
Artificial Intelligence Applications for Osteoporosis Classification Using Computed Tomography
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
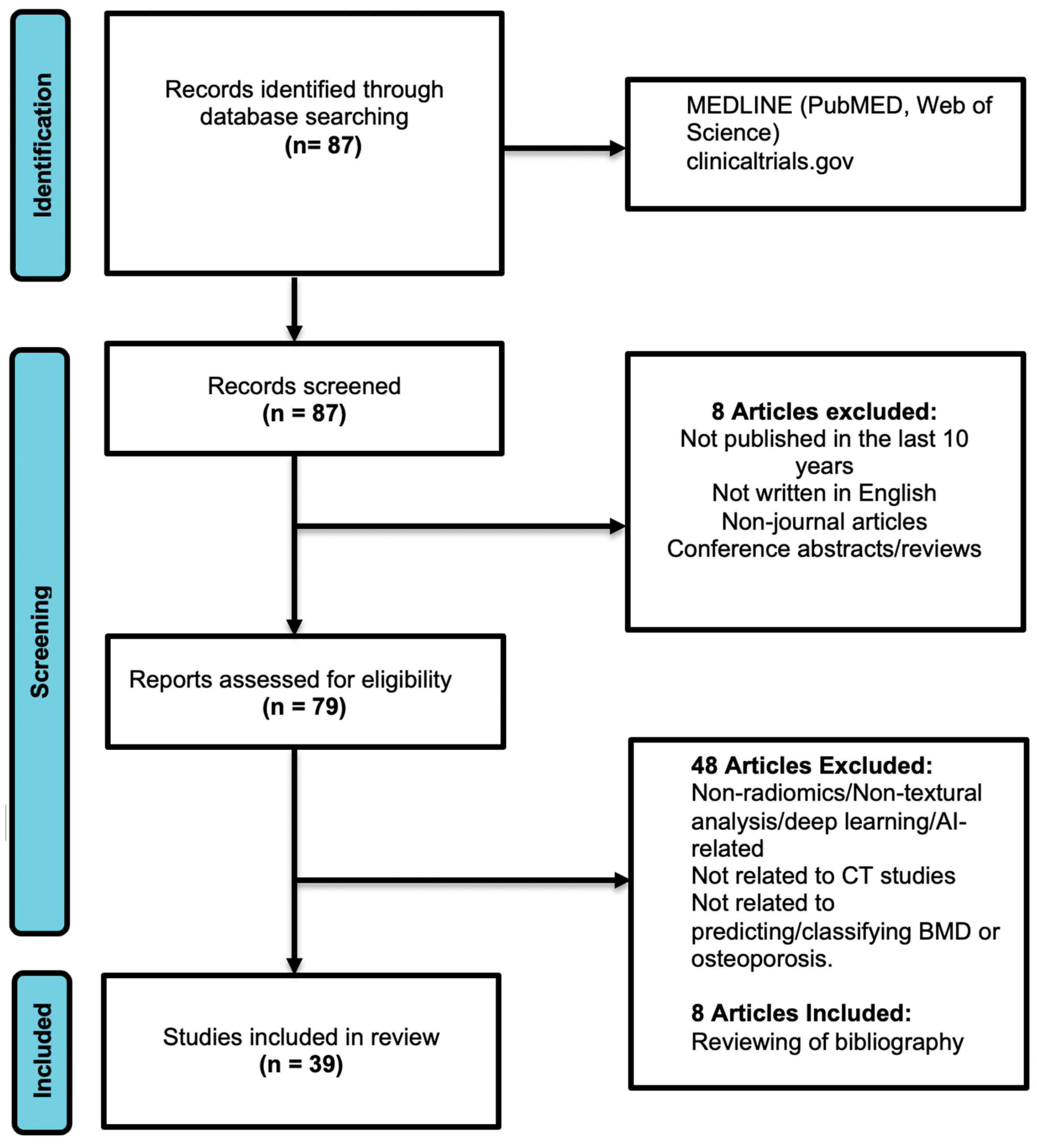
2.1. Literature Search Strategy
2.2. Study Screening and Selection Criteria
2.3. Data Extraction and Reporting
- Research article details: complete authorship, date of journal or publication, and journal name;
- Main clinical use: classify osteoporosis (either normal vs. abnormal BMD or normal vs. osteopenia vs. osteoporosis);
- Research study details: type of study, patient or imaging modality, body parts scanned, and area of bone segmented for analysis (e.g., internal or external data sets);
- Machine learning techniques used: radiomics, artificial or convolutional neural networks, etc.;
- Performance compared with DEXA: for example, the sensitivity, specificity, accuracy, correlation coefficients, and AUCs were obtained when possible.
3. Results
3.1. Search Results
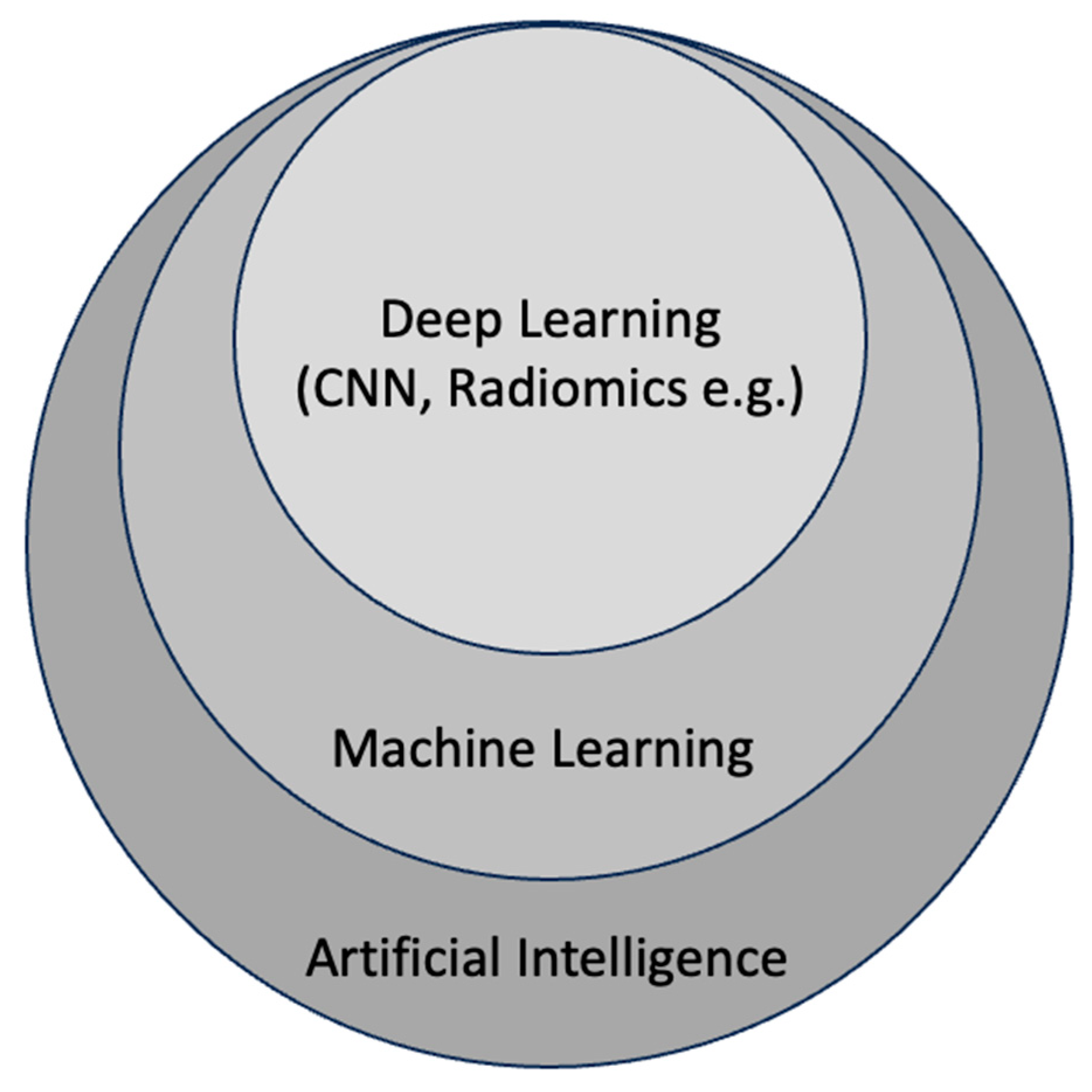
3.2. Artificial Intelligence
3.3. Machine Learning, Deep Learning, and Radiomics
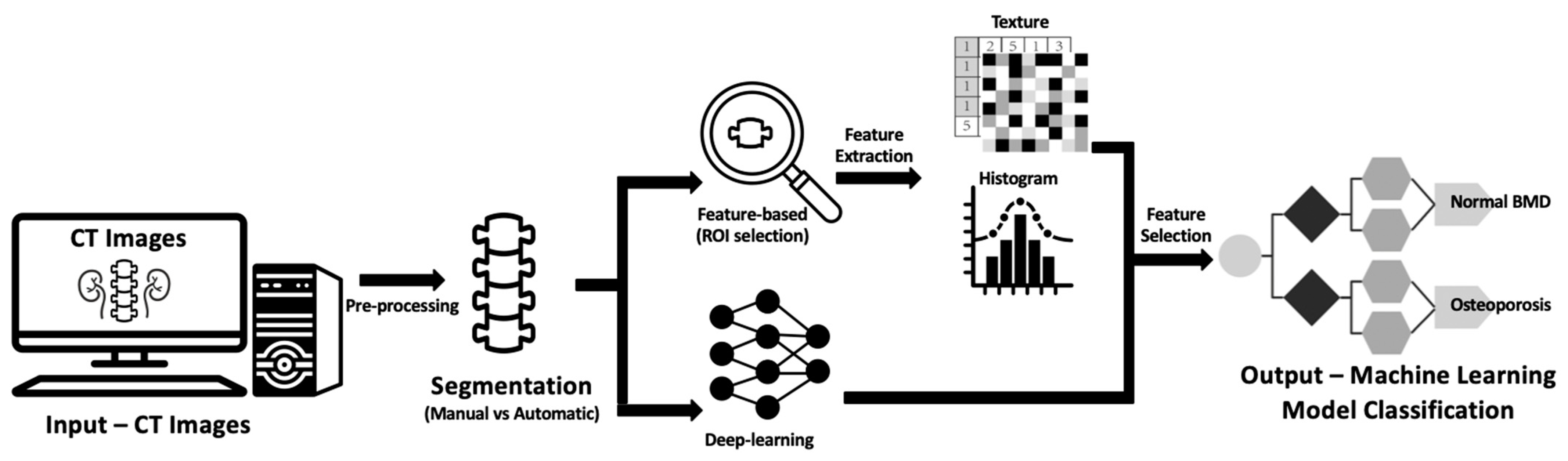
3.4. General Workflow of BMD Classification in CT
- Phantom-Based Calibration: This method involves placing phantoms containing known densities (such as dipotassium phosphate or calcium hydroxyapatite density rods) beneath the subject during scan acquisition [62,101]. These phantoms are used to calibrate measured HU values to BMD through linear equations. One challenge is that phantom placement is not routinely performed in clinical CT scans [102]. However, this challenge can be overcome by scanning the density phantom asynchronously using the same scanner and scan protocol but without the patient present.
- Phantomless Internal Calibration: In this approach, the HU peak values of internal reference regions, such as skeletal muscle and adipose tissue, are used. The reference BMD density values for these internal references are determined using phantom-calibrated scans from a cohort of patients [103]. These values are then extrapolated to create a standard calibration curve for converting the trabecular HU to BMD [104,105] through scan-specific equations.
- Feature-Based Imaging Feature Analysis: This approach involves manually extracting various features and incorporating them into a training set for AI-based imaging classification [117].
- Deep Learning-Based Analysis (e.g., CNNs): CNNs employ deep learning to automatically extract valuable imaging features by learning patterns directly from input images [118]. This enables the detection and processing of distinct diagnostic patterns and imaging features that go beyond what a human reader can accomplish [120], potentially improving BMD classification.

{kind=link}
{kind=link}
{kind=link}
| Authors | Artificial Intelligence Method | Publication Year | Main Objectives | Title of Journal | Main Type of CT | Areas Sampled | Performance |
|---|---|---|---|---|---|---|---|
| Yasaka K. et al. [66] | CNN | 2020 | Predict osteoporosis | European Radiology | Unenhanced CT of abdomen | L1 vertebra | r = 0.852 (p < 0.001), AUC = 0.965 (internal validation) 0.840 (p < 0.001), AUC = 0.970 (external validation) |
| Kang J.W. et al. [61] | ResNet-101v2, CNN | 2023 | Classify osteoporosis | Frontiers in Physiology | Unenhanced CT of abdomen | L1 vertebra | r = 0.900 F1 score = 0.875 |
| Uemura K. et al. [120] | Computer-aided system | 2023 | Classify osteoporosis | Archives of Osteoporosis | Unenhanced CT of abdomen | Axial slice of the L1 vertebra (L1-vBMD) Axial slices of L1–L4 (CT-vBMD) Coronal L1–L4 (CT-aBMD) | r = 0.364, AUC = 0.582 (L1-vBMD); r = 0.456, AUC = 0.657 (CT-vBMD); r = 0.911, AUC = 0.941 (CT-aBMD) |
| Savage R.H. et al. [121] | Wavelet features, AdaBoost, and local geometry constraints | 2020 | Classify osteoporosis | Journal of Thoracic Imaging | Unenhanced CT of thorax | Thoracic vertebrae | Moderate correlation, r = 0.55 (p < 0.001) Significant difference between normal control patients and osteoporotic group (p = 0.045) |
| Pickhardt P.J. et al. [101] | CNN (U-Net, TernausNet) | 2022 | Classify osteoporosis | Radiology | CT of abdomen | L1 bone (one to seven slices) | AUC = 0.860–0.930 Sensitivity: 85.4%–94.0%; Specificity: 94.6%–98.3%. Accuracy: 89.0%–94.0% |
| Fang Y. et al. [95] | CNN (DenseNet-121), U-Net | 2021 | Classify osteoporosis | European Radiology | CT of abdomen and CT of spine | L1–L4 vertebrae | r > 0.980 (p < 0.001) Cohen’s kappa = 0.868–0.888) |
| Pan Y. et al. [122] | U-Net | 2020 | Classify osteoporosis | European Radiology | Low-dose CT of thorax | T1–L2 vertebrae | r = 0.964–0.968 Mean errors: 2.2–4.0 mg/cm AUC = 0.927 (osteoporosis), 0.942 (low BMD) |
| Tang C. et al. [123] | CNN (MS-Net, BMDC-Net) | 2021 | Classify osteoporosis | Osteoporosis International | CT of abdomen or lumbar spine | L1 vertebra | Accuracy: 76.7% AUC = 0.917 |
| Dzierżak, R. et al. [93] | Deep CNN (VGG16, VGG19, MobileNetV2, Xception, ResNet50, and InceptionResNetV2 | 2022 | Classify osteoporosis | Sensors | CT of lumbosacral spine | L1 vertebra | AUC = 0.883–0.973 Accuracy: 84.0%–95.0% Sensitivity: 78.0%–96.0% Specificity: 86.0%–98.0% |
| Breit H.C. et al. [124] | CNN | 2023 | Classify osteoporosis | European Journal of Radiology | Non-contrast CT of thorax | Thoracic vertebrae | r = 0.51, p < 0.001 (hip BMD); r = 0.34, p = 0.01 (lumbar spine BMD) Accuracy: 75.0%, Sensitivity: 93.0%, Specificity: 61.0%; Significantly better than clinical reports |
| Summers R.M. et al. [125] | Computer-aided Software (QCT Pro software, versions 3.2, 4 or 4.1) | 2011 | Classify osteoporosis | Journal of Computer Assisted Tomography | CT, colonoscopy | L1–L2 vertebrae | r = 0.980 (p < 0.0001) 95% limits of agreement were (−9.79, 8.46) mg/cc |
| Valentinitsch, A. et al. [126] | RF classifier | 2019 | Classify osteoporosis | Osteoporosis International | CT of thoracolumbar spine | Thoracolumar vertebrae | AUC = 0.71–0.88 |
| Sebro R. et al. [103] | Naïve Bayes; RF; SVM; XGBoost | 2023 | Classify osteoporosis | Journal of Neuroradiology | CT of cervical spine | C1–T1 vertebrae | AUC = 0.622–0.843 Accuracy: 74.6%–99.4% Sensitivity: 85.0%–100% Specificity: 56.7%–98.5% |
| Sebro R. et al. [127] | (LASSO), Elastic Net, Ridge regression, and SVM with RBF | 2022 | Prediction of osteoporosis | European Journal of Radiology | CT of thorax | Ribs, thoracic vertebrae, sternum, and clavicle | r > 0.4, p < 0.001 AUC = 0.702–0.757 |
| Liu et al. [128] | LR, SVM with RBF, ANN, RF, eXtreme Gradient Boosting and Stacking | 2022 | Classify osteoporosis | BMC Bioinformatics | CT images covering lumbar vertebral bodies | L1–L4 vertebrae | AUC = 0.818–0.962 Accuracy: 86.6%–96.0% Sensitivity: 71.6%–96.4% Specificity: 91.6%–96.0% |
| Pan J. et al. [100] | ResNet-101 residual DCNN classification model | 2023 | Classify osteoporosis | Research Square | CT of thorax | L1–L2 vertebrae, L1 vertebra | AUC = 0.940–0.990 Accuracy: 86.6%–94.7% Sensitivity: 63.8%–97.6% Specificity: 83.8%–93.0% |
| Lim H.K. et al. [129] | Aquarius iNtuition v4.4.121, TeraRecon, Medip, RF | 2021 | Classify osteoporosis | PloS ONE | Unenhanced CT of abdomen and pelvis | Left femur | AUC = 0.959–0.960 Accuracy: 92.7%–92.9%; Sensitivity: 80.0%–86.6%; Specificity: 94.5%–95.8%; |
| Zhang K. et al. [130] | CNN | 2023 | Classify osteoporosis | Computational Intelligence and Neuroscience | CT images covering lumbar vertebral bodies | L1–L2 vertebra | AUC = 0.965–0.985 Accuracy: 93.3%–97.1% Sensitivity: 83.6%–96.4% Specificity: 92.2%–97.6% |
| Nam K.H. et al. [131] | MR, LR. Tensor flow and Python | 2019 | Classify osteoporosis | Journal of Korean Neurosurgical Society | CT of lumbar spine | L1–L3 vertebra | AUC = 0.900 Accuracy: 92.5% F1 score: 0.954; |
| Xu Y. et al. [132] | SVM and kNN | 2013 | Classify osteoporosis | Microscopy Research Technique | Micro-CT | - | F1 score: 0.900–0.958 Precision: 91.3%–95.3% |
| Löffler, M.T. et al. [98] | CNN | 2021 | Classify osteoporosis | European Radiology | CT of lumbar spine | L1–L4 | AUC = 0.860–0.885 Sensitivity: 41.0%–86.0% Specificity: 78.0%–98.0% (superior to DXA for predicting osteoporosis in patients with vertebral fractures |
| Krishnaraj A. et al. [133] | Machine learning-based regression | 2019 | Classify osteoporosis | Journal of American College of Radiology | CT of abdomen and pelvis | L1–L4 vertebrae | Accuracy: 82.0%; Sensitivity: 84.4%; Specificity: 72.7% |
| Chen Y.C. et al. [134] | CNN (ResNet50), SVM | 2023 | Classify osteoporosis | European Radiology | Low-dose CT of thorax | Thoracic vertebrae | AUC = 0.960–0.980 Accuracy: 85.0%–95.0% Sensitivity: 85.0%–94.0% Specificity: 85.0%–92.0% |
| Tariq A. et al. [135] | CNN (Densenet121) | 2023 | Classify osteoporosis | Medical Physics | Contrasted/non-contrasted CT of abdomen and pelvis | L3 vertebrae | AUC = 0.830 (axial), 0.830 (coronal), 0.860 (imaging + demographic factors) |
| Elmahdy, M. et al. [94] | SVM with RBF | 2023 | Classify osteoporosis | Studies in Health Technology and Informatics | CT of knee | Distal femur, proximal tibia and fibula, and patella | AUC = 0.937 Sensitivity: 83.3% Specificity: 100.0% |
| Sollmann N. et al. [136] | CNN (DenseNet) | 2022 | Classify osteoporosis | Journal of Bone Mineral Research | CT of abdomen and pelvis | T6 to L5 vertebrae | AUC = 0.815–0.862 |
| Yang J. et al. [69] | CNN | 2022 | Classify osteoporosis | Osteoporosis International | CT of thorax | Thoracic vertebrae | AUC = 0.831–0.972 Sensitivity: 73.8%–95.6% Specificity: 73.6%–88.0% |
| Sebro R. et al. [137] | SVM with RBF | 2022 | Classify osteoporosis | Diagnostics | CT of wrist/forearm | Forearm, carpal, and metacarpal bones | AUC = 0.818 (radius) Sensitivity: 69.2% Specificity: 77.1% r = 0.74–0.85 |
| Yoshida K. et al. [138] | CNN (ResNet50) | 2023 | Classify osteoporosis | Journal Computer Assisted Tomography | Non-contrasted CT images covering lumbar vertebral bodies | L1–L4 vertebrae | AUC = 0.921–0.969 r = 0.81 Accuracy: 73.0%–94.0% Sensitivity: 73.0%–100% Specificity: 73.0%–94.0% |
| Dai H. et al. [139] | LASSO regression model | 2023 | Classify osteoporosis | Acta Radiological | CT of abdomen | Lumbar vertebrae | r = 0.932 |
| Huang C.B. et al. [96] | LASSO, GNB, RF, LR, SVM, GBM, XGBoost | 2022 | Classify osteoporosis | BMC Geriatrics | CT of abdomen | Psoas at L3 level | AUC = 0.860 Accuracy: 81.0% Sensitivity: 70.0%, Specificity 92.0% |
| Naghavi M. et al. [140] | CNN (Unet) | 2023 | Classify osteoporosis | Journal of the American College of Radiology | CT, coronary artery calcium scoring | Thoracic vertebrae | r = 0.84 AutoBMD averaged 15 s per report vs. 5.5 min for manual measurements (p < 0.0001). |
| Naghavi M. et al. [99] | CNN (Unet) | 2023 | Classify osteoporosis | European Journal of Radiology Open | Low-dose CT of thorax, CT, coronary artery calcium scoring | Thoracic vertebrae | R2 = 0.95 (p < 0.0001) Similar results in both modalities |
| Küçükçiloğlu Y. et al. [97] | CNN (InceptionV, EfficientNetV2S, ResNet50 | 2023 | Classify osteoporosis | Diagnostic Interventional Radiology | CT of lumbar spine MRI of lumbar spine | Lumbar vertebrae |
AUC = 0.942–0.988(CT) Accuracy: 98.8% (CT) Sensitivity: 98.5% (CT) Specificity: 99.2% (CT) AUC = 0.980 (CT + MRI) Accuracy: 96.8% (CT + MRI) Sensitivity: 96.7% (CT + MRI) Specificity: 96.8% (CT + MRI) |
| Wang J. et al. [104] | PyRadiomics, LASSO | 2023 | Classify osteoporosis | BMC Musculoskeletal Disorder | CT of lumbar spine | L1 vertebra |
AUC = 0.902–0.988 Accuracy: 86.0%–94.0% Sensitivity: 85.7%–87.5% Specificity: 80.0%–97.2% |
| Jiang, Y.W. et al. [105] | mRMR, LASSO | 2022 | Detect osteoporosis | European Radiology | CT of lumbar spine | L1 vertebra |
AUC = 0.762–0.969 Accuracy: 75.9%–87.1% Sensitivity: 59.5%–73.0% Specificity: 83.5%–93.7% |
| Xue Z. et al. [141] | PyRadiomics, SVM, RF, KNN | 2022 | Detect osteoporosis | BMC Musculoskeletal Disorder | CT of lumbar spine | L1–L4 vertebrae |
AUC = 0.994 (normal vs. osteoporosis) AUC = 0.866 (osteopenia vs. osteoporosis) AUC = 0.940 (normal vs. osteopenia) |
| Qiu H. et al. [142] | mRMR, LASSO | 2022 | Detect osteoporosis | Frontiers in Endocrinology | CT covering lumbar vertebra bodies | Paravertebral muscles at the level of the L1 vertebra |
AUC = 0.900 (radiomics); 0.950 (radiomics + clinical features) Accuracy: 81.4%–88.1% Sensitivity: 85.7%–88.9% Specificity: 77.4%–87.5% |
| Mookiah M.R.K. et al. [143] | SVM | 2018 | Classify osteoporosis | Osteoporosis International | CT images covering thoracolumbar spine | Thoracolumbar spine |
Accuracy: 83.0% Sensitivity: 93.3% Specificity: 79.3% r = 0.91–0.96 |
| Areas Sampled | No. of Studies | Area under the Curve (AUC) | Accuracy | Sensitivity | Specificity | r |
|---|---|---|---|---|---|---|
| Cervical vertebrae | 1 | 0.622–0.843 | 74.6%–99.4% | 85.0%–100% | 56.7%–98.5% | 0.270–0.670 |
| Thoracic vertebrae | 6 | 0.831–0.980 | 85.0%–95.0% | 73.8%–95.6% | 73.6%–92.0% | 0.34 0–0.510 |
| Thoracolumbar vertebrae | 4 | 0.710–0.952 | 83.0% | 93.0% | 79.3% | 0.910–0.968 |
| Lumbar vertebrae | 21 | 0.582–0.994 | 73.0%–98.8% | 41.0%–100% | 73.0%–99.2% | 0.582–0.911 |
| Other regions | 7 | 0.630–0.960 | 61.8%–92.9% | 61.8%–95.0% | 31.0%–100% | 0.400–0.600 |
| Overall | 39 | 0.582–0.994 | 61.8%–99.4% | 41.0%–100% | 31.0%–100% | 0.270–0.968 |
4. Discussion
4.1. Advantages and Efficacy
4.1.1. Technical Considerations: Labeling and Segmentation
4.1.2. Technical Considerations: Contrast versus Non-Contrast
4.1.3. Technical Considerations: Areas Sampled
4.2. Other Potential Applications: Incorporating Molecular and Genetic Biomarkers
4.3. Challenges in Implementation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ensrud, K.E.; Crandall, C.J. Osteoporosis. Ann. Intern. Med. 2017, 167, itc17–itc32. [Google Scholar] [CrossRef]
- Salari, N.; Ghasemi, H.; Mohammadi, L.; Behzadi, M.h.; Rabieenia, E.; Shohaimi, S.; Mohammadi, M. The global prevalence of osteoporosis in the world: A comprehensive systematic review and meta-analysis. J. Orthop. Surg. Res. 2021, 16, 609. [Google Scholar] [CrossRef]
- Xiao, P.L.; Cui, A.Y.; Hsu, C.J.; Peng, R.; Jiang, N.; Xu, X.H.; Ma, Y.G.; Liu, D.; Lu, H.D. Global, regional prevalence, and risk factors of osteoporosis according to the World Health Organization diagnostic criteria: A systematic review and meta-analysis. Osteoporos. Int. 2022, 33, 2137–2153. [Google Scholar] [CrossRef] [PubMed]
- Center, J.R.; Nguyen, T.V.; Schneider, D.; Sambrook, P.N.; Eisman, J.A. Mortality after all major types of osteoporotic fracture in men and women: An observational study. Lancet 1999, 353, 878–882. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Atkinson, E.J.; Jacobsen, S.J.; O’Fallon, W.M.; Melton, L.J., 3rd. Population-based study of survival after osteoporotic fractures. Am. J. Epidemiol. 1993, 137, 1001–1005. [Google Scholar] [CrossRef] [PubMed]
- Melton, L.J., 3rd. Adverse outcomes of osteoporotic fractures in the general population. J. Bone Miner. Res. 2003, 18, 1139–1141. [Google Scholar] [CrossRef] [PubMed]
- D’Elia, R.; Iannazzo, S.; Rossigni, A.; Santi, A.L.; Patti, A.M. Osteoporosis: Problems and considerations of economical nature. Ann. Ig. 2004, 16, 59–67. [Google Scholar]
- Dunnewind, T.; Dvortsin, E.P.; Smeets, H.M.; Konijn, R.M.; Bos, J.H.J.; de Boer, P.T.; van den Bergh, J.P.; Postma, M.J. Economic Consequences and Potentially Preventable Costs Related to Osteoporosis in the Netherlands. Value Health 2017, 20, 762–768. [Google Scholar] [CrossRef]
- Kelly, R.R.; McDonald, L.T.; Jensen, N.R.; Sidles, S.J.; LaRue, A.C. Impacts of Psychological Stress on Osteoporosis: Clinical Implications and Treatment Interactions. Front. Psychiatry 2019, 10, 200. [Google Scholar] [CrossRef]
- Gold, D.T. The nonskeletal consequences of osteoporotic fractures. Psychologic and social outcomes. Rheum. Dis. Clin. N. Am. 2001, 27, 255–262. [Google Scholar] [CrossRef]
- Gold, T.; Williams, S.A.; Weiss, R.J.; Wang, Y.; Watkins, C.; Carroll, J.; Middleton, C.; Silverman, S. Impact of fractures on quality of life in patients with osteoporosis: A US cross-sectional survey. J. Drug Assess. 2019, 8, 175–183. [Google Scholar] [CrossRef]
- Singer, A.; McClung, M.R.; Tran, O.; Morrow, C.D.; Goldstein, S.; Kagan, R.; McDermott, M.; Yehoshua, A. Treatment rates and healthcare costs of patients with fragility fracture by site of care: A real-world data analysis. Arch. Osteoporos. 2023, 18, 42. [Google Scholar] [CrossRef]
- Williams, S.A.; Chastek, B.; Sundquist, K.; Barrera-Sierra, S.; Leader, D., Jr.; Weiss, R.J.; Wang, Y.; Curtis, J.R. Economic burden of osteoporotic fractures in US managed care enrollees. Am. J. Manag. Care 2020, 26, e142–e149. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.I.; Hinton, P.S. Physical activity and bone health. Mo. Med. 2014, 111, 59–64. [Google Scholar] [PubMed]
- Stanghelle, B.; Bentzen, H.; Giangregorio, L.; Pripp, A.H.; Bergland, A. Associations between health-related quality of life, physical function and pain in older women with osteoporosis and vertebral fracture. BMC Geriatr. 2019, 19, 298. [Google Scholar] [CrossRef]
- Cooper, C.; Campion, G.; Melton, L.J., 3rd. Hip fractures in the elderly: A world-wide projection. Osteoporos. Int. 1992, 2, 285–289. [Google Scholar] [CrossRef]
- Porter, J.L.; Varacallo, M. Osteoporosis; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Tucci, J.R. Importance of early diagnosis and treatment of osteoporosis to prevent fractures. Am. J. Manag. Care 2006, 12, S181–S190. [Google Scholar]
- Tothill, P.; Laskey, M.A.; Orphanidou, C.I.; van Wijk, M. Anomalies in dual energy X-ray absorptiometry measurements of total-body bone mineral during weight change using Lunar, Hologic and Norland instruments. Br. J. Radiol. 1999, 72, 661–669. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Assessment of Fracture Risk and Its Application to Screening for Postmenopausal Osteoporosis: Report of a WHO Study Group; meeting held in Rome from 22 to 25 June 1992; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Kanis, J.A.; Melton, L.J., 3rd; Christiansen, C.; Johnston, C.C.; Khaltaev, N. The diagnosis of osteoporosis. J. Bone Miner. Res. 1994, 9, 1137–1141. [Google Scholar] [CrossRef]
- Sheu, A.; Diamond, T. Bone mineral density: Testing for osteoporosis. Aust. Prescr. 2016, 39, 35–39. [Google Scholar] [CrossRef]
- Varacallo, M.; Seaman, T.J.; Jandu, J.S.; Pizzutillo, P. Osteopenia; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kanis, J. Assessment of Osteoporosis at the Primary Health-Care Level. Technical Report. 2008. Available online: http://www.shef.ac.uk/FRAX (accessed on 21 August 2023).
- Adams, J.E. Quantitative computed tomography. Eur. J. Radiol. 2009, 71, 415–424. [Google Scholar] [CrossRef]
- Cummings, S.R.; Bates, D.; Black, D.M. Clinical use of bone densitometry: Scientific review. JAMA 2002, 288, 1889–1897. [Google Scholar] [CrossRef] [PubMed]
- Nayak, S.; Roberts, M.S.; Greenspan, S.L. Cost-effectiveness of different screening strategies for osteoporosis in postmenopausal women. Ann. Intern. Med. 2011, 155, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Kling, J.M.; Clarke, B.L.; Sandhu, N.P. Osteoporosis prevention, screening, and treatment: A review. J. Womens Health 2014, 23, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Ito, K. Cost-effectiveness of Screening for Osteoporosis in Older Men With a History of Falls. JAMA Netw. Open 2020, 3, e2027584. [Google Scholar] [CrossRef] [PubMed]
- Small, R.E. Uses and limitations of bone mineral density measurements in the management of osteoporosis. Medscape Gen. Med. 2005, 7, 3. [Google Scholar]
- Miller, P.D.; Zapalowski, C.; Kulak, C.A.; Bilezikian, J.P. Bone densitometry: The best way to detect osteoporosis and to monitor therapy. J. Clin. Endocrinol. Metab. 1999, 84, 1867–1871. [Google Scholar] [CrossRef]
- Curtis, J.R.; Carbone, L.; Cheng, H.; Hayes, B.; Laster, A.; Matthews, R.; Saag, K.G.; Sepanski, R.; Tanner, S.B.; Delzell, E. Longitudinal trends in use of bone mass measurement among older americans, 1999–2005. J. Bone Min. Res. 2008, 23, 1061–1067. [Google Scholar] [CrossRef]
- Gillespie, C.W.; Morin, P.E. Trends and Disparities in Osteoporosis Screening Among Women in the United States, 2008–2014. Am. J. Med. 2017, 130, 306–316. [Google Scholar] [CrossRef]
- Siris, E.S.; Chen, Y.T.; Abbott, T.A.; Barrett-Connor, E.; Miller, P.D.; Wehren, L.E.; Berger, M.L. Bone mineral density thresholds for pharmacological intervention to prevent fractures. Arch. Intern. Med. 2004, 164, 1108–1112. [Google Scholar] [CrossRef]
- Williams, S.; Khan, L.; Licata, A.A. DXA and clinical challenges of fracture risk assessment in primary care. Clevel. Clin. J. Med. 2021, 88, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Tenne, M.; McGuigan, F.; Besjakov, J.; Gerdhem, P.; Åkesson, K. Degenerative changes at the lumbar spine--implications for bone mineral density measurement in elderly women. Osteoporos. Int. 2013, 24, 1419–1428. [Google Scholar] [CrossRef]
- Grams, A.E.; Rehwald, R.; Bartsch, A.; Honold, S.; Freyschlag, C.F.; Knoflach, M.; Gizewski, E.R.; Glodny, B. Correlation between degenerative spine disease and bone marrow density: A retrospective investigation. BMC Med. Imaging 2016, 16, 17. [Google Scholar] [CrossRef]
- Chirvi, S.; Pintar, F.A.; Yoganandan, N.; Stemper, B.; Kleinberger, M. Trabecular bone mineral density correlations using QCT: Central and peripheral human skeleton. J. Mech. Behav. Biomed. Mater. 2020, 112, 104076. [Google Scholar] [CrossRef]
- Jørgensen, H.S.; Borghs, H.; Heye, S.; Smout, D.; Claes, K.; Evenepoel, P. Vascular calcification of the abdominal aorta has minimal impact on lumbar spine bone density in patients with chronic kidney disease. Bone 2022, 162, 116482. [Google Scholar] [CrossRef]
- Spencer, R.P.; Szigeti, D.P.; Engin, I.O. Effect of Laminectomy on Measured Bone Density. J. Clin. Densitom. 1998, 1, 375–377. [Google Scholar] [CrossRef]
- Jacobson, J.A.; Jamadar, D.A.; Hayes, C.W. Dual X-ray absorptiometry: Recognizing image artifacts and pathology. Am. J. Roentgenol. 2000, 174, 1699–1705. [Google Scholar] [CrossRef]
- Garg, M.K.; Kharb, S. Dual energy X-ray absorptiometry: Pitfalls in measurement and interpretation of bone mineral density. Indian. J. Endocrinol. Metab. 2013, 17, 203–210. [Google Scholar] [CrossRef]
- Vetter, J.R.; Perman, W.H.; Kalender, W.A.; Mazess, R.B.; Holden, J.E. Evaluation of a prototype dual-energy computed tomographic apparatus. II. Determination of vertebral bone mineral content. Med. Phys. 1986, 13, 340–343. [Google Scholar] [CrossRef] [PubMed]
- van Hamersvelt, R.W.; Schilham, A.M.R.; Engelke, K.; den Harder, A.M.; de Keizer, B.; Verhaar, H.J.; Leiner, T.; de Jong, P.A.; Willemink, M.J. Accuracy of bone mineral density quantification using dual-layer spectral detector CT: A phantom study. Eur. Radiol. 2017, 27, 4351–4359. [Google Scholar] [CrossRef] [PubMed]
- Booz, C.; Noeske, J.; Albrecht, M.H.; Lenga, L.; Martin, S.S.; Yel, I.; Huizinga, N.A.; Vogl, T.J.; Wichmann, J.L. Diagnostic accuracy of quantitative dual-energy CT-based bone mineral density assessment in comparison to Hounsfield unit measurements using dual x-ray absorptiometry as standard of reference. Eur. J. Radiol. 2020, 132, 109321. [Google Scholar] [CrossRef]
- Li, N.; Li, X.-M.; Xu, L.; Sun, W.-J.; Cheng, X.-G.; Tian, W. Comparison of QCT and DXA: Osteoporosis Detection Rates in Postmenopausal Women. Int. J. Endocrinol. 2013, 2013, 895474. [Google Scholar] [CrossRef]
- Alawi, M.; Begum, A.; Harraz, M.; Alawi, H.; Bamagos, S.; Yaghmour, A.; Hafiz, L. Dual-Energy X-Ray Absorptiometry (DEXA) Scan Versus Computed Tomography for Bone Density Assessment. Cureus 2021, 13, e13261. [Google Scholar] [CrossRef]
- Choi, K.Y.; Lee, S.-W.; In, Y.; Kim, M.S.; Kim, Y.D.; Lee, S.-y.; Lee, J.-W.; Koh, I.J. Dual-Energy CT-Based Bone Mineral Density Has Practical Value for Osteoporosis Screening around the Knee. Medicina 2022, 58, 1085. [Google Scholar] [CrossRef]
- Gruenewald, L.D.; Koch, V.; Martin, S.S.; Yel, I.; Eichler, K.; Gruber-Rouh, T.; Lenga, L.; Wichmann, J.L.; Alizadeh, L.S.; Albrecht, M.H.; et al. Diagnostic accuracy of quantitative dual-energy CT-based volumetric bone mineral density assessment for the prediction of osteoporosis-associated fractures. Eur. Radiol. 2022, 32, 3076–3084. [Google Scholar] [CrossRef]
- Nickoloff, E.L.; Feldman, F.; Atherton, J.V. Bone mineral assessment: New dual-energy CT approach. Radiology 1988, 168, 223–228. [Google Scholar] [CrossRef]
- de Bakker, C.M.J.; Knowles, N.K.; Walker, R.E.A.; Manske, S.L.; Boyd, S.K. Independent changes in bone mineralized and marrow soft tissues following acute knee injury require dual-energy or high-resolution computed tomography for accurate assessment of bone mineral density and stiffness. J. Mech. Behav. Biomed. Mater. 2022, 127, 105091. [Google Scholar] [CrossRef]
- Roski, F.; Hammel, J.; Mei, K.; Baum, T.; Kirschke, J.S.; Laugerette, A.; Kopp, F.K.; Bodden, J.; Pfeiffer, D.; Pfeiffer, F.; et al. Bone mineral density measurements derived from dual-layer spectral CT enable opportunistic screening for osteoporosis. Eur. Radiol. 2019, 29, 6355–6363. [Google Scholar] [CrossRef]
- Damilakis, J.; Adams, J.E.; Guglielmi, G.; Link, T.M. Radiation exposure in X-ray-based imaging techniques used in osteoporosis. Eur. Radiol. 2010, 20, 2707–2714. [Google Scholar] [CrossRef]
- Zhou, S.; Zhu, L.; You, T.; Li, P.; Shen, H.; He, Y.; Gao, H.; Yan, L.; He, Z.; Guo, Y.; et al. In vivo quantification of bone mineral density of lumbar vertebrae using fast kVp switching dual-energy CT: Correlation with quantitative computed tomography. Quant. Imaging Med. Surg. 2020, 11, 341–350. [Google Scholar] [CrossRef]
- Ghasemi Shayan, R.; Oladghaffari, M.; Sajjadian, F.; Fazel Ghaziyani, M. Image Quality and Dose Comparison of Single-Energy CT (SECT) and Dual-Energy CT (DECT). Radiol. Res. Pract. 2020, 2020, 1403957. [Google Scholar] [CrossRef]
- Brown, J.K.; Timm, W.; Bodeen, G.; Chason, A.; Perry, M.; Vernacchia, F.; DeJournett, R. Asynchronously Calibrated Quantitative Bone Densitometry. J. Clin. Densitom. 2017, 20, 216–225. [Google Scholar] [CrossRef]
- Fischer, M.; Kempers, B. Phantom studies in osteoporosis. Eur. J. Nucl. Med. 1993, 20, 434–439. [Google Scholar] [CrossRef]
- Koch, V.; Hokamp, N.G.; Albrecht, M.H.; Gruenewald, L.D.; Yel, I.; Borggrefe, J.; Wesarg, S.; Eichler, K.; Burck, I.; Gruber-Rouh, T.; et al. Accuracy and precision of volumetric bone mineral density assessment using dual-source dual-energy versus quantitative CT: A phantom study. Eur. Radiol. Exp. 2021, 5, 43. [Google Scholar] [CrossRef]
- Mussmann, B.; Andersen, P.E.; Torfing, T.; Overgaard, S. Bone density measurements adjacent to acetabular cups in total hip arthroplasty using dual-energy CT: An in vivo reliability and agreement study. Acta Radiol. Open 2018, 7, 2058460118796539. [Google Scholar] [CrossRef]
- Engelke, K.; Adams, J.E.; Armbrecht, G.; Augat, P.; Bogado, C.E.; Bouxsein, M.L.; Felsenberg, D.; Ito, M.; Prevrhal, S.; Hans, D.B.; et al. Clinical use of quantitative computed tomography and peripheral quantitative computed tomography in the management of osteoporosis in adults: The 2007 ISCD Official Positions. J. Clin. Densitom. 2008, 11, 123–162. [Google Scholar] [CrossRef]
- Kang, J.W.; Park, C.; Lee, D.E.; Yoo, J.H.; Kim, M. Prediction of bone mineral density in CT using deep learning with explainability. Front. Physiol. 2022, 13, 1061911. [Google Scholar] [CrossRef]
- Issever, A.S.; Link, T.M.; Kentenich, M.; Rogalla, P.; Schwieger, K.; Huber, M.B.; Burghardt, A.J.; Majumdar, S.; Diederichs, G. Trabecular bone structure analysis in the osteoporotic spine using a clinical in vivo setup for 64-slice MDCT imaging: Comparison to microCT imaging and microFE modeling. J. Bone Miner. Res. 2009, 24, 1628–1637. [Google Scholar] [CrossRef]
- Schreiber, J.J.; Anderson, P.A.; Rosas, H.G.; Buchholz, A.L.; Au, A.G. Hounsfield units for assessing bone mineral density and strength: A tool for osteoporosis management. J. Bone Jt. Surg. Am. 2011, 93, 1057–1063. [Google Scholar] [CrossRef]
- Park, S.H.; Jeong, Y.M.; Lee, H.Y.; Kim, E.Y.; Kim, J.H.; Park, H.K.; Ahn, H.K. Opportunistic use of chest CT for screening osteoporosis and predicting the risk of incidental fracture in breast cancer patients: A retrospective longitudinal study. PLoS ONE 2020, 15, e0240084. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Lee, S.J.; Liu, J.; Yao, J.; Lay, N.; Graffy, P.M.; Summers, R.M. Population-based opportunistic osteoporosis screening: Validation of a fully automated CT tool for assessing longitudinal BMD changes. Br. J. Radiol. 2019, 92, 20180726. [Google Scholar] [CrossRef]
- Yasaka, K.; Akai, H.; Kunimatsu, A.; Kiryu, S.; Abe, O. Prediction of bone mineral density from computed tomography: Application of deep learning with a convolutional neural network. Eur. Radiol. 2020, 30, 3549–3557. [Google Scholar] [CrossRef]
- Vadera, S.; Osborne, T.; Shah, V.; Stephenson, J.A. Opportunistic screening for osteoporosis by abdominal CT in a British population. Insights Into Imaging 2023, 14, 57. [Google Scholar] [CrossRef]
- Lenchik, L.; Weaver, A.A.; Ward, R.J.; Boone, J.M.; Boutin, R.D. Opportunistic Screening for Osteoporosis Using Computed Tomography: State of the Art and Argument for Paradigm Shift. Curr. Rheumatol. Rep. 2018, 20, 74. [Google Scholar] [CrossRef]
- Yang, J.; Liao, M.; Wang, Y.; Chen, L.; He, L.; Ji, Y.; Xiao, Y.; Lu, Y.; Fan, W.; Nie, Z.; et al. Opportunistic osteoporosis screening using chest CT with artificial intelligence. Osteoporos. Int. 2022, 33, 2547–2561. [Google Scholar] [CrossRef]
- Cheng, X.; Zhao, K.; Zha, X.; Du, X.; Li, Y.; Chen, S.; Wu, Y.; Li, S.; Lu, Y.; Zhang, Y.; et al. Opportunistic Screening Using Low-Dose CT and the Prevalence of Osteoporosis in China: A Nationwide, Multicenter Study. J. Bone Miner. Res. 2021, 36, 427–435. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Correale, L.; Hassan, C. AI-based opportunistic CT screening of incidental cardiovascular disease, osteoporosis, and sarcopenia: Cost-effectiveness analysis. Abdom. Radiol. 2023, 48, 1181–1198. [Google Scholar] [CrossRef]
- Pickhardt, P.J. Value-added Opportunistic CT Screening: State of the Art. Radiology 2022, 303, 241–254. [Google Scholar] [CrossRef]
- Gausden, E.B.; Nwachukwu, B.U.; Schreiber, J.J.; Lorich, D.G.; Lane, J.M. Opportunistic Use of CT Imaging for Osteoporosis Screening and Bone Density Assessment: A Qualitative Systematic Review. J. Bone Jt. Surg. 2017, 99, 1580–1590. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Pooler, B.D.; Lauder, T.; del Rio, A.M.; Bruce, R.J.; Binkley, N. Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications. Ann. Intern. Med. 2013, 158, 588–595. [Google Scholar] [CrossRef]
- Emohare, O.; Cagan, A.; Morgan, R.; Davis, R.; Asis, M.; Switzer, J.; Polly, D.W., Jr. The use of computed tomography attenuation to evaluate osteoporosis following acute fractures of the thoracic and lumbar vertebra. Geriatr. Orthop. Surg. Rehabil. 2014, 5, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D. Screening of Bone Density at CT: An Overlooked Opportunity. Radiology 2019, 291, 368–369. [Google Scholar] [CrossRef]
- Zhu, Y.; Triphuridet, N.; Yip, R.; Becker, B.J.; Wang, Y.; Yankelevitz, D.F.; Henschke, C.I. Opportunistic CT screening of osteoporosis on thoracic and lumbar spine: A meta-analysis. Clin. Imaging 2021, 80, 382–390. [Google Scholar] [CrossRef]
- Jang, S.; Graffy, P.M.; Ziemlewicz, T.J.; Lee, S.J.; Summers, R.M.; Pickhardt, P.J. Opportunistic Osteoporosis Screening at Routine Abdominal and Thoracic CT: Normative L1 Trabecular Attenuation Values in More than 20,000 Adults. Radiology 2019, 291, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Bott, K.N.; Matheson, B.E.; Smith, A.C.J.; Tse, J.J.; Boyd, S.K.; Manske, S.L. Addressing Challenges of Opportunistic Computed Tomography Bone Mineral Density Analysis. Diagnostics 2023, 13, 2572. [Google Scholar] [CrossRef]
- Besler, B.A.; Michalski, A.S.; Kuczynski, M.T.; Abid, A.; Forkert, N.D.; Boyd, S.K. Bone and joint enhancement filtering: Application to proximal femur segmentation from uncalibrated computed tomography datasets. Med. Image Anal. 2021, 67, 101887. [Google Scholar] [CrossRef]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef]
- Gan, H.-S.; Ramlee, M.H.; Wahab, A.A.; Lee, Y.-S.; Shimizu, A. From classical to deep learning: Review on cartilage and bone segmentation techniques in knee osteoarthritis research. Artif. Intell. Rev. 2021, 54, 2445–2494. [Google Scholar] [CrossRef]
- Fasihi, L.; Tartibian, B.; Eslami, R.; Fasihi, H. Artificial intelligence used to diagnose osteoporosis from risk factors in clinical data and proposing sports protocols. Sci. Rep. 2022, 12, 18330. [Google Scholar] [CrossRef]
- Kim, S.K.; Yoo, T.K.; Oh, E.; Kim, D.W. Osteoporosis risk prediction using machine learning and conventional methods. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 188–191. [Google Scholar] [CrossRef]
- Yoo, T.K.; Kim, S.K.; Kim, D.W.; Choi, J.Y.; Lee, W.H.; Oh, E.; Park, E.C. Osteoporosis risk prediction for bone mineral density assessment of postmenopausal women using machine learning. Yonsei Med. J. 2013, 54, 1321–1330. [Google Scholar] [CrossRef]
- Dimai, H.P. New Horizons: Artificial Intelligence Tools for Managing Osteoporosis. J. Clin. Endocrinol. Metab. 2023, 108, 775–783. [Google Scholar] [CrossRef]
- Ferizi, U.; Honig, S.; Chang, G. Artificial intelligence, osteoporosis and fragility fractures. Curr. Opin. Rheumatol. 2019, 31, 368–375. [Google Scholar] [CrossRef]
- Hsieh, C.-I.; Zheng, K.; Lin, C.; Mei, L.; Lu, L.; Li, W.; Chen, F.-P.; Wang, Y.; Zhou, X.; Wang, F.; et al. Automated bone mineral density prediction and fracture risk assessment using plain radiographs via deep learning. Nat. Commun. 2021, 12, 5472. [Google Scholar] [CrossRef]
- Lis-Studniarska, D.; Lipnicka, M.; Studniarski, M.; Irzmański, R. Applications of Artificial Intelligence Methods for the Prediction of Osteoporotic Fractures. Life 2023, 13, 1738. [Google Scholar] [CrossRef]
- Rühling, S.; Navarro, F.; Sekuboyina, A.; El Husseini, M.; Baum, T.; Menze, B.; Braren, R.; Zimmer, C.; Kirschke, J.S. Automated detection of the contrast phase in MDCT by an artificial neural network improves the accuracy of opportunistic bone mineral density measurements. Eur. Radiol. 2022, 32, 1465–1474. [Google Scholar] [CrossRef]
- Sekuboyina, A.; Husseini, M.E.; Bayat, A.; Löffler, M.; Liebl, H.; Li, H.; Tetteh, G.; Kukačka, J.; Payer, C.; Štern, D.; et al. VerSe: A Vertebrae labelling and segmentation benchmark for multi-detector CT images. Med. Image Anal. 2021, 73, 102166. [Google Scholar] [CrossRef]
- Lessmann, N.; van Ginneken, B.; de Jong, P.A.; Išgum, I. Iterative fully convolutional neural networks for automatic vertebra segmentation and identification. Med. Image Anal. 2019, 53, 142–155. [Google Scholar] [CrossRef]
- Dzierżak, R.; Omiotek, Z. Application of Deep Convolutional Neural Networks in the Diagnosis of Osteoporosis. Sensors 2022, 22, 8189. [Google Scholar] [CrossRef]
- Elmahdy, M.; Sebro, R. Opportunistic Screening for Osteoporosis Using CT Scans of the Knee: A Pilot Study. Stud. Health Technol. Inform. 2023, 302, 909–910. [Google Scholar] [CrossRef]
- Fang, Y.; Li, W.; Chen, X.; Chen, K.; Kang, H.; Yu, P.; Zhang, R.; Liao, J.; Hong, G.; Li, S. Opportunistic osteoporosis screening in multi-detector CT images using deep convolutional neural networks. Eur. Radiol. 2021, 31, 1831–1842. [Google Scholar] [CrossRef]
- Huang, C.B.; Hu, J.S.; Tan, K.; Zhang, W.; Xu, T.H.; Yang, L. Application of machine learning model to predict osteoporosis based on abdominal computed tomography images of the psoas muscle: A retrospective study. BMC Geriatr. 2022, 22, 796. [Google Scholar] [CrossRef]
- Küçükçiloğlu, Y.; Şekeroğlu, B.; Adalı, T.; Şentürk, N. Prediction of osteoporosis using MRI and CT scans with unimodal and multimodal deep-learning models. Diagn. Interv. Radiol. 2023. [Google Scholar] [CrossRef]
- Löffler, M.T.; Jacob, A.; Scharr, A.; Sollmann, N.; Burian, E.; El Husseini, M.; Sekuboyina, A.; Tetteh, G.; Zimmer, C.; Gempt, J.; et al. Automatic opportunistic osteoporosis screening in routine CT: Improved prediction of patients with prevalent vertebral fractures compared to DXA. Eur. Radiol. 2021, 31, 6069–6077. [Google Scholar] [CrossRef]
- Naghavi, M.; De Oliveira, I.; Mao, S.S.; Jaberzadeh, A.; Montoya, J.; Zhang, C.; Atlas, K.; Manubolu, V.; Montes, M.; Li, D.; et al. Opportunistic AI-enabled automated bone mineral density measurements in lung cancer screening and coronary calcium scoring CT scans are equivalent. Eur. J. Radiol. Open 2023, 10, 100492. [Google Scholar] [CrossRef]
- Pan, J.; Lin, P.-C.; Gong, S.-C.; Wang, Z.; Cao, R.; Lv, Y.; Zhang, K.; Wang, L. Effectiveness of opportunistic osteoporosis screening on chest CT using the DCNN model. BMC Musculoskelet. Disord. 2023. submitted. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Nguyen, T.; Perez, A.A.; Graffy, P.M.; Jang, S.; Summers, R.M.; Garrett, J.W. Improved CT-based Osteoporosis Assessment with a Fully Automated Deep Learning Tool. Radiol. Artif. Intell. 2022, 4, e220042. [Google Scholar] [CrossRef]
- Resmi, S.L.; Hashim, V.; Mohammed, J.; Dileep, P.N. Bone Mineral Density Prediction from CT Image: A Novel Approach using ANN. Appl. Bionics Biomech. 2023, 2023, 1123953. [Google Scholar] [CrossRef]
- Sebro, R.; De la Garza-Ramos, C. Utilizing machine learning for opportunistic screening for low BMD using CT scans of the cervical spine. J. Neuroradiol. 2023, 50, 293–301. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, S.; Chen, S.; He, Y.; Gao, H.; Yan, L.; Hu, X.; Li, P.; Shen, H.; Luo, M.; et al. Prediction of osteoporosis using radiomics analysis derived from single source dual energy CT. BMC Musculoskelet. Disord. 2023, 24, 100. [Google Scholar] [CrossRef]
- Jiang, Y.-W.; Xu, X.-J.; Wang, R.; Chen, C.-M. Radiomics analysis based on lumbar spine CT to detect osteoporosis. Eur. Radiol. 2022, 32, 8019–8026. [Google Scholar] [CrossRef]
- Sarker, I.H. Machine Learning: Algorithms, Real-World Applications and Research Directions. SN Comput. Sci. 2021, 2, 160. [Google Scholar] [CrossRef]
- Lepakshi, V.A. Machine Learning and Deep Learning based AI Tools for Development of Diagnostic Tools. In Computational Approaches for Novel Therapeutic and Diagnostic Designing to Mitigate SARS-CoV-2 Infection; Academic Press: Cambridge, MA, USA, 2022. [Google Scholar] [CrossRef]
- Rajkomar, A.; Dean, J.; Kohane, I. Machine Learning in Medicine. N. Engl. J. Med. 2019, 380, 1347–1358. [Google Scholar] [CrossRef] [PubMed]
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H. Artificial intelligence in radiology. Nat. Rev. Cancer 2018, 18, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Mun, S.K.; Wong, K.H.; Lo, S.B.; Li, Y.; Bayarsaikhan, S. Artificial Intelligence for the Future Radiology Diagnostic Service. Front. Mol. Biosci. 2020, 7, 614258. [Google Scholar] [CrossRef] [PubMed]
- Alhajeri, M.; Aldosari, H.; Aldosari, B. Evaluating latest developments in PACS and their impact on radiology practices: A systematic literature review. Inform. Med. Unlocked 2017, 9, 181–190. [Google Scholar] [CrossRef]
- Gore, J.C. Artificial intelligence in medical imaging. Magn. Reson. Imaging 2020, 68, A1–A4. [Google Scholar] [CrossRef] [PubMed]
- Doi, K. Computer-aided diagnosis in medical imaging: Historical review, current status and future potential. Comput. Med. Imaging Graph. 2007, 31, 198–211. [Google Scholar] [CrossRef]
- Nagoev, Z.V.; Sundukov, Z.A.; Pshenokova, I.A.; Denisenko, V.A. Architecture of CAD for distributed artificial intelligence based on self-organizing neuro-cognitive architectures. News Kabard. Balkar. Sci. Cent. RAS 2020, 2, 40–47. [Google Scholar] [CrossRef]
- Kriegeskorte, N. Deep Neural Networks: A New Framework for Modeling Biological Vision and Brain Information Processing. Annu. Rev. Vis. Sci. 2015, 1, 417–446. [Google Scholar] [CrossRef]
- Liu, Z.; Wang, S.; Dong, D.; Wei, J.; Fang, C.; Zhou, X.; Sun, K.; Li, L.; Li, B.; Wang, M.; et al. The Applications of Radiomics in Precision Diagnosis and Treatment of Oncology: Opportunities and Challenges. Theranostics 2019, 9, 1303–1322. [Google Scholar] [CrossRef]
- Ciresan, D.C.; Meier, U.; Masci, J.; Gambardella, L.M.; Schmidhuber, J. Flexible, high performance convolutional neural networks for image classification. In Proceedings of the Twenty-Second International Joint Conference on Artificial Intelligence, Barcelona, Spain, 16–22 July 2011. [Google Scholar]
- Zaharchuk, G.; Gong, E.; Wintermark, M.; Rubin, D.; Langlotz, C.P. Deep Learning in Neuroradiology. Am. J. Neuroradiol. 2018, 39, 1776–1784. [Google Scholar] [CrossRef] [PubMed]
- Kaka, H.; Zhang, E.; Khan, N. Artificial intelligence and deep learning in neuroradiology: Exploring the new frontier. Can. Assoc. Radiol. J. 2021, 72, 35–44. [Google Scholar] [CrossRef]
- Uemura, K.; Fujimori, T.; Otake, Y.; Shimomoto, Y.; Kono, S.; Takashima, K.; Hamada, H.; Takenaka, S.; Kaito, T.; Sato, Y.; et al. Development of a system to assess the two- and three-dimensional bone mineral density of the lumbar vertebrae from clinical quantitative CT images. Arch. Osteoporos. 2023, 18, 22. [Google Scholar] [CrossRef] [PubMed]
- Savage, R.H.; van Assen, M.; Martin, S.S.; Sahbaee, P.; Griffith, L.P.; Giovagnoli, D.; Sperl, J.I.; Hopfgartner, C.; Kärgel, R.; Schoepf, U.J. Utilizing Artificial Intelligence to Determine Bone Mineral Density Via Chest Computed Tomography. J. Thorac. Imaging 2020, 35 (Suppl. S1), S35–S39. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Shi, D.; Wang, H.; Chen, T.; Cui, D.; Cheng, X.; Lu, Y. Automatic opportunistic osteoporosis screening using low-dose chest computed tomography scans obtained for lung cancer screening. Eur. Radiol. 2020, 30, 4107–4116. [Google Scholar] [CrossRef]
- Tang, C.; Zhang, W.; Li, H.; Li, L.; Li, Z.; Cai, A.; Wang, L.; Shi, D.; Yan, B. CNN-based qualitative detection of bone mineral density via diagnostic CT slices for osteoporosis screening. Osteoporos. Int. 2021, 32, 971–979. [Google Scholar] [CrossRef]
- Breit, H.C.; Varga-Szemes, A.; Schoepf, U.J.; Emrich, T.; Aldinger, J.; Kressig, R.W.; Beerli, N.; Andreas Buser, T.; Breil, D.; Derani, I.; et al. CNN-based evaluation of bone density improves diagnostic performance to detect osteopenia and osteoporosis in patients with non-contrast chest CT examinations. Eur. J. Radiol. 2023, 161, 110728. [Google Scholar] [CrossRef]
- Summers, R.M.; Baecher, N.; Yao, J.; Liu, J.; Pickhardt, P.J.; Choi, J.R.; Hill, S. Feasibility of simultaneous computed tomographic colonography and fully automated bone mineral densitometry in a single examination. J. Comput. Assist. Tomogr. 2011, 35, 212–216. [Google Scholar] [CrossRef]
- Valentinitsch, A.; Trebeschi, S.; Kaesmacher, J.; Lorenz, C.; Löffler, M.T.; Zimmer, C.; Baum, T.; Kirschke, J.S. Opportunistic osteoporosis screening in multi-detector CT images via local classification of textures. Osteoporos. Int. 2019, 30, 1275–1285. [Google Scholar] [CrossRef]
- Sebro, R.; De la Garza-Ramos, C. Machine learning for the prediction of osteopenia/osteoporosis using the CT attenuation of multiple osseous sites from chest CT. Eur. J. Radiol. 2022, 155, 110474. [Google Scholar] [CrossRef]
- Liu, L.; Si, M.; Ma, H.; Cong, M.; Xu, Q.; Sun, Q.; Wu, W.; Wang, C.; Fagan, M.J.; Mur, L.A.J.; et al. A hierarchical opportunistic screening model for osteoporosis using machine learning applied to clinical data and CT images. BMC Bioinform. 2022, 23, 63. [Google Scholar] [CrossRef]
- Lim, H.K.; Ha, H.I.; Park, S.-Y.; Han, J. Prediction of femoral osteoporosis using machine-learning analysis with radiomics features and abdomen-pelvic CT: A retrospective single center preliminary study. PLoS ONE 2021, 16, e0247330. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Lin, P.; Pan, J.; Xu, P.; Qiu, X.; Crookes, D.; Hua, L.; Wang, L. End to End Multitask Joint Learning Model for Osteoporosis Classification in CT Images. Comput. Intell. Neurosci. 2023, 2023, 3018320. [Google Scholar] [CrossRef]
- Nam, K.H.; Seo, I.; Kim, D.H.; Lee, J.I.; Choi, B.K.; Han, I.H. Machine Learning Model to Predict Osteoporotic Spine with Hounsfield Units on Lumbar Computed Tomography. J. Korean Neurosurg. Soc. 2019, 62, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Li, D.; Chen, Q.; Fan, Y. Full supervised learning for osteoporosis diagnosis using micro-CT images. Microsc. Res. Tech. 2013, 76, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Krishnaraj, A.; Barrett, S.; Bregman-Amitai, O.; Cohen-Sfady, M.; Bar, A.; Chettrit, D.; Orlovsky, M.; Elnekave, E. Simulating Dual-Energy X-Ray Absorptiometry in CT Using Deep-Learning Segmentation Cascade. J. Am. Coll. Radiol. 2019, 16, 1473–1479. [Google Scholar] [CrossRef]
- Chen, Y.C.; Li, Y.T.; Kuo, P.C.; Cheng, S.J.; Chung, Y.H.; Kuo, D.P.; Chen, C.Y. Automatic segmentation and radiomic texture analysis for osteoporosis screening using chest low-dose computed tomography. Eur. Radiol. 2023, 33, 5097–5106. [Google Scholar] [CrossRef]
- Tariq, A.; Patel, B.N.; Sensakovic, W.F.; Fahrenholtz, S.J.; Banerjee, I. Opportunistic screening for low bone density using abdominopelvic computed tomography scans. Med. Phys. 2023, 50, 4296–4307. [Google Scholar] [CrossRef] [PubMed]
- Sollmann, N.; Löffler, M.T.; El Husseini, M.; Sekuboyina, A.; Dieckmeyer, M.; Rühling, S.; Zimmer, C.; Menze, B.; Joseph, G.B.; Baum, T.; et al. Automated Opportunistic Osteoporosis Screening in Routine Computed Tomography of the Spine: Comparison With Dedicated Quantitative CT. J. Bone Miner. Res. 2022, 37, 1287–1296. [Google Scholar] [CrossRef]
- Sebro, R.; De la Garza-Ramos, C. Machine Learning for Opportunistic Screening for Osteoporosis from CT Scans of the Wrist and Forearm. Diagnostics 2022, 12, 691. [Google Scholar] [CrossRef]
- Yoshida, K.; Tanabe, Y.; Nishiyama, H.; Matsuda, T.; Toritani, H.; Kitamura, T.; Sakai, S.; Watamori, K.; Takao, M.; Kimura, E.; et al. Feasibility of Bone Mineral Density and Bone Microarchitecture Assessment Using Deep Learning With a Convolutional Neural Network. J. Comput. Assist. Tomogr. 2023, 47, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Dai, H.; Wang, Y.; Fu, R.; Ye, S.; He, X.; Luo, S.; Jin, W. Radiomics and stacking regression model for measuring bone mineral density using abdominal computed tomography. Acta Radiol. 2023, 64, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Naghavi, M.; Atlas, K.; Jaberzadeh, A.; Zhang, C.; Manubolu, V.; Li, D.; Budoff, M. Validation of Opportunistic Artificial Intelligence-based Bone Mineral Density Measurements in Coronary Artery Calcium Scans. J. Am. Coll. Radiol. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Xue, Z.; Huo, J.; Sun, X.; Sun, X.; Ai, S.T.; Zhang, L.; Liu, C. Using radiomic features of lumbar spine CT images to differentiate osteoporosis from normal bone density. BMC Musculoskelet. Disord. 2022, 23, 336. [Google Scholar] [CrossRef] [PubMed]
- Qiu, H.; Yang, H.; Yang, Z.; Yao, Q.; Duan, S.; Qin, J.; Zhu, J. The value of radiomics to predict abnormal bone mass in type 2 diabetes mellitus patients based on CT imaging for paravertebral muscles. Front. Endocrinol. 2022, 13, 963246. [Google Scholar] [CrossRef]
- Mookiah, M.R.K.; Rohrmeier, A.; Dieckmeyer, M.; Mei, K.; Kopp, F.K.; Noel, P.B.; Kirschke, J.S.; Baum, T.; Subburaj, K. Feasibility of opportunistic osteoporosis screening in routine contrast-enhanced multi detector computed tomography (MDCT) using texture analysis. Osteoporos. Int. 2018, 29, 825–835. [Google Scholar] [CrossRef]
- Lee, S.J.; Binkley, N.; Lubner, M.G.; Bruce, R.J.; Ziemlewicz, T.J.; Pickhardt, P.J. Opportunistic screening for osteoporosis using the sagittal reconstruction from routine abdominal CT for combined assessment of vertebral fractures and density. Osteoporos. Int. 2016, 27, 1131–1136. [Google Scholar] [CrossRef]
- Johannesdottir, F.; Allaire, B.; Bouxsein, M.L. Fracture Prediction by Computed Tomography and Finite Element Analysis: Current and Future Perspectives. Curr. Osteoporos. Rep. 2018, 16, 411–422. [Google Scholar] [CrossRef]
- Dagan, N.; Elnekave, E.; Barda, N.; Bregman-Amitai, O.; Bar, A.; Orlovsky, M.; Bachmat, E.; Balicer, R.D. Automated opportunistic osteoporotic fracture risk assessment using computed tomography scans to aid in FRAX underutilization. Nat. Med. 2020, 26, 77–82. [Google Scholar] [CrossRef]
- Roux, C.; Rozes, A.; Reizine, D.; Hajage, D.; Daniel, C.; Maire, A.; Bréant, S.; Taright, N.; Gordon, R.; Fechtenbaum, J.; et al. Fully automated opportunistic screening of vertebral fractures and osteoporosis on more than 150 000 routine computed tomography scans. Rheumatology 2022, 61, 3269–3278. [Google Scholar] [CrossRef]
- Graffy, P.M.; Lee, S.J.; Ziemlewicz, T.J.; Pickhardt, P.J. Prevalence of Vertebral Compression Fractures on Routine CT Scans According to L1 Trabecular Attenuation: Determining Relevant Thresholds for Opportunistic Osteoporosis Screening. Am. J. Roentgenol. 2017, 209, 491–496. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Graffy, P.M.; Zea, R.; Lee, S.J.; Liu, J.; Sandfort, V.; Summers, R.M. Automated Abdominal CT Imaging Biomarkers for Opportunistic Prediction of Future Major Osteoporotic Fractures in Asymptomatic Adults. Radiology 2020, 297, 64–72. [Google Scholar] [CrossRef]
- Watts, N.B. The Fracture Risk Assessment Tool (FRAX®): Applications in clinical practice. J. Womens Health 2011, 20, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Turečková, A.; Tureček, T.; Komínková Oplatková, Z.; Rodríguez-Sánchez, A. Improving CT Image Tumor Segmentation Through Deep Supervision and Attentional Gates. Front. Robot. AI 2020, 7, 106. [Google Scholar] [CrossRef]
- Herrmann, P.; Busana, M.; Cressoni, M.; Lotz, J.; Moerer, O.; Saager, L.; Meissner, K.; Quintel, M.; Gattinoni, L. Using Artificial Intelligence for Automatic Segmentation of CT Lung Images in Acute Respiratory Distress Syndrome. Front. Physiol. 2021, 12, 1484. [Google Scholar] [CrossRef]
- Paudyal, R.; Shah, A.D.; Akin, O.; Do, R.K.G.; Konar, A.S.; Hatzoglou, V.; Mahmood, U.; Lee, N.; Wong, R.J.; Banerjee, S.; et al. Artificial Intelligence in CT and MR Imaging for Oncological Applications. Cancers 2023, 15, 2573. [Google Scholar] [CrossRef] [PubMed]
- Park, C.W.; Oh, S.J.; Kim, K.S.; Jang, M.C.; Kim, I.S.; Lee, Y.K.; Chung, M.J.; Cho, B.H.; Seo, S.W. Artificial intelligence-based classification of bone tumors in the proximal femur on plain radiographs: System development and validation. PLoS ONE 2022, 17, e0264140. [Google Scholar] [CrossRef]
- Ong, W.; Zhu, L.; Tan, Y.L.; Teo, E.C.; Tan, J.H.; Kumar, N.; Vellayappan, B.A.; Ooi, B.C.; Quek, S.T.; Makmur, A.; et al. Application of Machine Learning for Differentiating Bone Malignancy on Imaging: A Systematic Review. Cancers 2023, 15, 1837. [Google Scholar] [CrossRef] [PubMed]
- Hallinan, J.T.P.D.; Zhu, L.; Zhang, W.; Lim, D.S.W.; Baskar, S.; Low, X.Z.; Yeong, K.Y.; Teo, E.C.; Kumarakulasinghe, N.B.; Yap, Q.V.; et al. Deep Learning Model for Classifying Metastatic Epidural Spinal Cord Compression on MRI. Front. Oncol. 2022, 12, 1479. [Google Scholar] [CrossRef]
- Engelke, K. Quantitative Computed Tomography-Current Status and New Developments. J. Clin. Densitom. 2017, 20, 309–321. [Google Scholar] [CrossRef]
- Lee, S.; Chung, C.K.; Oh, S.H.; Park, S.B. Correlation between Bone Mineral Density Measured by Dual-Energy X-Ray Absorptiometry and Hounsfield Units Measured by Diagnostic CT in Lumbar Spine. J. Korean Neurosurg. Soc. 2013, 54, 384–389. [Google Scholar] [CrossRef]
- Wang, L.; Su, Y.; Wang, Q.; Duanmu, Y.; Yang, M.; Yi, C.; Cheng, X. Validation of asynchronous quantitative bone densitometry of the spine: Accuracy, short-term reproducibility, and a comparison with conventional quantitative computed tomography. Sci. Rep. 2017, 7, 6284. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Z.; Cai, N.; Zhou, Y.; Xiao, D. A Prediction Model for the Risk of Osteoporosis Fracture in the Elderly Based on a Neural Network. In Proceedings of the Advances in Neural Networks–ISNN 2018: 15th International Symposium on Neural Networks, ISNN 2018, Minsk, Belarus, 25–28 June 2018; Springer International Publishing: Cham, Switzerland, 2018; pp. 815–823. [Google Scholar]
- Yu, X.; Ye, C.; Xiang, L. Application of artificial neural network in the diagnostic system of osteoporosis. Neurocomputing 2016, 214, 376–381. [Google Scholar] [CrossRef]
- Beaudoin, C.; Moore, L.; Gagné, M.; Bessette, L.; Ste-Marie, L.G.; Brown, J.P.; Jean, S. Performance of predictive tools to identify individuals at risk of non-traumatic fracture: A systematic review, meta-analysis, and meta-regression. Osteoporos. Int. 2019, 30, 721–740. [Google Scholar] [CrossRef]
- Klinder, T.; Ostermann, J.; Ehm, M.; Franz, A.; Kneser, R.; Lorenz, C. Automated model-based vertebra detection, identification, and segmentation in CT images. Med. Image Anal. 2009, 13, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Anderst, W.J.; Thorhauer, E.D.; Lee, J.Y.; Donaldson, W.F.; Kang, J.D. Cervical spine bone mineral density as a function of vertebral level and anatomic location. Spine J. 2011, 11, 659–667. [Google Scholar] [CrossRef]
- Johannesdottir, F.; Allaire, B.; Kopperdahl, D.L.; Keaveny, T.M.; Sigurdsson, S.; Bredella, M.A.; Anderson, D.E.; Samelson, E.J.; Kiel, D.P.; Gudnason, V.G.; et al. Bone density and strength from thoracic and lumbar CT scans both predict incident vertebral fractures independently of fracture location. Osteoporos. Int. 2021, 32, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.S.; Henning, T.D.; Müeller, D.; Lu, Y.; Majumdar, S.; Link, T.M. Volumetric quantitative CT of the spine and hip derived from contrast-enhanced MDCT: Conversion factors. Am. J. Roentgenol. 2007, 188, 1294–1301. [Google Scholar] [CrossRef] [PubMed]
- Cummings, S.R.; Black, D.M.; Nevitt, M.C.; Browner, W.; Cauley, J.; Ensrud, K.; Genant, H.K.; Palermo, L.; Scott, J.; Vogt, T.M. Bone density at various sites for prediction of hip fractures. The Study of Osteoporotic Fractures Research Group. Lancet 1993, 341, 72–75. [Google Scholar] [CrossRef]
- Melton, L.J., 3rd; Looker, A.C.; Shepherd, J.A.; O’Connor, M.K.; Achenbach, S.J.; Riggs, B.L.; Khosla, S. Osteoporosis assessment by whole body region vs. site-specific DXA. Osteoporos. Int. 2005, 16, 1558–1564. [Google Scholar] [CrossRef]
- Kanis, J.A. Diagnosis of osteoporosis and assessment of fracture risk. Lancet 2002, 359, 1929–1936. [Google Scholar] [CrossRef] [PubMed]
- Guglielmi, G.; Muscarella, S.; Bazzocchi, A. Integrated imaging approach to osteoporosis: State-of-the-art review and update. Radiographics 2011, 31, 1343–1364. [Google Scholar] [CrossRef] [PubMed]
- Zou, D.; Li, W.; Deng, C.; Du, G.; Xu, N. The use of CT Hounsfield unit values to identify the undiagnosed spinal osteoporosis in patients with lumbar degenerative diseases. Eur. Spine J. 2019, 28, 1758–1766. [Google Scholar] [CrossRef] [PubMed]
- Oheim, R.; Tsourdi, E.; Seefried, L.; Beller, G.; Schubach, M.; Vettorazzi, E.; Stürznickel, J.; Rolvien, T.; Ehmke, N.; Delsmann, A.; et al. Genetic Diagnostics in Routine Osteological Assessment of Adult Low Bone Mass Disorders. J. Clin. Endocrinol. Metab. 2022, 107, e3048–e3057. [Google Scholar] [CrossRef] [PubMed]
- Adejuyigbe, B.; Kallini, J.; Chiou, D.; Kallini, J.R. Osteoporosis: Molecular Pathology, Diagnostics, and Therapeutics. Int. J. Mol. Sci. 2023, 24, 14583. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Camacho, P. Use of bone turnover markers in the management of osteoporosis. Curr. Opin. Endocrinol. Diabetes Obes. 2018, 25, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Biver, E.; Chopin, F.; Coiffier, G.; Brentano, T.F.; Bouvard, B.; Garnero, P.; Cortet, B. Bone turnover markers for osteoporotic status assessment? A systematic review of their diagnosis value at baseline in osteoporosis. Jt. Bone Spine 2012, 79, 20–25. [Google Scholar] [CrossRef]
- Gillett, M.J.; Vasikaran, S.D.; Inderjeeth, C.A. The Role of PINP in Diagnosis and Management of Metabolic Bone Disease. Clin. Biochem. Rev. 2021, 42, 3–10. [Google Scholar] [CrossRef]
- Greenblatt, M.B.; Tsai, J.N.; Wein, M.N. Bone Turnover Markers in the Diagnosis and Monitoring of Metabolic Bone Disease. Clin. Chem. 2017, 63, 464–474. [Google Scholar] [CrossRef]
- Kusec, V. Biochemical markers of bone turnover—Clinical application and limitations. Lijec. Vjesn. 2005, 127, 139–145. [Google Scholar]
- Lee, J.; Vasikaran, S. Current recommendations for laboratory testing and use of bone turnover markers in management of osteoporosis. Ann. Lab. Med. 2012, 32, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Bhattoa, H.P. Laboratory aspects and clinical utility of bone turnover markers. Ejifcc 2018, 29, 117–128. [Google Scholar] [PubMed]
- Shetty, S.; Kapoor, N.; Bondu, J.D.; Thomas, N.; Paul, T.V. Bone turnover markers: Emerging tool in the management of osteoporosis. Indian. J. Endocrinol. Metab. 2016, 20, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Saxena, S.; Jena, B.; Gupta, N.; Das, S.; Sarmah, D.; Bhattacharya, P.; Nath, T.; Paul, S.; Fouda, M.M.; Kalra, M.; et al. Role of Artificial Intelligence in Radiogenomics for Cancers in the Era of Precision Medicine. Cancers 2022, 14, 2860. [Google Scholar] [CrossRef]
- Bodalal, Z.; Trebeschi, S.; Nguyen-Kim, T.D.L.; Schats, W.; Beets-Tan, R. Radiogenomics: Bridging imaging and genomics. Abdom. Radiol. 2019, 44, 1960–1984. [Google Scholar] [CrossRef] [PubMed]
- Ren, M.; Yang, H.; Lai, Q.; Shi, D.; Liu, G.; Shuang, X.; Su, J.; Xie, L.; Dong, Y.; Jiang, X. MRI-based radiomics analysis for predicting the EGFR mutation based on thoracic spinal metastases in lung adenocarcinoma patients. Med. Phys. 2021, 48, 5142–5151. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Dong, Y.; Yang, H.; Chen, H.; Yu, Y.; Wang, X.; Wang, X.; Yu, T.; Luo, Y.; Jiang, X. Subregional radiomics analysis for the detection of the EGFR mutation on thoracic spinal metastases from lung cancer. Phys. Med. Biol. 2021, 66, 215008. [Google Scholar] [CrossRef]
- Xu, R.; You, T.; Liu, C.; Lin, Q.; Guo, Q.; Zhong, G.; Liu, L.; Ouyang, Q. Ultrasound-based radiomics model for predicting molecular biomarkers in breast cancer. Front. Oncol. 2023, 13, 1216446. [Google Scholar] [CrossRef]
- European Society of Radiology (ESR). The new EU General Data Protection Regulation: What the radiologist should know. Insights Imaging 2017, 8, 295–299. [Google Scholar] [CrossRef]
- Candemir, S.; Nguyen, X.V.; Folio, L.R.; Prevedello, L.M. Training Strategies for Radiology Deep Learning Models in Data-limited Scenarios. Radiol Artif Intell. 2021, 3, e210014. [Google Scholar] [CrossRef]
- Eche, T.; Schwartz, L.H.; Mokrane, F.-Z.; Dercle, L. Toward Generalizability in the Deployment of Artificial Intelligence in Radiology: Role of Computation Stress Testing to Overcome Underspecification. Radiol. Artif. Intell. 2021, 3, e210097. [Google Scholar] [CrossRef] [PubMed]
- Orlhac, F.; Boughdad, S.; Philippe, C.; Stalla-Bourdillon, H.; Nioche, C.; Champion, L.; Soussan, M.; Frouin, F.; Frouin, V.; Buvat, I. Orlhac F, Boughdad S, Philippe C, Stalla-Bourdillon H, Nioche C, Champion L, et al. A Postreconstruction Harmonization Method for Multicenter Radiomic Studies in PET. J. Nucl. Med. 2018, 59, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.E.W.; Pollard, T.J.; Shen, L.; Lehman, L.-w.H.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Celi, L.A.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef] [PubMed]
- Olson, R.S.; La Cava, W.; Orzechowski, P.; Urbanowicz, R.J.; Moore, J.H. PMLB: A large benchmark suite for machine learning evaluation and comparison. BioData Min. 2017, 10, 36. [Google Scholar] [CrossRef] [PubMed]
- Harutyunyan, H.; Khachatrian, H.; Kale, D.C.; Ver Steeg, G.; Galstyan, A. Multitask learning and benchmarking with clinical time series data. Sci. Data 2019, 6, 96. [Google Scholar] [CrossRef]
- van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging-“how-to” guide and critical reflection. Insights Imaging 2020, 11, 91. [Google Scholar] [CrossRef]
- Kotter, E.; Ranschaert, E. Challenges and solutions for introducing artificial intelligence (AI) in daily clinical workflow. Eur. Radiol. 2021, 31, 5–7. [Google Scholar] [CrossRef]
- Recht, M.P.; Dewey, M.; Dreyer, K.; Langlotz, C.; Niessen, W.; Prainsack, B.; Smith, J.J. Integrating artificial intelligence into the clinical practice of radiology: Challenges and recommendations. Eur. Radiol. 2020, 30, 3576–3584. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ong, W.; Liu, R.W.; Makmur, A.; Low, X.Z.; Sng, W.J.; Tan, J.H.; Kumar, N.; Hallinan, J.T.P.D. Artificial Intelligence Applications for Osteoporosis Classification Using Computed Tomography. Bioengineering 2023, 10, 1364. https://doi.org/10.3390/bioengineering10121364
Ong W, Liu RW, Makmur A, Low XZ, Sng WJ, Tan JH, Kumar N, Hallinan JTPD. Artificial Intelligence Applications for Osteoporosis Classification Using Computed Tomography. Bioengineering. 2023; 10(12):1364. https://doi.org/10.3390/bioengineering10121364
Chicago/Turabian StyleOng, Wilson, Ren Wei Liu, Andrew Makmur, Xi Zhen Low, Weizhong Jonathan Sng, Jiong Hao Tan, Naresh Kumar, and James Thomas Patrick Decourcy Hallinan. 2023. "Artificial Intelligence Applications for Osteoporosis Classification Using Computed Tomography" Bioengineering 10, no. 12: 1364. https://doi.org/10.3390/bioengineering10121364