Google Scholar] [CrossRef]
- Wan, C.; Li, H.; Cao, G.F.; Jiang, Q.; Yang, W.H. An Artificial Intelligent Risk Classification Method of High Myopia Based on Fundus Images. J. Clin. Med. 2021, 10, 4488. [Google Scholar] [CrossRef]
- Urfalioglu, S.; Ozdemir, G.; Guler, M.; Duman, G.G. The evaluation of patients with optic disc edema: A retrospective study. North. Clin. Istanb. 2021, 8, 280. [Google Scholar] [CrossRef]
- Benjamin, O. Optic Neuritis: Pathophysiology, Clinical Features, and Diagnosis. Available online: https://www.uptodate.com/contents/optic-neuritis-pathophysiology-clinical-features-and-diagnosis (accessed on 12 December 2022).
- Pachade, S.; Porwal, P.; Thulkar, D.; Kokare, M.; Deshmukh, G.; Sahasrabuddhe, V.; Giancardo, L.; Quellec, G.; Mériaudeau, F. Retinal fundus multi-disease image dataset (RFMiD): A dataset for multi-disease detection research. Data 2021, 6, 14. [Google Scholar] [CrossRef]
- Karagiannis, D.; Kontadakis, G.A.; Flanagan, D. ND: YAG laser for preretinal hemorrhage in diabetic retinopathy. Am. J. Ophthalmol. Case Rep. 2018, 10, 8–9. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Guo, C.; Nie, D.; Lin, D.; Zhu, Y.; Chen, C.; Wu, X.; Xu, F.; Jin, C.; Zhang, X.; et al. Deep learning for detecting retinal detachment and discerning macular status using ultra-widefield fundus images. Commun. Biol. 2020, 3, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russel, L. Retinal Holes and Tears. Available online: https://www.optometrists.org/general-practice-optometry/guide-to-eye-conditions/guide-to-retinal-diseases/retinal-holes-and-tears/ (accessed on 23 December 2022).
- Hamel, C. Retinitis pigmentosa. Orphanet J. Rare Dis. 2006, 1, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Bonilha, V.L. Age and disease-related structural changes in the retinal pigment epithelium. Clin. Ophthalmol. 2008, 2, 413–424. [Google Scholar] [CrossRef] [Green Version]
- Gupta, K.; Tripathy, N. Retinitis. Available online: https://pubmed.ncbi.nlm.nih.gov/32809355/ (accessed on 22 December 2022).
- Gonvers, M. Temporary Silicone Oil Tamponade in the Management of Retinal Detachment with Proliferative Vitreoretinopathy. Am. J. Ophthalmol. 1985, 100, 239–245. [Google Scholar] [CrossRef]
- Cohen, S.Y.; Vignal-Clermont, C.; Trinh, L.; Ohno-Matsui, K. Tilted disc syndrome (TDS): New hypotheses for posterior segment complications and their implications in other retinal diseases. Prog. Retin. Eye Res. 2021, 88, 101020. [Google Scholar] [CrossRef]
- Ohno-Matsui, K.; Lai, T.Y.; Lai, C.C.; Cheung, C.M.G. Updates of pathologic myopia. Prog. Retin. Eye Res. 2016, 52, 156–187. [Google Scholar] [CrossRef]
- Lyu, H.; Chen, Q.; Hu, G.; Shi, Y.; Ye, L.; Yin, Y.; Fan, Y.; Zou, H.; He, J.; Zhu, J.; et al. Characteristics of Fundal Changes in Fundus Tessellation in Young Adults. Front. Med. 2021, 8, 616249. [Google Scholar] [CrossRef]
- Joshi, V.; Reinhardt, J.M.; Abràmoff, M.D. Automated measurement of retinal blood vessel tortuosity. In Medical Imaging 2010: Computer-Aided Diagnosis, Proceedings of the SPIE Medical Imaging, San Diego, CA, USA, 13–18 February 2010; SPIE: Bellingham, WA, USA, 2010; Volume 7624, pp. 929–937. [Google Scholar] [CrossRef]
- Jennette, J.C.; Falk, R.J. Small-Vessel Vasculitis. N. Engl. J. Med. 1997, 337, 1512–1523. [Google Scholar] [CrossRef]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject area | Ophthalmology, Biomedical Data |
| More specific subject area | Multiple Disease Classification of Retinal fundus images |
| Type of data | Images, CSV files |
| How data was acquired | TOPCON TRC-NW300 |
| Data format | Labelling and Annotation of .JPEG, .PNG image files into .CSV files |
| Experimental factors | Most of the patients were subjected to mydriasis with one drop of tropicamide at 0.5% Concentration. The non-Mydriatic process is conducted for some subjects. |
| Experimental features | The fundus images were captured with position and orientation of the patient sitting upright with 40.7 mm (TOPCON TRC-NW300) and 42 mm (CARL ZEISS FF450) working distance between lenses and examined eye using non-invasive fundus camera. |
| Data source location | State of Art Eye Care Hospital, Shri Ganpati Netralaya located at Jalna, Maharashtra, India. Center of Excellence in Signal and Image Processing, SGGS Institute of Engineering and Technology, Nanded, Maharashtra, India. |
| Sr. No. | Normal/Disease | Fundus Images | Sr. No. | Normal/Disease | Fundus Images |
|---|---|---|---|---|---|
| 1 | WNL | 262 | 26 | MH | 41 |
| 2 | AH | 2 | 27 | MHL | 7 |
| 3 | AION | 4 | 28 | MS | 31 |
| 4 | ARMD | 10 | 29 | MYA | 43 |
| 5 | BRVO | 22 | 30 | ODC | 37 |
| 6 | CB | 4 | 31 | ODE | 20 |
| 7 | CF | 7 | 32 | ODP | 18 |
| 8 | CL | 6 | 33 | ON | 2 |
| 9 | CNV | 2 | 34 | OPDM | 1 |
| 10 | CRAO | 1 | 35 | PRH | 12 |
| 11 | CRS | 41 | 36 | RD | 16 |
| 12 | CRVO | 12 | 37 | RHL | 1 |
| 13 | CSR | 16 | 38 | RTR | 2 |
| 14 | CWS | 31 | 39 | RP | 4 |
| 15 | CSC | 1 | 40 | RPEC | 4 |
| 16 | DN | 6 | 41 | RS | 8 |
| 17 | DR | 70 | 42 | RT | 41 |
| 18 | EDN | 70 | 43 | SOFE | 4 |
| 19 | ERM | 5 | 44 | ST | 4 |
| 20 | GRT | 1 | 45 | TD | 16 |
| 21 | HPED | 3 | 46 | TSLN | 37 |
| 22 | HR | 86 | 47 | TV | 18 |
| 23 | LS | 16 | 48 | VS | 7 |
| 24 | MCA | 8 | 49 | HTN | 11 |
| 25 | ME | 41 | 50 | IIH | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panchal, S.; Naik, A.; Kokare, M.; Pachade, S.; Naigaonkar, R.; Phadnis, P.; Bhange, A. Retinal Fundus Multi-Disease Image Dataset (RFMiD) 2.0: A Dataset of Frequently and Rarely Identified Diseases. Data 2023, 8, 29. https://doi.org/10.3390/data8020029
Panchal S, Naik A, Kokare M, Pachade S, Naigaonkar R, Phadnis P, Bhange A. Retinal Fundus Multi-Disease Image Dataset (RFMiD) 2.0: A Dataset of Frequently and Rarely Identified Diseases. Data. 2023; 8(2):29. https://doi.org/10.3390/data8020029
Chicago/Turabian StylePanchal, Sachin, Ankita Naik, Manesh Kokare, Samiksha Pachade, Rushikesh Naigaonkar, Prerana Phadnis, and Archana Bhange. 2023. "Retinal Fundus Multi-Disease Image Dataset (RFMiD) 2.0: A Dataset of Frequently and Rarely Identified Diseases" Data 8, no. 2: 29. https://doi.org/10.3390/data8020029