
Swept-Source Anterior Segment Optical Coherence Tomography Imaging and Quantification of Bleb Parameters in Glaucoma Filtration Surgery
Abstract
:1. Introduction
2. Methods
2.1. Surgical Technique
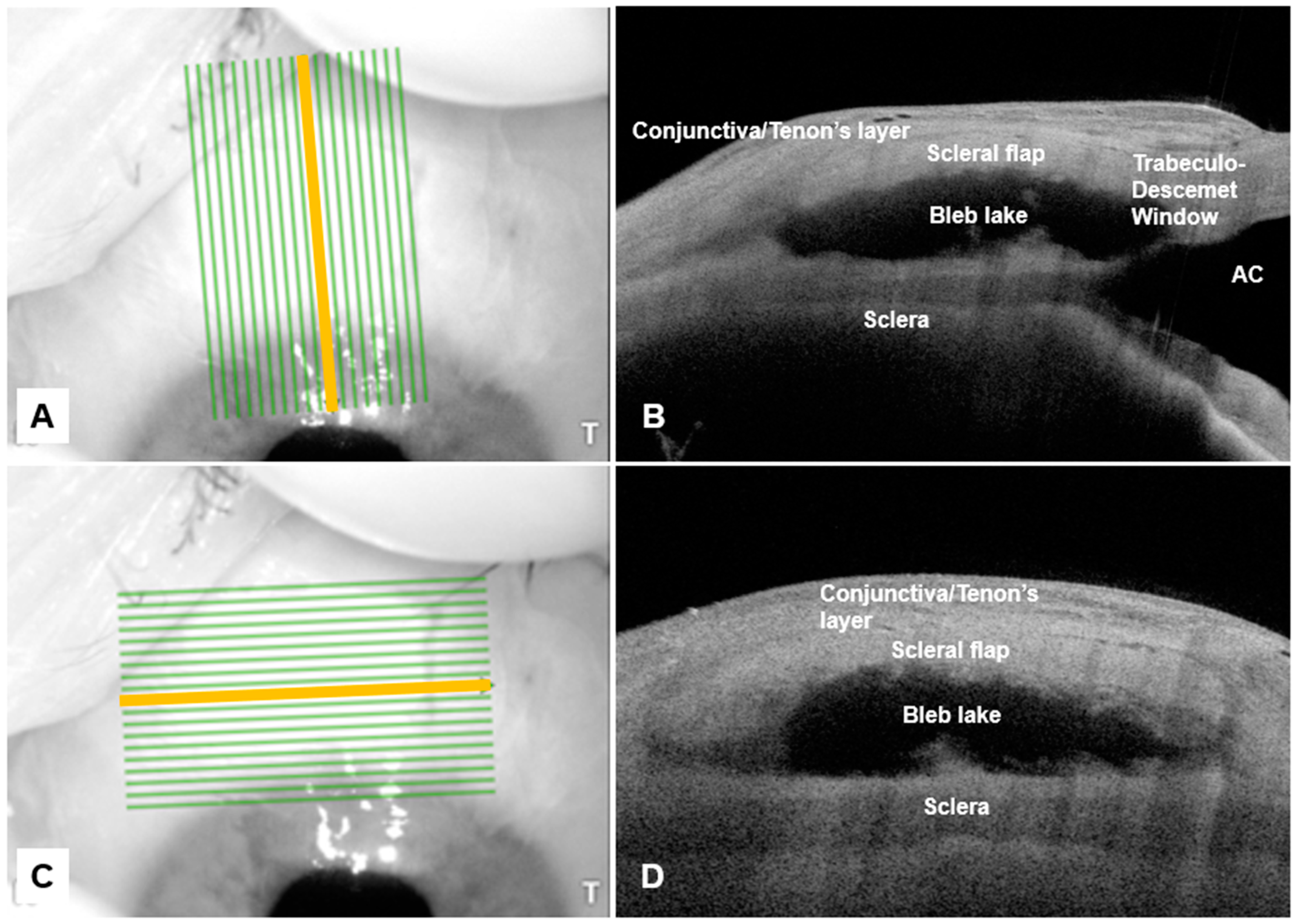
2.2. Anterior-Segment Optical Coherence Tomography Imaging of Filtering Bleb
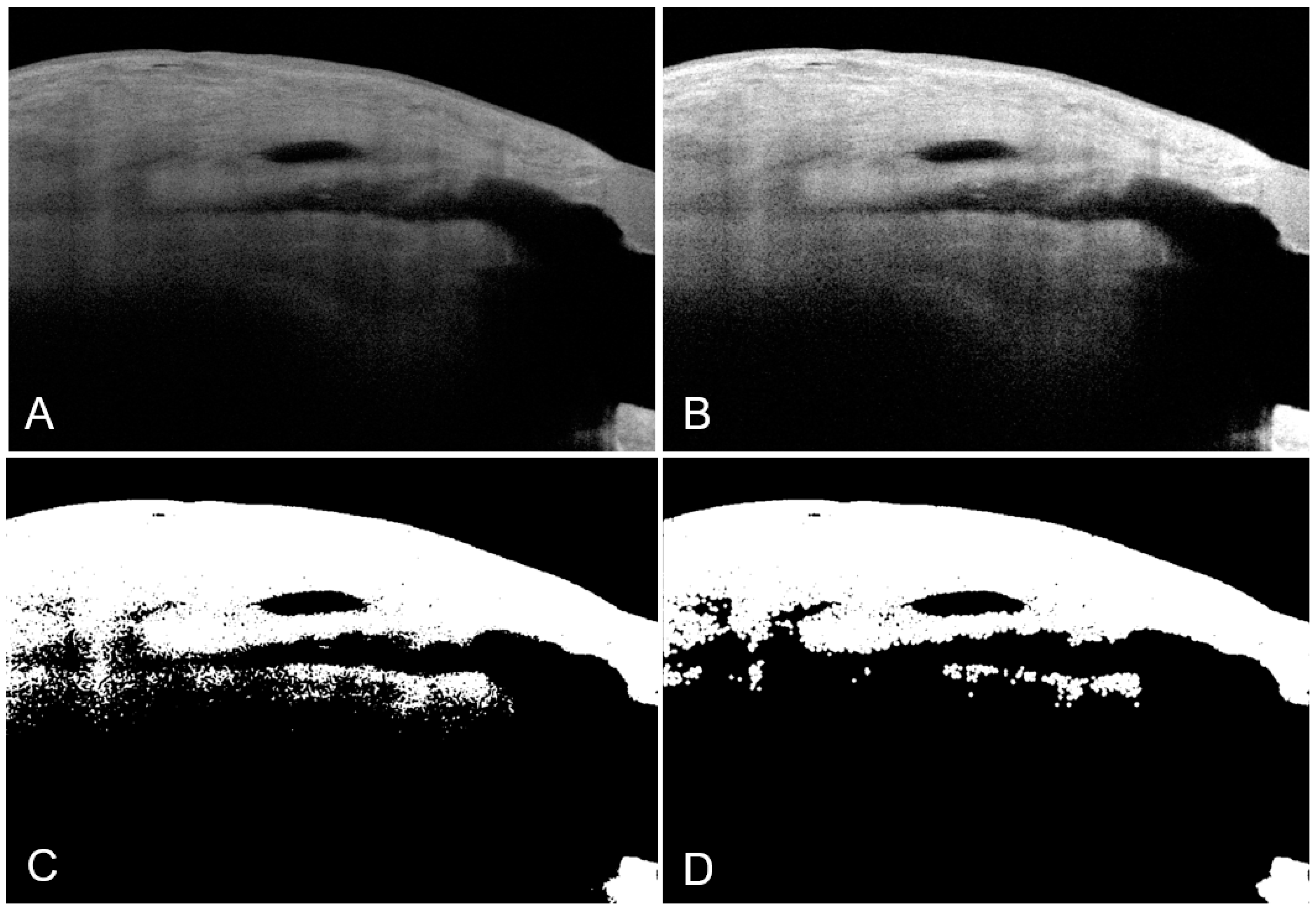
2.3. Image Preprocessing
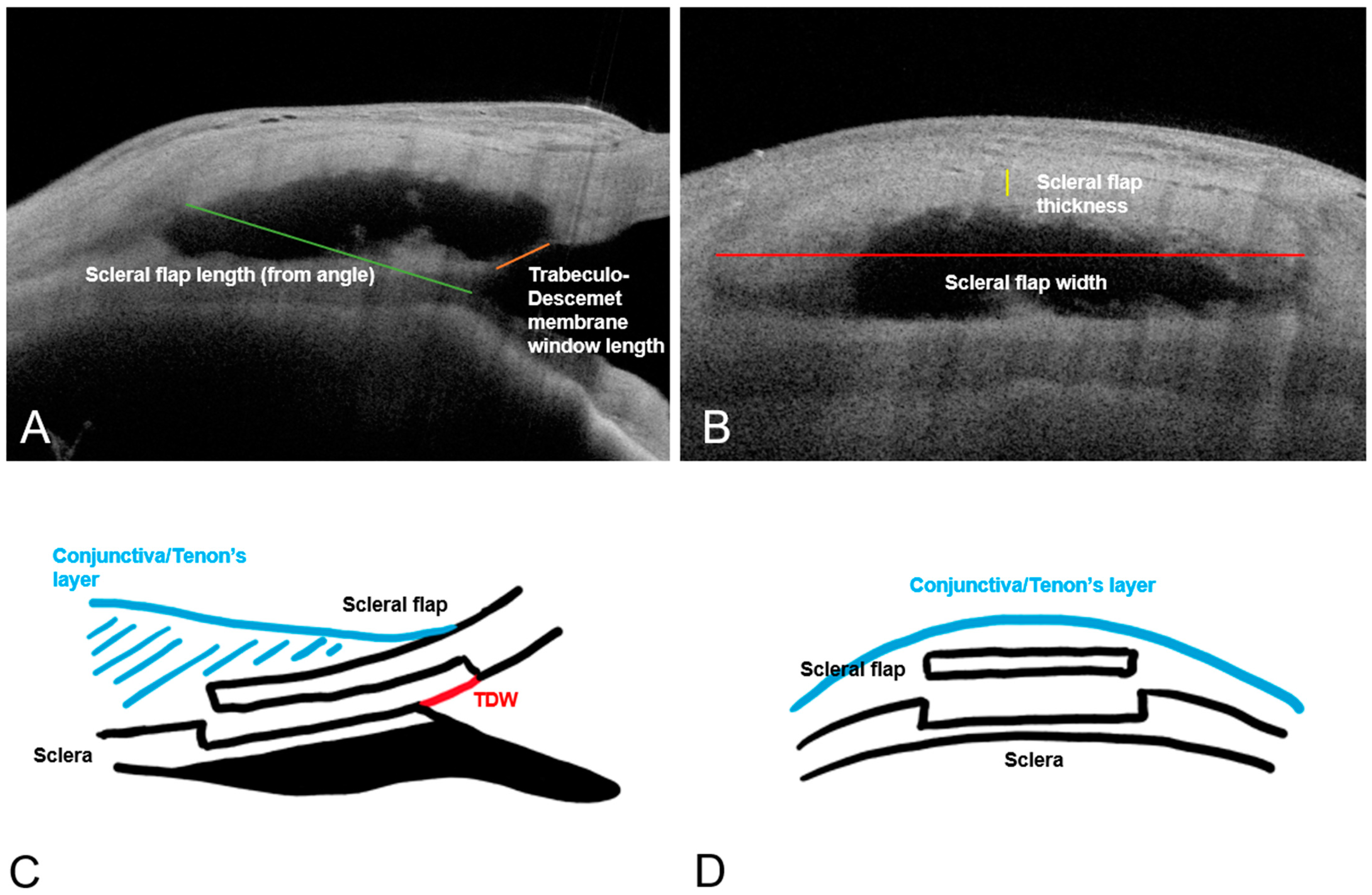
2.4. Visualisation and Quantification of Surgical Parameters
2.5. Definitions of Surgical Success
2.6. Statistical Analysis
3. Results
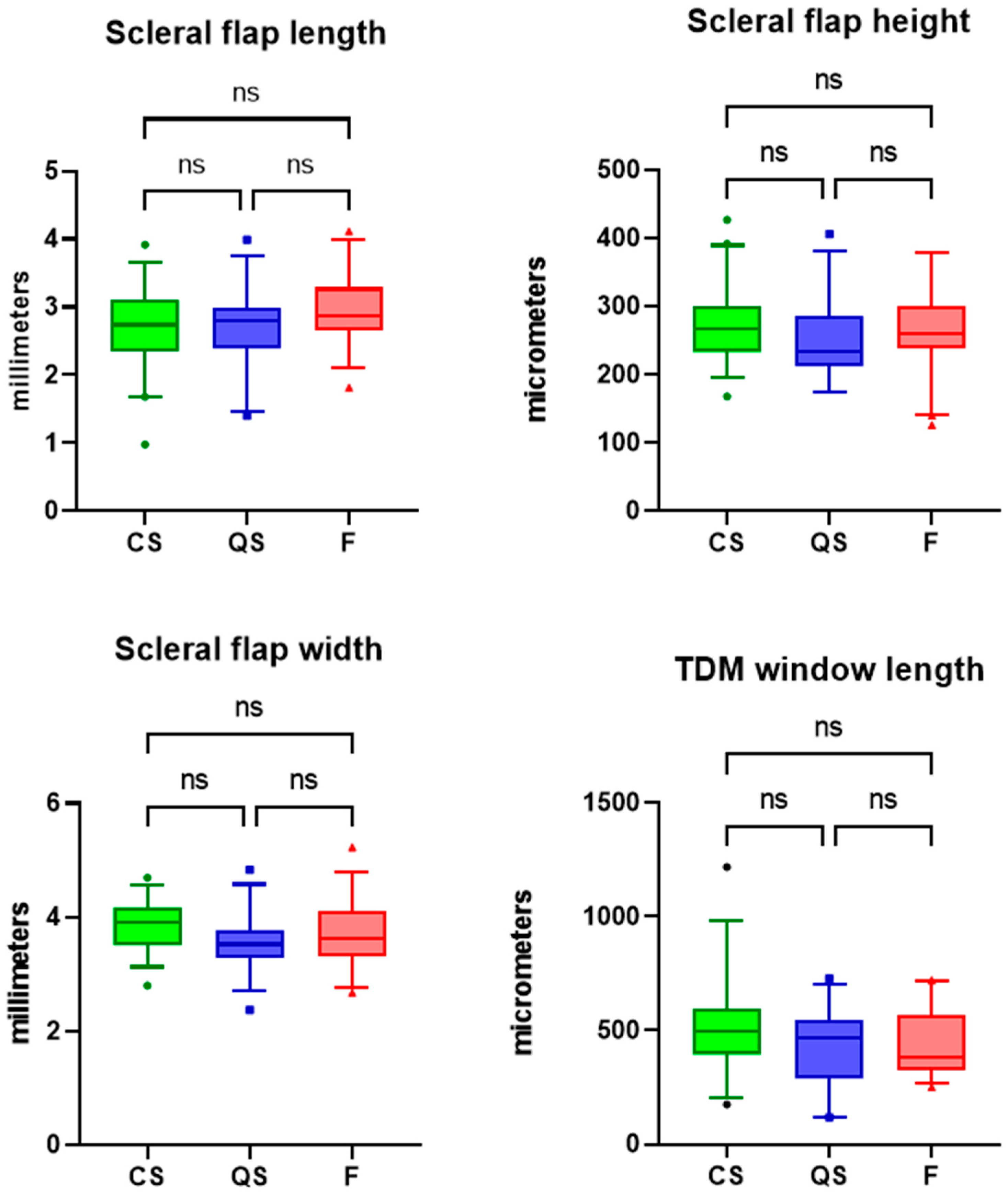
3.1. Bleb Height, Scleral Flap and Trabeculo-Descemet Window Dimensions and Surgical Outcomes
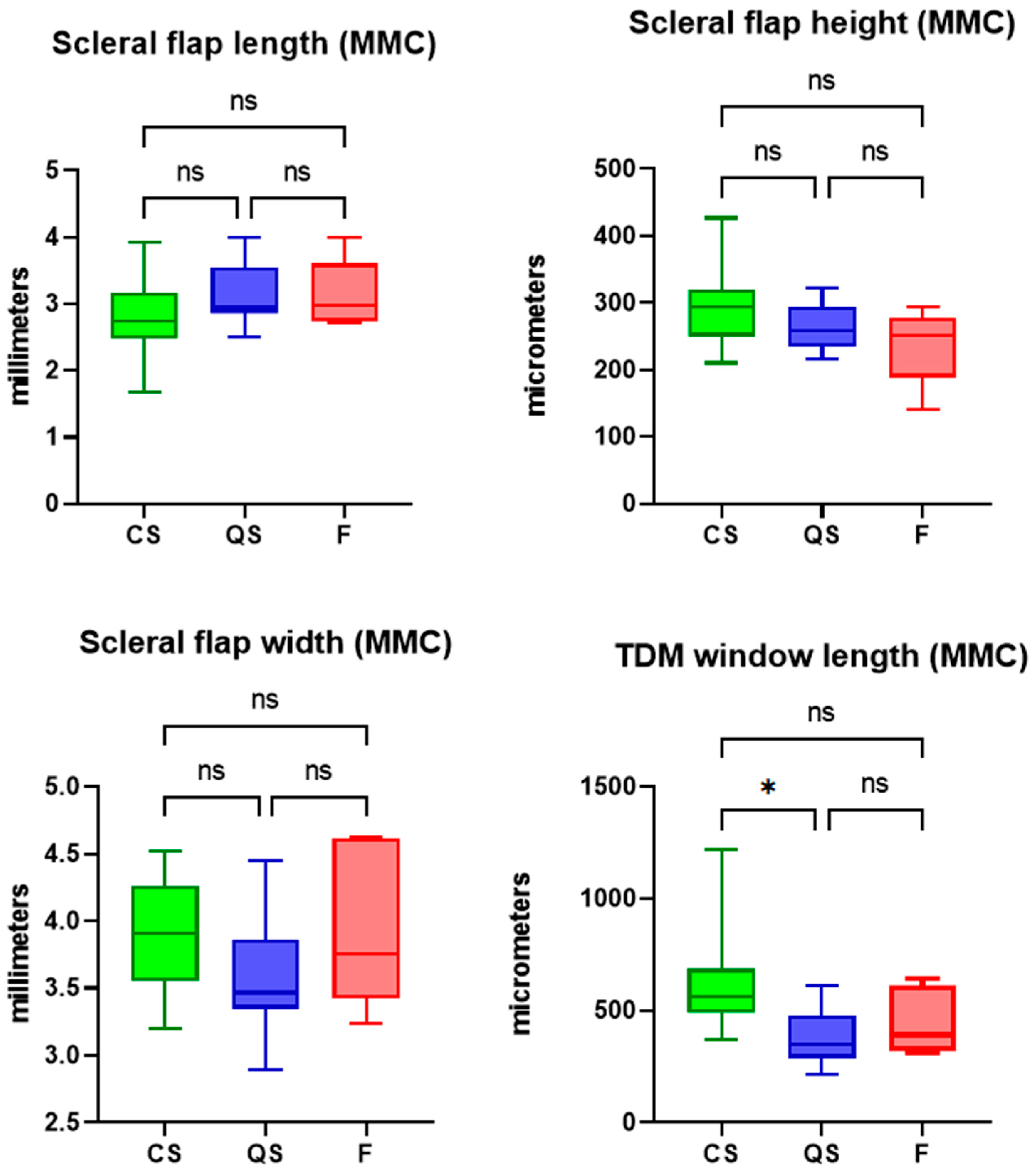
3.2. Subanalysis in Deep Sclerectomy Cases Augmented with Intraoperative Mitomycin-C
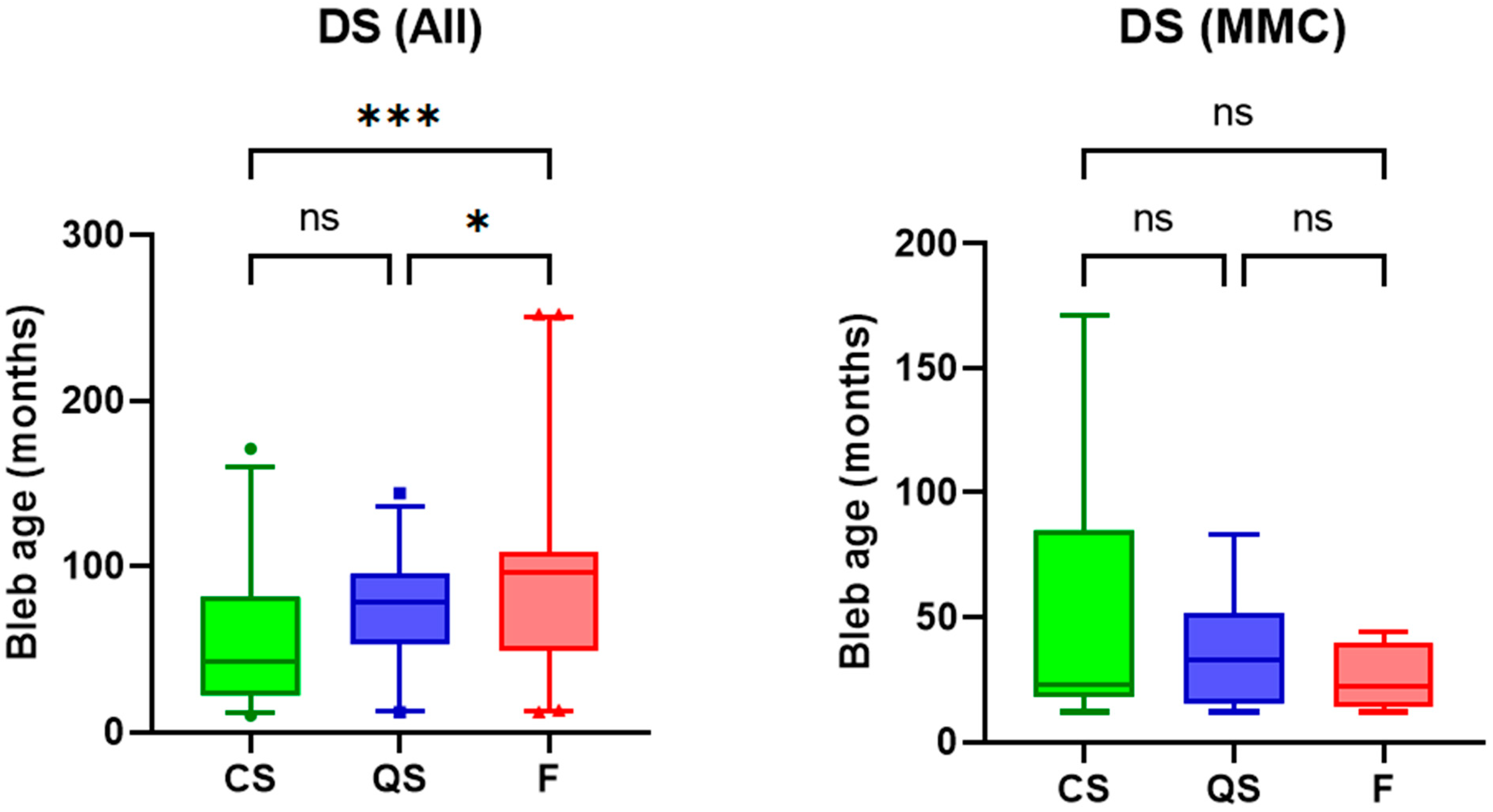
3.3. Post-Operative Duration and Surgical Outcomes
4. Discussion
4.1. Post-Operative Evaluation of Filtering Blebs
4.2. Swept-Source AS-OCT Technology for More Precise Visualization of Glaucoma Surgeries during the Post-Operative Course
4.3. Use of Anterior Segment-OCT in Post-Operative Bleb Evaluation
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Jayaram, H. Intraocular pressure reduction in glaucoma: Does every mmHg count? Taiwan J. Ophthalmol. 2020, 10, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Wolters, J.E.J.; van Mechelen, R.J.S.; Al Majidi, R.; Pinchuk, L.; Webers, C.A.B.; Beckers, H.J.M.; Gorgels, T. History, presence, and future of mitomycin C in glaucoma filtration surgery. Curr. Opin. Ophthalmol. 2021, 32, 148–159. [Google Scholar] [CrossRef]
- Mendrinos, E.; Mermoud, A.; Shaarawy, T. Nonpenetrating glaucoma surgery. Surv. Ophthalmol. 2008, 53, 592–630. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Shaarawy, T. Deep sclerectomy: Safety and efficacy. Middle East Afr. J. Ophthalmol. 2009, 16, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.H.; Kim, Y.A.; Park, K.H.; Lee, Y. Evaluation of Functional Filtering Bleb Using Optical Coherence Tomography Angiography. Transl. Vis. Sci. Technol. 2019, 8, 14. [Google Scholar] [CrossRef]
- Hayek, S.; Labbé, A.; Brasnu, E.; Hamard, P.; Baudouin, C. Optical Coherence Tomography Angiography Evaluation of Conjunctival Vessels During Filtering Surgery. Transl. Vis. Sci. Technol. 2019, 8, 4. [Google Scholar] [CrossRef]
- Oh, L.J.; Wong, E.; Lam, J.; Clement, C.I. Comparison of bleb morphology between trabeculectomy and deep sclerectomy using a clinical grading scale and anterior segment optical coherence tomography. Clin. Exp. Ophthalmol. 2017, 45, 701–707. [Google Scholar] [CrossRef]
- Miura, M.; Kawana, K.; Iwasaki, T.; Kiuchi, T.; Oshika, T.; Mori, H.; Yamanari, M.; Makita, S.; Yatagai, T.; Yasuno, Y. Three-dimensional anterior segment optical coherence tomography of filtering blebs after trabeculectomy. J. Glaucoma 2008, 17, 193–196. [Google Scholar] [CrossRef]
- Heuer, D.; Barton, K.; Grehn, F.; Shaarway, T.; Sherwood, M. Consensus on Definitions of Success; Kugler Publications: Amsterdam, The Netherlands, 2018; Volume 2018. [Google Scholar]
- Gedde, S.J.; Feuer, W.J.; Lim, K.S.; Barton, K.; Goyal, S.; Ahmed, I.I.; Brandt, J.D. Treatment Outcomes in the Primary Tube Versus Trabeculectomy Study after 5 Years of Follow-up. Ophthalmology 2022, 129, 1344–1356. [Google Scholar] [CrossRef]
- Conlon, R.; Saheb, H.; Ahmed, I.I. Glaucoma treatment trends: A review. Can. J. Ophthalmol. 2017, 52, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.; Tham, C.C. Management of bleb complications after trabeculectomy. Semin. Ophthalmol. 2013, 28, 144–156. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, E.M.; Herzog, D.; Wasielica-Poslednik, J.; Butsch, C.; Schuster, A.K. Bleb grading by photographs versus bleb grading by slit-lamp examination. Acta Ophthalmol. 2019, 98, e607–e610. [Google Scholar] [CrossRef]
- Kudsieh, B.; Fernández-Vigo, J.I.; Canut Jordana, M.I.; Vila-Arteaga, J.; Urcola, J.A.; Ruiz Moreno, J.M.; García-Feijóo, J.; Fernández-Vigo, J. Updates on the utility of anterior segment optical coherence tomography in the assessment of filtration blebs after glaucoma surgery. Acta Ophthalmol. 2022, 100, e29–e37. [Google Scholar] [CrossRef]
- Lenzhofer, M.; Strohmaier, C.; Hohensinn, M.; Hitzl, W.; Sperl, P.; Gerner, M.; Steiner, V.; Moussa, S.; Krall, E.; Reitsamer, H.A. Longitudinal bleb morphology in anterior segment OCT after minimally invasive transscleral ab interno Glaucoma Gel Microstent implantation. Acta Ophthalmol. 2019, 97, e231–e237. [Google Scholar] [CrossRef] [PubMed]
- Konstantopoulos, A.; Yadegarfar, M.E.; Yadegarfar, G.; Stinghe, A.; Macleod, A.; Jacob, A.; Hossain, P. Deep sclerectomy versus trabeculectomy: A morphological study with anterior segment optical coherence tomography. Br. J. Ophthalmol. 2013, 97, 708–714. [Google Scholar] [CrossRef] [PubMed]
- Ibarz Barberá, M.; Morales Fernández, L.; Tañá Rivero, P.; Gómez de Liaño, R.; Teus, M.A. Anterior-segment optical coherence tomography of filtering blebs in the early postoperative period of ab externo SIBS microshunt implantation with mitomycin C: Morphological analysis and correlation with intraocular pressure reduction. Acta Ophthalmol. 2022, 100, e192–e203. [Google Scholar] [CrossRef]
- Gambini, G.; Carlà, M.M.; Giannuzzi, F.; Boselli, F.; Grieco, G.; Caporossi, T.; De Vico, U.; Savastano, A.; Baldascino, A.; Rizzo, C.; et al. Anterior Segment-Optical Coherence Tomography Bleb Morphology Comparison in Minimally Invasive Glaucoma Surgery: XEN Gel Stent vs. PreserFlo MicroShunt. Diagnostics 2022, 12, 1250. [Google Scholar] [CrossRef]
- Anand, N.; Pilling, R. Nd:YAG laser goniopuncture after deep sclerectomy: Outcomes. Acta Ophthalmol. 2010, 88, 110–115. [Google Scholar] [CrossRef]
- Mermoud, A.; Karlen, M.E.; Schnyder, C.C.; Sickenberg, M.; Chiou, A.G.; Hédiguer, S.E.; Sanchez, E. Nd:Yag goniopuncture after deep sclerectomy with collagen implant. Ophthalmic Surg. Lasers 1999, 30, 120–125. [Google Scholar] [CrossRef]
- Wilkins, M.; Indar, A.; Wormald, R. Intra-operative mitomycin C for glaucoma surgery. Cochrane Database Syst. Rev. 2005, 2005, Cd002897. [Google Scholar] [CrossRef] [PubMed]
- Batterbury, M.; Wishart, P.K. Is high initial aqueous outflow of benefit in trabeculectomy? Eye 1993, 7 Pt 1, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Wells, A.P.; Bunce, C.; Khaw, P.T. Flap and suture manipulation after trabeculectomy with adjustable sutures: Titration of flow and intraocular pressure in guarded filtration surgery. J. Glaucoma 2004, 13, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.H.; Fatehi, N.; Romero, P.; Miraftabi, A.; Kim, E.; Morales, E.; Giaconi, J.; Coleman, A.L.; Law, S.K.; Caprioli, J.; et al. Observational Outcomes of Initial Trabeculectomy With Mitomycin C in Patients of African Descent vs Patients of European Descent: Five-Year Results. JAMA Ophthalmol. 2018, 136, 1106–1113. [Google Scholar] [CrossRef] [PubMed]
- Issa de Fendi, L.; Cena de Oliveira, T.; Bigheti Pereira, C.; Pereira Bigheti, C.; Viani, G.A. Additive Effect of Risk Factors for Trabeculectomy Failure in Glaucoma Patients: A Risk-group From a Cohort Study. J. Glaucoma 2016, 25, e879–e883. [Google Scholar] [CrossRef]
- The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration.The AGIS Investigators. Am. J. Ophthalmol. 2000, 130, 429–440. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Imaging Plane | Surgical Parameters of Interest | Anatomical Reference Points of Surgical Parameter |
|---|---|---|
| Sagittal | Scleral flap length | Posterior edge of scleral flap to iridocorneal angle |
| Trabeculo-Descemet window length | Anterior edge of TDW to posterior edge of TDW | |
| Coronal | Scleral flap width | Nasal edge of scleral flap to temporal edge of scleral flap at midpoint of flap |
| Scleral flap thickness | Superior edge of scleral flap to inferior edge of scleral flap at midpoint of flap |
| Parameter | CS | QS | F | p Value |
|---|---|---|---|---|
| Bleb height (mm) | 1.48 | 1.17 | 1.10 | 0.001 |
| 0.44 | 0.44 | 0.40 | ||
| Scleral flap length (mm) | 2.71 | 2.73 | 2.96 | 0.178 |
| 0.60 | 0.54 | 0.53 | ||
| Scleral flap thickness (µm) | 270.40 | 249.90 | 267.60 | 0.437 |
| 53.54 | 53.15 | 57.26 | ||
| Scleral flap width (mm) | 3.85 | 3.56 | 3.71 | 0.088 |
| 0.44 | 0.47 | 0.58 | ||
| Window length (µm) | 519.00 | 432.90 | 441.30 | 0.094 |
| 206.40 | 164.30 | 146.60 | ||
| Scleral flap length, MMC (mm) | 2.77 | 3.11 | 3.15 | 0.150 |
| 0.54 | 0.45 | 0.51 | ||
| Scleral flap thickness, MMC (µm) | 298.30 | 264.40 | 236.60 | 0.027 |
| 53.48 | 34.79 | 57.81 | ||
| Scleral flap width, MMC, (mm) | 3.90 | 3.58 | 3.97 | 0.273 |
| 0.40 | 0.46 | 0.62 | ||
| Window length, MMC (µm) | 613.70 | 378.10 | 450.80 | 0.004 |
| 200.20 | 127.80 | 152.40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, J.C.K.; Muntasser, H.; Choudhary, A.; Batterbury, M.; Vallabh, N.A. Swept-Source Anterior Segment Optical Coherence Tomography Imaging and Quantification of Bleb Parameters in Glaucoma Filtration Surgery. Bioengineering 2023, 10, 1186. https://doi.org/10.3390/bioengineering10101186
Tan JCK, Muntasser H, Choudhary A, Batterbury M, Vallabh NA. Swept-Source Anterior Segment Optical Coherence Tomography Imaging and Quantification of Bleb Parameters in Glaucoma Filtration Surgery. Bioengineering. 2023; 10(10):1186. https://doi.org/10.3390/bioengineering10101186
Chicago/Turabian StyleTan, Jeremy C.K., Hussameddin Muntasser, Anshoo Choudhary, Mark Batterbury, and Neeru A. Vallabh. 2023. "Swept-Source Anterior Segment Optical Coherence Tomography Imaging and Quantification of Bleb Parameters in Glaucoma Filtration Surgery" Bioengineering 10, no. 10: 1186. https://doi.org/10.3390/bioengineering10101186