
PERSIST: A Multimodal Dataset for the Prediction of Perceived Exertion during Resistance Training

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Flywheel Training Machine
2.3. Study Setup
2.4. Inertial Measurement Unit Sensors
2.5. Electrocardiography Device
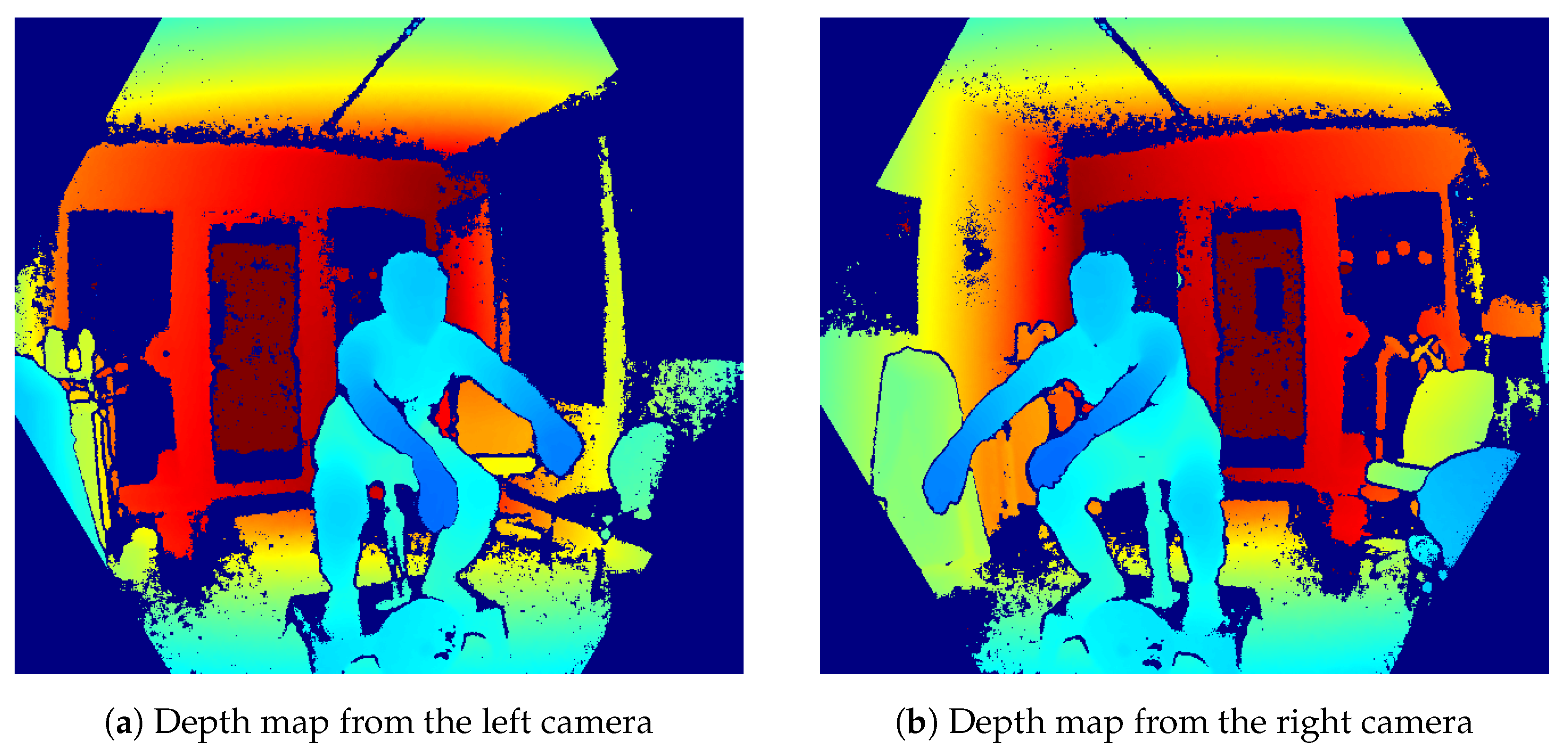
2.6. Microsoft Azure Kinect Cameras
2.7. Protocol Definition
3. Data
3.1. Dataset Structure
- anthro.json: contains anthropometric data and subject information, such as age, weight, height, lactate values, session RPE, and repetition time from the max speed test.
- rpe.json: contains RPE values for each set.
- kmeter.json: contains Flywheel data, such as peak speed, average power, power concentric, power eccentric, force, and range for each repetition.
- time_selection.json: contains manually selected timestamps for the start and end of the entire fatigue protocol as well as for each set
- truncate_info.json: This file contains information regarding additional cropping of the selection from time_selection.json using an automated process to remove even more sensor data not observed during a squat movement
3.2. ECG Data Processing
3.3. Skeleton Data Processing
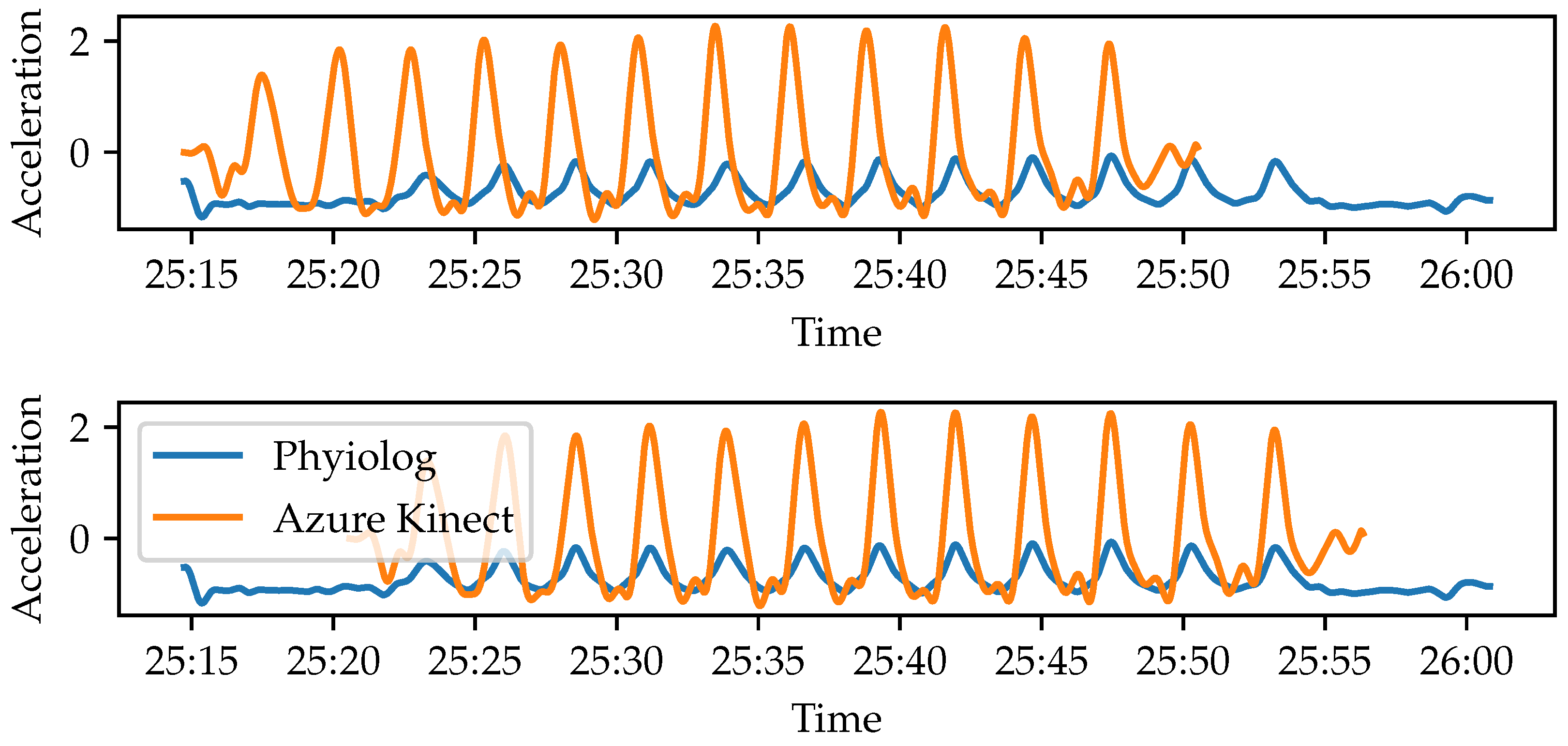
3.4. Synchronization of Azure Kinect and IMU Data
4. Evaluation
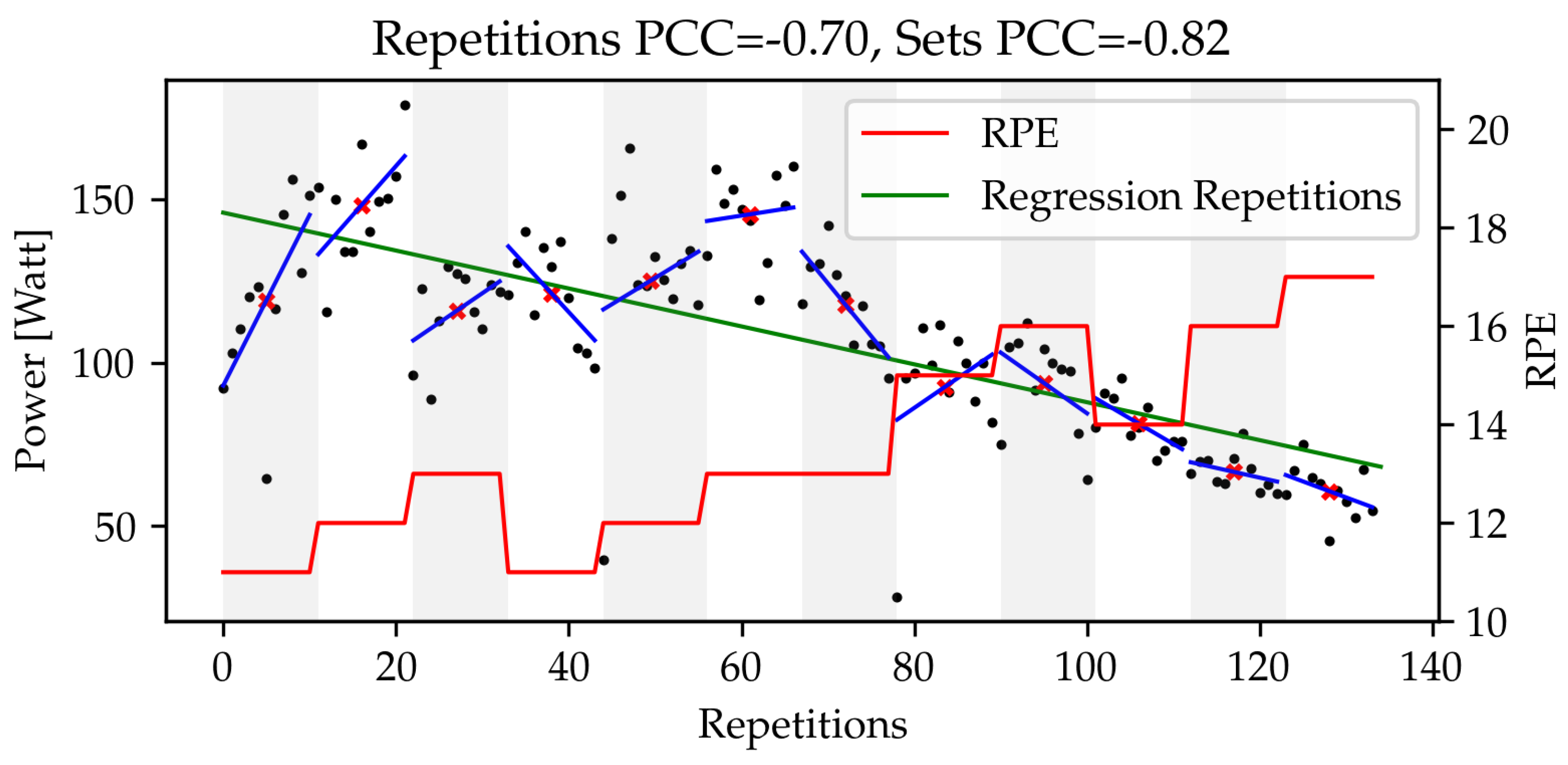
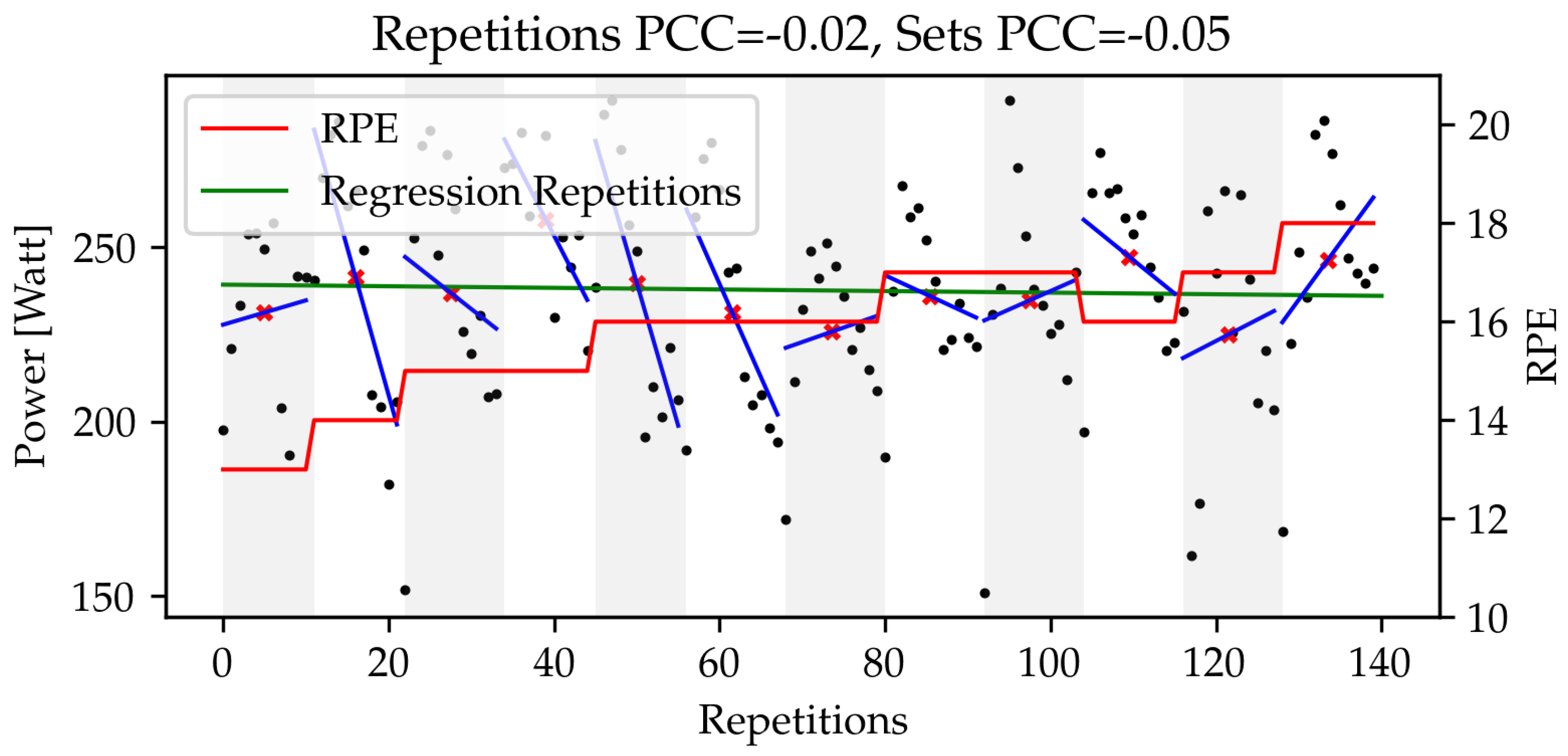
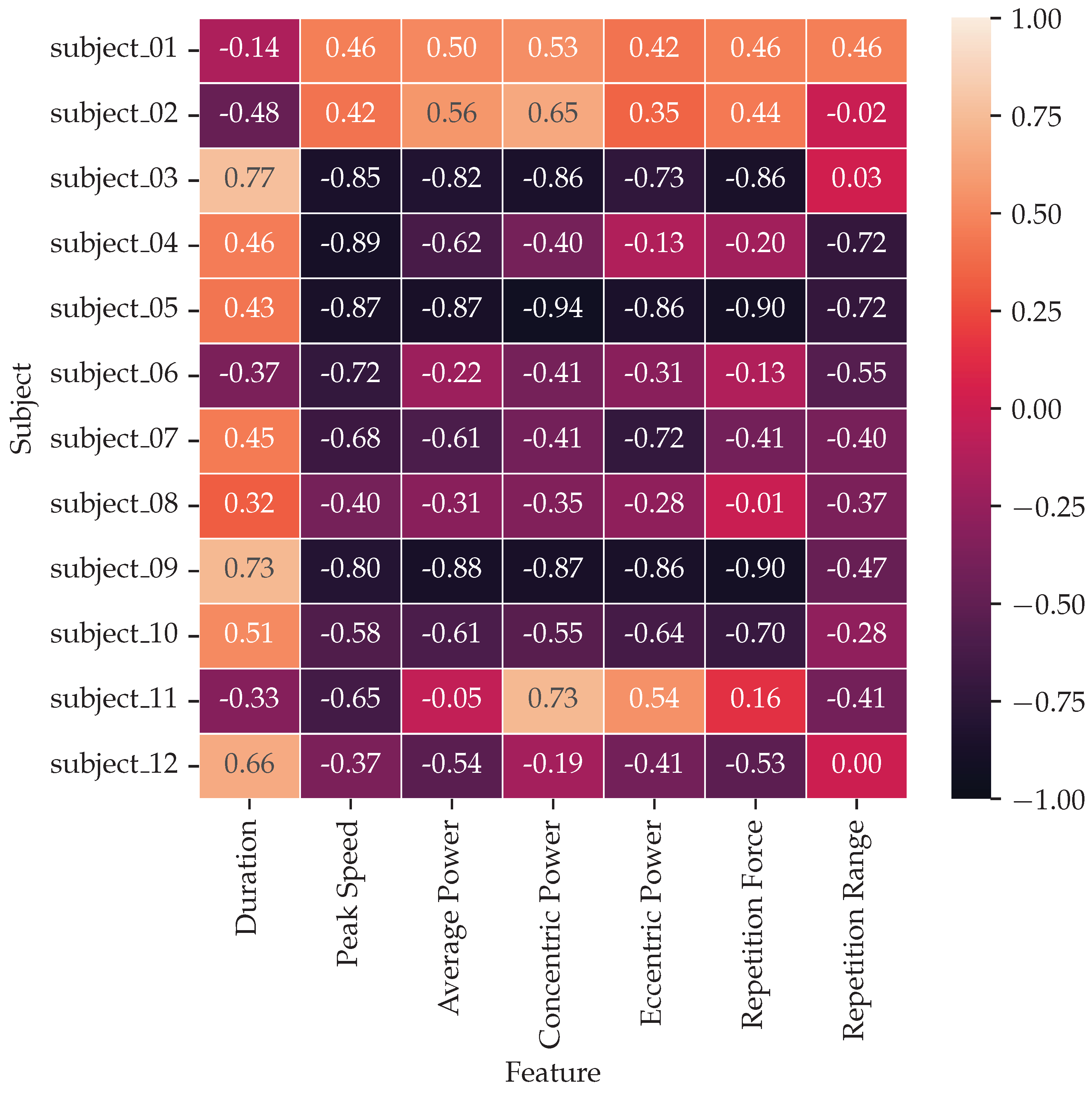
4.1. Exploratory Data Analysis
4.2. Prediction of Subjective Exertion Using Heart Rate and IMU Data
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Borresen, J.; Lambert, M.I. The quantification of training load, the training response and the effect on performance. Sport. Med. 2009, 39, 779–795. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.R.; Duthie, G.M.; Thornton, H.R.; Dascombe, B.J. Training monitoring for resistance exercise: Theory and applications. Sport. Med. 2016, 46, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar]
- Davidson, P.; Düking, P.; Zinner, C.; Sperlich, B.; Hotho, A. Smartwatch-derived data and machine learning algorithms estimate classes of ratings of perceived exertion in runners: A pilot study. Sensors 2020, 20, 2637. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Hernandez, V.; Venture, G.; Kulić, D.K.; Chen, B. A data-driven approach to predict fatigue in exercise based on motion data from wearable sensors or force plate. Sensors 2021, 21, 1499. [Google Scholar] [CrossRef] [PubMed]
- Pernek, I.; Kurillo, G.; Stiglic, G.; Bajcsy, R. Recognizing the intensity of strength training exercises with wearable sensors. J. Biomed. Inform. 2015, 58, 145–155. [Google Scholar] [CrossRef] [Green Version]
- Carey, D.L.; Ong, K.; Morris, M.E.; Crow, J.; Crossley, K.M. Predicting ratings of perceived exertion in Australian football players: Methods for live estimation. Int. J. Comput. Sci. Sport 2016, 15, 64–77. [Google Scholar] [CrossRef] [Green Version]
- Vandewiele, G.; Geurkink, Y.; Lievens, M.; Ongenae, F.; De Turck, F.; Boone, J. Enabling training personalization by predicting the session rate of perceived exertion (sRPE). In Proceedings of the Machine Learning and Data Mining for Sports Analytics ECML/PKDD 2017 Workshop, Skopje, Macedonia, 18 September 2017; pp. 1–12. [Google Scholar]
- Chowdhury, A.K.; Tjondronegoro, D.; Chandran, V.; Zhang, J.; Trost, S.G. Prediction of relative physical activity intensity using multimodal sensing of physiological data. Sensors 2019, 19, 4509. [Google Scholar] [CrossRef] [Green Version]
- Geurkink, Y.; Vandewiele, G.; Lievens, M.; De Turck, F.; Ongenae, F.; Matthys, S.P.; Boone, J.; Bourgois, J.G. Modeling the prediction of the session rating of perceived exertion in soccer: Unraveling the puzzle of predictive indicators. Int. J. Sport. Physiol. Perform. 2019, 14, 841–846. [Google Scholar] [CrossRef]
- Raeder, C.; Wiewelhove, T.; Westphal-Martinez, M.P.; Fernandez-Fernandez, J.; de Paula Simola, R.A.; Kellmann, M.; Meyer, T.; Pfeiffer, M.; Ferrauti, A. Neuromuscular fatigue and physiological responses after five dynamic squat exercise protocols. J. Strength Cond. Res. 2016, 30, 953–965. [Google Scholar] [CrossRef] [Green Version]
- Beato, M.; Maroto-Izquierdo, S.; Hernández-Davó, J.L.; Raya-González, J. Flywheel training periodization in team sports. Front. Physiol. 2021, 12, 732802. [Google Scholar] [CrossRef] [PubMed]
- Maroto-Izquierdo, S.; Raya-González, J.; Hernández-Davó, J.L.; Beato, M. Load Quantification and Testing Using Flywheel Devices in Sports. Front. Physiol. 2021, 12, 739399. [Google Scholar] [CrossRef] [PubMed]
- Cardinal, B.J.; Esters, J.; Cardinal, M.K. Evaluation of the revised physical activity readiness questionnaire in older adults. Med. Sci. Sport. Exerc. 1996, 28 4, 468–472. [Google Scholar] [CrossRef]
- Weakley, J.; Fernández-Valdés, B.; Thomas, L.; Ramirez-Lopez, C.; Jones, B. Criterion validity of force and power outputs for a commonly used flywheel resistance training device and bluetooth app. J. Strength Cond. Res. 2019, 33, 1180–1184. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, M.A.; Whelan, D.F.; Ward, T.E.; Delahunt, E.; Caulfield, B.M. Technology in strength and conditioning: Assessing bodyweight squat technique with wearable sensors. J. Strength Cond. Res. 2017, 31, 2303–2312. [Google Scholar] [CrossRef]
- Lee, J.; Joo, H.; Lee, J.; Chee, Y. Automatic classification of squat posture using inertial sensors: Deep learning approach. Sensors 2020, 20, 361. [Google Scholar] [CrossRef] [Green Version]
- Chromik, J.; Kirsten, K.; Herdick, A.; Kappattanavar, A.M.; Arnrich, B. SensorHub: Multimodal sensing in real-life enables home-based studies. Sensors 2022, 22, 408. [Google Scholar] [CrossRef]
- Camm, A.J.; Malik, M.; Bigger, J.T.; Breithardt, G.; Cerutti, S.; Cohen, R.J.; Coumel, P.; Fallen, E.L.; Kennedy, H.L.; Kleiger, R.E.; et al. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Ann. Noninvasive Electrocardiol. 1996, 1, 151–181. [Google Scholar]
- Ryselis, K.; Petkus, T.; Blažauskas, T.; Maskeliūnas, R.; Damaševičius, R. Multiple Kinect based system to monitor and analyze key performance indicators of physical training. Hum.-Cent. Comput. Inf. Sci. 2020, 10, 51. [Google Scholar] [CrossRef]
- Kotsifaki, A.; Whiteley, R.; Hansen, C. Dual Kinect v2 system can capture lower limb kinematics reasonably well in a clinical setting: Concurrent validity of a dual camera markerless motion capture system in professional football players. BMJ Open Sport Exerc. Med. 2018, 4, e000441. [Google Scholar] [CrossRef] [Green Version]
- Albert, J.A.; Owolabi, V.; Gebel, A.; Brahms, C.M.; Granacher, U.; Arnrich, B. Evaluation of the pose tracking performance of the azure kinect and kinect v2 for gait analysis in comparison with a gold standard: A pilot study. Sensors 2020, 20, 5104. [Google Scholar] [CrossRef] [PubMed]
- Xing, Q.J.; Shen, Y.Y.; Cao, R.; Zong, S.X.; Zhao, S.X.; Shen, Y.F. Functional movement screen dataset collected with two azure kinect depth sensors. Sci. Data 2022, 9, 104. [Google Scholar] [CrossRef] [PubMed]
- Faude, O.; Kindermann, W.; Meyer, T. Lactate threshold concepts. Sport. Med. 2009, 39, 469–490. [Google Scholar] [CrossRef] [PubMed]
- Tarvainen, M.P.; Niskanen, J.P.; Lipponen, J.A.; Ranta-Aho, P.O.; Karjalainen, P.A. Kubios HRV–heart rate variability analysis software. Comput. Methods Programs Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef]
- Morton, R.H.; Fitz-Clarke, J.R.; Banister, E.W. Modeling human performance in running. J. Appl. Physiol. 1990, 69, 1171–1177. [Google Scholar] [CrossRef]
- Albert, J.A.; Herdick, A.; Brahms, C.M.; Granacher, U.; Arnrich, B. Using Machine Learning to Predict Perceived Exertion During Resistance Training With Wearable Heart Rate and Movement Sensors. In Proceedings of the 2021 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Houston, TX, USA, 9–12 December 2021; pp. 801–808. [Google Scholar]
- Antico, M.; Balletti, N.; Laudato, G.; Lazich, A.; Notarantonio, M.; Oliveto, R.; Ricciardi, S.; Scalabrino, S.; Simeone, J. Postural control assessment via Microsoft Azure Kinect DK: An evaluation study. Comput. Methods Programs Biomed. 2021, 209, 106324. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author et al. | Study Cohort | Sensors | Study Protocol | RPE Scale | PA |
|---|---|---|---|---|---|
| Pernek 2015 [6] | 11 subjects (3 female, 8 male) | IMU | 6 upper body exercises, 10 repetitions of each exercise, repeated with 4 different weights | Classic Borg scale, ranging from 6–20, individually normalized into the interval | No |
| Carey 2016 [7] | 45 Australian football players | HR, GPS, IMU | Training session of American football | Borg CR-10 scale, ranging from 1–10 | No |
| Vandewiele 2017 [8] | 45 Belgian soccer players | HR, GPS, IMU | Multiple soccer training sessions | Borg CR-10 scale, ranging from 1–10 | No |
| Chowdhury 2019 [9] | 22 subjects (17 male, 5 female) | HR, EDA, skin temperature | Physical activity protocol consisting of quiet sitting or standing, comfortable walking, brisk walking, jogging, fast running | Classic Borg scale, ranging from 6–20, intensity divided into three classes, i.e., low: , moderate: , and high: | On request |
| Geurkink 2019 [10] | 46 Belgian soccer players | HR, GPS | 61 soccer training sessions | Custom RPE scale, ranging from 1–10 | No |
| Davidson 2020 [4] | 12 male subjects | HR, GPS, peak | Running until exhaustion (parkour of 5 km and 2 km for trained, untrained, respectively | Classic Borg scale, ranging from 6–20, intensity divided into two classes, i.e., medium: , high: | No |
| Jiang 2021 [5] | 14 subjects (12 male, 2 female) | IMU, MoCap, force plates | Physical exercise protocol, three exercises (squat, high knee jack, and corkscrew toe-touch), five repetitions per set until exhaustion | Custom RPE scale, ranging from 1–10 | No |
| This study | 12 male subjects | IMU, HRV, MoCap, Flywheel energy | Flywheel squat exercise protocol, 12 sets with 12 repetitions each | Classic Borg scale, ranging from 6–20 | Yes |
| Minimum | Mean ± SD | Maximum | |
|---|---|---|---|
| Age (y) | 19.9 | 23.3 ± 2.9 | 29.1 |
| Body mass (kg) | 75.0 | 82.6 ± 4.8 | 90.0 |
| Height (cm) | 174.0 | 183.8 ± 5.3 | 192.0 |
| Training experience (y) | 1.0 | 3.7 ± 2.3 | 10.0 |
| Workouts per week | 2 | 3.4 ± 1.3 | 6 |
| Training duration (m) | 50.0 | 75.0 ± 19.8 | 120.0 |
| Workouts per week since COVID | 0 | 2.7 ± 1.5 | 6 |
| Training duration since COVID (m) | 0.0 | 60.4 ± 33.3 | 120.0 |
| Category | Parameters |
|---|---|
| Overview | Artifacts [%] |
| Time Domain | Mean RR [ms], SD RR [ms], Mean HR [1/min], SD HR [1/min], Min HR [1/min], Max HR [1/min], RMSSD [ms], NN50, pNN50 [%], HRVti, TINN [ms], Intensity (TRIMP/min), Load (TRIMP) |
| Frequency Domain | VLF Peak [Hz], LF peak [Hz], HF peak [Hz], VLF power [ms], LF power [ms], HF Power [ms], VLF power [log], LF power [log], HF Power [log], VLF power [%], LF power [%], HF Power [%], LF/HF ratio, EDR [Hz] |
| Nonlinear Domain | SD1 [ms], SD2 [ms], SD2/SD1 |
| MAPE (%) | MSE | RMSE | ||||||
|---|---|---|---|---|---|---|---|---|
| Model | IMU | IMU + HRV | IMU | IMU+HRV | IMU | IMU + HRV | IMU | IMU + HRV |
| GBRT | ± | ± | ± | ± | ± | |||
| SVRL | ± | ± | ± | ± | ± | ± | ± | ± |
| SVRR | ± | ± | ± | ± | ± | ± | ± | ± |
| RF | ± | ± | ± | ± | ± | ± | ± | |
| Feature | Modality | Rank |
|---|---|---|
| Load (TRIMP) | HRV | 1 |
| Thigh, Left GX, Max. | IMU | 2 |
| Tibia, Right GX, Min. | IMU | 3 |
| Tibia, Right GZ, Min. | IMU | 4 |
| Tibia, Right AX, Skewness | IMU | 5 |
| Thigh, Left GX, Mean | IMU | 6 |
| Thigh, Left GX, Med. | IMU | 7 |
| Tibia, Right GX, Max. | IMU | 8 |
| Tibia, Right GZ, Max. | IMU | 9 |
| Tibia, Right AZ, Min. | IMU | 10 |
| Intensity (TRIMP/min) | HRV | 11 |
| Thigh, Right AZ, Min. | IMU | 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albert, J.A.; Herdick, A.; Brahms, C.M.; Granacher, U.; Arnrich, B. PERSIST: A Multimodal Dataset for the Prediction of Perceived Exertion during Resistance Training. Data 2023, 8, 9. https://doi.org/10.3390/data8010009
Albert JA, Herdick A, Brahms CM, Granacher U, Arnrich B. PERSIST: A Multimodal Dataset for the Prediction of Perceived Exertion during Resistance Training. Data. 2023; 8(1):9. https://doi.org/10.3390/data8010009
Chicago/Turabian StyleAlbert, Justin Amadeus, Arne Herdick, Clemens Markus Brahms, Urs Granacher, and Bert Arnrich. 2023. "PERSIST: A Multimodal Dataset for the Prediction of Perceived Exertion during Resistance Training" Data 8, no. 1: 9. https://doi.org/10.3390/data8010009