

Computerised Cardiotocography Analysis for the Automated Detection of Fetal Compromise during Labour: A Review

Abstract
:
1. Introduction
2. Physiological Basis for CTG Monitoring during Labour
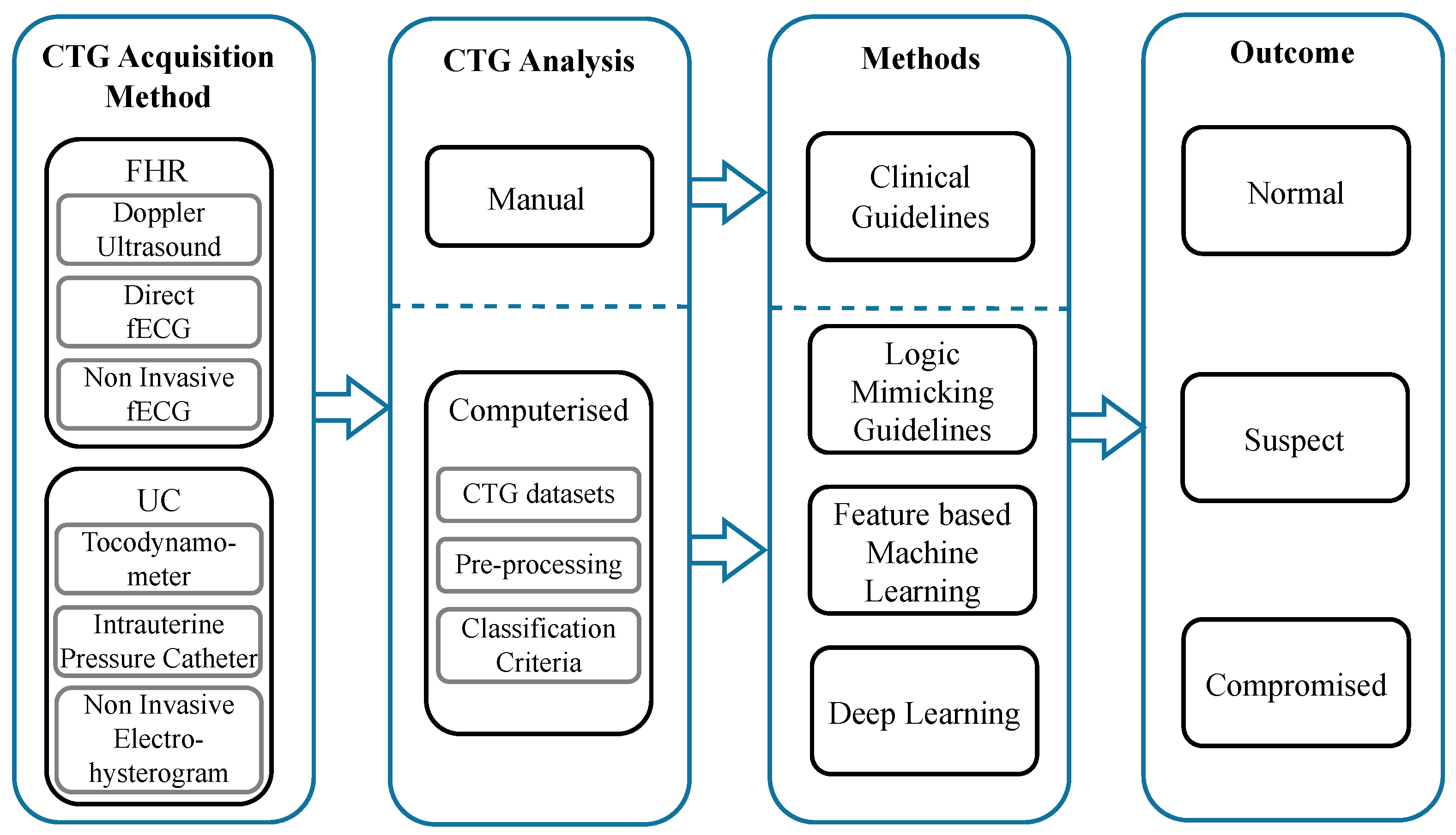
3. Fetal Heart Rate and Uterine Contraction Monitoring Technologies
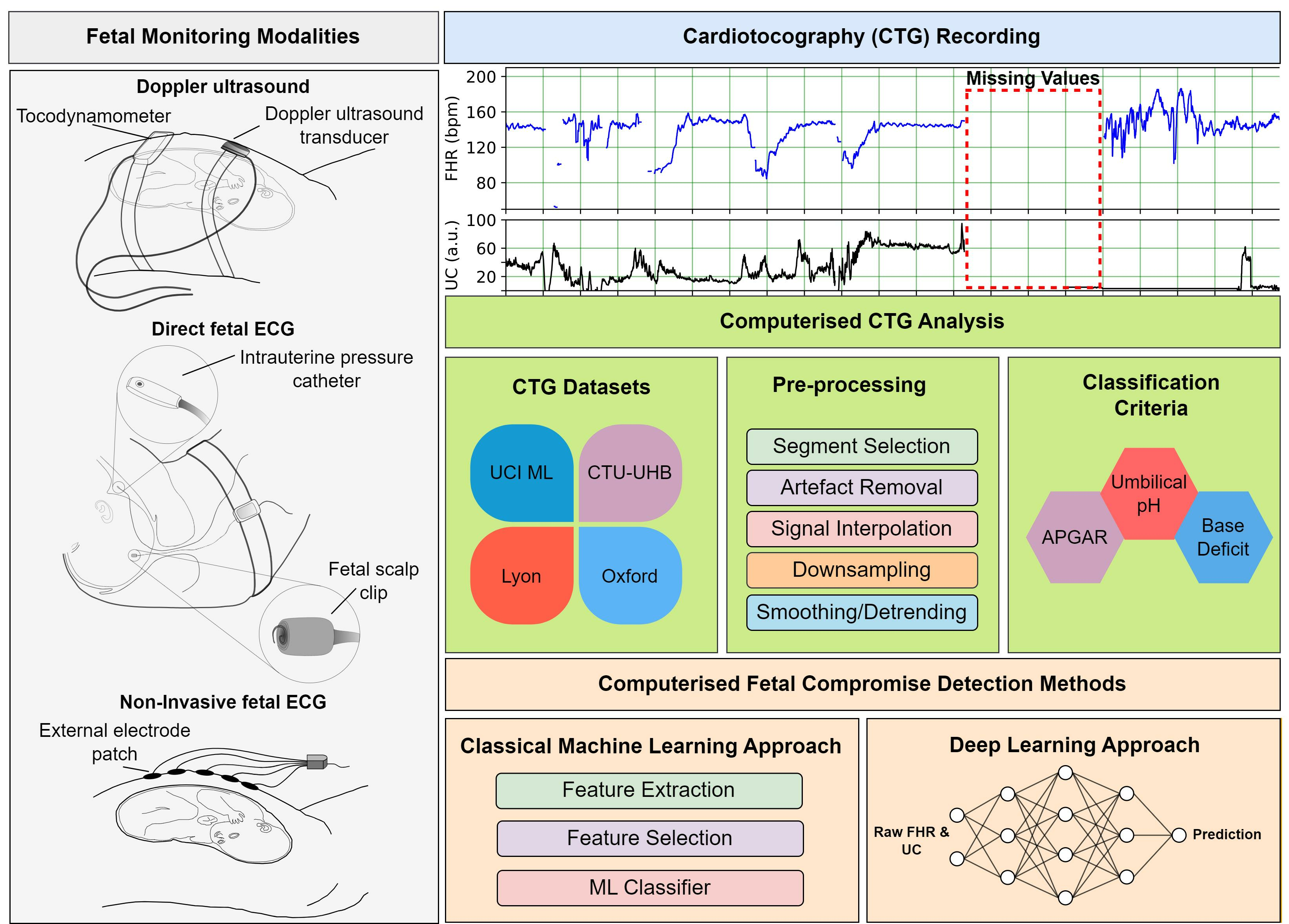
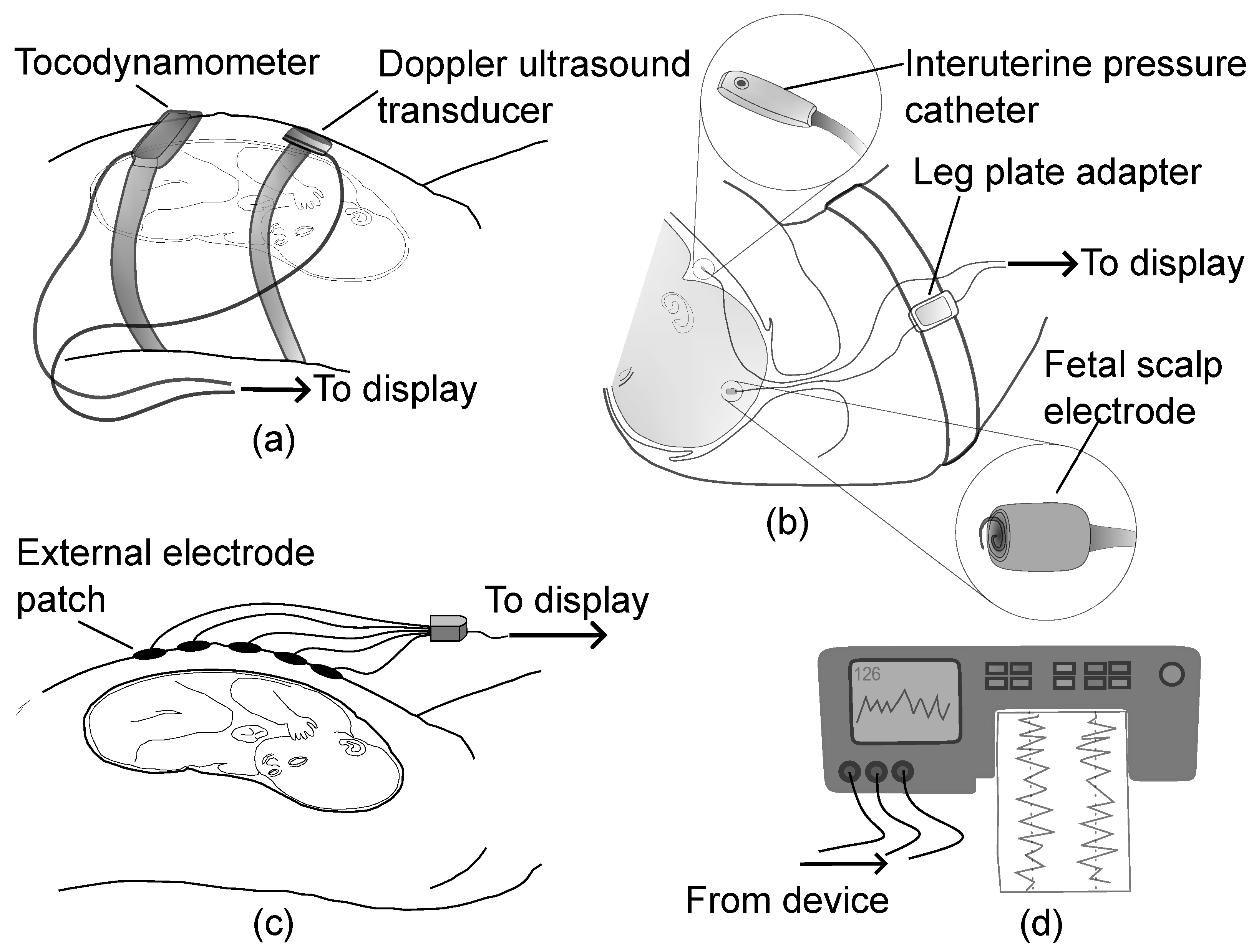
3.1. Fetal Heart Rate Monitoring Technologies
3.1.1. Doppler Ultrasound
3.1.2. Direct Fetal Electrocardiogram
3.1.3. Non-Invasive Fetal Electrocardiogram
3.2. Uterine Contraction Technologies
3.2.1. External Tocodynamometer
3.2.2. Intrauterine Pressure Catheter
3.2.3. Non-Invasive Electrohysterogram
4. Computerised CTG Analysis Systems in Clinical Practice
5. CTG Datasets
6. FHR Pre-Processing Techniques
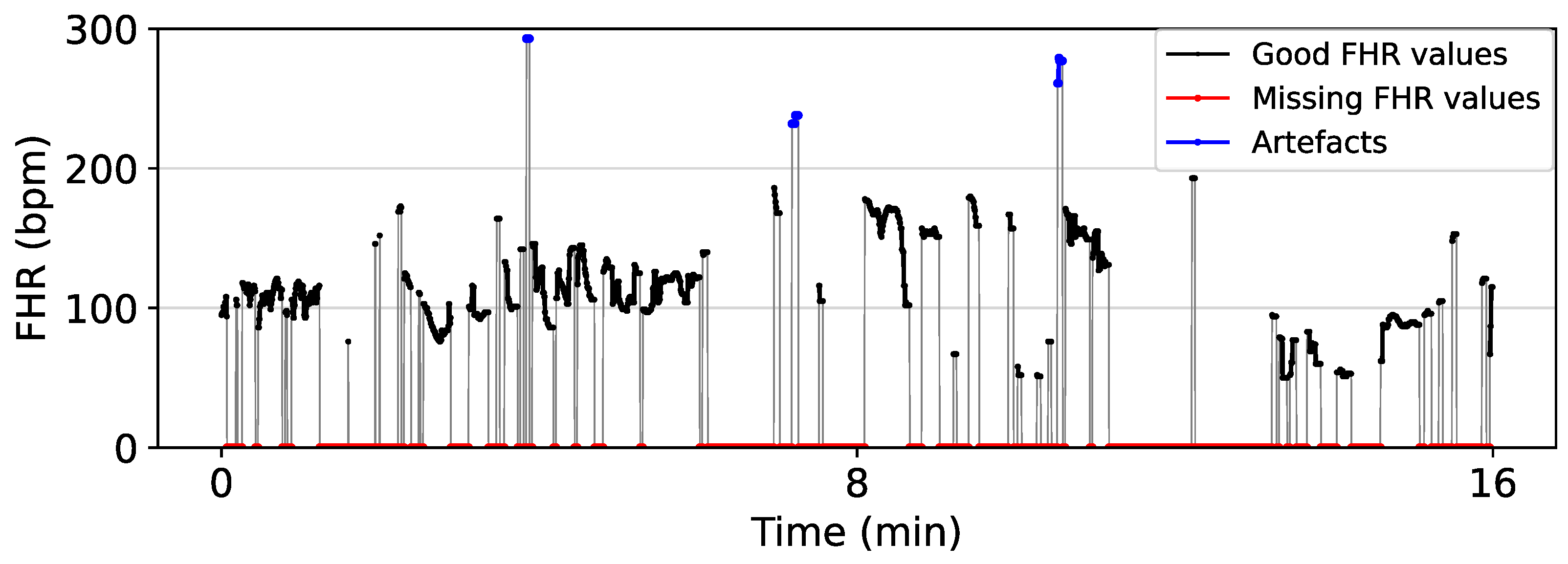
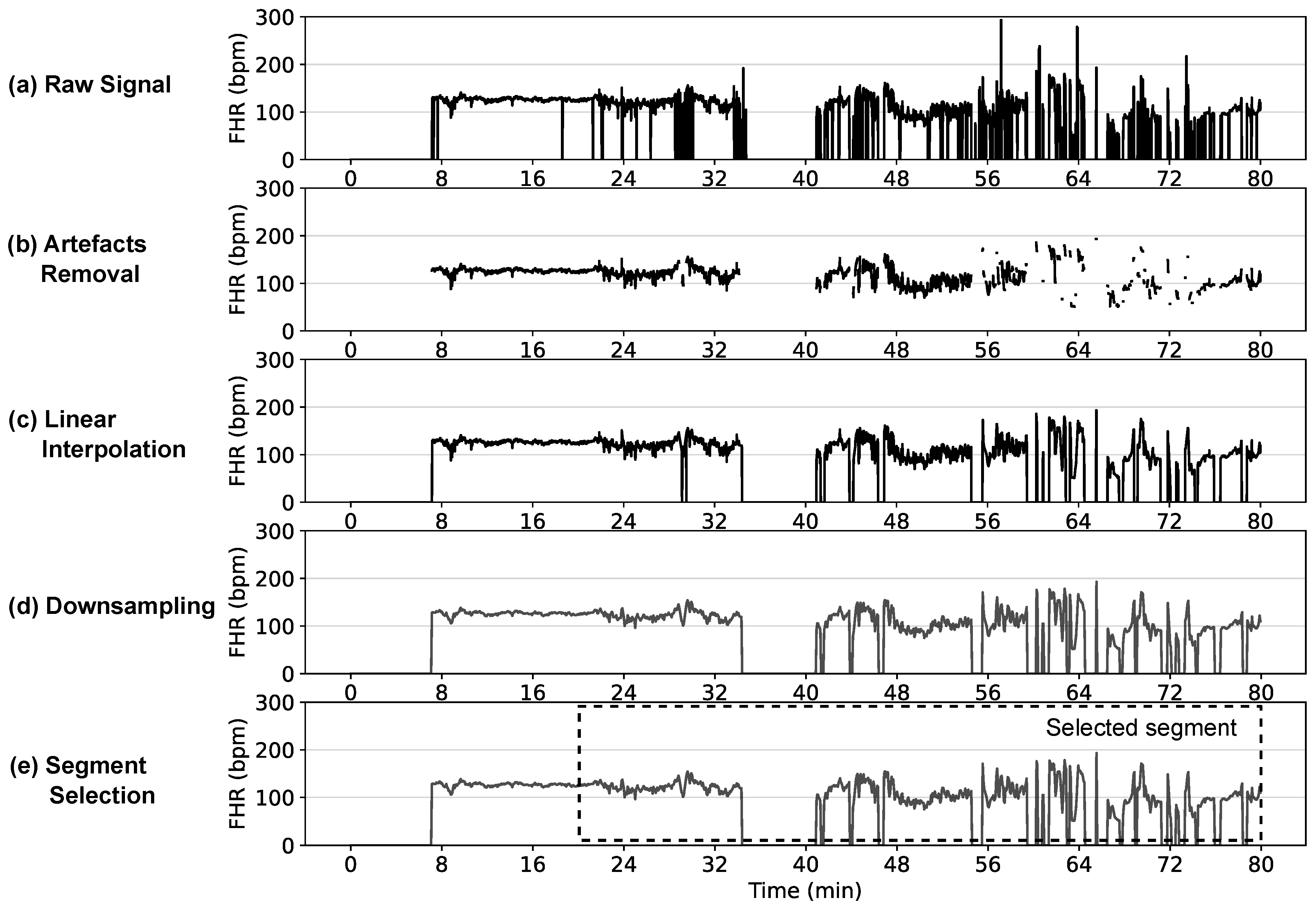
- Segment SelectionIn clinical practice, labour is divided into three stages: Stage I is where the cervix starts dilating (<10 cm) and frequent contractions occur; Stage II is the period from when the cervix is fully dilated (10 cm) to when the baby is born; Stage III starts after the baby is born and continues until delivery of placenta and membranes. In the segment selection step, a signal segment with sufficient quality that is closer to the delivery of the baby is typically selected as this is representative of the level of asphyxia and correlates best with the cord pH at birth. Unfortunately, the FHR signal is typically most affected by noise and artefacts at this point of labour [85]. FIGO guidelines require the signal loss to be less than 20% for a signal to be acceptable for evaluation [14]. Different prior studies have selected signal lengths varying from 10–60 min before birth to analyse, whilst others simply select the segment of trace during a certain stage of the labour [44].
- Artefact RemovalA typical baseline heart rate of a normal fetus varies between 110 bpm and 160 bpm, and accelerations or decelerations occur when amplitude varies 15 bpm above or below the baseline lasting for more than 15 s respectively [11]. In the artefact removal step, values below 50 bpm and above 200 bpm are typically considered outliers and removed [36]. In some studies, consecutive missing values of more than 15 s (long gaps) are removed from the analysis [36,40,86]. For others, when the difference between two adjacent FHR values exceeds 25 bpm, the corresponding signal segment from the previous FHR value to the next stable segment is considered unstable and removed [45,85]. A stable segment is a signal segment with five consecutive FHR values having a difference of less than 10 bpm between them [31].
- Signal InterpolationThe signal interpolation step employs techniques like linear [87] and spline [35] interpolation to fill the missing FHR values created from the previous steps. Generally, the interpolation is performed for gaps < 15 s, and the gaps > 15 s in the FHR are either skipped or removed in subsequent feature extraction and deep learning training processes [35,39,86]. In linear interpolation, these missing gaps are approximated using the slope of the data points on either side of the gap. Spline interpolation uses a set of low-degree polynomials called a spline to estimate the missing gaps to make the signal smoother and continuous. When polynomials of degree 3 are used in the spline, the resulting interpolation is called cubic spline interpolation. The Hermite spline interpolation uses polynomials defined by the values and the derivatives at the endpoints of the corresponding interval to estimate the missing values.
- DownsamplingA typical fetal heart beats less than 3 times per second (<180 bpm), making some data of the original FHR signals sampled at 4 Hz redundant [46,87]. Therefore, in this step, the FHR signal is sometimes downsampled to reduce the computational complexity and memory needed to process the input signals. For example, only 900 values are required to represent a 60 min FHR signal at 0.25 Hz, compared to the 14,400 values required for the same signal at 4 Hz.
- Smoothing and Detrending
7. UC Pre-Processing Techniques
8. Fetal Compromise Classification Criteria
9. Automated Fetal Compromise Classification Methods
9.1. Feature Extraction
9.1.1. Morphological and Time Domain
9.1.2. Frequency Domain
9.1.3. Non-Linear Domain
9.2. Feature Selection
9.3. Classical Machine Learning Classifiers
9.3.1. AdaBoost
9.3.2. Artificial Neural Networks
9.3.3. Bayesian Models
9.3.4. Decision Trees
9.3.5. Deep Gaussian Processes
9.3.6. Logistic Regression
9.3.7. Random Forest
9.3.8. SVM
9.4. Deep Learning-Based Classifiers
9.4.1. Convolutional Neural Networks
9.4.2. Long Short-Term Memory Networks
9.5. Performance Evaluation
10. Discussion
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations Inter-agency Group for Child Mortality Estimation (UN IGME). A Neglected Tragedy: The Global Burden of Stillbirths; Report; United Nations Children’s Fund: New York, NY, USA, 2020. [Google Scholar]
- Lawn, J.E.; Lee, A.C.; Kinney, M.; Sibley, L.; Carlo, W.A.; Paul, V.K.; Pattinson, R.; Darmstadt, G.L. Two million intrapartum-related stillbirths and neonatal deaths: Where, why, and what can be done? Int. J. Gynecol. Obstet. 2009, 107, S5–S19. [Google Scholar] [CrossRef]
- Lawn, J.E.; Gravett, M.G.; Nunes, T.M.; Rubens, C.E.; Stanton, C.; the GAPPS Review Group. Global report on preterm birth and stillbirth (1 of 7): Definitions, description of the burden and opportunities to improve data. BMC Pregnancy Childbirth 2010, 10, S1. [Google Scholar] [CrossRef]
- Vogel, J.; Souza, J.; Mori, R.; Morisaki, N.; Lumbiganon, P.; Laopaiboon, M.; Ortiz-Panozo, E.; Hernandez, B.; Pérez-Cuevas, R.; Roy, M.; et al. Maternal complications and perinatal mortality: Findings of the World Health Organization Multicountry Survey on Maternal and Newborn Health. Bjog Int. J. Obstet. Gynaecol. 2014, 121, 76–88. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Das, J.K.; Bahl, R.; Lawn, J.E.; Salam, R.A.; Paul, V.K.; Sankar, M.J.; Blencowe, H.; Rizvi, A.; Chou, V.B.; et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet 2014, 384, 347–370. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.L.; Harrison, M.S.; McClure, E.M. Stillbirths: The Hidden Birth Asphyxia—US and Global Perspectives. Clin. Perinatol. 2016, 43, 439–453. [Google Scholar] [CrossRef] [PubMed]
- Low, J.A. Intrapartum fetal asphyxia: Definition, diagnosis, and classification. Am. J. Obstet. Gynecol. 1997, 176, 957–959. [Google Scholar] [CrossRef] [PubMed]
- Bennet, L.; Gunn, A.J. The Fetal Heart Rate Response to Hypoxia: Insights from Animal Models. Clin. Perinatol. 2009, 36, 655–672. [Google Scholar] [CrossRef] [PubMed]
- Dilenge, M.E.; Majnemer, A.; Shevell, M.I. Topical Review: Long-Term Developmental Outcome of Asphyxiated Term Neonates. J. Child Neurol. 2001, 16, 781–792. [Google Scholar] [CrossRef]
- Kawagoe, Y.; Sameshima, H. Hypoxia: Animal experiments and clinical implications. J. Obstet. Gynaecol. Res. 2017, 43, 1381–1390. [Google Scholar] [CrossRef]
- Ayres-de Campos, D.; Spong, C.Y.; Chandraharan, E.; FIGO Intrapartum Fetal Monitoring Expert Consensus Panel. FIGO consensus guidelines on intrapartum fetal monitoring: Cardiotocography. Int. J. Gynecol. Obstet. 2015, 131, 13–24. [Google Scholar] [CrossRef]
- Ayres-de Campos, D. Electronic fetal monitoring or cardiotocography, 50 years later: What’s in a name? Am. J. Obstet. Gynecol. 2018, 218, 545–546. [Google Scholar] [CrossRef] [PubMed]
- Reinhard, J.; Hayes-Gill, B.R.; Schiermeier, S.; Hatzmann, W.; Herrmann, E.; Heinrich, T.M.; Louwen, F. Intrapartum signal quality with external fetal heart rate monitoring: A two way trial of external Doppler CTG ultrasound and the abdominal fetal electrocardiogram. Arch. Gynecol. Obstet. 2012, 286, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Bakker, P.; Colenbrander, G.; Verstraeten, A.; Van Geijn, H. The quality of intrapartum fetal heart rate monitoring. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 116, 22–27. [Google Scholar] [CrossRef]
- Bakker, P.C.A.M.; Rijsiwijk, S.V.; Geijn, H.P.v. Uterine activity monitoring during labor. J. Perinat. Med. 2007, 35, 468–477. [Google Scholar] [CrossRef] [PubMed]
- Euliano, T.Y.; Nguyen, M.T.; Darmanjian, S.; Mcgowrray, S.P.; Euliano, N.; Onkala, A.; Gregg, A.R. Monitoring uterine activity during labor: A comparison of three methods. Am. J. Obstet. Gynecol. 2013, 208, 66.e1–66.e6. [Google Scholar] [CrossRef]
- Lempersz, C.; Noben, L.; van Osta, G.; Wassen, M.L.H.; Meershoek, B.P.J.; Bakker, P.; Jacquemyn, Y.; Cuerva, M.J.; Vullings, R.; Westerhuis, M.E.M.H.; et al. Intrapartum non-invasive electrophysiological monitoring: A prospective observational study. Acta Obstet. Gynecol. Scand. 2020, 99, 1387–1395. [Google Scholar] [CrossRef]
- Alfirevic, Z.; Gyte, G.M.; Cuthbert, A.; Devane, D. Continuous cardiotocography (CTG) as a form of electronic fetal monitoring (EFM) for fetal assessment during labour. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Grivell, R.M.; Alfirevic, Z.; Gyte, G.M.; Devane, D. Antenatal cardiotocography for fetal assessment. Cochrane Database Syst. Rev. 2015, 2015, CD007863. [Google Scholar] [CrossRef]
- Devane, D.; Lalor, J.G.; Daly, S.; McGuire, W.; Cuthbert, A.; Smith, V. Cardiotocography versus intermittent auscultation of fetal heart on admission to labour ward for assessment of fetal wellbeing. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Hruban, L.; Spilka, J.; Chudáček, V.; Janků, P.; Huptych, M.; Burša, M.; Hudec, A.; Kacerovský, M.; Koucký, M.; Procházka, M.; et al. Agreement on intrapartum cardiotocogram recordings between expert obstetricians. J. Eval. Clin. Pract. 2015, 21, 694–702. [Google Scholar] [CrossRef]
- Devane, D.; Lalor, J. Midwives’ visual interpretation of intrapartum cardiotocographs: Intra- and inter-observer agreement. J. Adv. Nurs. 2005, 52, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, S.P.; Klauser, C.K.; Woodring, T.C.; Sanderson, M.; Magann, E.F.; Morrison, J.C. Intrapartum nonreassuring fetal heart rate tracing and prediction of adverse outcomes: Interobserver variability. Am. J. Obstet. Gynecol. 2008, 199, 623.e1–623.e5. [Google Scholar] [CrossRef] [PubMed]
- Steer, P.J. Has electronic fetal heart rate monitoring made a difference. Semin. Fetal Neonatal Med. 2008, 13, 2–7. [Google Scholar] [CrossRef]
- Armstrong, L.; Stenson, B.J. Use of umbilical cord blood gas analysis in the assessment of the newborn. Arch. Dis. Child. Fetal Neonatal Ed. 2007, 92, F430–F434. [Google Scholar] [CrossRef] [PubMed]
- Ayres-de Campos, D.; Arulkumaran, S.; Panel, F.I.F.M.E.C. FIGO consensus guidelines on intrapartum fetal monitoring: Physiology of fetal oxygenation and the main goals of intrapartum fetal monitoring. Int. J. Gynecol. Obstet. 2015, 131, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Wayenberg, J.L. Threshold of metabolic acidosis associated with neonatal encephalopathy in the term newborn. J. Matern.-Fetal Neonatal Med. 2005, 18, 381–385. [Google Scholar] [CrossRef]
- Casey, B.M.; McIntire, D.D.; Leveno, K.J. The Continuing Value of the Apgar Score for the Assessment of Newborn Infants. N. Engl. J. Med. 2001, 344, 467–471. [Google Scholar] [CrossRef]
- Chung, T.K.H.; Mohajer, M.P.; Yang, Z.J.; Chang, A.M.Z.; Sahota, D.S. The prediction of fetal acidosis at birth by computerised analysis of intrapartum cardiotocography. Bjog Int. J. Obstet. Gynaecol. 1995, 102, 454–460. [Google Scholar] [CrossRef]
- Dawes, G.S.; Moulden, M.; Redman, C.W. System 8000: Computerised antenatal FHR analysis. J. Perinat. Med. 1991, 19, 47–51. [Google Scholar] [CrossRef]
- Bernardes, J.; Moura, C.; de Sa, J.P.; Leite, L.P. The Porto system for automated cardiotocographic signal analysis. J. Perinat. Med. 1991, 19, 61–65. [Google Scholar] [CrossRef]
- Keith, R.D.; Greene, K.R. Development, evaluation and validation of an intelligent system for the management of labour. Bailliere’S Clin. Obstet. Gynaecol. 1994, 8, 583–605. [Google Scholar] [CrossRef] [PubMed]
- Group, T.I.C. Computerised interpretation of fetal heart rate during labour (INFANT): A randomised controlled trial. Lancet 2017, 389, 1719–1729. [Google Scholar] [CrossRef]
- Georgieva, A.; Redman, C.W.G.; Papageorghiou, A.T. Computerised data-driven interpretation of the intrapartum cardiotocogram: A cohort study. Acta Obstet. Gynecol. Scand. 2017, 96, 883–891. [Google Scholar] [CrossRef]
- Spilka, J.; Georgoulas, G.; Karvelis, P.; Oikonomou, V.P.; Chudáček, V.; Stylios, C.; Lhotská, L.; Janků, P. Automatic Evaluation of FHR Recordings from CTU-UHB CTG Database. In Information Technology in Bio- and Medical Informatics, Proceedings of the 4th International Conference, ITBAM 2013, Prague, Czech Republic, 28 August 2013; Bursa, M., Khuri, S., Renda, M.E., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 47–61. [Google Scholar] [CrossRef]
- Spilka, J.; Georgoulas, G.; Karvelis, P.; Chudáček, V.; Stylios, C.D.; Lhotská, L. Discriminating Normal from “Abnormal” Pregnancy Cases Using an Automated FHR Evaluation Method. In Artificial Intelligence: Methods and Applications, Proceedings of the 8th Hellenic Conference on AI, SETN 2014, Ioannina, Greece, 15–17May 2014; Likas, A., Blekas, K., Kalles, D., Eds.; Springer: Cham, Switzerland, 2014; pp. 521–531. [Google Scholar] [CrossRef]
- Petrozziello, A.; Redman, C.W.G.; Papageorghiou, A.T.; Jordanov, I.; Georgieva, A. Multimodal Convolutional Neural Networks to Detect Fetal Compromise During Labor and Delivery. IEEE Access 2019, 7, 112026–112036. [Google Scholar] [CrossRef]
- Spilka, J.; Chudáček, V.; Huptych, M.; Leonarduzzi, R.; Abry, P.; Doret, M. Intrapartum Fetal Heart Rate Classification: Cross-Database Evaluation. In Proceedings of the XIV Mediterranean Conference on Medical and Biological Engineering and Computing 2016, Paphos, Cyprus, 31 March–2 April 2016; Kyriacou, E., Christofides, S., Pattichis, C.S., Eds.; Springer: Cham, Switzerland, 2016; pp. 1199–1204. [Google Scholar] [CrossRef]
- Stylios, C.D.; Georgoulas, G.; Karvelis, P.; Spilka, J.; Chudáček, V.; Lhotska, L. Least Squares Support Vector Machines for FHR Classification and Assessing the pH Based Categorization. In Proceedings of the XIV Mediterranean Conference on Medical and Biological Engineering and Computing 2016, Paphos, Cyprus, 31 March–2 April 2016; Kyriacou, E., Christofides, S., Pattichis, C.S., Eds.; Springer: Cham, Switzerland, 2016; pp. 1211–1215. [Google Scholar] [CrossRef]
- Georgoulas, G.; Karvelis, P.; Spilka, J.; Chudáček, V.; Stylios, C.D.; Lhotská, L. Investigating pH based evaluation of fetal heart rate (FHR) recordings. Health Technol. 2017, 7, 241–254. [Google Scholar] [CrossRef]
- Feng, G.; Quirk, J.G.; Djurić, P.M. Supervised and Unsupervised Learning of Fetal Heart Rate Tracings with Deep Gaussian Processes. In Proceedings of the 2018 14th Symposium on Neural Networks and Applications (NEUREL), Belgrade, Serbia, 20–21 November 2018; pp. 1–6. [Google Scholar] [CrossRef]
- Gonçalves, H.; Rocha, A.P.; Ayres-de Campos, D.; Bernardes, J. Linear and nonlinear fetal heart rate analysis of normal and acidemic fetuses in the minutes preceding delivery. Med. Biol. Eng. Comput. 2006, 44, 847. [Google Scholar] [CrossRef]
- Zhao, Z.; Zhang, Y.; Deng, Y. A Comprehensive Feature Analysis of the Fetal Heart Rate Signal for the Intelligent Assessment of Fetal State. J. Clin. Med. 2018, 7, 223. [Google Scholar] [CrossRef]
- Cömert, Z.; Kocamaz, A.F.; Subha, V. Prognostic model based on image-based time-frequency features and genetic algorithm for fetal hypoxia assessment. Comput. Biol. Med. 2018, 99, 85–97. [Google Scholar] [CrossRef]
- Zhao, Z.; Zhang, Y.; Comert, Z.; Deng, Y. Computer-Aided Diagnosis System of Fetal Hypoxia Incorporating Recurrence Plot With Convolutional Neural Network. Front. Physiol. 2019, 10, 255. [Google Scholar] [CrossRef]
- Liu, M.; Lu, Y.; Long, S.; Bai, J.; Lian, W. An attention-based CNN-BiLSTM hybrid neural network enhanced with features of discrete wavelet transformation for fetal acidosis classification. Expert Syst. Appl. 2021, 186, 115714. [Google Scholar] [CrossRef]
- Cömert, Z.; Kocamaz, A.F. Open-access software for analysis of fetal heart rate signals. Biomed. Signal Process. Control 2018, 45, 98–108. [Google Scholar] [CrossRef]
- Tournier, A.; Beacom, M.; Westgate, J.A.; Bennet, L.; Garabedian, C.; Ugwumadu, A.; Gunn, A.J.; Lear, C.A. Physiological control of fetal heart rate variability during labour: Implications and controversies. J. Physiol. 2022, 600, 431–450. [Google Scholar] [CrossRef] [PubMed]
- Ponsiglione, A.M.; Cosentino, C.; Cesarelli, G.; Amato, F.; Romano, M. A Comprehensive Review of Techniques for Processing and Analyzing Fetal Heart Rate Signals. Sensors 2021, 21, 6136. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.; Monteiro-Santos, J.; Castro, L.; Antunes, L.; Costa-Santos, C.; Teixeira, A.; Henriques, T.S. Non-linear Methods Predominant in Fetal Heart Rate Analysis: A Systematic Review. Front. Med. 2021, 8, 661226. [Google Scholar] [CrossRef]
- Castro, L.; Loureiro, M.; Henriques, T.S.; Nunes, I. Systematic Review of Intrapartum Fetal Heart Rate Spectral Analysis and an Application in the Detection of Fetal Acidemia. Front. Pediatr. 2021, 9, 661400. [Google Scholar] [CrossRef]
- O’Sullivan, M.E.; Considine, E.C.; O’Riordan, M.; Marnane, W.P.; Rennie, J.M.; Boylan, G.B. Challenges of Developing Robust AI for Intrapartum Fetal Heart Rate Monitoring. Front. Artif. Intell. 2021, 4, 765210. [Google Scholar] [CrossRef] [PubMed]
- Ben M’Barek, I.; Jauvion, G.; Ceccaldi, P. Computerised cardiotocography analysis during labor—A state-of-the-art review. Acta Obstet. Gynecol. Scand. 2022, 102, 130–137. [Google Scholar] [CrossRef]
- Bernardes, J. Computerised analysis of cardiotocograms in clinical practice and the SisPorto® system thirty-two years after: Technological, physiopathological and clinical studies. J. Perinat. Med. 2023, 51, 145–160. [Google Scholar] [CrossRef]
- Nageotte, M.P. Fetal heart rate monitoring. Semin. Fetal Neonatal Med. 2015, 20, 144–148. [Google Scholar] [CrossRef]
- Pinas, A.; Chandraharan, E. Continuous cardiotocography during labour: Analysis, classification and management. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 30, 33–47. [Google Scholar] [CrossRef]
- Ugwumadu, A. Understanding cardiotocographic patterns associated with intrapartum fetal hypoxia and neurologic injury. Best Pract. Res. Clin. Obstet. Gynaecol. 2013, 27, 509–536. [Google Scholar] [CrossRef]
- Divon, M.Y.; Torres, F.P.; Yeh, S.Y.; Paul, R.H. Autocorrelation techniques in fetal monitoring. Am. J. Obstet. Gynecol. 1985, 151, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.C. Signal processing and display—cardiotocographs. Bjog Int. J. Obstet. Gynaecol. 1993, 100, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Cohen, W.R.; Hayes-Gill, B. Influence of maternal body mass index on accuracy and reliability of external fetal monitoring techniques. Acta Obstet. Gynecol. Scand. 2014, 93, 590–595. [Google Scholar] [CrossRef]
- Cohen, W.R.; Ommani, S.; Hassan, S.; Mirza, F.G.; Solomon, M.; Brown, R.; Schifrin, B.S.; Himsworth, J.M.; Hayes-Gill, B.R. Accuracy and reliability of fetal heart rate monitoring using maternal abdominal surface electrodes. Acta Obstet. Gynecol. Scand. 2012, 91, 1306–1313. [Google Scholar] [CrossRef] [PubMed]
- Euliano, T.Y.; Darmanjian, S.; Nguyen, M.T.; Busowski, J.D.; Euliano, N.; Gregg, A.R. Monitoring Fetal Heart Rate during Labor: A Comparison of Three Methods. J. Pregnancy 2017, 2017, 8529816. [Google Scholar] [CrossRef]
- Declercq, E.R.; Sakala, C.; Corry, M.P.; Applebaum, S.; Herrlich, A. Major Survey Findings of Listening to MothersSM III: Pregnancy and Birth. J. Perinat. Educ. 2014, 23, 9–16. [Google Scholar] [CrossRef]
- Wood, P.L.; Dobbie, H.G. Equipment. In Electronic Fetal Heart Rate Monitoring: A Practical Guide; Wood, P.L., Dobbie, H.G., Eds.; Macmillan Education: London, UK, 1989; pp. 6–11. [Google Scholar] [CrossRef]
- Neilson, D.R.; Freeman, R.K.; Mangan, S. Signal ambiguity resulting in unexpected outcome with external fetal heart rate monitoring. Am. J. Obstet. Gynecol. 2008, 198, 717–724. [Google Scholar] [CrossRef]
- Behar, J.; Andreotti, F.; Zaunseder, S.; Oster, J.; Clifford, G.D. A practical guide to non-invasive foetal electrocardiogram extraction and analysis. Physiol. Meas. 2016, 37, R1–R35. [Google Scholar] [CrossRef]
- Agostinelli, A.; Grillo, M.; Biagini, A.; Giuliani, C.; Burattini, L.; Fioretti, S.; Di Nardo, F.; Giannubilo, S.R.; Ciavattini, A.; Burattini, L. Noninvasive Fetal Electrocardiography: An Overview of the Signal Electrophysiological Meaning, Recording Procedures, and Processing Techniques. Ann. Noninvasive Electrocardiol. Off. J. Int. Soc. Holter Noninvasive Electrocardiol. Inc. 2015, 20, 303–313. [Google Scholar] [CrossRef]
- Keenan, E.; Karmakar, C.; Brownfoot, F.C.; Palaniswami, M. Personalised anatomic modeling for non-invasive fetal ECG: Methodology and applications. Eee Trans. Instrum. Meas. 2021, 70, 4004312. [Google Scholar] [CrossRef]
- Keenan, E.; Karmakar, C.K.; Palaniswami, M. The effects of asymmetric volume conductor modeling on non-invasive fetal ECG extraction. Physiol. Meas. 2018, 39, 105013. [Google Scholar] [CrossRef] [PubMed]
- Bhogal, K. Focus on cardiotocography: Intrapartum monitoring of uterine contractions. Br. J. Midwifery 2017, 25, 491–497. [Google Scholar] [CrossRef]
- Euliano, T.Y.; Nguyen, M.T.; Marossero, D.; Edwards, R.K. Monitoring Contractions in Obese Parturients: Electrohysterography Compared With Traditional Monitoring. Obstet. Gynecol. 2007, 109, 1136–1140. [Google Scholar] [CrossRef] [PubMed]
- Wilmink, F.A.; Wilms, F.F.; Heydanus, R.; Mol, B.W.J.; Papatsonis, D.N.M. Fetal complications after placement of an intrauterine pressure catheter: A report of two cases and review of the literature. J. Matern.-Fetal Neonatal Med. 2008, 21, 880–883. [Google Scholar] [CrossRef]
- Cohen, W.R. Clinical assessment of uterine contractions. Int. J. Gynecol. Obstet. 2017, 139, 137–142. [Google Scholar] [CrossRef]
- Ayres-de Campos, D.; Bernardes, J.; Garrido, A.; Marques-de Sá, J.; Pereira-Leite, L. Sisporto 2.0: A program for automated analysis of cardiotocograms. J. Matern.-Fetal Med. 2000, 9, 311–318. [Google Scholar]
- Ayres-de Campos, D.; Sousa, P.; Costa, A.; Bernardes, J. Omniview-SisPorto® 3.5—A central fetal monitoring station with online alerts based on computerised cardiotocogram+ST event analysis. J. Perinat. Med. 2008, 36, 260–264. [Google Scholar] [CrossRef]
- Ayres-de Campos, D.; Rei, M.; Nunes, I.; Sousa, P.; Bernardes, J. SisPorto 4.0—Computer analysis following the 2015 FIGO Guidelines for intrapartum fetal monitoring. J. Matern.-Fetal Neonatal Med. 2017, 30, 62–67. [Google Scholar] [CrossRef]
- Nunes, I.; Ayres-de Campos, D.; Ugwumadu, A.; Amin, P.; Banfield, P.; Nicoll, A.; Cunningham, S.; Sousa, P.; Costa-Santos, C.; Bernardes, J.; et al. Central Fetal Monitoring With and Without Computer Analysis: A Randomised Controlled Trial. Obstet. Gynecol. 2017, 129, 83. [Google Scholar] [CrossRef]
- Balayla, J.; Shrem, G. Use of artificial intelligence (AI) in the interpretation of intrapartum fetal heart rate (FHR) tracings: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2019, 300, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Campanile, M.; D’Alessandro, P.; Della Corte, L.; Saccone, G.; Tagliaferri, S.; Arduino, B.; Esposito, G.; Esposito, F.G.; Raffone, A.; Signorini, M.G.; et al. Intrapartum cardiotocography with and without computer analysis: A systematic review and meta-analysis of randomised controlled trials. J. Matern.-Fetal Neonatal Med. 2020, 33, 2284–2290. [Google Scholar] [CrossRef] [PubMed]
- Campos, D.; Bernardes, J. Cardiotocography. UCI Machine Learning Repository. 2010. Available online: https://archive.ics.uci.edu/dataset/193/cardiotocography (accessed on 10 July 2023). [CrossRef]
- Chudáček, V.; Spilka, J.; Burša, M.; Janků, P.; Hruban, L.; Huptych, M.; Lhotská, L. Open access intrapartum CTG database. BMC Pregnancy Childbirth 2014, 14, 16. [Google Scholar] [CrossRef] [PubMed]
- Spencer, J.A.; Belcher, R.; Dawes, G.S. The influence of signal loss on the comparison between computer analyses of the fetal heart rate in labour using pulsed Doppler ultrasound (with autocorrelation) and simultaneous scalp electrocardiogram. Eur. J. Obstet. Gynecol. Reprod. Biol. 1987, 25, 29–34. [Google Scholar] [CrossRef]
- Jezewski, J.; Wrobel, J.; Matonia, A.; Horoba, K.; Martinek, R.; Kupka, T.; Jezewski, M. Is Abdominal Fetal Electrocardiography an Alternative to Doppler Ultrasound for FHR Variability Evaluation? Front. Physiol. 2017, 8, 305. [Google Scholar] [CrossRef] [PubMed]
- Gudivada, V.; Apon, A.; Ding, J. Data Quality Considerations for Big Data and Machine Learning: Going Beyond Data Cleaning and Transformations. Int. J. Adv. Softw. 2017, 10, 1–20. [Google Scholar]
- Chudácčk, V.; Huptych, M.; Koucký, M.; Spilka, J.; Bauer, L.; Lhotská, L. Fetal heart rate data pre-processing and annotation. In Proceedings of the 2009 9th International Conference on Information Technology and Applications in Biomedicine, Larnaka, Cyprus, 4–7 November 2009; pp. 1–4, ISSN: 2168–2208. [Google Scholar] [CrossRef]
- Zhao, Z.; Deng, Y.; Zhang, Y.; Zhang, Y.; Zhang, X.; Shao, L. DeepFHR: Intelligent prediction of fetal Acidemia using fetal heart rate signals based on convolutional neural network. BMC Med. Inform. Decis. Mak. 2019, 19, 286. [Google Scholar] [CrossRef]
- Petrozziello, A.; Jordanov, I.; Aris Papageorghiou, T.; Christopher Redman, W.G.; Georgieva, A. Deep Learning for Continuous Electronic Fetal Monitoring in Labor. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Honolulu, HI, USA, 18–21 July 2018; Volume 2018, pp. 5866–5869. [Google Scholar] [CrossRef]
- Cömert, Z.; Yang, Z.; Velappan, S.; Boopathi, A.M.; Kocamaz, A.F. Performance evaluation of Empirical Mode Decomposition and Discrete Wavelet Transform for computerised hypoxia detection and prediction. In Proceedings of the 2018 26th Signal Processing and Communications Applications Conference (SIU), Izmir, Turkey, 2–5 May 2018; pp. 1–4. [Google Scholar] [CrossRef]
- Liang, S.; Li, Q. Automatic Evaluation of Fetal Heart Rate Based on Deep Learning. In Proceedings of the 2021 2nd Information Communication Technologies Conference (ICTC), Nanjing, China, 7–9 May 2021; pp. 235–240. [Google Scholar] [CrossRef]
- Krupa, B.N.; Ali, M.A.M.; Zahedi, E. The application of empirical mode decomposition for the enhancement of cardiotocograph signals. Physiol. Meas. 2009, 30, 729–743. [Google Scholar] [CrossRef]
- Oikonomou, V.P.; Spilka, J.; Stylios, C.; Lhostka, L. An adaptive method for the recovery of missing samples from FHR time series. In Proceedings of the Proceedings of the 26th IEEE International Symposium on Computer-Based Medical Systems, Porto, Portugal, 20–22 June 2013; pp. 337–342, ISSN: 1063–7125. [CrossRef]
- Fuentealba, P.; Illanes, A.; Ortmeier, F. Cardiotocograph Data Classification Improvement by Using Empirical Mode Decomposition*. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 5646–5649, ISSN: 1558–4615. [Google Scholar] [CrossRef]
- O’Sullivan, M.; Gabruseva, T.; Boylan, G.; O’Riordan, M.; Lightbody, G.; Marnane, W. Classification of fetal compromise during labour: Signal processing and feature engineering of the cardiotocograph. In Proceedings of the 2021 29th European Signal Processing Conference (EUSIPCO), Dublin, Ireland, 23–27 August 2021; pp. 1331–1335, ISSN: 2076–1465. [Google Scholar] [CrossRef]
- Lear, C.A.; Galinsky, R.; Wassink, G.; Yamaguchi, K.; Davidson, J.O.; Westgate, J.A.; Bennet, L.; Gunn, A.J. The myths and physiology surrounding intrapartum decelerations: The critical role of the peripheral chemoreflex. J. Physiol. 2016, 594, 4711–4725. [Google Scholar] [CrossRef]
- Chudáček, V.; Spilka, J.; Janků, P.; Koucký, M.; Lhotská, L.; Huptych, M. Automatic evaluation of intrapartum fetal heart rate recordings: A comprehensive analysis of useful features. Physiol. Meas. 2011, 32, 1347–1360. [Google Scholar] [CrossRef]
- Cazares, S.; Moulden, M.; Redman, C.W.G.; Tarassenko, L. Tracking poles with an autoregressive model: A confidence index for the analysis of the intrapartum cardiotocogram. Med. Eng. Phys. 2001, 23, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Georgieva, A.; Payne, S.J.; Moulden, M.; Redman, C.W.G. Artificial neural networks applied to fetal monitoring in labour. Neural Comput. Appl. 2013, 22, 85–93. [Google Scholar] [CrossRef]
- Spilka, J.; Frecon, J.; Leonarduzzi, R.; Pustelnik, N.; Abry, P.; Doret, M. Sparse Support Vector Machine for Intrapartum Fetal Heart Rate Classification. IEEE J. Biomed. Health Inform. 2017, 21, 664–671. [Google Scholar] [CrossRef]
- Furuya, N.; Hasegawa, J.; Imai, H.; Homma, C.; Kurasaki, A.; Kondo, H.; Suzuki, N. Accuracy of predicting neonatal distress using a five-level classification of fetal heart rate monitoring. J. Obstet. Gynaecol. Res. 2020, 47, 254–261. [Google Scholar] [CrossRef]
- Georgoulas, G.; Stylios, C.; Nokas, G.; Groumpos, P. Classification of fetal heart rate during labour using hidden Markov models. In Proceedings of the 2004 IEEE International Joint Conference on Neural Networks (IEEE Cat. No.04CH37541), Budapest, Hungary, 25–29 July 2004; Volume 3, pp. 2471–2475, ISSN: 1098–7576. [Google Scholar] [CrossRef]
- Signorini, M.; Magenes, G.; Cerutti, S.; Arduini, D. Linear and nonlinear parameters for the analysisof fetal heart rate signal from cardiotocographic recordings. IEEE Trans. Biomed. Eng. 2003, 50, 365–374. [Google Scholar] [CrossRef]
- Gonçalves, H.; Bernardes, J.; Paula Rocha, A.; Ayres-de Campos, D. Linear and nonlinear analysis of heart rate patterns associated with fetal behavioral states in the antepartum period. Early Hum. Dev. 2007, 83, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol.-Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef]
- Ferrario, M.; Signorini, M.; Magenes, G. Complexity analysis of the fetal heart rate for the identification of pathology in fetuses. In Proceedings of the Computers in Cardiology, Lyon, France, 25–28 September 2005; pp. 989–992, ISSN: 2325–8853. [Google Scholar] [CrossRef]
- Georgieva, A.; Papageorghiou, A.; Payne, S.; Moulden, M.; Redman, C. Phase-rectified signal averaging for intrapartum electronic fetal heart rate monitoring is related to acidaemia at birth. Bjog Int. J. Obstet. Gynaecol. 2014, 121, 889–894. [Google Scholar] [CrossRef]
- Spilka, J.; Chudáček, V.; Koucký, M.; Lhotská, L.; Huptych, M.; Janků, P.; Georgoulas, G.; Stylios, C. Using nonlinear features for fetal heart rate classification. Biomed. Signal Process. Control 2012, 7, 350–357. [Google Scholar] [CrossRef]
- Georgoulas, G.; Stylios, D.; Groumpos, P. Predicting the risk of metabolic acidosis for newborns based on fetal heart rate signal classification using support vector machines. IEEE Trans. Biomed. Eng. 2006, 53, 875–884. [Google Scholar] [CrossRef]
- Dash, S.; Quirk, J.G.; Djurić, P.M. Fetal Heart Rate Classification Using Generative Models. IEEE Trans. Biomed. Eng. 2014, 61, 2796–2805. [Google Scholar] [CrossRef] [PubMed]
- Krupa, N.; MA, M.A.; Zahedi, E.; Ahmed, S.; Hassan, F.M. Antepartum fetal heart rate feature extraction and classification using empirical mode decomposition and support vector machine. Biomed. Eng. Online 2011, 10, 6. [Google Scholar] [CrossRef]
- Afridi, R.; Iqbal, Z.; Khan, M.; Ahmad, A.; Naseem, R. Fetal Heart Rate Classification and Comparative Analysis Using Cardiotocography Data and Known Classifiers. Int. J. Grid Distrib. Comput. 2019, 12, 31–42. [Google Scholar] [CrossRef]
- Cömert, Z.; Kocamaz, A. Evaluation of Fetal Distress Diagnosis during Delivery Stages based on Linear and Nonlinear Features of Fetal Heart Rate for Neural Network Community. Int. J. Comput. Appl. 2016, 156, 26–31. [Google Scholar] [CrossRef]
- Cömert, Z.; Kocamaz, A. A Study Based on Gray Level Co-Occurrence Matrix and Neural Network Community for Determination of Hypoxic Fetuses. In Proceedings of the International Artificial Intelligence and Data Processing Symposium, Malatya, Turkey, 17–18 September 2016. [Google Scholar]
- Cömert, Z.; Kocamaz, A. Comparison of Machine Learning Techniques for Fetal Heart Rate Classification. Acta Phys. Pol. A 2017, 132, 451–454. [Google Scholar] [CrossRef]
- Georgoulas, G.; Stylios, C.; Groumpos, P. Classification of fetal heart rate using scale dependent features and support vector machines. IFAC Proc. Vol. 2005, 38, 313–318. [Google Scholar] [CrossRef]
- Kiranyaz, S.; Avci, O.; Abdeljaber, O.; Ince, T.; Gabbouj, M.; Inman, D.J. 1D convolutional neural networks and applications: A survey. Mech. Syst. Signal Process. 2021, 151, 107398. [Google Scholar] [CrossRef]
- Li, J.; Chen, Z.Z.; Huang, L.; Fang, M.; Li, B.; Fu, X.; Wang, H.; Zhao, Q. Automatic Classification of Fetal Heart Rate Based on Convolutional Neural Network. IEEE Internet Things J. 2019, 6, 1394–1401. [Google Scholar] [CrossRef]
- Yefei, Z.; Yanjun, D.; Xiaohong, Z.; Lihuan, S.; Zhidong, Z. Bidirectional Long Short-term Memory-based Intelligent Auxiliary Diagnosis of Fetal Health. In Proceedings of the 2021 IEEE Region 10 Symposium (TENSYMP), Jeju, Republic of Korea, 23–25 August 2021; pp. 1–5, ISSN: 2642–6102. [Google Scholar] [CrossRef]
- He, H.; Garcia, E.A. Learning from Imbalanced Data. IEEE Trans. Knowl. Data Eng. 2009, 21, 1263–1284. [Google Scholar] [CrossRef]
- Georgieva, A.; Moulden, M.; Redman, C.W.G. Umbilical cord gases in relation to the neonatal condition: The EveREst plot. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 168, 155–160. [Google Scholar] [CrossRef]
- Malin, G.L.; Morris, R.K.; Khan, K.S. Strength of association between umbilical cord pH and perinatal and long term outcomes: Systematic review and meta-analysis. BMJ Br. Med. J. 2010, 340, 1121. [Google Scholar] [CrossRef]
- Wen, J.; Thibeau-Sutre, E.; Diaz-Melo, M.; Samper-González, J.; Routier, A.; Bottani, S.; Dormont, D.; Durrleman, S.; Burgos, N.; Colliot, O. Convolutional neural networks for classification of Alzheimer’s disease: Overview and reproducible evaluation. Med. Image Anal. 2020, 63, 101694. [Google Scholar] [CrossRef] [PubMed]
- Cheong-See, F.; Allotey, J.; Marlin, N.; Mol, B.; Schuit, E.; ter Riet, G.; Riley, R.; Moons, K.; Khan, K.; Thangaratinam, S. Prediction models in obstetrics: Understanding the treatment paradox and potential solutions to the threat it poses. Bjog Int. J. Obstet. Gynaecol. 2016, 123, 1060–1064. [Google Scholar] [CrossRef] [PubMed]
- Romagnoli, S.; Sbrollini, A.; Burattini, L.; Marcantoni, I.; Morettini, M.; Burattini, L. Annotation dataset of the cardiotocographic recordings constituting the “CTU-CHB intra-partum CTG database”. Data Brief 2020, 31, 105690. [Google Scholar] [CrossRef] [PubMed]
- Abry, P.; Spilka, J.; Leonarduzzi, R.; Chudáček, V.; Pustelnik, N.; Doret, M. Sparse learning for Intrapartum fetal heart rate analysis. Biomed. Phys. Eng. Express 2018, 4, 034002. [Google Scholar] [CrossRef]
- Georgieva, A.; Abry, P.; Chudáček, V.; Djurić, P.M.; Frasch, M.G.; Kok, R.; Lear, C.A.; Lemmens, S.N.; Nunes, I.; Papageorghiou, A.T.; et al. Computer-based intrapartum fetal monitoring and beyond: A review of the 2nd Workshop on Signal Processing and Monitoring in Labor (October 2017, Oxford, UK). Acta Obstet. Gynecol. Scand. 2019, 98, 1207–1217. [Google Scholar] [CrossRef]
- Georgieva, A.; Abry, P.; Nunes, I.; Frasch, M.G. Editorial: Fetal-maternal monitoring in the age of artificial intelligence and computer-aided decision support: A multidisciplinary perspective. Front. Pediatr. 2022, 10, 1007799. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Signal Format | Outcome Data | Number of Recordings | Availability |
|---|---|---|---|---|
| UCI ML Repository [80] | FHR and UC features only | Three classes: Normal (N) Suspect (S) Pathological (P) | 2126 N = 1655 S = 295 P = 176 | Public |
| CTU-UHB Dataset [81] | Raw FHR and UC at 4 Hz | pH | 552 | Public |
| Lyon Dataset [38] | Raw FHR and UC at 10 Hz | pH | 1288 | Private |
| Oxford Dataset [37] | Raw FHR and UC at 4 Hz | pH | 35,429 | Private |
| Year | Authors | Segment Selection | Artefact Removal | Signal Interpolation | Downsampling Frequency | Smoothing and Detrending |
|---|---|---|---|---|---|---|
| 2013, 2014 | Spilka et al. [35,36] | Not specified | FHR < 50 bpm or FHR > 210 bpm corrected Long gaps > 15 s not included | Hermite spline | None | None |
| 2016 | Stylios et al. [39] | Last 30 min of 1st stage of labour | Not specified | Hermite spline | None | None |
| 2017 | Georgoulas et al. [40] | Not specified | FHR < 50 bpm or FHR > 200 bpm corrected Long gaps > 15 s not included | Hermite spline | None | None |
| 2018 | Cömert and Kocamaz [47] | Last 15 min of 2nd stage of labour | FHR < 50 bpm or FHR > 200 bpm corrected Long gaps > 15 s not included | Cubic Hermite spline | None | None |
| 2018 | Petrozziello et al. [87] | Last 60 min of labour | Not specified | Linear | None | None |
| 2018 | Zhao et al. [43] | Not specified | Adjacent 5 FHR values with variability < 10 bpm and signal with zeros for >10 s not included FHR ≤ 50 bpm or FHR ≥ 200 bpm corrected FHR values with differences in adjacent values exceeding 25 bpm corrected | Linear and spline | None | None |
| 2018 | Cömert et al. [44] | Last 30 min of 1st stage of labour | Outliers and artefacts corrected | Cubic spline | None | Detrending: 2nd order polynomial |
| 2018 | Cömert et al. [88] | Last part of the 1st stage of labour | Long gaps > 15 s not included Outliers corrected | Cubic Hermite spline | None | Smoothing: Median filter Detrending: Not specified |
| 2019 | Fuentealba et al. [92] | Last 25 min of labour | FHR < 50 bpm or FHR > 200 bpm corrected | Hermite spline | None | None |
| 2019 | Petrozziello et al. [37] | Last 60 min regardless of labour stage | Not specified | Linear | 0.25 Hz | None |
| 2019 | Zhao et al. [45,86] | Not specified | FHR < 50 bpm or FHR > 200 bpm corrected Long gaps >15 s not included FHR values with differences in adjacent values exceeding 25 bpm are corrected | Linear and cubic spline | None | None |
| 2021 | Liang and Li [89] | Last 30 min of labour | FHR< 50 bpm or FHR > 200 bpm corrected Long gaps >15 s not included | Hermite spline | 1 Hz | Smoothing: Median filter |
| 2021 | Liu et al. [46] | Last 20 min of FHR | FHR < 50 bpm or FHR > 200 bpm corrected Long gaps > 15 s not included FHR values with differences in adjacent values exceeding 25 bpm are corrected | Linear and Hermite spline | 1 Hz | None |
| 2021 | O’Sullivan et al. [93] | Not specified | FHR < 50 bpm or FHR > 210 bpm are corrected Patients with more than 30% traces missing are removed from the study FHR values with a change greater than 30% from the moving average are corrected | Not specified | None | None |
| Year | Authors | Datasets | Classification Criteria (Denoting All Unhealthy Classes as Compromised and Healthy Classes as Normal) | Number of Recordings |
|---|---|---|---|---|
| 2013 | Spilka et al. [35] | CTU-UHB | pH ≤ 7.05 as Compromised | Total = 552 Normal = 508 Compromised = 44 |
| 2013 | Georgieva et al. [97] | Subset of Oxford Dataset | Training: 7.27 < pH < 7.33 as Normal pH < 7.1 as Compromised Testing: 7.22 < pH < 7.27 as Normal pH < 7.1 as Compromised | Training set: Total = 124 Normal = 62 Compromised = 62 Testing set: Total = 252 Normal = 126 Compromised = 126 |
| 2016 | Spilka et al. [38] | Lyon Dataset CTU-UHB | pH ≤ 7.05 as Compromised | Training: Lyon DB Total = 1288 Normal = 1251 Compromised = 37 Testing: CTU-UHB Total = 420 Normal = 400 Compromised = 20 |
| 2016 | Stylios et al. [39] | CTU-UHB | pH ≤ 7.05 as Compromised | Total = 552 Normal = 508 Compromised = 44 |
| 2017 | Georgoulas et al. [40] | CTU-UHB | pH ≤ 7.05 as Compromised | Total = 552 Normal = 508 Compromised = 44 |
| 2017 | Spilka et al. [98] | Lyon Dataset | pH ≤ 7.05 as Compromised | Total = 1288 Normal = 1251 Compromised = 37 |
| 2018 | Cömert and Kocamaz [47] | CTU-UHB | pH < 7.2 as Compromised | Total = 552 Normal = 375 Compromised = 177 |
| 2018 | Feng et al. [41] | CTU-UHB | pH > 7.2 as Normal pH < 7.1 as Compromised | Total = 447 Normal = 358 Compromised = 62 |
| 2018 | Petrozziello et al. [87] | Oxford Dataset | pH < 7.05 as Compromised | Total = 35,429 Normal = 33,959 Compromised = 1470 |
| 2018 | Zhao et al. [43] | CTU-UHB | pH < 7.15 as Compromised | Total = 552 Normal = 447 Compromised = 105 |
| 2018 | Cömert et al. [44] | CTU-UHB | pH ≤ 7.15 as Compromised | Total = 552 Normal = 439 Compromised = 113 |
| 2018 | Cömert et al. [88] | CTU-UHB | pH ≤ 7.15 as Compromised | Total = 552 Normal = 439 Compromised = 113 |
| 2019 | Fuentealba et al. [92] | CTU-UHB | pH > 7.2 and BDecf < 12 as Normal pH < 7.05 and BDecf ≥ 12 as Compromised | Total = 372 Normal = 354 Compromised = 18 |
| 2019 | Petrozziello et al. [37] | Oxford Dataset CTU-UHB Lyon Dataset | Normal: pH ≥ 7.15 Severe Compromise: pH < 7.05 and a composite outcome of stillbirth; neonatal death; neonatal encephalopathy; intubation or cardiac massage followed by admission to neonatal intensive care for ≥ 48 h Moderate Compromise: pH < 7.05 Intermediate: 7.05 ≤ pH < 7.15 | Oxford Dataset Training: 30,115 Testing: 4429 Normal = 4249 Moderate/Severe compromise with pH < 7.05 = 180 Testing: CTU-UHB Total = 552 Normal = 512 Compromised = 40 |
| 2019 | Zhao et al. [86] | CTU-UHB | pH ≥ 7.15 as Normal pH < 7.15 as Compromised | Normal = 447, Compromised = 105 After CWT: Normal = 2682 Compromised = 630 |
| 2019 | Zhao et al. [45] | CTU-UHB | pH < 7.15 as Compromised | Normal = 105, Compromised = 105 After RP 2D: Normal = 21,000 Compromised = 21,000 |
| 2020 | Furuya et al. [99] | Private | 5-min Apgar score < 8 or pH < 7.1 as Compromised | Total = 1301 Normal = 1184 Compromised = 117 |
| 2021 | Liang and Li [89] | CTU-UHB | pH ≤ 7.05 as Compromised | Total = 552 Normal = 508 Compromised = 44 |
| 2021 | Liu et al. [46] | CTU-UHB | pH ≤ 7.15 as Compromised | Total = 552 Normal = 439 Compromised = 113 |
| 2021 | O’Sullivan et al. [93] | CTU-UHB | pH ≥ 7.15 and Apgar 5 ≥ 9 as Normal pH ≤ 7.0 or Apgar 5 ≤ 6 as Compromised | Total = 333 Normal = 310 Compromised = 23 |
| Computerised Method | Strengths | Limitations | Computational Cost | |
|---|---|---|---|---|
| Features | Morphological and Time Domain | Macroscopic features suitable for visual inspection Recognised clinical value for several features | Some features based on statistical computation with no direct link to fetal physiology | NA |
| Frequency Domain | Capture periodic trends in FHR variations | Difficult to observe via visual inspective Sensitive to artefacts Does not identify non-periodic trends in FHR variations | ||
| Non-Linear | Quantify complex non-periodic variations of FHR | Sensitive to artefacts Values depend on the choice of parameters Some highly depend on the FHR signal length | ||
| Classical Machine Learning | Internal operation is more easily understandable | Human involvement needed for feature extraction and selection | Low–High | |
| ML Classifiers | Adaboost | Reduces the risk of overfitting by combining multiple weak classifiers | Computationally expensive due to the iterative nature of the algorithm | Medium |
| ANN | Learns complex relationships among features | Prone to overfitting when a higher number of layers used | Medium | |
| Bayesian Models | Can incorporate prior knowledge and domain expertise through prior distributions | Computationally expensive for large datasets | High | |
| Decision Trees | Easy to interpret and visualise | Prone to overfitting if not properly regularised | Low | |
| Deep Gaussian Processes | Can learn complex, non-linear relationships | Can be challenging to interpret and visualise Computationally expensive for large datasets | High | |
| Logistic Regression | Simple and efficient Provides probabilistic outputs useful for interpretation | May not capture complex interactions between features | Low | |
| Random Forest | Robust against overfitting due to ensemble of decision trees | Computationally expensive for large datasets | Medium | |
| SVM | Effective in high-dimensional spaces Works well on small datasets Can handle linear and non-linear decision boundaries | Can be sensitive to the choice of kernel function and hyperparameters Computationally expensive for large datasets | Medium | |
| Deep Learning | Feature extraction and selection are not needed Learns complex features from raw data | Lack of interpretability and transparency of operation High computational complexity | High | |
| DL Classifiers | CNN | Reduces the complexity of the model by weight sharing and subsampling | Does not learn global relationships Requires more training samples for generalisation | High |
| LSTM | Widely used for time series forecasting Learns temporal features | Takes longer time to train Requires more training samples for generalisation | Higher | |
| Metric Name | Equation | Description |
|---|---|---|
| Accuracy (Acc) | The simple ratio between the number of correctly predicted points to the total number of points (probability of correct predictions) Not suitable for imbalanced datasets | |
| Sensitivity (Se) | The proportion of the correctly predicted positive instances from the total positive instances | |
| Specificity (Sp) | The proportion of the correctly predicted negative instances from the total negative instances | |
| Precision | The proportion of the correctly predicted positive instances from the total classified positive instances | |
| Geometric mean (g − mean) | Measure of the balance between classification performances in both the majority and minority classes | |
| Harmonic mean (F − measure) | A measure of the effectiveness of classification | |
| Matthew’s correlation coefficient (MCC) | Minimally influenced by imbalanced data, the correlation coefficient between the observed and predicted classifications (range from −1 to +1), +1: perfect prediction 0: no better than random prediction −1: worst prediction | |
| Area under the receiver operating characteristic curve (AUC) | Plot of the true positive rate vs. the false positive rate at all possible thresholds | Higher the AUC, the better the performance of the model at distinguishing between the classes Used to compare and evaluate different classification algorithms |
| Year | Authors | Training Method | Sensitivity (%) | Specificity (%) | AUC | Independent Test/Train Data | Complete CTU-UHB at Threshold pH < 7.05 or pH ≤ 7.05 |
|---|---|---|---|---|---|---|---|
| 2013 | Spilka et al. [35] | ID: FHR features augmented by SMOTE CT: Nearest mean classifier with AdaBoost CV: 44-fold | 64.00 | 65.00 | Not specified | Yes | Yes |
| 2014 | Spilka et al. [36] | ID: FHR features CT: RF CV: 2-fold repeated 5 times | 72.00 | 78.00 | Not specified | Yes | No, subset of dataset used and labelled using clinical annotations. |
| 2016 | Cömert and Kocamaz [112] | ID: FHR features CT: ANN CV: 5-fold | 88.70 | 85.10 | Not specified | Yes | No, subset of 100 records randomly chosen. |
| 2016 | Cömert and Kocamaz [111] | ID: FHR features CT: ANN, for 3 stages of labour CV: 10-fold | I = 95.89 II = 87.06 III = 85.87 | I = 74.75 II = 75.90 III = 72.73 | Not specified | Yes | No, complete dataset used but labelled using clinical annotations. |
| 2016 | Spilka et al. [38] | ID: FHR features CT: Sparse SVM CV: Train—Lyon Dataset, Test—CTU-UHB | 40.00 | 86.00 | 0.79 | Yes | No, subset of dataset which has less than 50% signal loss. |
| 2016 | Stylios et al. [39] | ID: FHR features CT: LS SVM with RBF kernel CV: 44-fold repeated 15 times | 68.50 | 77.70 | Not specified | Yes | Yes |
| 2017 | Georgoulas et al. [40] | ID: FHR features CT: LS SVM CV: 44-fold | 72.12 | 65.30 | Not specified | Yes | Yes |
| 2018 | Cömert and Kocamaz [47] | ID: FHR features CT: ANN, SVM, k-NN CV: 10-fold repeated 30 times | ANN = 68.52 SVM = 76.83 k-NN = 53.28 | ANN = 70.29 SVM = 78.27 k-NN = 66.80 | ANN = 0.76 SVM = 0.84 k-NN = 0.64 | Yes | No, complete dataset used but with compromise defined by pH < 7.2. |
| 2018 | Feng et al. [41] | ID: FHR and UC features CT: Supervised two-layer DGP network CV: No CV but repeated 5 times | FHR = 73.00 FHR+UC = 91.00 | FHR = 91.00 FHR+UC = 82.00 | Not specified | Yes | No, subset of dataset used with compromise defined by pH < 7.1. |
| 2018 | Petrozziello et al. [87] | ID: Raw FHR and UC CT: CNN, LSTM CV: Train—Oxford dataset, Test—CTU-UHB | Not specified | Not specified | CNN = 0.82 LSTM = 0.81 | Yes | Yes |
| 2018 | Zhao et al. [43] | ID: FHR features CT: AdaBoost CV: 10-fold CV | 92.00 | 90.00 | 0.91 | No, unclear whether data samples have been used multiple times. | No, complete dataset used with compromise defined by pH < 7.15. |
| 2018 | Cömert et al. [44] | ID: FHR features CT: LS SVM with RBF kernel CV: 10-fol repeated 100 times | 63.45 | 65.88 | 0.65 | Yes | No, complete dataset used with compromise defined by pH < 7.15. |
| 2018 | Cömert et al. [88] | ID: FHR features CT: SVM with RBF kernel CV: 10-fold repeated 30 times | 57.42 | 70.11 | Not specified | Yes | No, complete dataset used with compromise defined by pH < 7.15. |
| 2019 | Petrozziello et al. [37] | ID: Raw FHR and UC, FHR quality score CT: MCNN, stacked MCNN CV: Train—Oxford dataset, Test—CTU-UHB | MCNN * 33.00 48.00 58.00 65.00 Stacked MCNN * 33.00 45.00 58.00 65.00 | MCNN * 95.00 90.00 85.00 80.00 Stacked MCNN * 95.00 90.00 85.00 80.00 | MCNN = 0.81 Stacked MCNN = 0.82 | Yes | Yes |
| 2019 | Zhao et al. [86] | ID: Raw FHR transformed to 2D using CWT CT: 8-layer CNN CV: 10-fold | 98.22 | 94.84 | 0.97 | No, data augmented before data split. | No, complete dataset used with compromise defined by pH < 7.15. |
| 2019 | Zhao et al. [45] | ID: Raw FHR transformed to 2D image using RP CT: 8-layer CNN CV: 10-fold | 99.29 | 98.1 | 0.98 | No, data augmented before data split. | No, subset of dataset used with compromise defined by pH < 7.15. |
| 2021 | Liang and Li [89] | ID: Raw FHR CT: CNN based on a weighted voting mechanism CV: No CV but holdout test set | 80.93 | 79.85 | 0.90 | Yes | No, performance is reported on a small holdout set of the dataset. |
| 2021 | Liu et al. [46] | ID: Raw FHR CT: CNN + BiLSTM + Attention + DWT CV: 10-fold repeated 10 times | 75.23 | 70.82 | Not specified | Yes | No, complete dataset used with compromise defined by pH < 7.15. |
| 2021 | O’Sullivan et al. [93] | ID: FHR and UC features, EHR, duration of stage I and II labour CT: Logistic regression CV: 5-fold | 82.60 | 77.70 | 0.81 | Yes | No, subset of dataset used with compromise defined by pH < 7.0 or Apgar ≤ 6. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendis, L.; Palaniswami, M.; Brownfoot, F.; Keenan, E. Computerised Cardiotocography Analysis for the Automated Detection of Fetal Compromise during Labour: A Review. Bioengineering 2023, 10, 1007. https://doi.org/10.3390/bioengineering10091007
Mendis L, Palaniswami M, Brownfoot F, Keenan E. Computerised Cardiotocography Analysis for the Automated Detection of Fetal Compromise during Labour: A Review. Bioengineering. 2023; 10(9):1007. https://doi.org/10.3390/bioengineering10091007
Chicago/Turabian StyleMendis, Lochana, Marimuthu Palaniswami, Fiona Brownfoot, and Emerson Keenan. 2023. "Computerised Cardiotocography Analysis for the Automated Detection of Fetal Compromise during Labour: A Review" Bioengineering 10, no. 9: 1007. https://doi.org/10.3390/bioengineering10091007