Current Understanding of the Biomechanics of Ventricular Tissues in Heart Failure


Abstract
:1. Introduction
2. Characterization of the Mechanical Behavior of Ventricles
2.1. Ex Vivo Measurements
2.1.1. Preconditioning and Residual Stress Measurement
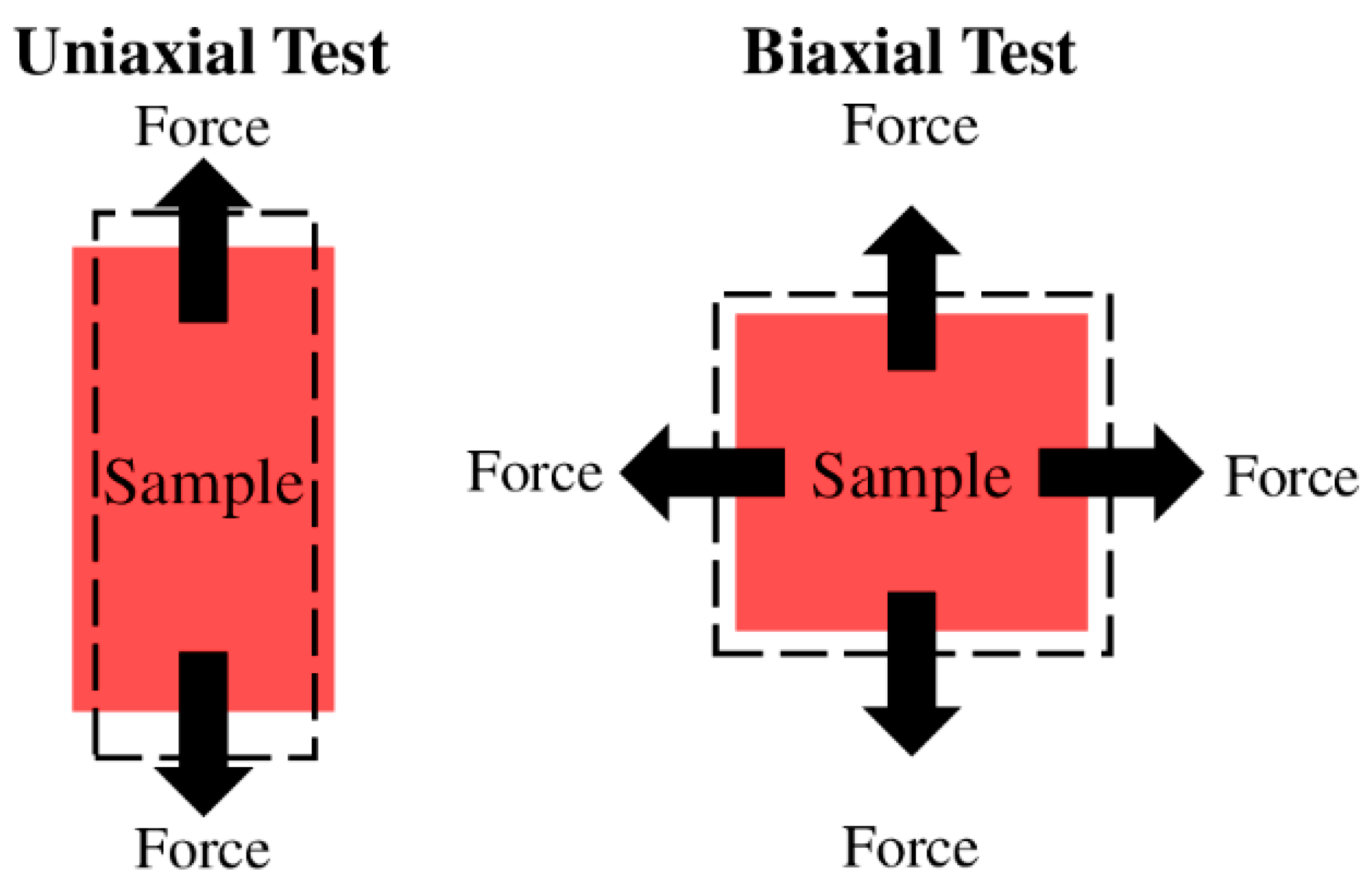
2.1.2. Uniaxial and Biaxial Tensile Mechanical Tests
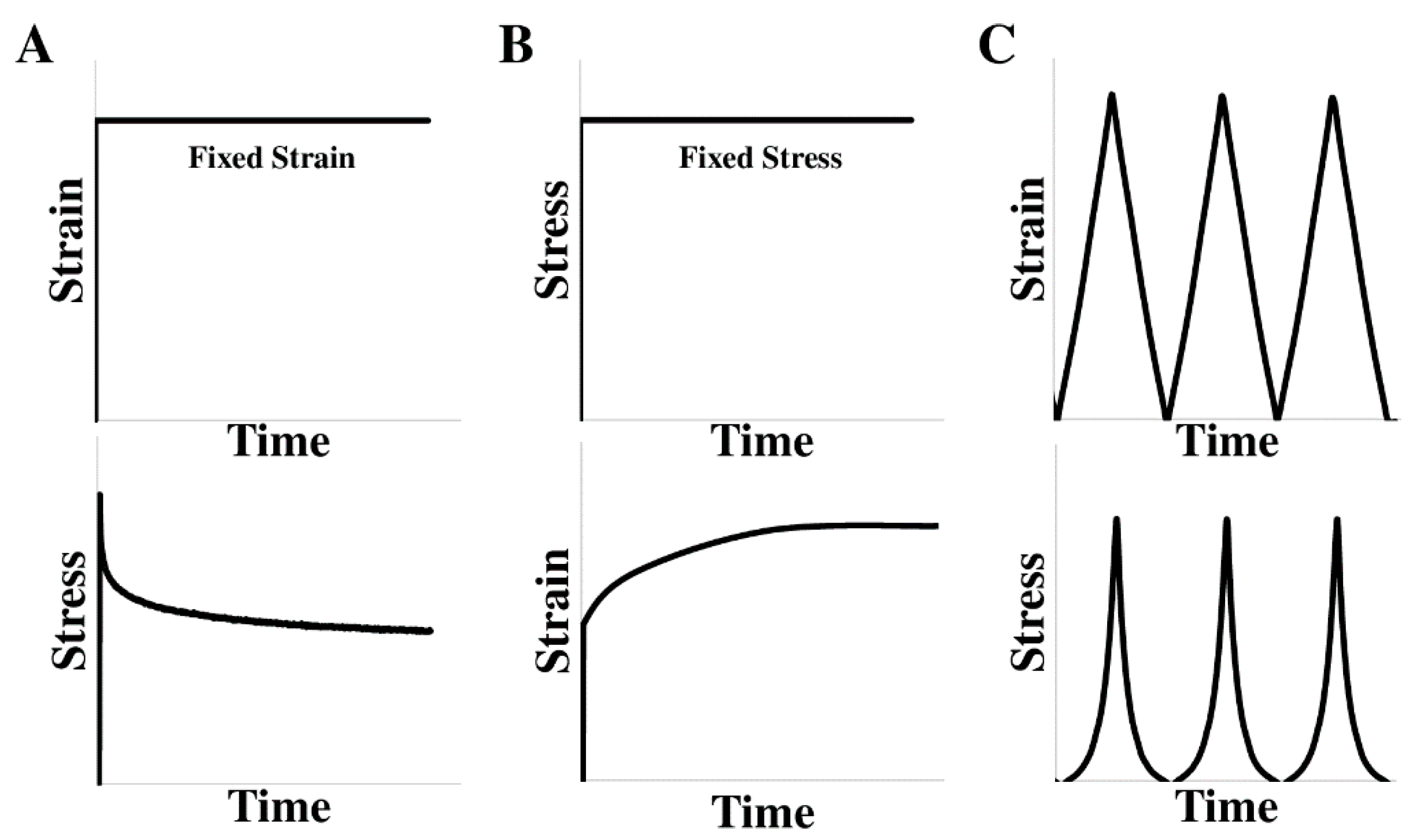
2.1.3. Stress Relaxation and Creep Tests
2.2. In Vivo Measurements
2.2.1. The Elasticity Measurement
2.2.2. The Viscoelasticity Measurement
2.3. Basic Behavior of Ventricles—Tissue with Anisotropy and Viscoelasticity
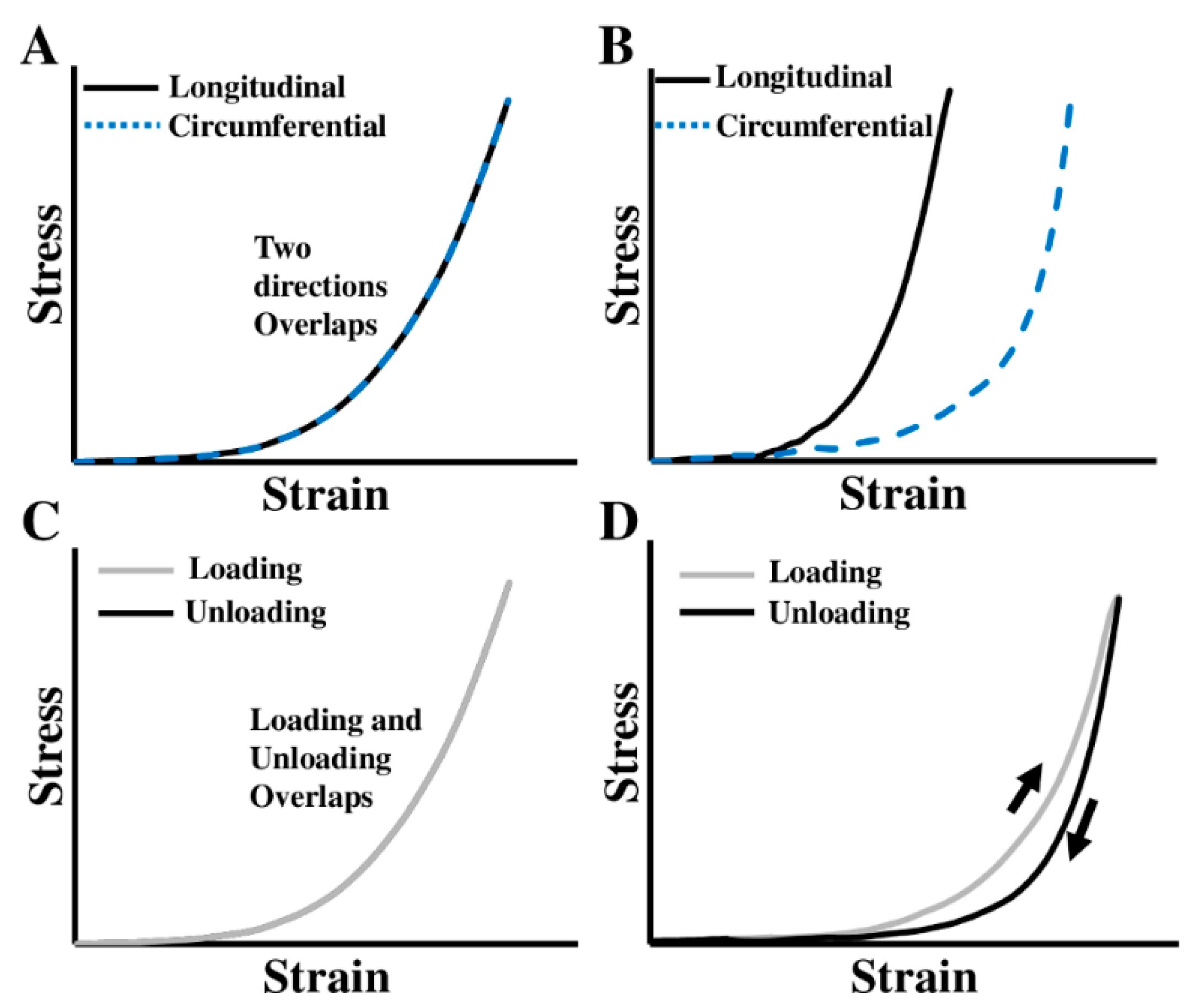
2.3.1. Anisotropic Behavior of Ventricles
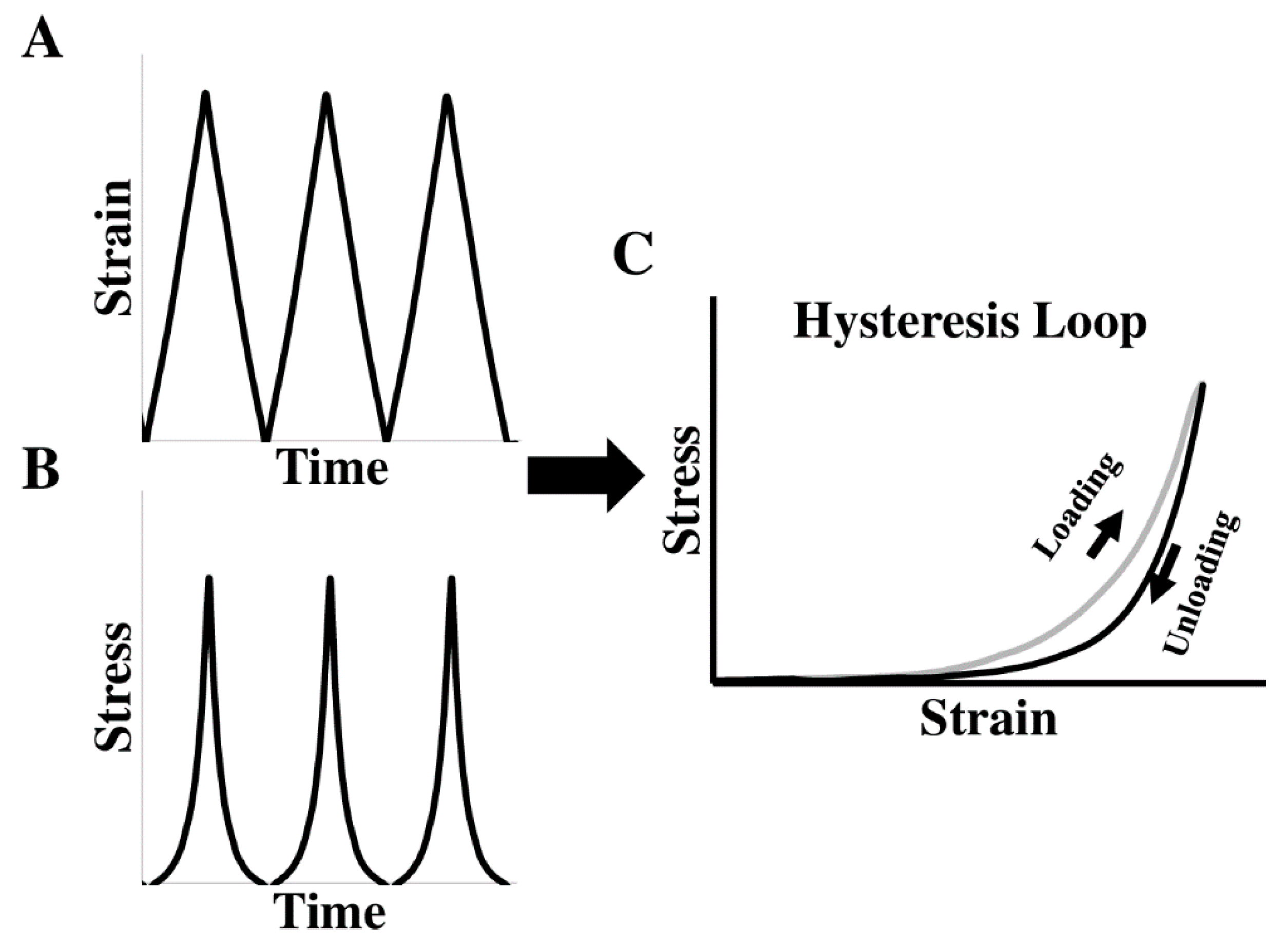
2.3.2. Viscoelastic Behavior of Ventricles
2.4. Computational Modeling of Ventricular Biomechanics
3. Biomechanical Changes of Ventricles in Heart Failure Development
4. Clinical Relevance of Ventricular Mechanical Alterations
4.1. Significance of Ventricular Stiffening in Heart Failure
4.2. Significance of Altered Ventricular Viscoelasticity in Heart Failure
5. Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Wayne, R.; Katherine, F.; Karen, F.; Alan, G.; Kurt, G.; Nancy, H.; Susan, M.H.; Michael, H.; Virginia, H.; Brett, K.; et al. Heart Disease and Stroke Statistics—2008 Update. Circulation 2008, 117, e25–e146. [Google Scholar]
- Douglas, D.S.; Emelia, J.B.; Gregg, C.F.; Harlan, M.K.; Daniel, L.; George, A.M.; Jagat, N.; Eileen, S.S.; James, B.Y.; Yuling, H. Prevention of Heart Failure. Circulation 2008, 117, 2544–2565. [Google Scholar]
- Lloyd-Jones, D.M.; Larson, M.G.; Leip, E.P.; Beiser, A.; D’Agostino, R.B.; Kannel, W.B.; Murabito, J.M.; Vasan, R.S.; Benjamin, E.J.; Levy, D. Lifetime Risk for Developing Congestive Heart Failure. Circulation 2002, 106, 3068–3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, K.K.L.; Pinsky, J.L.; Kannel, W.B.; Levy, D. The epidemiology of heart failure: The Framingham Study. J. Am. Coll. Cardiol. 1993, 22, A6–A13. [Google Scholar] [CrossRef] [Green Version]
- Schocken, D.D.; Arrieta, M.I.; Leaverton, P.E.; Ross, E.A. Prevalence and mortality rate of congestive heart failure in the United States. J. Am. Coll. Cardiol. 1992, 20, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Levy, D.; Kenchaiah, S.; Larson, M.G.; Benjamin, E.J.; Kupka, M.J.; Ho, K.K.L.; Murabito, J.M.; Vasan, R.S. Long-Term Trends in the Incidence of and Survival with Heart Failure. N. Engl. J. Med. 2002, 347, 1397–1402. [Google Scholar] [CrossRef] [PubMed]
- Yancy Clyde, W.; Mariell, J.; Biykem, B.; Javed, B.; Casey Donald, E.; Drazner Mark, H.; Fonarow Gregg, C.; Geraci Stephen, A.; Tamara, H.; Januzzi James, L.; et al. ACCF/AHA Guideline for the Management of Heart Failure. Circulation 2013, 128, e240–e327. [Google Scholar]
- Dhingra, A.; Garg, A.; Kaur, S.; Chopra, S.; Batra, J.S.; Pandey, A.; Chaanine, A.H.; Agarwal, S.K. Epidemiology of Heart Failure with Preserved Ejection Fraction. Curr. Heart Fail. Rep. 2014, 11, 354–365. [Google Scholar] [CrossRef]
- Owan, T.E.; Hodge, D.O.; Herges, R.M.; Jacobsen, S.J.; Roger, V.L.; Redfield, M.M. Trends in Prevalence and Outcome of Heart Failure with Preserved Ejection Fraction. N. Engl. J. Med. 2006, 355, 251–259. [Google Scholar] [CrossRef] [Green Version]
- Konstam, M.A.; Kiernan, M.S.; Bernstein, D.; Bozkurt, B.; Jacob, M.; Kapur, N.K.; Kociol, R.D.; Lewis, E.F.; Mehra, M.R.; Pagani, F.D.; et al. On behalf of the American Heart Association Coun-cil on Clinical Cardiology; Council on Cardiovas-cular Disease in the Young; and Council on Cardiovascular Surgery and Anesthesia. Circulation 2018, 137, 578–622. [Google Scholar]
- Lahm, T.; Douglas, I.S.; Archer, S.L.; Bogaard, H.J.; Chesler, N.C.; Haddad, F.; Hemnes, A.R.; Kawut, S.M.; Kline, J.A.; Kolb, T.M.; et al. Assessment of right ventricular function in the research setting: Knowledge gaps and pathways forward an official American thoracic society research statement. Am. J. Respir. Crit. Care Med. 2018, 198, e15–e43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Köhler, D.; Arnold, R.; Loukanov, T.; Gorenflo, M. Right Ventricular Failure and Pathobiology in Patients with Congenital Heart Disease—Implications for Long-Term Follow-Up. Front. Pediatr. 2013, 1, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddad, F.; Hunt, S.A.; Rosenthal, D.N.; Murphy, D.J. Right ventricular function in cardiovascular disease, part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation 2008, 117, 1436–1448. [Google Scholar] [CrossRef] [PubMed]
- Voelkel, N.F.; Quaife, R.A.; Leinwand, L.A.; Barst, R.J.; Mcgoon, M.D.; Meldrum, D.R.; Dupuis, J.; Long, C.S.; Rubin, L.J.; Smart, F.W.; et al. Right Ventricular Function and Failure Report of a National Heart, Lung, and Blood Institute Working Group on Cellular and Molecular Mechanisms of Right Heart Failure The Normal Right Ventricle The Right Ventricle in Pulmonary Hypertension Special Report. Circulation 2006, 114, 1883–1891. [Google Scholar] [CrossRef] [Green Version]
- Golob, M.; Moss, R.L.; Chesler, N.C. Cardiac tissue structure, properties, and performance: A materials science perspective. Ann. Biomed. Eng. 2014, 42, 2003–2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellofiore, A.; Chesler, N.C. Methods for measuring right ventricular function and hemodynamic coupling with the pulmonary vasculature. Ann. Biomed. Eng. 2013, 41, 1384–1398. [Google Scholar] [CrossRef] [Green Version]
- Sacks, M.S.; Chuong, C.J. Biaxial Mechanical Properties of Passive Right Ventricular Free Wall Myocardium. J. Biomech. Eng. 1993, 115, 202–205. [Google Scholar] [CrossRef]
- Wang, Z.; Golob, M.J.; Chesler, N.C. Viscoelastic Properties of Cardiovascular Tissues. In Viscoelastic and Viscoplastic Materials; Golob, M.J., Ed.; IntechOpen: Rijeka, Croatia, 2016; p. 7. ISBN 978-953-51-2603-4. [Google Scholar]
- Nguyen-Truong, M.; Wang, Z. Biomechanical properties and mechanobiology of cardiac ECM. In Advances in Experimental Medicine and Biology; Springer: Cham, Switzerland, 2018; Volume 1098, pp. 1–19. [Google Scholar]
- Jang, S.; Vanderpool, R.R.; Avazmohammadi, R.; Lapshin, E.; Bachman, T.N.; Sacks, M.; Simon, M.A. Biomechanical and Hemodynamic Measures of Right Ventricular Diastolic Function: Translating Tissue Biomechanics to Clinical Relevance. J. Am. Hear. Assoc. Cardiovasc. Cerebrovasc. Dis. 2017, 6, e006084. [Google Scholar] [CrossRef] [Green Version]
- Fung, Y.C.; Fronek, K.; Patitucci, P. Pseudoelasticity of arteries and the choice of its mathematical expression. Am. J. Physiol. Circ. Physiol. 1979, 237, H620–H631. [Google Scholar] [CrossRef]
- Ghaemi, H.; Behdinan, K.; Spence, A.D. In vitro technique in estimation of passive mechanical properties of bovine heart: Part I. Experimental techniques and data. Med. Eng. Phys. 2009, 31, 76–82. [Google Scholar] [CrossRef]
- Sommer, G.; Schriefl, A.J.; Andrä, M.; Sacherer, M.; Viertler, C.; Wolinski, H.; Holzapfel, G.A. Biomechanical properties and microstructure of human ventricular myocardium. Acta Biomater. 2015, 24, 172–192. [Google Scholar] [CrossRef] [PubMed]
- Yin, F.C.P.; Strumpf, R.K.; Chew, P.H.; Zeger, S.L. Quantification of the mechanical properties of noncontracting canine myocardium under simultaneous biaxial loading. J. Biomech. 1987, 20, 577–589. [Google Scholar] [CrossRef]
- Humphrey, J.D.; Strumpf, R.K.; Yin, F.C.P. Determination of a Constitutive Relation for Passive Myocardium: I. A New Functional Form. J. Biomech. Eng. 1990, 112, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Novak, V.P.; Yin, F.C.P.; Humphrey, J.D. Regional mechanical properties of passive myocardium. J. Biomech. 1994, 27, 403–412. [Google Scholar] [CrossRef]
- Lin, D.H.S.; Yin, F.C.P. A Multiaxial Constitutive Law for Mammalian Left Ventricular Myocardium in Steady-State Barium Contracture or Tetanus. J. Biomech. Eng. 1998, 120, 504–517. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.B.; Ratcliffe, M.B.; Fallert, M.A.; Edmunds, L.H.; Bogen, D.K. Changes in passive mechanical stiffness of myocardial tissue with aneurysm formation. Circulation 1994, 89, 2315–2326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valdez-Jasso, D.; Simon, M.A.; Champion, H.C.; Sacks, M.S. A murine experimental model for the mechanical behaviour of viable right-ventricular myocardium. J. Physiol. 2012, 590, 4571–4584. [Google Scholar] [CrossRef]
- Fatemifar, F.; Feldman, M.D.; Oglesby, M.; Han, H.-C. Comparison of Biomechanical Properties and Microstructure of Trabeculae Carneae, Papillary Muscles, and Myocardium in the Human Heart. J. Biomech. Eng. 2018, 141, 021007. [Google Scholar] [CrossRef]
- Ooi, C.Y.; Wang, Z.; Tabima, D.M.; Eickhoff, J.C.; Chesler, N.C. The role of collagen in extralobar pulmonary artery stiffening in response to hypoxia-induced pulmonary hypertension. Am. J. Physiol. Circ. Physiol. 2010, 299, H1823–H1831. [Google Scholar] [CrossRef] [Green Version]
- Lakes, R.S. Viscoelastic Solids; CRC Press Revivals; CRC Press: Boca Raton, FL, USA, 1998; ISBN 9781351355650. [Google Scholar]
- Fung, Y.C. What are the residual stresses doing in our blood vessels? Ann. Biomed. Eng. 1991, 19, 237–249. [Google Scholar] [CrossRef]
- Shi, X.; Liu, Y.; Copeland, K.M.; McMahan, S.R.; Zhang, S.; Butler, J.R.; Hong, Y.; Cho, M.; Bajona, P.; Gao, H. Epicardial prestrained confinement and residual stresses: A newly observed heart ventricle confinement interface. J. R. Soc. Interface 2019, 16, 20190028. [Google Scholar] [CrossRef] [PubMed]
- Omens, J.H.; Fung, Y.C. Residual strain in rat left ventricle. Circ. Res. 1990, 66, 37–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genet, M.; Rausch, M.K.; Lee, L.C.; Choy, S.; Zhao, X.; Kassab, G.S.; Kozerke, S.; Guccione, J.M.; Kuhl, E. Heterogeneous growth-induced prestrain in the heart. J. Biomech. 2015, 48, 2080–2089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jöbsis, P.D.; Ashikaga, H.; Wen, H.; Rothstein, E.C.; Horvath, K.A.; McVeigh, E.R.; Balaban, R.S. The visceral pericardium: Macromolecular structure and contribution to passive mechanical properties of the left ventricle. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H3379–H3387. [Google Scholar] [CrossRef] [Green Version]
- Hoskins, P.R.; Lawford, P.V.; Doyle, B.J. Cardiovascular Biomechanics. Cardiovasc. Biomech. 2017, 1–462. [Google Scholar]
- Demer, L.L.; Yin, F.C. Passive biaxial mechanical properties of isolated canine myocardium. J. Physiol. 1983, 339, 615–630. [Google Scholar] [CrossRef]
- Hill, M.R.; Simon, M.A.; Valdez-Jasso, D.; Zhang, W.; Champion, H.C.; Sacks, M.S. Structural and Mechanical Adaptations of Right Ventricular Free Wall Myocardium to Pulmonary-Hypertension Induced Pressure Overload. Ann. Biomed. Eng. 2014, 42, 2451–2465. [Google Scholar] [CrossRef] [Green Version]
- Sacks, M. Biaxial Mechanical Evaluation of Planar Biological Materials. J. Elast. Phys. Sci. Solids 2000, 61, 199. [Google Scholar]
- Holzapfel, G.A.; Ogden, R.W. Constitutive modelling of passive myocardium: A structurally based framework for material characterization. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2009, 367, 3445–3475. [Google Scholar] [CrossRef]
- Humphrey, J.D.; Strumpf, R.K.; Yin, F.C. Biaxial mechanical behavior of excised ventricular epicardium. Am. J. Physiol. Circ. Physiol. 1990, 259, H101–H108. [Google Scholar] [CrossRef]
- Javani, S.; Gordon, M.; Azadani, A.N. Biomechanical Properties and Microstructure of Heart Chambers: A Paired Comparison Study in an Ovine Model. Ann. Biomed. Eng. 2016, 44, 3266–3283. [Google Scholar] [CrossRef] [PubMed]
- Sirry, M.S.; Butler, J.R.; Patnaik, S.S.; Brazile, B.; Bertucci, R.; Claude, A.; McLaughlin, R.; Davies, N.H.; Liao, J.; Franz, T. Characterisation of the mechanical properties of infarcted myocardium in the rat under biaxial tension and uniaxial compression. J. Mech. Behav. Biomed. Mater. 2016, 63, 252–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, F.; Prabhu, R.J.; Liao, J.; Soe, S.; Jones, M.D.; Miller, J.; Berthelson, P.; Enge, D.; Copeland, K.M.; Shaabeth, S.; et al. Biomechanical properties and microstructure of neonatal porcine ventricles. J. Mech. Behav. Biomed. Mater. 2018, 88, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Ramo, N.L.; Troyer, K.L.; Puttlitz, C.M. Viscoelasticity of spinal cord and meningeal tissues. Acta Biomater. 2018, 75, 253–262. [Google Scholar] [CrossRef]
- Ramo, N.L.; Puttlitz, C.M.; Troyer, K.L. The development and validation of a numerical integration method for non-linear viscoelastic modeling. PLoS ONE 2018, 13, e0190137. [Google Scholar] [CrossRef] [Green Version]
- Ramo, N.L.; Lee, J.H.T.; Troyer, K.L.; Kwon, B.K.; Puttlitz, C.M.; Cripton, P.; Streijger, F.; Shetye, S.S. Comparison of in vivo and ex vivo viscoelastic behavior of the spinal cord. Acta Biomater. 2017, 68, 78–89. [Google Scholar] [CrossRef]
- Troyer, K.L.; Puttlitz, C.M. Nonlinear viscoelasticty plays an essential role in the functional behavior of spinal ligaments. J. Biomech. 2012, 45, 684–691. [Google Scholar] [CrossRef]
- Troyer, K.L.; Estep, D.J.; Puttlitz, C.M. Viscoelastic effects during loading play an integral role in soft tissue mechanics. Acta Biomater. 2012, 8, 234–243. [Google Scholar] [CrossRef]
- Stella, J.A.; Liao, J.; Sacks, M.S. Time-dependent biaxial mechanical behavior of the aortic heart valve leaflet. J. Biomech. 2007, 40, 3169–3177. [Google Scholar] [CrossRef] [Green Version]
- Liao, J.; Yang, L.; Grashow, J.; Sacks, M.S. The Relation Between Collagen Fibril Kinematics and Mechanical Properties in the Mitral Valve Anterior Leaflet. J. Biomech. Eng. 2006, 129, 78–87. [Google Scholar] [CrossRef]
- Little, R.; Wead, W. Diastolic viscoelastic properties of active and quiescent cardiac muscle. Am. J. Physiol. Content 1971, 221, 1120–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsaturyan, A.K.; Izacov, V.J.; Zhelamsky, S.V.; Bykov, B.L. Extracellular fluid filtration as the reason for the viscoelastic behaviour of the passive myocardium. J. Biomech. 1984, 17, 749–755. [Google Scholar] [CrossRef]
- Miller, C.E.; Vanni, M.A.; Keller, B.B. Characterization of passive embryonic myocardium by quasi-linear viscoelasticity theory. J. Biomech. 1997, 30, 985–988. [Google Scholar] [CrossRef]
- Miller, C.E.; Wong, C.L. Trabeculated embryonic myocardium shows rapid stress relaxation and non-quasi-linear viscoelastic behavior. J. Biomech. 2000, 33, 615–622. [Google Scholar] [CrossRef]
- Loeffler, L.; Sagawa, K. A one dimensional viscoelastic model of cat heart muscle studied by small length perturbations during isometric contraction. Circ. Res. 1975, 36, 498–512. [Google Scholar] [CrossRef] [Green Version]
- Faconti, L.; Bruno, R.M.; Ghiadoni, L.; Virdis, S.; Virdis, A. Ventricular and Vascular Stiffening in Aging and Hypertension. Curr. Hypertens. Rev. 2015, 11, 100–109. [Google Scholar] [CrossRef]
- Borlaug, B.A.; Redfield, M.M.; Melenovsky, V.; Kane, G.C.; Karon, B.L.; Jacobsen, S.J.; Rodeheffer, R.J. Longitudinal changes in left ventricular stiffness: A community-based study. Circ. Heart Fail. 2013, 6, 944–952. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Schreier, D.A.; Hacker, T.A.; Chesler, N.C. Progressive right ventricular functional and structural changes in a mouse model of pulmonary arterial hypertension. Physiol. Rep. 2013, 1, e00184. [Google Scholar] [CrossRef]
- Wang, Z.; Chesler, N.C. Pulmonary vascular mechanics: Important contributors to the increased right ventricular afterload of pulmonary hypertension. Exp. Physiol. 2013, 98, 1267–1273. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Chesler, N.C. Pulmonary Vascular Wall Stiffness: An Important Contributor to the Increased Right Ventricular Afterload with Pulmonary Hypertension. Pulm. Circ. 2011, 1, 212–223. [Google Scholar] [CrossRef] [Green Version]
- Tabima, D.M.; Philip, J.L.; Chesler, N.C. Right ventricular-pulmonary vascular interactions. Physiology 2017, 32, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, E.-S.H. Myocardial tagging by Cardiovascular Magnetic Resonance: Evolution of techniques–pulse sequences, analysis algorithms, and applications. J. Cardiovasc. Magn. Reson. 2011, 13, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, Y.; Ishizu, T.; Aonuma, K. Current status of 3-dimensional speckle tracking echocardiography: A review from our experiences. J. Cardiovasc. Ultrasound 2014, 22, 49–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voigt, J.-U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Hear. J. Cardiovasc. Imaging 2014, 16, 1–11. [Google Scholar]
- Bossone, E.; D’Andrea, A.; D’Alto, M.; Citro, R.; Argiento, P.; Ferrara, F.; Cittadini, A.; Rubenfire, M.; Naeije, R. Echocardiography in Pulmonary Arterial Hypertension: From Diagnosis to Prognosis. J. Am. Soc. Echocardiogr. 2013, 26, 1–14. [Google Scholar] [CrossRef]
- Leng, S.; Jiang, M.; Zhao, X.-D.; Allen, J.C.; Kassab, G.S.; Ouyang, R.-Z.; Tan, J.-L.; He, B.; Tan, R.-S.; Zhong, L. Three-Dimensional Tricuspid Annular Motion Analysis from Cardiac Magnetic Resonance Feature-Tracking. Ann. Biomed. Eng. 2016, 44, 3522–3538. [Google Scholar] [CrossRef]
- Zou, H.; Xi, C.; Zhao, X.; Koh, A.S.; Gao, F.; Su, Y.; Tan, R.-S.; Allen, J.; Lee, L.C.; Genet, M.; et al. Quantification of Biventricular Strains in Heart Failure With Preserved Ejection Fraction Patient Using Hyperelastic Warping Method. Front. Physiol. 2018, 9, 1295. [Google Scholar] [CrossRef]
- Genet, M.; Stoeck, C.; von Deuster, C.; Chuan Lee, L.; Guccione, J.; Kozerke, S. Finite Element Digital Image Correlation for Cardiac Strain Analysis from 3D Whole-Heart Tagging. In Proceedings of the ISMRM 24rd Annual Meeting and Exhibition, Singapore, 7–13 May 2016. [Google Scholar]
- Genet, M.; Stoeck, C.T.; von Deuster, C.; Lee, L.C.; Kozerke, S. Equilibrated warping: Finite element image registration with finite strain equilibrium gap regularization. Med. Image Anal. 2018, 50, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Phatak, N.S.; Maas, S.A.; Veress, A.I.; Pack, N.A.; Di Bella, E.V.R.; Weiss, J.A. Strain measurement in the left ventricle during systole with deformable image registration. Med. Image Anal. 2009, 13, 354–361. [Google Scholar] [CrossRef]
- Finsberg, H.N.T.; Sundnes, J.S.; Xi, C.; Lee, L.C.; Zhao, X.; Tan, J.L.; Genet, M.; Zhong, L.; Wall, S.T. Computational quantification of patient specific changes in ventricular dynamics associated with pulmonary hypertension. Am. J. Physiol. Heart Circ. Physiol. 2019, 317, H1363–H1375. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Fakhouri, F.; Majeed, W.; Kolipaka, A. Cardiovascular magnetic resonance elastography: A review. NMR Biomed. 2018, 31, e3853. [Google Scholar] [CrossRef] [PubMed]
- Arani, A.; Arunachalam, S.P.; Chang, I.C.Y.; Baffour, F.; Rossman, P.J.; Glaser, K.J.; Trzasko, J.D.; McGee, K.P.; Manduca, A.; Grogan, M.; et al. Cardiac MR elastography for quantitative assessment of elevated myocardial stiffness in cardiac amyloidosis. J. Magn. Reson. Imaging 2017, 46, 1361–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, L.; Yao, J.; Yang, C.; Tang, D.; Xu, D. Infarcted Left Ventricles Have Stiffer Material Properties and Lower Stiffness Variation: Three-Dimensional Echo-Based Modeling to Quantify In Vivo Ventricle Material Properties. J. Biomech. Eng. 2015, 137, 81005. [Google Scholar] [CrossRef] [Green Version]
- Mojsejenko, D.; McGarvey, J.R.; Dorsey, S.M.; Gorman, J.H., 3rd; Burdick, J.A.; Pilla, J.J.; Gorman, R.C.; Wenk, J.F. Estimating passive mechanical properties in a myocardial infarction using MRI and finite element simulations. Biomech. Model. Mechanobiol. 2015, 14, 633–647. [Google Scholar] [CrossRef] [Green Version]
- Tang, D.; Yang, C.; Geva, T.; Del Nido, P.J. Patient-specific MRI-based 3D FSI RV/LV/patch models for pulmonary valve replacement surgery and patch optimization. J. Biomech. Eng. 2008, 130, 41010. [Google Scholar] [CrossRef] [Green Version]
- Acosta, S.; Puelz, C.; Rivière, B.; Penny, D.J.; Brady, K.M.; Rusin, C.G. Cardiovascular mechanics in the early stages of pulmonary hypertension: A computational study. Biomech. Model. Mechanobiol. 2017, 16, 2093–2112. [Google Scholar] [CrossRef]
- Avazmohammadi, R.; Mendiola, E.A.; Soares, J.S.; Li, D.S.; Chen, Z.; Merchant, S.; Hsu, E.W.; Vanderslice, P.; Dixon, R.A.F.; Sacks, M.S. A Computational Cardiac Model for the Adaptation to Pulmonary Arterial Hypertension in the Rat. Ann. Biomed. Eng. 2019, 47, 138–153. [Google Scholar] [CrossRef]
- Xi, C.; Latnie, C.; Zhao, X.; Tan, J.L.; Wall, S.T.; Genet, M.; Zhong, L.; Lee, L.C. Patient-Specific Computational Analysis of Ventricular Mechanics in Pulmonary Arterial Hypertension. J. Biomech. Eng. 2016, 138, 111001. [Google Scholar] [CrossRef]
- Humphrey, J.D. Cardiovascular Solid Mechanics: Cells, Tissues, and Organs; Springer: New York, NY, USA, 2002; ISBN 0387951687. [Google Scholar]
- Fan, R.; Tang, D.; Yao, J.; Yang, C.; Xu, D. 3D Echo-Based Patient-Specific Computational Left Ventricle Models to Quantify Material Properties and Stress/Strain Differences between Ventricles with and without Infarct. Comput. Model. Eng. Sci. 2014, 99, 491–508. [Google Scholar]
- Hassaballah, A.I.; Hassan, M.A.; Mardi, A.N.; Hamdi, M. An inverse finite element method for determining the tissue compressibility of human left ventricular wall during the cardiac cycle. PLoS ONE 2013, 8, e82703. [Google Scholar] [CrossRef] [PubMed]
- Hess, O.M.; Grimm, J.; Krayenbuehl, H.P. Diastolic simple elastic and viscoelastic properties of the left ventricle in man. Circulation 1979, 59, 1178–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hess, O.M.; Schneider, J.; Koch, R.; Bamert, C.; Grimm, J.; Krayenbuehl, H.P. Diastolic function and myocardial structure in patients with myocardial hypertrophy. Special reference to normalized viscoelastic data. Circulation 1981, 63, 360–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pouleur, H.; Karliner, J.S.; Lewinter, M.M.; Covell, J.W. Diastolic viscous properties of the intact canine left ventricle. Circ. Res. 1979, 67, 352–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, F.; Soe, S.; White, N.; Johnston, R.; Khan, I.; Liao, J.; Jones, M.; Prabhu, R.; Maconochie, I.; Theobald, P. Region-Specific Microstructure in the Neonatal Ventricles of a Porcine Model. Ann. Biomed. Eng. 2018, 46, 2162–2176. [Google Scholar] [CrossRef] [Green Version]
- Dokos, S.; Smaill, B.H.; Young, A.A.; Legrice, I.J.; Legrice, I.J. Shear properties of passive ventricular myocardium. Am. J. Physiol. Hear. Circ. Physiol. 2002, 283, 2650–2659. [Google Scholar] [CrossRef] [Green Version]
- Rankin, J.S.; Arentzen, C.E.; Mchale, P.A.; Ling, D.; Anderson, R.W. Diastolic anisotropic properties of the left ventricle in the conscious dog. Circ. Res. 1977, 69, 765–778. [Google Scholar]
- Stroud, J.D.; Baicu, C.F.; Barnes, M.A.; Spinale, F.G.; Zile1, M.R. Viscoelastic properties of pressure overload hypertrophied myocardium: Effect of serine protease treatment. Am. J. Physiol. Hear. Circ. Physiol. 2002, 315, 1691–1702. [Google Scholar] [CrossRef] [Green Version]
- Cansız, F.B.C.; Dal, H.; Kaliske, M. An orthotropic viscoelastic material model for passive myocardium: Theory and algorithmic treatment. Comput. Methods Biomech. Biomed. Eng. 2015, 18, 1160–1172. [Google Scholar] [CrossRef]
- Shetye, S.S.; Troyer, K.L.; Streijger, F.; Lee, J.H.T.; Kwon, B.K.; Cripton, P.A.; Puttlitz, C.M. Nonlinear viscoelastic characterization of the porcine spinal cord. Acta Biomater. 2014, 10, 792–797. [Google Scholar] [CrossRef] [Green Version]
- Troyer, K.L.; Shetye, S.S.; Puttlitz, C.M. Experimental Characterization and Finite Element Implementation of Soft Tissue Nonlinear Viscoelasticity. J. Biomech. Eng. 2012, 134, 114501. [Google Scholar] [CrossRef] [PubMed]
- Wheatley, B.B.; Morrow, D.A.; Odegard, G.M.; Kaufman, K.R.; Haut Donahue, T.L. Skeletal muscle tensile strain dependence: Hyperviscoelastic nonlinearity. J. Mech. Behav. Biomed. Mater. 2016, 53, 445–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gültekin, O.; Sommer, G.; Holzapfel, G.A. An orthotropic viscoelastic model for the passive myocardium: Continuum basis and numerical treatment. Comput. Methods Biomech. Biomed. Eng. 2016, 19, 1647–1664. [Google Scholar] [CrossRef] [PubMed]
- Huyghe, J.M.; van Campen, D.H.; Arts, T.; Heethaar, R.M. The constitutive behaviour of passive heart muscle tissue: A quasi-linear viscoelastic formulation. J. Biomech. 1991, 24, 841–849. [Google Scholar] [CrossRef] [Green Version]
- Rosano, G.M.; Vitale, C. Metabolic Modulation of Cardiac Metabolism in Heart Failure. Card. Fail. Rev. 2018, 4, 99–103. [Google Scholar] [CrossRef]
- Leonard, B.L.; Smaill, B.H.; LeGrice, I.J. Structural Remodeling and Mechanical Function in Heart Failure. Microsc. Microanal. 2012, 18, 50–67. [Google Scholar] [CrossRef]
- Gupte, R.S.; Vijay, V.; Marks, B.; Levine, R.J.; Sabbah, H.N.; Wolin, M.S.; Recchia, F.A.; Gupte, S.A. Upregulation of Glucose-6-Phosphate Dehydrogenase and NAD(P)H Oxidase Activity Increases Oxidative Stress in Failing Human Heart. J. Card. Fail. 2007, 13, 497–506. [Google Scholar] [CrossRef]
- Chen, B.; Frangogiannis, N.G. Macrophages in the Remodeling Failing Heart. Circ. Res. 2016, 119, 776–778. [Google Scholar] [CrossRef] [Green Version]
- Helmes, M.; Trombitás, K.; Centner, T.; Kellermayer, M.; Labeit, S.; Linke, W.A.; Granzier, H. Mechanically driven contour-length adjustment in rat cardiac titin’s unique N2B sequence. Titin is an adjustable spring. Circ. Res. 1999, 84, 1339–1352. [Google Scholar] [CrossRef] [Green Version]
- Francisco, J.V. Interstitial Fibrosis in Heart Failure; Springer: New York, NY, USA, 2005; ISBN 978-0-387-22824-2. [Google Scholar]
- Bishop, J.E.; Laurent, G.J. Collagen turnover and its regulation in the normal and hypertrophying heart. Eur. Heart J. 1995, 16, 38–44. [Google Scholar] [CrossRef]
- Brower, G.L.; Gardner, J.D.; Forman, M.F.; Murray, D.B.; Voloshenyuk, T.; Levick, S.P.; Janicki, J.S. The relationship between myocardial extracellular matrix remodeling and ventricular function. Eur. J. Cardio-Thoracic Surg. 2006, 30, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Golob, M.J.; Wang, Z.; Prostrollo, A.J.; Hacker, T.A.; Chesler, N.C. Limiting collagen turnover via collagenase-resistance attenuates right ventricular dysfunction and fibrosis in pulmonary arterial hypertension. Physiol. Rep. 2016, 4, e12815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plaksej, R.; Kosmala, W.; Frantz, S.; Herrmann, S.; Niemann, M.; Störk, S.; Wachter, R.; Angermann, C.E.; Ertl, G.; Bijnens, B.; et al. Relation of circulating markers of fibrosis and progression of left and right ventricular dysfunction in hypertensive patients with heart failure. J. Hypertens. 2009, 27, 2483–2491. [Google Scholar] [CrossRef] [PubMed]
- Segura, A.M.; Frazier, O.H.; Buja, L.M. Fibrosis and heart failure. Heart Fail. Rev. 2014, 19, 173–185. [Google Scholar] [CrossRef]
- Yu, L.; Ruifrok, W.P.T.; Meissner, M.; Bos, E.M.; Van Goor, H.; Sanjabi, B.; Van Der Harst, P.; Pitt, B.; Goldstein, I.J.; Koerts, J.A.; et al. Genetic and pharmacological inhibition of galectin-3 prevents cardiac remodeling by interfering with myocardial fibrogenesis. Circ. Hear. Fail. 2013, 6, 107–117. [Google Scholar] [CrossRef] [Green Version]
- Begoña, L.; Ramón, Q.; Arantxa, G.; Javier, B.; Mariano, L.; Javier, D. Impact of Treatment on Myocardial Lysyl Oxidase Expression and Collagen Cross-Linking in Patients With Heart Failure. Hypertension 2009, 53, 236–242. [Google Scholar]
- López, B.; González, A.; Querejeta, R.; Larman, M.; Díez, J. Alterations in the Pattern of Collagen Deposition May Contribute to the Deterioration of Systolic Function in Hypertensive Patients With Heart Failure. J. Am. Coll. Cardiol. 2006, 48, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Berk, B.C.; Fujiwara, K.; Lehoux, S. ECM remodeling in hypertensive heart disease. J. Clin. Investiga. 2007, 117, 568–575. [Google Scholar] [CrossRef]
- Rossi, M.A. Pathologic fibrosis and connective tissue matrix in left ventricular hypertrophy due to chronic arterial hypertension in humans. J. Hypertens. 1998, 16, 1031–1041. [Google Scholar] [CrossRef]
- Brower, G.L.; Janicki, J.S. Contribution of ventricular remodeling to pathogenesis of heart failure in rats. Am. J. Physiol. Circ. Physiol. 2001, 280, H674–H683. [Google Scholar] [CrossRef]
- Ryan, T.D.; Rothstein, E.C.; Aban, I.; Tallaj, J.A.; Husain, A.; Lucchesi, P.A.; Dell’Italia, L.J. Left Ventricular Eccentric Remodeling and Matrix Loss Are Mediated by Bradykinin and Precede Cardiomyocyte Elongation in Rats With Volume Overload. J. Am. Coll. Cardiol. 2007, 49, 811–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, J.; Chen, Y.; Pat, B.; Dell’italia, L.A.; Tillson, M.; Dillon, A.R.; Powell, P.C.; Shi, K.; Shah, N.; Denney, T.; et al. Microarray identifies extensive downregulation of noncollagen extracellular matrix and profibrotic growth factor genes in chronic isolated mitral regurgitation in the dog. Circulation 2009, 119, 2086–2095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takashi, N.; Hiroyuki, T.; Hirofumi, T.; Masaru, T.; Keiko, S.; Toshiyuki, K.; Makoto, U.; Kyoko, I.-Y.; Tsutomu, I.; Akira, T. Regulation of Fibrillar Collagen Gene Expression and Protein Accumulation in Volume-Overloaded Cardiac Hypertrophy. Circulation 1997, 95, 2448–2454. [Google Scholar]
- LeWinter, M.M.; Meyer, M. Mechanisms of diastolic dysfunction in heart failure with a preserved ejection fraction: If it’s not one thing it’s another. Circ. Heart Fail. 2013, 6, 1112–1115. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Golfín, C.; Pachón, M.; Corros, C.; Bustos, A.; Cabeza, B.; Ferreirós, J.; de Isla, L.P.; Macaya, C.; Zamorano, J. Left ventricular trabeculae: Quantification in different cardiac diseases and impact on left ventricular morphological and functional parameters assessed with cardiac magnetic resonance. J. Cardiovasc. Med. 2009, 10, 827–833. [Google Scholar] [CrossRef]
- Van de Veerdonk, M.C.; Dusoswa, S.A.; Tim Marcus, J.; Bogaard, H.-J.; Spruijt, O.; Kind, T.; Westerhof, N.; Vonk-Noordegraaf, A. The importance of trabecular hypertrophy in right ventricular adaptation to chronic pressure overload. Int. J. Cardiovasc. Imaging 2014, 30, 357–365. [Google Scholar] [CrossRef]
- Zile, M.R.; Baicu, C.F.; Gaasch, W.H. Diastolic Heart Failure—Abnormalities in Active Relaxation and Passive Stiffness of the Left Ventricle. N. Engl. J. Med. 2004, 350, 1953–1959. [Google Scholar] [CrossRef] [Green Version]
- Prasad, A.; Hastings, J.L.; Shibata, S.; Popovic, Z.B.; Arbab-Zadeh, A.; Bhella, P.S.; Okazaki, K.; Fu, Q.; Berk, M.; Palmer, D.; et al. Characterization of static and dynamic left ventricular diastolic function in patients with heart failure with a preserved ejection fraction. Circ. Heart Fail. 2010, 3, 617–626. [Google Scholar] [CrossRef] [Green Version]
- Røe, Å.T.; Aronsen, J.M.; Skårdal, K.; Hamdani, N.; Linke, W.A.; Danielsen, H.E.; Sejersted, O.M.; Sjaastad, I.; Louch, W.E. Increased passive stiffness promotes diastolic dysfunction despite improved Ca2+ handling during left ventricular concentric hypertrophy. Cardiovasc. Res. 2017, 113, 1161–1172. [Google Scholar] [CrossRef] [Green Version]
- Sakata, Y.; Ohtani, T.; Takeda, Y.; Yamamoto, K.; Mano, T. Left Ventricular Stiffening as Therapeutic Target for Heart Failure With Preserved Ejection Fraction. Circ. J. 2013, 77, 886–892. [Google Scholar] [CrossRef] [Green Version]
- Kraigher-Krainer, E.; Shah, A.M.; Gupta, D.K.; Santos, A.; Claggett, B.; Pieske, B.; Zile, M.R.; Voors, A.A.; Lefkowitz, M.P.; Packer, M.; et al. Impaired Systolic Function by Strain Imaging in Heart Failure With Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2014, 63, 447–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opitz, C.F.; Hoeper, M.M.; Gibbs, J.S.R.; Kaemmerer, H.; Pepke-Zaba, J.; Coghlan, J.G.; Scelsi, L.; D’Alto, M.; Olsson, K.M.; Ulrich, S.; et al. Pre-Capillary, Combined, and Post-Capillary Pulmonary Hypertension: A Pathophysiological Continuum. J. Am. Coll. Cardiol. 2016, 68, 368–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puwanant, S.; Park, M.; Popović, Z.B.; Tang, W.H.W.; Farha, S.; George, D.; Sharp, J.; Puntawangkoon, J.; Loyd, J.E.; Erzurum, S.C.; et al. Ventricular geometry, strain, and rotational mechanics in pulmonary hypertension. Circulation 2010, 121, 259–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sachdev, A.; Villarraga, H.R.; Frantz, R.P.; McGoon, M.D.; Hsiao, J.-F.; Maalouf, J.F.; Ammash, N.M.; McCully, R.B.; Miller, F.A.; Pellikka, P.A.; et al. Right Ventricular Strain for Prediction of Survival in Patients With Pulmonary Arterial Hypertension. Chest 2011, 139, 1299–1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haeck, M.L.; Scherptong, R.W.; Marsan, N.A.; Holman, E.R.; Schalij, M.J.; Bax, J.J.; Vliegen, H.W.; Delgado, V. Prognostic Value of Right Ventricular Longitudinal Peak Systolic Strain in Patients With Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2012, 5, 628–636. [Google Scholar] [CrossRef] [Green Version]
- Finsberg, H.; Xi, C.; Tan, J.L.; Zhong, L.; Genet, M.; Sundnes, J.; Lee, L.C.; Wall, S.T. Efficient estimation of personalized biventricular mechanical function employing gradient-based optimization. Int. J. Numer. Methods Biomed. Eng. 2018, 34, e2982. [Google Scholar] [CrossRef] [Green Version]
- Kennish, A.; Yellin, E.; Frater, R.W.; Frater, W. Dynamic stiffness profiles in the left ventricle. J. Appl. Physiol. 1975, 39, 665–671. [Google Scholar] [CrossRef]
- LeWinter, M.M.; Engler, R.; Pavelec, R.S. Time-dependent shifts of the left ventricular diastolic filling relationship in conscious dogs. Circ. Res. 1979, 45, 641–653. [Google Scholar] [CrossRef] [Green Version]
- Gaasch, W.H.; Zile, M.R. Left Ventricular Diastolic Dysfunction and Diastolic Heart Failure. Ann. Rev. Med. 2004, 55, 373–394. [Google Scholar] [CrossRef]
- Burlew, B.S.; Weber, K.T. Cardiac Fibrosis as a Cause of Diastolic Dysfunction. Herz 2002, 27, 92–98. [Google Scholar] [CrossRef]
- Weber, K.T.; Brilla, C.G. Pathological hypertrophy and cardiac interstitium. Fibrosis and renin-angiotensin-aldosterone system. Circulation 1991, 83, 1849–1865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maron, B.J.; Bonow, R.O.; Cannon, R.O.; Leon, M.B.; Epstein, S.E. Hypertrophic Cardiomyopathy. N. Engl. J. Med. 1987, 316, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Borbély, A.; Van Der Velden, J.; Papp, Z.; Bronzwaer, J.G.; Edes, I.; Stienen, G.J.; Paulus, W.J. Cardiomyocyte Stiffness in Diastolic Heart Failure. Circulation 2005, 111, 774–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Method | Axial Definition | Preconditioning Cycles | Strain Range/Rate | Bath Medium | Temperature | Immerse Condition |
|---|---|---|---|---|---|---|---|
| Canine RV [17] | Biaxial | Main fiber direction | 10 | 30% / | Water with recycle required oxygenated carioplegic solution | Room temperature | Immersed |
| Rat RV [20] | Biaxial | Outflow tract | / | / / | Modified Kreb’s solution with 2,3-butanedione 2-monoxime and oxygen | / | Immersed |
| Bovine LV/RV [22] | Biaxial and uniaxial | Main fiber direction | 5 | 20% 0.10.75 cm/s | Saline with O2 and CO2 (pH = 7.4) | Physiological range | Immersed |
| Human LV/RV [23] | Biaxial* and Triaxial | Main fiber direction | 4 | 20% Quasi-static | CPS with 20 mM BDM | 37 °C | Immersed |
| Canine LV [24] | Biaxial | Main fiber direction | ≥7 | / 50s/cycle | Modified Kreb’s Ringers solution with a ~ 10 mM potassium, O2, and CO2 (pH = 7.4) | 30 °C | Float |
| Canine LV [25] | Biaxial | Main fiber direction | 5–7 | 20% 0.05 or 0.1Hz | Bath containing the oxygenated solution | Room temperature | Immersed |
| Canine LV [26] | Biaxial | Main fiber direction | 7–10 | 5%–27% 0.1 Hz | Oxygenated cardioplegic solution | Room temperature | Immersed |
| Rabbit LV [27] | Biaxial | Main fiber direction | Several | / | BDM–Krebs solution | / | Immersed |
| Ovine LV [28] | Biaxial | / | 10 | 20%–25% 0.5 Hz | Isotonic cardioplegic solution (pH:7.4) | 20 °C | Immersed |
| Murine RV [29] | Biaxial | Outflow tract | 10 | 5–25 kPa / | Modified Kreb’s solution with BDM | Room temperature | Immersed |
| Human LV/RV [30] | Biaxial and uniaxial | Main fiber direction | 5 | 40% ~6 mm/min | Phosphate-buffered saline (PBS) | 37 °C | Immersed |
| Canine LV [39] | Biaxial and uniaxial* | Main fiber direction | 9 | / 0.0025–0.25 mm/s | Tyrode solution with O2 and CO2 (pH:7.4) | 29.5–30.5 °C | Float |
| Rat RV [40] | Biaxial | Outflow tract | / | / / | Modified Kreb’s solution with BDM and oxygen | Room temperature | Immersed |
| Canine LV/RV [43] | Biaxial | Apex to base | / | / / | Oxygenated solution | Room temperature | Immersed |
| Ovine LV/RV [44] | Biaxial | Main fiber direction | 10 | 40% 8 s per cycle | Saline bath | 37 °C | Immersed |
| Rat LV [45] | Biaxial and uniaxial | / | 10 | / 0.5mm/s | PBS | 37 °C | Submerged |
| Porcine LV/RV [46] | Biaxial and uniaxial* | Main fiber direction | / | / 0.5mm/s | PBS | 37 °C | Submerged |
| Sample | Method | Ramp Speed | Stretch Level | Duration | Bath Condition |
|---|---|---|---|---|---|
| Human LV/RV [23] | Stress relaxation | 100 mm/min | 10% | 5 min | CPS with 20 mM BDM at 37 °C |
| Rabbit LV papillary muscle [54] | Stress relaxation and creep | / | / | 5 min | Ringer–Lacke solution with O2, CO2, pH = 7.38 |
| Cats, Rabbits papillary muscle; Frog and Turtle LV [55] | Stress relaxation and creep | / | 20%, 30% | / | Tyrode solution with O2, CO2, pH = 7.3, at 24 °C (for papillary muscles); Modified PBS solution at pH = 7.3 (for LVs) |
| Chicken embryonic heart [56] | Stress relaxation | Fast linear | 10%, 20%, 40% | 10 min | Oxygenated KHB–CPS at 35 °C |
| Chicken LV/RV [57] | Stress relaxation | 1000% axial strain/s | 5%, 10%, 20%, 30% | 5 min | Oxygenated KHB–CPS at 35 °C |
| Cat LV papillary muscle [58] | Stress relaxation | / | / | / | Oxygenated Kreb’s–Ringer’s solution at 20 °C |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, W.; Wang, Z. Current Understanding of the Biomechanics of Ventricular Tissues in Heart Failure. Bioengineering 2020, 7, 2. https://doi.org/10.3390/bioengineering7010002
Liu W, Wang Z. Current Understanding of the Biomechanics of Ventricular Tissues in Heart Failure. Bioengineering. 2020; 7(1):2. https://doi.org/10.3390/bioengineering7010002
Chicago/Turabian StyleLiu, Wenqiang, and Zhijie Wang. 2020. "Current Understanding of the Biomechanics of Ventricular Tissues in Heart Failure" Bioengineering 7, no. 1: 2. https://doi.org/10.3390/bioengineering7010002