
Bedside Hyperspectral Imaging and Organ Dysfunction Severity in Critically Ill COVID-19 Patients—A Prospective, Monocentric Observational Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Hospital Setting
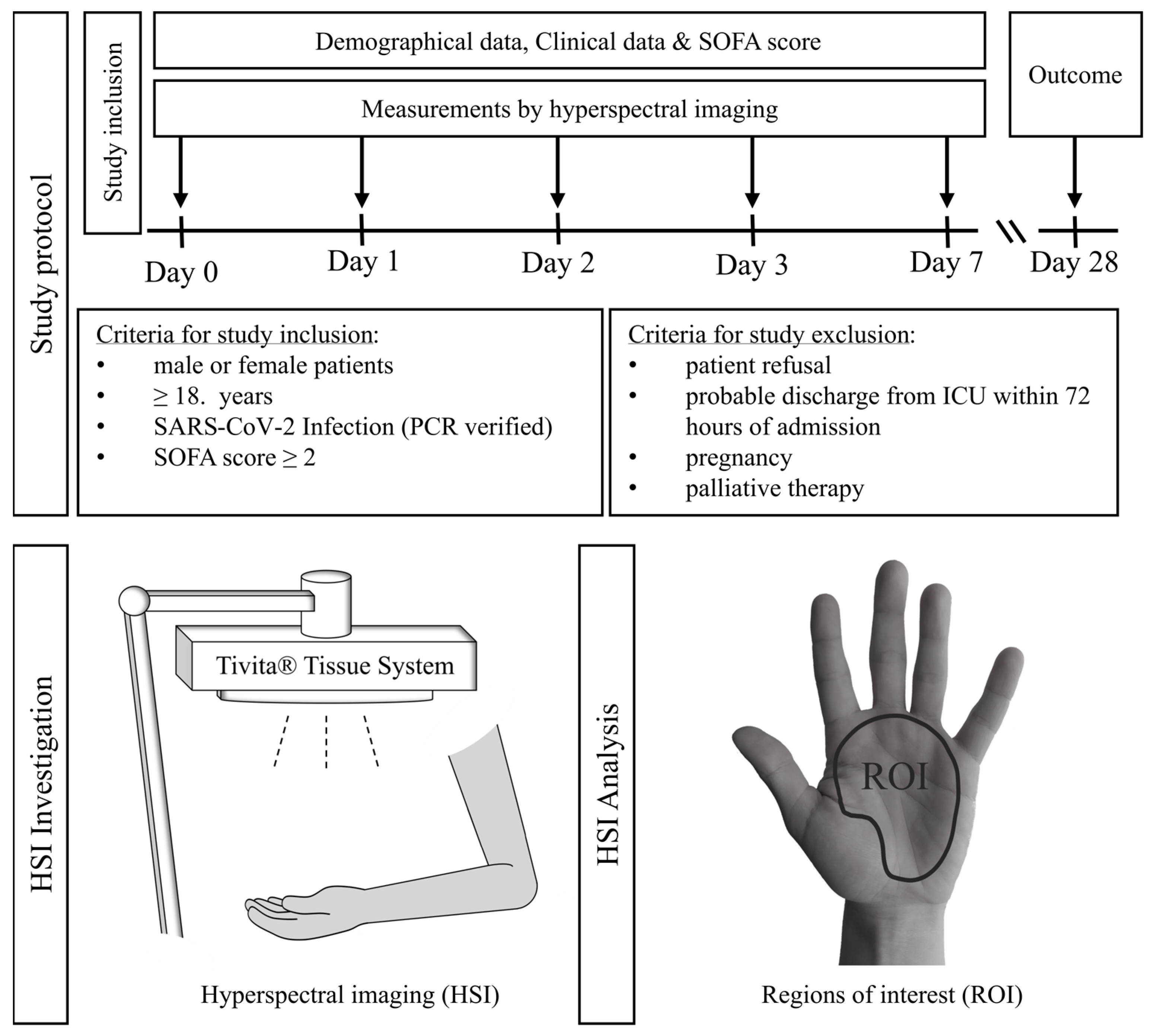
2.2. Patient Recruitment and Study Protocol
2.3. Patient Treatment
2.4. HSI Measurement
2.4.1. HSI Camera System
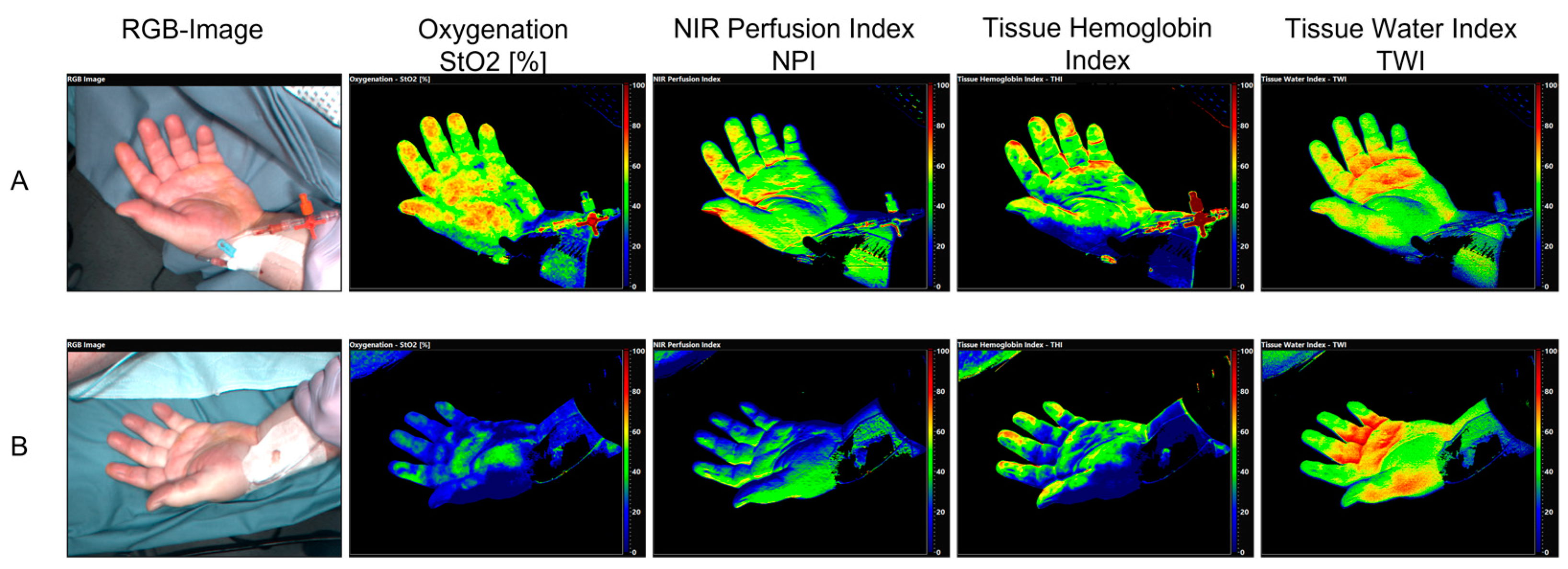
- Tissue Oxygenation (StO2) (wavelength range: 570–590 nm, penetration depth < 1 mm).
- Near infrared perfusion index (NPI) (wavelength range: 655–735 nm and 825–925 nm, penetration depth: 3–5 mm).
- Tissue Hemoglobin index (THI) (wavelength range: 530–590 nm and 785–825 nm).
- Tissue Water Index (TWI) (wavelength range: 880–900 nm and 955–980 nm).
2.4.2. Image Acquisition
2.4.3. Clinical Data Acquisition and SOFA Score Calculation
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Critically Ill COVID-19 Patients
3.2. Hyperspectral Imaging (HSI) in Critically Ill COVID-19 Patients
3.3. The Association between HSI Measurements and Disease Severity in Critically Ill COVID-19 Patients
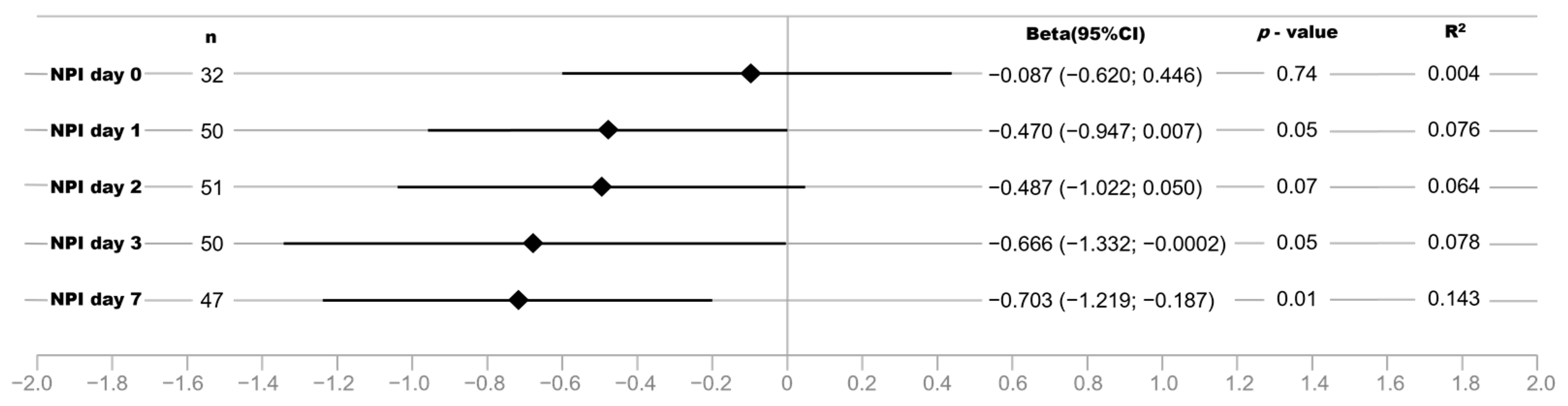
3.4. Strength of the Association between NPI and Disease Severity Increases with Length of ICU Treatment in Critically Ill COVID-19 Patients
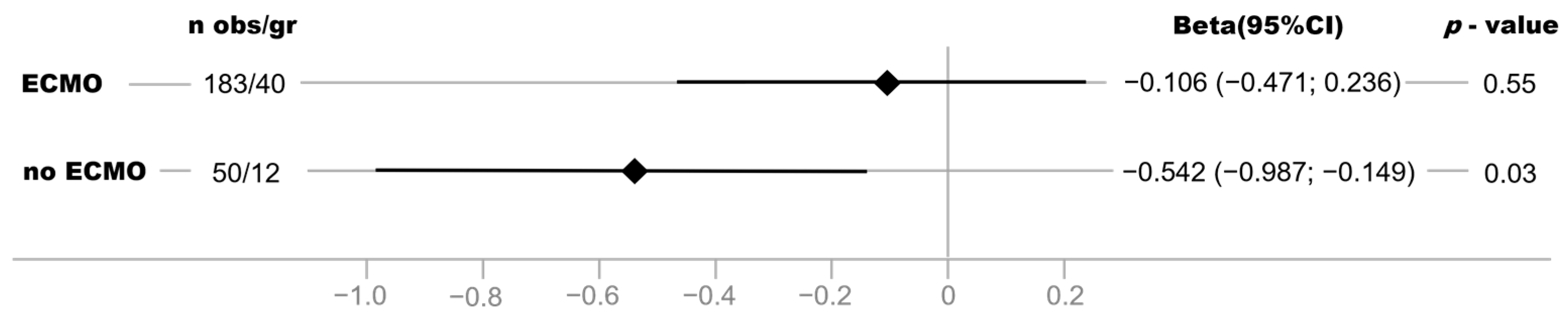
3.5. Association between NPI and Disease Severity Is Stronger in Critically COVID-19 Patients without vvECMO Therapy
3.6. StO2 and NPI Are Strongly Associated with Norepinephrine Support and Blood Lactate Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kanoore Edul, V.S.; Caminos Eguillor, J.F.; Ferrara, G.; Estenssoro, E.; Siles, D.S.P.; Cesio, C.E.; Dubin, A. Microcirculation alterations in severe COVID-19 pneumonia. J. Crit. Care. 2021, 61, 73–75. [Google Scholar] [CrossRef]
- Martini, R. The compelling arguments for the need of microvascular investigation in COVID-19 critical patients. Clin. Hemorheol. Microcirc. 2020, 75, 27–34. [Google Scholar] [CrossRef]
- Duranteau, J.; De Backer, D.; Donadello, K.; Shapiro, N.I.; Hutchings, S.D.; Rovas, A.; Legrand, M.; Harrois, A.; Ince, C. The future of intensive care: The study of the microcirculation will help to guide our therapies. Crit. Care 2023, 27, 190. [Google Scholar] [CrossRef]
- Ince, C. Hemodynamic coherence and the rationale for monitoring the microcirculation. Crit. Care 2015, 19, S8. [Google Scholar] [CrossRef] [PubMed]
- Tafner, P.F.D.A.; Chen, F.K.; Rabello Filho, R.; Corrêa, T.D.; Chaves, R.C.D.F.; Serpa Neto, A. Recent advances in bedside microcirculation assessment in critically ill patients. Rev. Bras. De Ter. Intensiv. 2017, 29, 238–247. [Google Scholar] [CrossRef]
- Hariri, G.; Joffre, J.; Leblanc, G.; Bonsey, M.; Lavillegrand, J.-R.; Urbina, T.; Guidet, B.; Maury, E.; Bakker, J.; Ait-Oufella, H. Narrative review: Clinical assessment of peripheral tissue perfusion in septic shock. Ann. Intensive Care 2019, 9, 37. [Google Scholar] [CrossRef]
- Kattan, E.; Castro, R.; Vera, M.; HernáNdez, G. Optimal target in septic shock resuscitation. Ann. Transl. Med. 2020, 8, 789. [Google Scholar] [CrossRef] [PubMed]
- Holmer, A.; Tetschke, F.; Marotz, J.; Malberg, H.; Markgraf, W.; Thiele, C.; Kulcke, A. Oxygenation and perfusion monitoring with a hyperspectral camera system for chemical based tissue analysis of skin and organs. Physiol. Meas. 2016, 37, 2064–2078. [Google Scholar] [CrossRef] [PubMed]
- Barberio, M.; Benedicenti, S.; Pizzicannella, M.; Felli, E.; Collins, T.; Jansen-Winkeln, B.; Marescaux, J.; Viola, M.G.; Diana, M. Intraoperative Guidance Using Hyperspectral Imaging: A Review for Surgeons. Diagnostics 2021, 11, 2066. [Google Scholar] [CrossRef]
- Dietrich, M.; Marx, S.; von der Forst, M.; Bruckner, T.; Schmitt, F.C.F.; Fiedler, M.O.; Nickel, F.; Studier-Fischer, A.; Müller-Stich, B.P.; Hackert, T.; et al. Bedside hyperspectral imaging indicates a microcirculatory sepsis pattern—An observational study. Microvasc. Res. 2021, 136, 104164. [Google Scholar] [CrossRef]
- Kazune, S.; Caica, A.; Luksevics, E.; Volceka, K.; Grabovskis, A. Impact of increased mean arterial pressure on skin microcirculatory oxygenation in vasopressor-requiring septic patients: An interventional study. Ann. Intensive Care 2019, 9, 97. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, M.; Marx, S.; Von Der Forst, M.; Bruckner, T.; Schmitt, F.C.F.; Fiedler, M.O.; Nickel, F.; Studier-Fischer, A.; Müller-Stich, B.P.; Hackert, T.; et al. Hyperspectral imaging for perioperative monitoring of microcirculatory tissue oxygenation and tissue water content in pancreatic surgery—An observational clinical pilot study. Perioper. Med. 2021, 10, 42. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, M.; Özdemir, B.; Gruneberg, D.; Petersen, C.; Studier-Fischer, A.; Von Der Forst, M.; Schmitt, F.C.F.; Fiedler, M.O.; Nickel, F.; Müller-Stich, B.P.; et al. Hyperspectral Imaging for the Evaluation of Microcirculatory Tissue Oxygenation and Perfusion Quality in Haemorrhagic Shock: A Porcine Study. Biomedicines 2021, 9, 1829. [Google Scholar] [CrossRef] [PubMed]
- Espeter, F.; Künne, D.; Garczarek, L.; Kuhlmann, H.; Skarabis, A.; Zivkovic, A.R.; Brenner, T.; Schmidt, K. Critically Ill COVID-19 Patients Show Reduced Point of Care-Measured Butyrylcholinesterase Activity—A Prospective, Monocentric Observational Study. Diagnostics 2022, 12, 2150. [Google Scholar] [CrossRef] [PubMed]
- Herbstreit, F.; Overbeck, M.; Berger, M.M.; Skarabis, A.; Brenner, T.; Schmidt, K. Characteristics of Critically Ill Patients with COVID-19 Compared to Patients with Influenza—A Single Center Experience. J. Clin. Med. 2021, 10, 2056. [Google Scholar] [CrossRef]
- Badulak, J.; Antonini, M.V.; Stead, C.M.; Shekerdemian, L.; Raman, L.; Paden, M.L.; Agerstrand, C.; Bartlett, R.H.; Barrett, N.; Combes, A.; et al. Extracorporeal Membrane Oxygenation for COVID-19: Updated 2021 Guidelines from the Extracorporeal Life Support Organization. ASAIO J. 2021, 67, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Fachgruppe COVRIIN. COVID-19 Therapiehinweise Und-Empfehlungen. 2023. Available online: https://www.rki.de/DE/Content/Kommissionen/COVRIIN/Therapie_Versorgung/FG_COVRIIN_Therapie_Versorgung_node.html (accessed on 4 July 2023).
- Holmer, A.; Marotz, J.; Wahl, P.; Dau, M.; Kämmerer, P.W. Hyperspectral imaging in perfusion and wound diagnostics—Methods and algorithms for the determination of tissue parameters. Biomed. Tech. 2018, 63, 547–556. [Google Scholar] [CrossRef]
- Kulcke, A.; Holmer, A.; Wahl, P.; Siemers, F.; Wild, T.; Daeschlein, G. A compact hyperspectral camera for measurement of perfusion parameters in medicine. Biomed. Eng. Biomed. Tech. 2018, 63, 519–527. [Google Scholar] [CrossRef]
- Vasilevskis, E.E.; Pandharipande, P.P.; Graves, A.J.; Shintani, A.; Tsuruta, R.; Ely, E.W.; Girard, T.D. Validity of a Modified Sequential Organ Failure Assessment Score Using the Richmond Agitation-Sedation Scale. Crit. Care Med. 2016, 44, 138–146. [Google Scholar] [CrossRef]
- Barnett, A.G. Regression to the mean: What it is and how to deal with it. Int. J. Epidemiol. 2004, 34, 215–220. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- The ARDS Definition Task Force. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Mesquida, J.; Caballer, A.; Cortese, L.; Vila, C.; Karadeniz, U.; Pagliazzi, M.; Zanoletti, M.; Pacheco, A.P.; Castro, P.; García-De-Acilu, M.; et al. Peripheral microcirculatory alterations are associated with the severity of acute respiratory distress syndrome in COVID-19 patients admitted to intermediate respiratory and intensive care units. Crit. Care 2021, 25, 381. [Google Scholar] [CrossRef]
- Di Dedda, U.; Ascari, A.; Fantinato, A.; Fina, D.; Baryshnikova, E.; Ranucci, M. Microcirculatory Alterations in Critically Ill Patients with COVID-19-Associated Acute Respiratory Distress Syndrome. J. Clin. Med. 2022, 11, 1032. [Google Scholar] [CrossRef]
- Do Espírito Santo, D.A.; Lemos, A.C.B.; Miranda, C.H. In vivo demonstration of microvascular thrombosis in severe COVID-19. J. Thromb. Thrombolysis 2020, 50, 790–794. [Google Scholar] [CrossRef]
- Rovas, A.; Buscher, K.; Osiaevi, I.; Drost, C.C.; Sackarnd, J.; Tepasse, P.-R.; Fobker, M.; Kühn, J.; Braune, S.; Göbel, U.; et al. Microvascular and proteomic signatures overlap in COVID-19 and bacterial sepsis: The MICROCODE study. Angiogenesis 2022, 25, 503–515. [Google Scholar] [CrossRef]
- Carsetti, A.; Damiani, E.; Casarotta, E.; Scorcella, C.; Domizi, R.; Montomoli, J.; Gasparri, F.; Gabbanelli, V.; Pantanetti, S.; Carozza, R.; et al. Sublingual microcirculation in patients with SARS-CoV-2 undergoing veno-venous extracorporeal membrane oxygenation. Microvasc Res 2020, 132, 104064. [Google Scholar] [CrossRef]
- Kazune, S.; Caica, A.; Volceka, K.; Suba, O.; Rubins, U.; Grabovskis, A. Relationship of mottling score, skin microcirculatory perfusion indices and biomarkers of endothelial dysfunction in patients with septic shock: An observational study. Crit. Care 2019, 23, 331. [Google Scholar] [CrossRef]
- Hilty, M.P.; Favaron, E.; Wendel Garcia, P.D.; Ahiska, Y.; Uz, Z.; Akin, S.; Flick, M.; Arbous, S.; Hofmaenner, D.A.; Saugel, B.; et al. Microcirculatory alterations in critically ill COVID-19 patients analyzed using artificial intelligence. Critical Care 2022, 26. [Google Scholar] [CrossRef]
- Cui, R.; Yu, H.; Xu, T.; Xing, X.; Cao, X.; Yan, K.; Chen, J. Deep Learning in Medical Hyperspectral Images: A Review. Sensors 2022, 22, 9790. [Google Scholar] [CrossRef]
- Studier-Fischer, A.; Seidlitz, S.; Sellner, J.; Özdemir, B.; Wiesenfarth, M.; Ayala, L.; Odenthal, J.; Knödler, S.; Kowalewski, K.F.; Haney, C.M.; et al. Spectral organ fingerprints for machine learning-based intraoperative tissue classification with hyperspectral imaging in a porcine model. Sci. Rep. 2022, 12, 11028. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Mostert, C.; Hentschker, C.; Voshaar, T.; Malzahn, J.; Schillinger, G.; Klauber, J.; Janssens, U.; Marx, G.; Weber-Carstens, S.; et al. Case characteristics, resource use, and outcomes of 10,021 patients with COVID-19 admitted to 920 German hospitals: An observational study. Lancet Respir. Med. 2020, 8, 853–862. [Google Scholar] [CrossRef]
- Herrmann, J.; Lotz, C.; Karagiannidis, C.; Weber-Carstens, S.; Kluge, S.; Putensen, C.; Wehrfritz, A.; Schmidt, K.; Ellerkmann, R.K.; Oswald, D.; et al. Key characteristics impacting survival of COVID-19 extracorporeal membrane oxygenation. Crit. Care 2022, 26, 190. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease Severity, Resuscitation Therapy and Clinical Parameters of All Critically Ill COVID-19 Patients (n = 52) | |||||
|---|---|---|---|---|---|
| Day 0 | Day 1 | Day 2 | Day 3 | Day 7 | |
| Disease severity | |||||
| SOFA Score * | 12 (± 5) [11] | 12 (± 4) [0] | 12 (± 4) [0] | 12 (± 4) [0] | 13 (± 5) [4] |
| Resuscitation Therapy | |||||
| Fluids (ml per 24 h) * | 234 (± 1505) [12] | −816 (± 1628) [0] | −482 (± 2217) [0] | −587 (± 1277) [1] | 153 (± 2055) [5] |
| Norepinephrine dose (mcg/kg/min) # | 0.16 (0.08–0.40) [20] | 0.10 (0.04–0.19) [16] | 0.04 (0.02–0.10) [15] | 0.06 (0.02–0.10) [20] | 0.06 (0.02–0.20) [12] |
| Clinical Parameters | |||||
| Lactate (mmol/L) # | 1.7 (1.4–2.3) [11] | 1.6 (1.2–1.9) [0] | 1.4 (1.0–1.9) [0] | 1.2 (0.9–1.8) [0] | 1.5 (0.9–1.9) [4] |
| Hemoglobin (g/dl) # | 11.2 (9.3–13.0) [11] | 9.8 (8.9–12.4) [0] | 9.0 (8.1–11.4) [0] | 9.1 (8.5–10.6) [0] | 9.2 (8.4–10.0) [4] |
| Temperature (Degree Celsius (°C)) # | 37.0 (36.5–37.4) [11] | 37.0 (36.6–37.4) [0] | 37.0 (36.6–37.2) [0] | 37.1 (36.8–37.4) [0] | 37.0 (36.8–37.4) [4] |
| Mean arterial pressure (mmHg) * | 90 (± 13) [11] | 88 (± 14) [0] | 88 (± 13) [0] | 88 (± 13) [0] | 80 (± 12) [4] |
| Heart rate (beats/min) * | 92 (± 22) [11] | 82 (± 16) [0] | 81 (± 20) [0] | 79 (± 14) [0] | 85 (± 15) [4] |
| pH value # | 7.37 (7.28–7.42) [11] | 7.40 (7.35–7.46) [0] | 7.42 (7.36–7.46) [0] | 7.43 (7.39–7.45) [0] | 7.39 (7.35–7.44) [3] |
| Partial pressure of carbon dioxide (mmHg) # | 49 (42–61) [11] | 49 (43–54) [1] | 48 (42–54) [0] | 47 (41–54) [0] | 47 (42–53) [3] |
| Partial pressure of oxygen (mmHg) # | 82 (69–101) [11] | 78 (68–88) [0] | 75 (64–85) [0] | 73 (66–83) [0] | 74 (67–86) [4] |
| paO2/FiO2 # | 140 (83–210) [11] | 192 (136–243) [0] | 184 (122–220) [0] | 179 (120–245) [0] | 156 (115–220) [4] |
| Peripheral oxygen saturation (%) # | 96 (94–99) [11] | 95 (94–97) [0] | 96 (93–97) [0] | 95 (93–96) [0] | 94 (93–97) [6] |
| Disease Severity, Resuscitation Therapy and Clinical Parameters of Critically Ill COVID-19 Patients with vvECMO (n = 40) | |||||
|---|---|---|---|---|---|
| Day 0 | Day 1 | Day 2 | Day 3 | Day 7 | |
| Disease severity | |||||
| SOFA Score * | 14 (± 3) [9] | 13 (± 2) [0] | 13 (± 2) [0] | 13 (± 2) [0] | 14 (± 4) [2] |
| Resuscitation Therapy | |||||
| Fluids (ml per 24 h) * | 375 (± 1478) [10] | −924 (± 1675) [0] | −566 (± 2435) [0] | −531 (± 1310) [0] | 317 (± 2186) [3] |
| Norepinephrine dose (mcg/kg/min) # | 0.17 (0.09–0.40) [13] | 0.10 (0.04–0.20) [10] | 0.04 (0.02–0.10) [10] | 0.06 (0.02–0.11) [15] | 0.07 (0.03–0.20) [8] |
| ECMO blood flow (L/min) # | 4.2 (3.8–4.6) [12] | 3.9 (3.3–4.7) [5] | 4.2 (3.1–4.8) [5] | 3.8 (3.2–4.8) [5] | 4.1 (3.1–4.9) [7] |
| ECMO air flow (L/min) # | 3 (2.00–6) [12] | 4 (3–6) [5] | 4 (3–6) [5] | 4 (2–6) [9] | 4 (2–6) [9] |
| Clinical Parameters | |||||
| Lactate (mmol/L) # | 1.9 (1.5–2.4) [9] | 1.6 (1.2–1.9) [0] | 1.4 (1.0–1.9) [0] | 1.2 (0.9–1.7) [0] | 1.5 (0.9–1.8) [2] |
| Hemoglobin (g/dl) # | 10.3 (9.3–12.3) [9] | 9.6 (8.9–11.1) [0] | 8.9 (8.1–9.8) [0] | 9.0 (8.3–9.7) [0] | 9.1 (8.3–9.5) [2] |
| Temperature (Degree Celsius (°C)) # | 37.0 (36.4–37.4) [9] | 37.0 (36.7–37.2) [0] | 37.0 (36.4–37.2) [0] | 37.0 (36.8–37.4) [0] | 37.1 (37.0–37.4) [2] |
| Mean arterial pressure (mmHg) * | 90 (± 12) [9] | 89 (± 14) [0] | 88 (± 13) [0] | 88 (± 13) [0] | 81 (± 14) [2] |
| Heart rate (beats/min) * | 93 (± 22) [9] | 83 (± 16) [0] | 84 (± 21) [0] | 80 (± 15) [0] | 86 (± 16) [2] |
| pH value # | 7.34 (7.24–7.40) [9] | 7.36 (7.36–7.45) [0] | 7.42 (7.36–7.45) [0] | 7.42 (7.39–7.45) [0] | 7.38 (7.35–7.45) [2] |
| Partial pressure of carbon dioxide (mmHg) # | 52 (44–62) [9] | 49 (44–56) [1] | 48 (43–53) [0] | 49 (43–54) [0] | 47.8 (42–52) [2] |
| Partial pressure of oxygen (mmHg) # | 82 (68–101) [9] | 79 (54–90) [0] | 76 (69–89) [0] | 74 (69–89) [0] | 73 (65–88) [2] |
| paO2/FiO2 # | 107 (79–215) [9] | 192 (126–243) [0] | 184 (122–220) [0] | 179 (120–245) [0] | 156 (120–221) [2] |
| Peripheral oxygen saturation (%) # | 95 (92–98) [9] | 96 (94–97) [0] | 95 (93–97) [0] | 95 (93–97) [0] | 94 (91–96) [2] |
| HSI Parameters in All Critically Ill COVID-19 Patients (n = 52). | |||||
| Day 0 | Day 1 | Day 2 | Day 3 | Day 7 | |
| StO2 | 57.05 (± 12.02) [20] | 55.23 (± 11.47) [2] | 57.62 (± 10.23) [1] | 55.86 (± 10.57) [2] | 51.82 (± 11.38) [5] |
| THI | 30.55 (± 10.83) [20] | 29.83 (± 10.64) [2] | 31.38 (± 11.92) [1] | 34.92 (± 10.33) [2] | 37.10 (± 11.20) [5] |
| NPI | 48.06 (± 7.26) [20] | 48.24 (± 6.99) [2] | 49.41 (± 7.82) [1] | 47.28 (± 8.56) [2] | 45.30 (± 8.40) [5] |
| TWI | 58.10 (± 7.09) [20] | 58.72 (± 6.81) [2] | 57.56 (± 7.28) [1] | 57.30 (± 7.54) [2] | 57.40 (± 6.49) [5] |
| HSI Parameters in Critically Ill COVID-19 Patients with ECMO (n = 40) | |||||
| Day 0 | Day 1 | Day 2 | Day 3 | Day 7 | |
| StO2 | 55.80 (± 12.91) [15] | 54.08 (± 12.19) [1] | 57.05 (± 11.08) [1] | 55.40 (± 11.02) [0] | 50.99 (± 12.17) [1] |
| THI | 30.37 (± 12.04) [15] | 32.26 (± 12.79) [1] | 31.38 (± 11.92) [1] | 34.98 (± 10.98) [0] | 38.24 (± 10.42) [1] |
| NPI | 48.12 (± 7.81) [15] | 48.40 (± 7.86) [1] | 49.41 (± 7.82) [1] | 47.04 (± 9.07) [0] | 44.54 (± 7.36) [1] |
| TWI | 58.94 (± 6.77) [15] | 58.37 (± 6.80) [1] | 57.56 (± 7.28) [1] | 58.33 (± 7.28) [0] | 58.87 (± 5.90) [1] |
| n obs/gr | beta | 95% CI | p Value | |
|---|---|---|---|---|
| StO2 | 233/52 | −0.250 | (−0.630; 0.117) | 0.19 |
| NPI | 233/52 | −0.308 | (−0.596; −0.035) | 0.03 |
| THI | 233/52 | 0.272 | (−0.106; 0.677) | 0.17 |
| TWI | 233/52 | 0.205 | (−0.034; 0.457) | 0.10 |
| Association of StO2, NPI, THI, TWI with Norepinephrine Dosage | ||||
| nobs/gr | beta | 95% CI | p Value | |
| StO2 | 167/49 | −4.621 | (−7.271; −1.963) | 0.001 |
| NPI | 167/49 | −3.198 | (−5.191; −1.201) | 0.002 |
| THI | 167/49 | −1.630 | (−4.483; 1.322) | 0.27 |
| TWI | 167/49 | 0.683 | (−1.228; 2.595) | 0.49 |
| Association of StO2, NPI, THI, TWI with Lactate | ||||
| nobs/gr | beta | 95% CI | p Value | |
| StO2 | 230/52 | −1.658 | (−2.370; −0.951) | 0.0000 |
| NPI | 230/52 | −1.048 | (−1.619; −0.477) | 0.0004 |
| THI | 230/52 | −0.722 | (−1.511; 0.082) | 0.08 |
| TWI | 230/52 | −0.038 | (−0.539; 0.464) | 0.88 |
| Association of StO2, NPI, THI, TWI with MAP | ||||
| nobs/gr | beta | 95% CI | p Value | |
| StO2 | 229/52 | 0.060 | (−0.025; 0.145) | 0.17 |
| NPI | 229/52 | 0.031 | (−0.037; −0.097) | 0.37 |
| THI | 229/52 | −0.060 | (−0.152; 0.031) | 0.20 |
| TWI | 229/52 | 0.067 | (0.009; 0.123) | 0.02 |
| Association of StO2, NPI, THI, TWI with SaO2 | ||||
| nobs/gr | beta | 95% CI | p Value | |
| StO2 | 229/52 | 0.283 | (0.085; 0.480) | 0.005 |
| NPI | 229/52 | 0.172 | (0.011; 0.328) | 0.03 |
| THI | 229/52 | −0.168 | (−0.384; 0.050) | 0.13 |
| TWI | 229/52 | −0.004 | (−0.141; 0.131) | 0.96 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuhlmann, H.; Garczarek, L.; Künne, D.; Pattberg, K.; Skarabis, A.; Frank, M.; Schmidt, B.; Arends, S.; Herbstreit, F.; Brenner, T.; et al. Bedside Hyperspectral Imaging and Organ Dysfunction Severity in Critically Ill COVID-19 Patients—A Prospective, Monocentric Observational Study. Bioengineering 2023, 10, 1167. https://doi.org/10.3390/bioengineering10101167
Kuhlmann H, Garczarek L, Künne D, Pattberg K, Skarabis A, Frank M, Schmidt B, Arends S, Herbstreit F, Brenner T, et al. Bedside Hyperspectral Imaging and Organ Dysfunction Severity in Critically Ill COVID-19 Patients—A Prospective, Monocentric Observational Study. Bioengineering. 2023; 10(10):1167. https://doi.org/10.3390/bioengineering10101167
Chicago/Turabian StyleKuhlmann, Henning, Lena Garczarek, David Künne, Kevin Pattberg, Annabell Skarabis, Mirjam Frank, Börge Schmidt, Sven Arends, Frank Herbstreit, Thorsten Brenner, and et al. 2023. "Bedside Hyperspectral Imaging and Organ Dysfunction Severity in Critically Ill COVID-19 Patients—A Prospective, Monocentric Observational Study" Bioengineering 10, no. 10: 1167. https://doi.org/10.3390/bioengineering10101167