
Characteristics of Abnormalities in Somatosensory Submodalities Observed in Residents Exposed to Methylmercury

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Epidemiologic Conditions and Questionnaire on Complaints
2.3. Standard Neurological Examination
2.4. Quantitative Sensory Measurements
2.4.1. Minimal Tactile Sense by Semmes–Weinstein Monofilaments
2.4.2. Vibration Sense
2.4.3. Position Sense
2.4.4. Two-Point Discrimination Sense
2.5. Neurophysiologic, Neuroradiological, and Other Laboratory Tests
2.6. Statistical Methods
2.6.1. Questionnaire and Neurological Examination
2.6.2. Percentage of Touch and Pain Disturbance
2.6.3. Relationship between Complaints and Sensory Disturbance Level
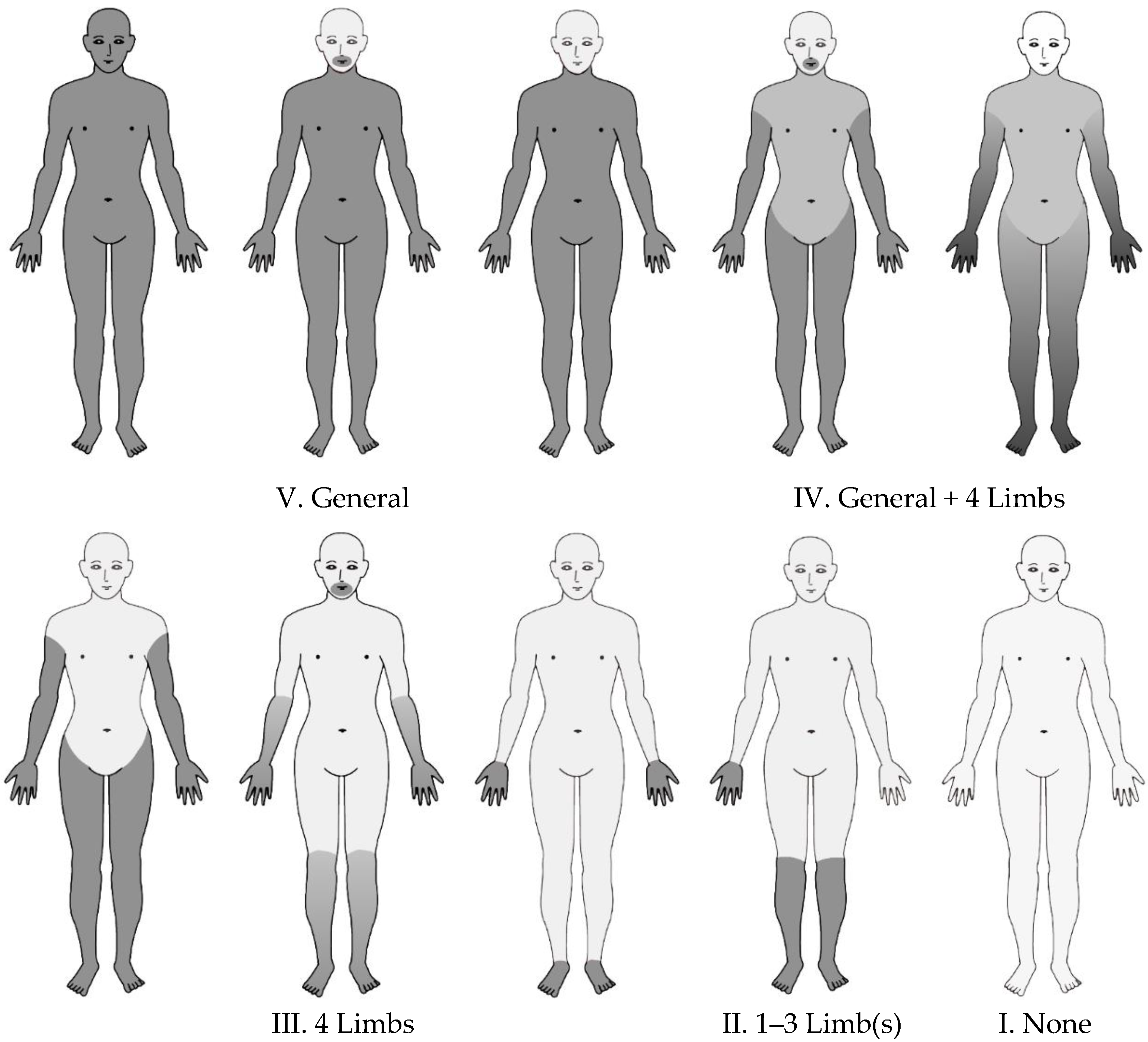
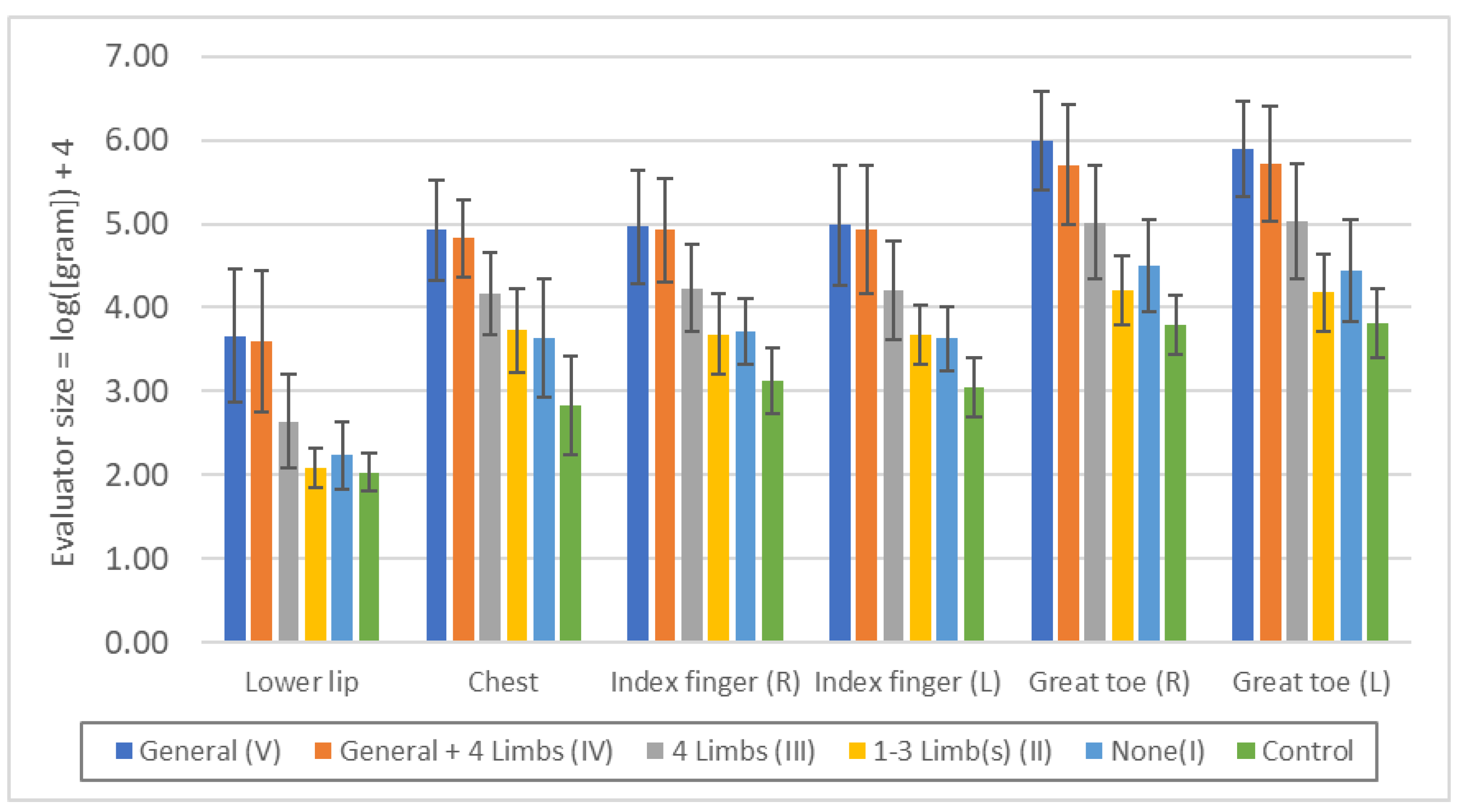
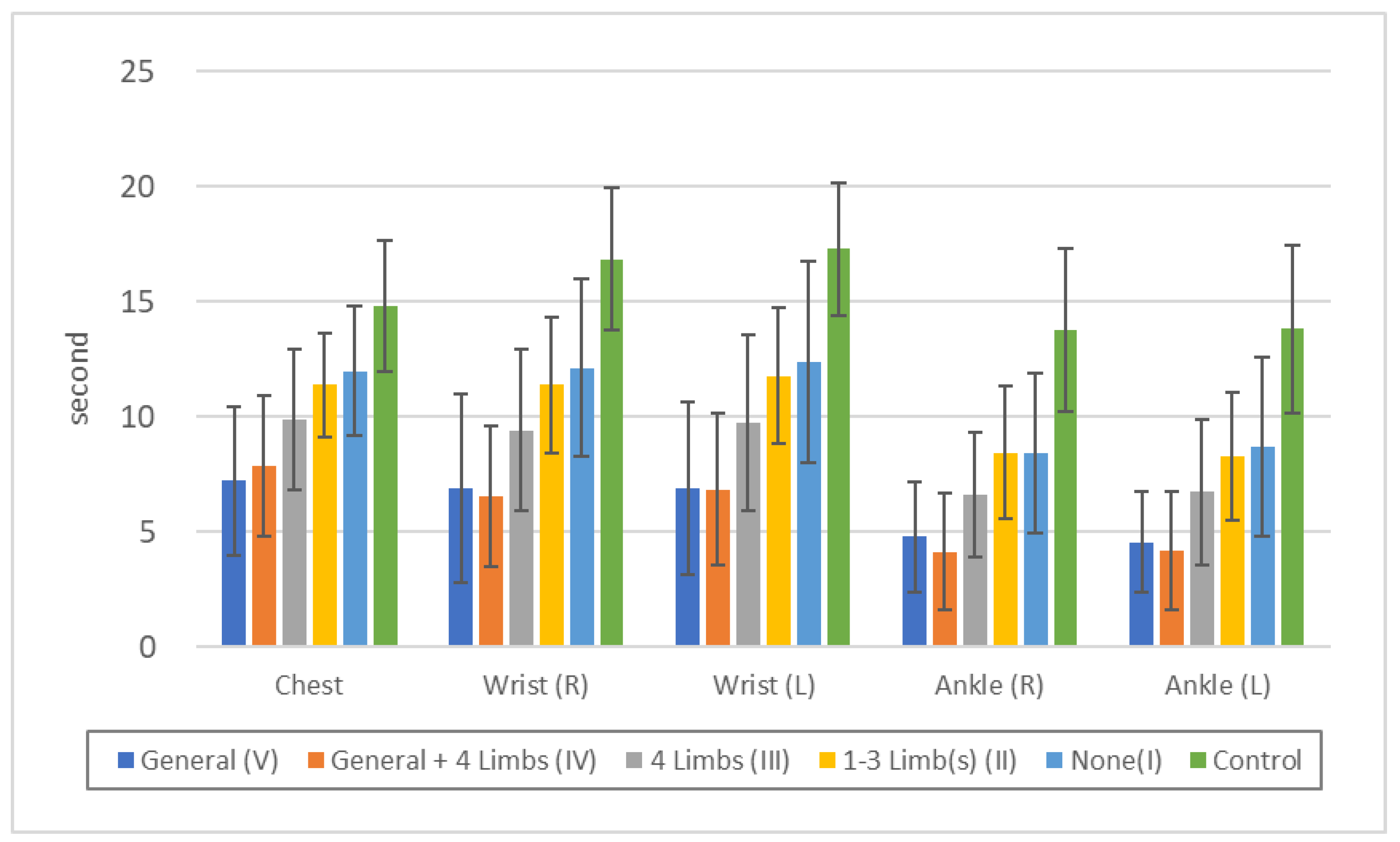
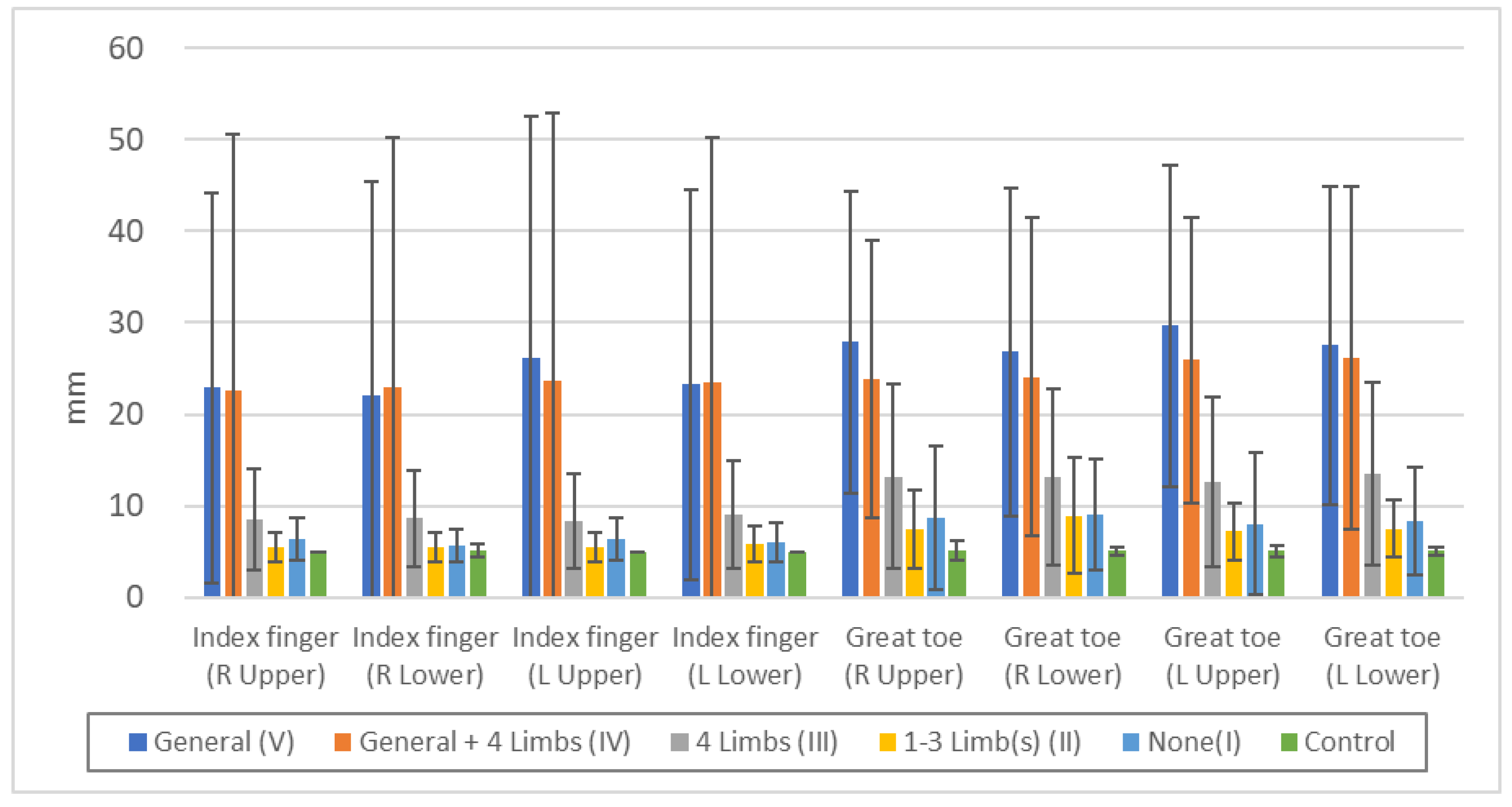
2.6.4. Relationship between Touch Disturbance Category (V–I) and Results of Quantitative Sensory Measurements, Perimeter, and Audiometry
2.6.5. Relationship Minimal Tactile Sense and Two-Point Discrimination Sense
2.6.6. Relationship between Quantitative Sensory Measurements and Results of Evoked Electromyography
3. Results
3.1. Backgrounds of Subjects
3.2. Complaints and Neurological Examination
3.3. Comparison of Touch and Pain Disturbance
3.4. Relationship between Complaints and Sensory Disturbance Level (Level 4–0)
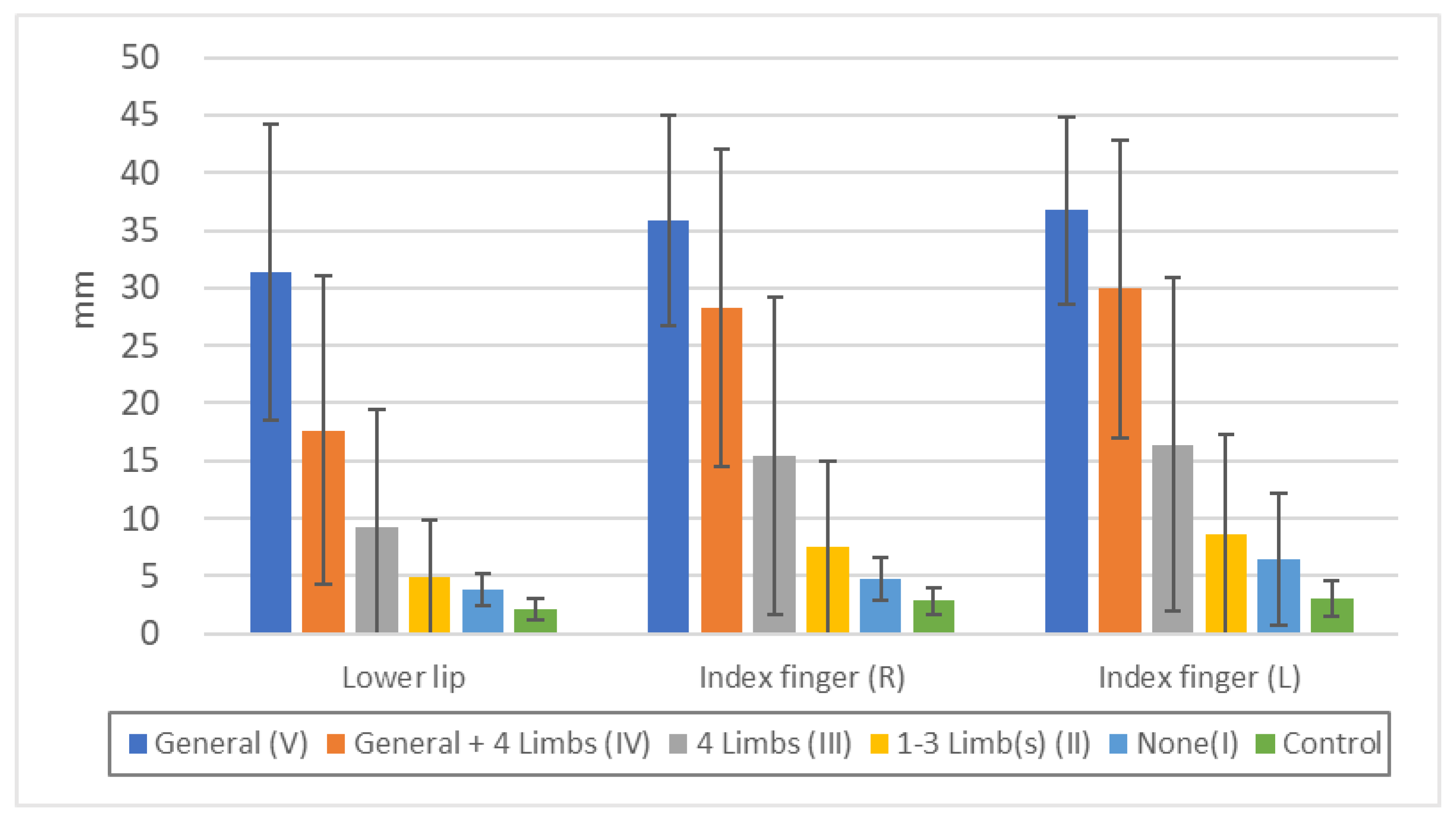
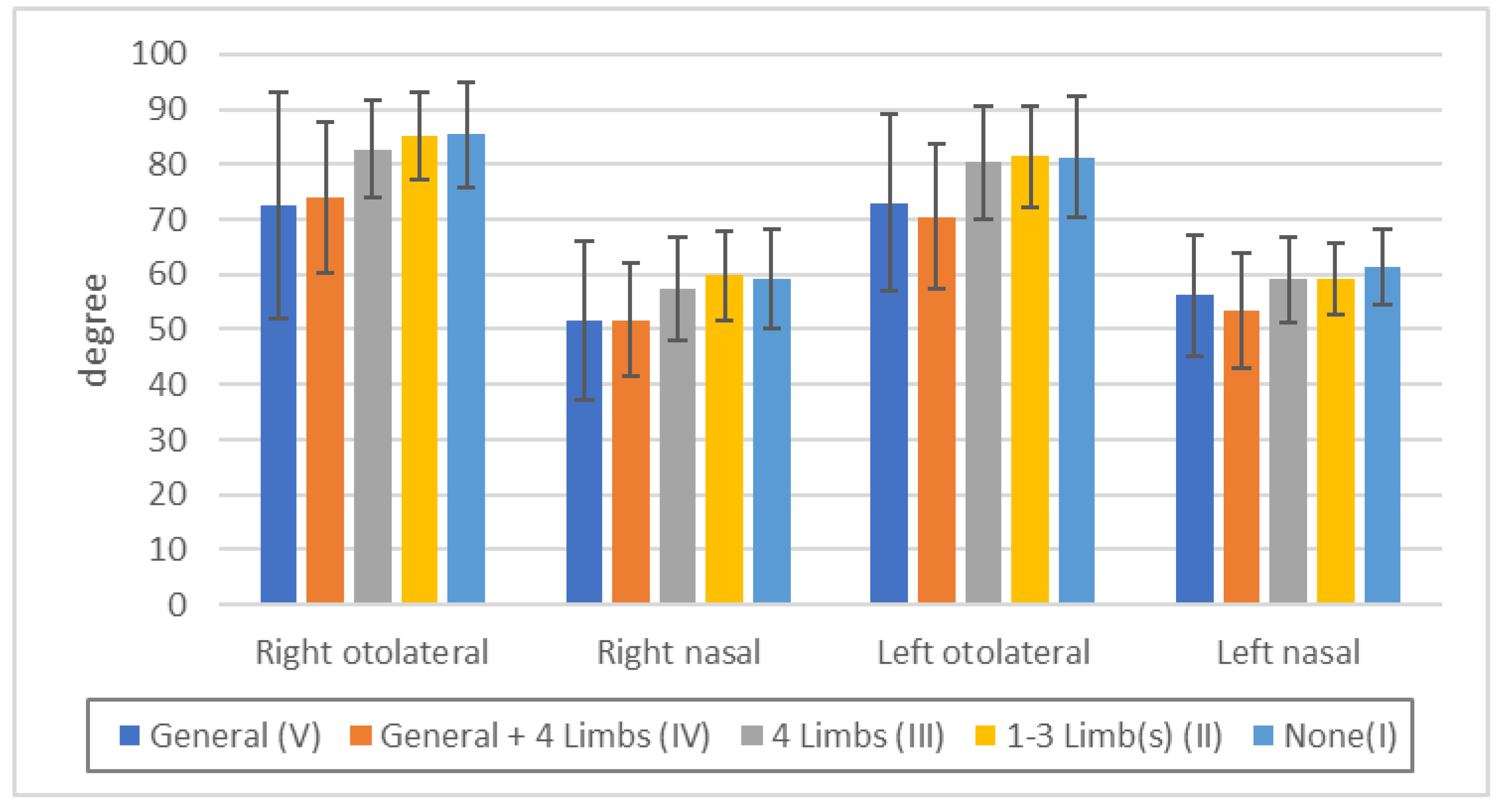
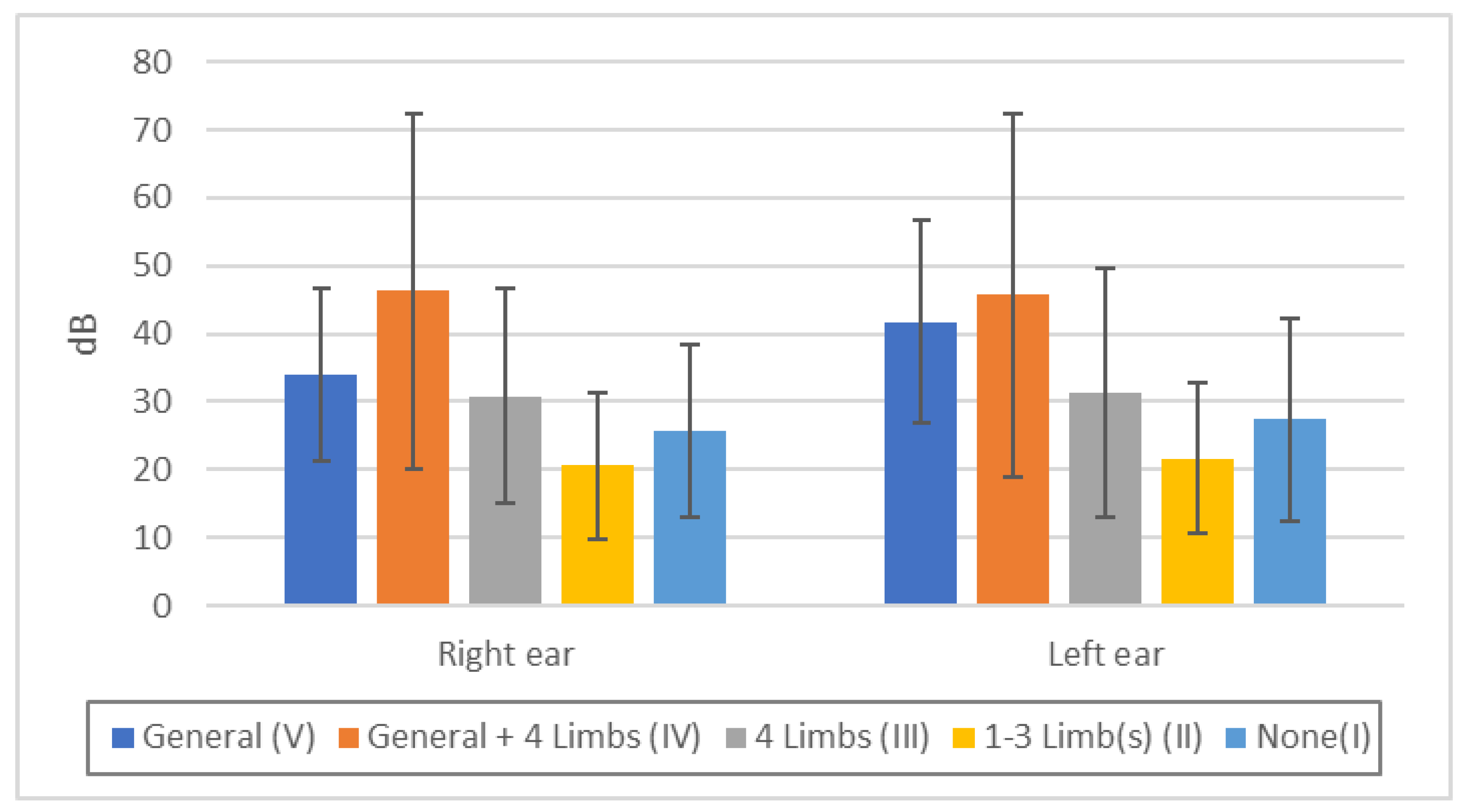
3.5. Relationship between Touch Disturbance Categories (V–I) and Quantitative Sensory Measurements, Perimeter, and Audiometry
3.6. Relationship between Minimal Tactile Sense and Two-Point Discrimination Sense
3.7. Relationship between Quantitative Sensory Measurements and Results of Evoked Electromyography
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Edwards, G. Two cases of poisoning by mercuric methide. St. Bartholomew’s Hosp. Rep. 1865, 1, 141–150. [Google Scholar]
- Hunter, D.; Bomford, R.R.; Russell, D.S. Poisoning by methyl mercury compounds. Q. J. Med. 1940, 9, 193–213. [Google Scholar]
- Harada, M. Minamata disease: Methylmercury poisoning in Japan caused by environmental pollution. Crit. Rev. Toxicol. 1995, 25, 1–24. [Google Scholar] [CrossRef]
- Bakir, F.; Rustam, H.; Tikriti, S.; Al-Damluji, S.F.; Shihristani, H. Clinical and epidemiological aspects of methylmercury poisoning. Postgrad. Med. J. 1980, 56, 1–10. [Google Scholar] [CrossRef]
- Kjellström, T.; Kennedy, P.; Wallis, S.; Stewart, A.; Friberg, L.; Lind, B.; Wutherspoon, T.; Mantell, C. Physical and Mental Development of Children with Prenatal Exposure to Mercury from Fish. Stage II. Interviews and Psychological Tests at Age 6. Report 3642; Swedish Environmental Protection Board: Solna, Sweden, 1989. [Google Scholar]
- Grandjean, P.; Weihe, P.; White, R.F.; Debes, F.; Araki, S.; Yokoyama, K.; Murata, K.; Sorensen, N.; Dahl, R.; Jorgensen, P.J. Cognitive deficit in 7-year-old children with prenatal exposure to methylmercury. Neurotoxicol. Teratol. 1997, 19, 417–428. [Google Scholar] [CrossRef]
- Karagas, M.R.; Choi, A.L.; Oken, E.; Horvat, M.; Schoeny, R.; Kamai, E.; Cowell, W.; Grandjean, P.; Korrick, S. Evidence on the human health effects of low-level methylmercury exposure. Environ. Health Perspect. 2012, 120, 799–806. [Google Scholar] [CrossRef]
- Kurland, L.T.; Faro, S.N.; Siedler, H. Minamata disease. The outbreak of a neurologic disorder in Minamata, Japan, and its relationship to the ingestion of seafood contaminated by mercuric compounds. World Neurol. 1960, 1, 370–395. [Google Scholar]
- Tsubaki, T. Tracking Minamata Disease in Niigata. Kagaku 1972, 42, 526–531. (In Japanese) [Google Scholar]
- Tsubaki, T. Recent Problems Regarding the Diagnosis of Minamata Disease. Shinkei Kenkyu No Shimpo 1974, 18, 882–889. (In Japanese) [Google Scholar]
- Ekino, S.; Ninomiya, T.; Imamura, K.; Susa, M. Methylmercury causes diffuse damage to the somatosensory cortex: How to diagnose Minamata disease. Seishin Shinkeigaku Zasshi 2007, 109, 420–437. (In Japanese) [Google Scholar]
- Ninomiya, T.; Imamura, K.; Kuwahata, M.; Kindaichi, M.; Susa, M.; Ekino, S. Reappraisal of somatosensory disorders in methylmercury poisoning. Neurotoxicol. Teratol. 2005, 27, 643–653. [Google Scholar] [CrossRef]
- Takaoka, S.; Kawakami, Y.; Fujino, T.; Oh-ishi, F.; Motokura, F.; Kumagai, Y.; Miyaoka, T. Somatosensory disturbance by methylmercury exposure. Environ. Res. 2008, 107, 6–19. [Google Scholar] [CrossRef]
- Uchino, M.; Araki, S. Clinical features of chronic Minamata disease (organic mercury poisoning). Analysis of the neurological findings in the most recent 100 cases. Rinsho Shinkeigaku 1984, 24, 235–239. (In Japanese) [Google Scholar]
- Katsuki, S.; Tokuomi, H.; Okajima, T.; Kanai, J.; Tsunoda, M.; Ishizaka, K.; Hidaka, T.; Akashi, A.; Iemura, T.; Shimada, T.; et al. Central nervous disease of unknown origin occurred in Minamata district—Especially on clinical observations. Kumamoto Med. J. 1957, 31, 23–36. (In Japanese) [Google Scholar]
- Le Quesne, P.M.; Damluji, S.F.; Rustam, H. Electrophysiological studies of peripheral nerves in patients with organic mercury poisoning. J. Neurol. Neurosurg. Psychiatry 1974, 37, 333–339. [Google Scholar] [CrossRef]
- Snyder, R.D.; Seelinger, D.F. Methylmercury poisoning, Clinical follow-up and sensory nerve conduction studies. J. Neurol. Neurosurg. Psychiatry 1976, 39, 701–704. [Google Scholar] [CrossRef]
- Oliveira, R.A.A.; Pinto, B.D.; Reboucas, B.H.; Ciampi de Andrade, D.; Vasconcellos, A.C.S.; Basta, P.C. Neurological Impacts of Chronic Methylmercury Exposure in Munduruku Indigenous Adults: Somatosensory, Motor, and Cognitive Abnormalities. Int. J. Environ. Res. Public Health 2021, 18, 10270. [Google Scholar] [CrossRef]
- Khoury, E.D.; Souza Gda, S.; da Costa, C.A.; de Araujo, A.A.; de Oliveira, C.S.; Silveira, L.C.; Pinheiro Mda, C. Somatosensory Psychophysical Losses in Inhabitants of Riverside Communities of the Tapajos River Basin, Amazon, Brazil: Exposure to Methylmercury Is Possibly Involved. PLoS ONE 2015, 10, e0144625. [Google Scholar] [CrossRef]
- Nierenberg, D.W.; Nordgren, R.E.; Chang, M.B.; Siegler, R.W.; Blayney, M.B.; Hochberg, F.; Toribara, T.Y.; Cernichiari, E.; Clarkson, T. Delayed cerebellar disease and death after accidental exposure to dimethylmercury. N. Engl. J. Med. 1998, 338, 1672–1676. [Google Scholar] [CrossRef]
- Kandel, E.R. Nerve Cell and Behavior. In Principles of Neural Science, 4th ed.; Kandel, E.R., Schwartz, J.H., Jessell, T.M., Eds.; McGraw-Hill Companies: New York, NY, USA, 2000; p. 34. [Google Scholar]
- Miura, K.; Suzuki, K.; Imura, N. Effects of methylmercury on mitotic mouse glioma cells. Environ. Res. 1978, 17, 453–471. [Google Scholar] [CrossRef]
- Imura, N.; Miura, K.; Inokawa, M.; Nakada, S. Mechanism of methylmercury cytotoxicity: By biochemical and morphological experiments using cultured cells. Toxicology 1980, 17, 241–254. [Google Scholar] [CrossRef]
- Ben-Ze’ev, A.; Farmer, S.R.; Penman, S. Mechanisms of regulating tubulin synthesis in cultured mammalian cells. Cell 1979, 17, 319–325. [Google Scholar] [CrossRef]
- Sager, P.R.; Doherty, R.A.; Olmsted, J.B. Interaction of methylmercury with microtubules in cultured cells and in vitro. Exp. Cell Res. 1983, 146, 127–137. [Google Scholar] [CrossRef]
- Kawamori, Y.; Tokuomi, H.; Okajima, T.; Kanai, J.; Tsunoda, M.; Ishizaka, K.; Murohara, I.; Akatsuka, A.; Iemura, T.; Yonemitsu, K.; et al. Central nervous disease of unknown origin occurred in Minamata district—Follow-up report. Kumamoto Med. J. 1957, 31, 251–261. (In Japanese) [Google Scholar]
- Tatetsu, S.; Murayama, E.; Harada, M.; Miyakawa, T. Sequelae of acquired Minamata disease. Symptoms and changes 4 1/2–7 1/2 years from onset. Shinkei Kenkyu No Shimpo 1969, 13, 76–83. (In Japanese) [Google Scholar]
- Weiss, B.; Clarkson, T.W.; Simon, W. Silent latency periods in methylmercury poisoning and in neurodegenerative disease. Environ. Health Perspect. 2002, 110 (Suppl. S5), 851–854. [Google Scholar] [CrossRef]
- Takaoka, S.; Fujino, T.; Kawakami, Y.; Shigeoka, S.I.; Yorifuji, T. Survey of the Extent of the Persisting Effects of Methylmercury Pollution on the Inhabitants around the Shiranui Sea, Japan. Toxics 2018, 6, 39. [Google Scholar] [CrossRef]
- Shirakawa, K. Delayed Onset Minamata disease. In Minamata Disease—20 Years of Research and Current Challenges; Arima, S., Ed.; Seirin-Sha: Tokyo, Japan, 1979; pp. 331–344. (In Japanese) [Google Scholar]
- Louis, E.D. Merritt’s Neurology, 14th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2021. [Google Scholar]
- Axelrod, F.B.; Gold-von Simson, G. Hereditary sensory and autonomic neuropathies: Types II, III, and IV. Orphanet. J. Rare Dis. 2007, 2, 39. [Google Scholar] [CrossRef]
- Sterman, A.B.; Schaumburg, H.H.; Asbury, A.K. The acute sensory neuronopathy syndrome: A distinct clinical entity. Ann. Neurol. 1980, 7, 354–358. [Google Scholar] [CrossRef]
- Bakir, F.; Damluji, S.F.; Amin-Zaki, L.; Murtadha, M.; Khalidi, A.; Al-Rawi, N.Y.; Tikriti, S.; Dahahir, H.I.; Clarkson, T.W.; Smith, J.C.; et al. Methylmercury poisoning in Iraq. Science 1973, 181, 230–241. [Google Scholar] [CrossRef]
- Living Hygiene Division. Niigata Prefecture. Niigata Mercury Poisoning Incident Special Study Report (Ministry of Health and Welfare, Research Division), 1967. pp. 88–94. Available online: https://wedocs.unep.org/xmlui/bitstream/handle/20.500.11822/29275/EHC1MERCURY.pdf?sequence=1&isAllowed=y (accessed on 11 December 2023).
- Cinca, I.; Dumitrescu, I.; Onaca, P.; Serbanescu, A.; Nestorescu, B. Accidental ethyl mercury poisoning with nervous system, skeletal muscle, and myocardium injury. J. Neurol. Neurosurg. Psychiatry 1980, 43, 143–149. [Google Scholar] [CrossRef]
- Nagaki, J.; Ohnishi, A.; Kuroiwa, Y. Electrophysiologic and histopathologic studies on sural nerves from Minamata disease patients of delayed onset showing distal sensory impairments. Rinsho Shinkeigaku 1985, 25, 88–94. (In Japanese) [Google Scholar]
- Hunter, D.; Russell, D.S. Focal cerebral and cerebellar atrophy in a human subject due to organic mercury compounds. J. Neurol. Neurosurg. Psychiatry 1954, 17, 235–241. [Google Scholar] [CrossRef]
- Takeuchi, T.; Kambara, T.; Morikawa, N.; Matsumoto, H.; Shiraishi, Y.; Ito, H. Pathologic observations of the Minamata disease. Acta Pathol. Jpn. 1959, 9, 769–783. [Google Scholar] [CrossRef]
- Eto, K.; Okajima, T. Clinico-pathological Study on the Autopsy Cases Showing Glove-and-stocking Type Sensory Disturbance in Relation to Minamata Disease. Kumamoto Med. J. 1994, 68, 59–71. (In Japanese) [Google Scholar]
- Dyck, P.T. Pathology of the peripheral nervous system. In Peripheral Neuropathy, 3rd ed.; Dyck, P.T., Thomas, P.K., Eds.; W.B. Saunders Company: Philadelphia, PA, USA, 1993; p. 533. [Google Scholar]
- Eto, K.; Tokunaga, H.; Nagashima, K.; Takeuchi, T. An autopsy case of minamata disease (methylmercury poisoning)--pathological viewpoints of peripheral nerves. Toxicol. Pathol. 2002, 30, 714–722. [Google Scholar] [CrossRef]
- Eto, K. Two autopsy cases of clinical Minamata disease without pathological findings of organic mercury toxicosis. Neuropathology 1988, 8, 289–300. (In Japanese) [Google Scholar]
- Ikuta, F. LETTERS The reality underlying the diagnosis, recognition and sentencing of Minamata disease symptoms: From the number of nerve cell dropouts. Brain Nerve 2018, 70, 938–942. (In Japanese) [Google Scholar]
- Hanewinckel, R.; van Oijen, M.; Ikram, M.A.; van Doorn, P.A. The epidemiology and risk factors of chronic polyneuropathy. Eur. J. Epidemiol. 2016, 31, 5–20. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Touch Disturbance | Pain Disturbance | |
|---|---|---|
| Level 4 | type V, IV | type V, IV |
| Level 3 | type V, IV | type III, II, I |
| type III, II, I | type V, IV | |
| Level 2 | type III | type III |
| Level 1 | type III | type II, I |
| type II, I | type III | |
| Level 0 | type II, I | type II, I |
| Group E | Group E + N | Exposed (Total) | Control | ||
|---|---|---|---|---|---|
| (n = 81) | (n = 116) | (n = 197) | (n = 130) | ||
| Sex, n (%) | |||||
| Male | 26 (32.1) | 54 (46.6) | 80 (40.6) | 51 (39.2) | |
| Female | 55 (67.9) | 62 (53.4) | 117 (59.4) | 79 (60.8) | |
| Age ** | |||||
| Mean ± SD | 59.9 ± 11.8 | 65.6 ± 9.2 | 63.2 ± 10.7 | 63.7 ± 9.3 | |
| Range (min–max) | 37–85 | 43–89 | 37–89 | 50–86 | |
| Smoking, n (%) | |||||
| Non-smoker | 46 (69.7) | 74 (69.8) | 120 (69.8) | 102 (79.1) | |
| Smoker | 20 (30.3) | 32 (30.2) | 52 (30.2) | 27(20.9) | |
| Alcohol drinking, n (%) * | |||||
| Non-drinker | 42 (66.7) | 67 (65.7) | 109 (66.1) | 67 (51.9) | |
| Drinker | 21 (33.3) | 35 (34.3) | 56 (33.9) | 62 (48.1) | |
| Frequency of fish intake, n (%) ** | |||||
| Three times a day | 43 (53.8) | 43 (37.4) | 86 (44.1) | 6 (4.8) | |
| Twice a day | 20 (25.0) | 45 (39.1) | 65 (33.3) | 7 (5.6) | |
| Once a day | 15 (18.8) | 21 (18.3) | 36 (18.5) | 26 (20.8) | |
| More than once a week | 2 (2.5) | 3 (2.6) | 5 (2.6) | 59 (47.2) | |
| Less than once a week | 0 (0.0) | 3 (2.6) | 3 (1.5) | 27 (21.6) | |
| Occupation, n (%) | |||||
| Non-Fishermen (subject) ** | 72 (88.9) | 108 (93.1) | 180 (91.4) | 130 (100) | |
| Fishermen (subject) | 9 (11.1) | 8 (6.9) | 17 (8.6) | 0 (0.0) | |
| Non-Fishermen (subject’s parent) ** | 44 (54.3) | 87 (76.3) | 131 (67.2) | 116 (99.1) | |
| Fishermen (subject’s parent) | 37 (45.7) | 27 (23.7) | 64 (32.8) | 1 (0.9) | |
| Neurologically related complications, n (%) a | |||||
| Diabetes Mellitus | 0 (0.0) | 34 (29.3) | 34 (17.3) | 3 (2.3) | |
| Cervical Spondylosis | 0 (0.0) | 54 (46.6) | 54 (27.4) | 13 (10.0) | |
| Lumbar Spondylosis | 0 (0.0) | 15 (12.9) | 15 (7.6) | 0 (0.0) | |
| Carpal Tunnel Syndrome | 0 (0.0) | 37 (31.9) | 37 (18.8) | 0 (0.0) | |
| Cerebrovascular Diseases | 0 (0.0) | 29 25.0) | 29 (14.7) | 1 (0.8) | |
| Other Neurological Diseases | 0 (0.0) | 14 (12.1) | 14 (7.1) | 2 (1.5) | |
| Total | 0 (0.0) | 116 (100) | 116 (58.9) | 18 (13.8) | |
| Family history, n (%) ** | |||||
| Minamata disease (−) | 23 (28.4) | 31 (27.0) | 54 (27.6) | 130 (100) | |
| Minamata disease (+) | 58 (71.6) | 84 (73.0) | 142 (72.4) | 0 (0.0) | |
| No | Questionnaire | Group E | Group E + N | Exposed (Total) | Control |
|---|---|---|---|---|---|
| 1 | Sensory numbness in both hands | 43% | 55% | 50% | 2% |
| 2 | Sensory numbness in both legs | 38% | 47% | 44% | 1% |
| 3 | Hot sensation in the hand | 12% | 12% | 12% | 0% |
| 4 | Hot sensation in the leg | 17% | 20% | 19% | 0% |
| 5 | No pain when burn or wounded | 12% | 19% | 16% | 0% |
| 6 | Difficulty in judging the adequate temperature of bath water | 9% | 17% | 14% | 0% |
| 7 | Hanging a bag with elbow or shoulder instead of holding it in your hand | 32% | 36% | 34% | 2% |
| 8 | Headache | 36% | 28% | 32% | 0% |
| 9 | Shoulder stiffness | 65% | 68% | 67% | 9% |
| 10 | Lower back pain | 53% | 57% | 55% | 6% |
| 11 | Muscle cramps | 24% | 33% | 30% | 4% |
| 12 | Disturbed vision | 43% | 59% | 53% | 3% |
| 13 | Limited peripheral vision | 28% | 36% | 33% | 1% |
| 14 | Difficulty in recognizing a thing in your sight when you continue to stare it | 19% | 26% | 24% | 0% |
| 15 | Difficulty in finding a good in the shop | 39% | 33% | 35% | 1% |
| 16 | Difficulty in hearing | 27% | 47% | 39% | 10% |
| 17 | Difficulty in understanding a word or a sentence even if you can hear it | 8% | 16% | 13% | 1% |
| 18 | Tinnitus | 28% | 37% | 33% | 6% |
| 19 | Difficulty in smelling | 16% | 27% | 23% | 1% |
| 20 | Difficulty in tasting | 18% | 19% | 19% | 0% |
| 21 | Difficulty in judging the taste of your own cooking | 14% | 14% | 14% | 1% |
| 22 | Stumbling on flat ground | 4% | 12% | 9% | 0% |
| 23 | Difficulty in wearing slippers | 21% | 36% | 30% | 0% |
| 24 | Coming off your slippers or sandals while walking | 17% | 29% | 24% | 0% |
| 25 | Difficulty in fine finger task | 52% | 63% | 58% | 0% |
| 26 | Difficulty in buttoning | 14% | 38% | 29% | 0% |
| 27 | Dropping things in the hand | 14% | 26% | 21% | 0% |
| 28 | Dropping chopsticks while eating | 4% | 12% | 9% | 0% |
| 29 | Difficulty in speaking words or sentences well | 5% | 18% | 13% | 0% |
| 30 | Hand weakness | 57% | 59% | 58% | 2% |
| 31 | Leg weakness | 46% | 58% | 53% | 2% |
| 32 | Hand tremor while moving | 17% | 27% | 23% | 2% |
| 33 | Hand tremor at rest | 10% | 18% | 15% | 1% |
| 34 | Vertigo (feeling of spinning around) | 9% | 10% | 9% | 0% |
| 35 | Swaying dizziness | 8% | 8% | 8% | 0% |
| 36 | Fainting (syncope like) dizziness | 4% | 4% | 4% | 0% |
| 37 | Dizziness when standing up | 18% | 13% | 15% | 0% |
| 38 | General fatigue | 41% | 39% | 40% | 1% |
| 39 | Difficulty in sleeping | 31% | 41% | 37% | 4% |
| 40 | Appetite loss | 9% | 7% | 8% | 0% |
| 41 | No will to do anything | 23% | 27% | 26% | 1% |
| 42 | Cannot persevere or cannot keep working | 25% | 38% | 33% | 0% |
| 43 | Feeling as if your mind has become blank or empty | 3% | 10% | 7% | 0% |
| 44 | Cannot think about anything | 3% | 10% | 7% | 0% |
| 45 | Losing your train of thought during conversation | 10% | 16% | 14% | 0% |
| 46 | Forgetfulness | 32% | 41% | 37% | 1% |
| 47 | Feeling as if you are not yourself | 8% | 11% | 10% | 0% |
| 48 | Irritation | 32% | 31% | 31% | 0% |
| 49 | Feeling sad | 16% | 17% | 17% | 0% |
| 50 | Difficulty in finding something when interrupted | 22% | 30% | 27% | 2% |
| No | Questionnaire | Group E | Group E + N | Exposed (Total) | Control |
|---|---|---|---|---|---|
| 1 | Sensory numbness in both hands | 90% | 91% | 91% | 8% |
| 2 | Sensory numbness in both legs | 90% | 83% | 86% | 8% |
| 3 | Hot sensation in the hand | 46% | 45% | 46% | 0% |
| 4 | Hot sensation in the leg | 56% | 55% | 56% | 1% |
| 5 | No pain when burn or wounded | 41% | 46% | 44% | 0% |
| 6 | Difficulty in judging the adequate temperature of bath water | 41% | 36% | 38% | 1% |
| 7 | Hanging a bag with elbow or shoulder instead of holding it in your hand | 68% | 71% | 70% | 3% |
| 8 | Headache | 86% | 82% | 83% | 23% |
| 9 | Shoulder stiffness | 96% | 92% | 94% | 50% |
| 10 | Lower back pain | 88% | 90% | 90% | 51% |
| 11 | Muscle cramps | 97% | 88% | 92% | 40% |
| 12 | Disturbed vision | 80% | 90% | 86% | 19% |
| 13 | Limited peripheral vision | 67% | 66% | 66% | 8% |
| 14 | Difficulty in recognizing a thing in your sight when you continue to stare it | 57% | 62% | 60% | 2% |
| 15 | Difficulty in finding a good in the shop | 78% | 71% | 74% | 9% |
| 16 | Difficulty in hearing | 62% | 79% | 72% | 20% |
| 17 | Difficulty in understanding a word or a sentence even if you can hear it | 49% | 52% | 51% | 7% |
| 18 | Tinnitus | 75% | 77% | 76% | 17% |
| 19 | Difficulty in smelling | 49% | 50% | 50% | 6% |
| 20 | Difficulty in tasting | 47% | 43% | 45% | 2% |
| 21 | Difficulty in judging the taste of your own cooking | 46% | 41% | 43% | 2% |
| 22 | Stumbling on flat ground | 64% | 72% | 68% | 2% |
| 23 | Difficulty in wearing slippers | 62% | 78% | 71% | 2% |
| 24 | Coming off your slippers or sandals while walking | 69% | 78% | 74% | 2% |
| 25 | Difficulty in fine finger task | 86% | 86% | 86% | 9% |
| 26 | Difficulty in buttoning | 53% | 69% | 62% | 0% |
| 27 | Dropping things in the hand | 76% | 80% | 78% | 7% |
| 28 | Dropping chopsticks while eating | 61% | 65% | 64% | 1% |
| 29 | Difficulty in speaking words or sentences well | 51% | 63% | 58% | 3% |
| 30 | Hand weakness | 83% | 84% | 84% | 7% |
| 31 | Leg weakness | 83% | 79% | 81% | 5% |
| 32 | Hand tremor while moving | 71% | 72% | 72% | 6% |
| 33 | Hand tremor at rest | 51% | 50% | 51% | 1% |
| 34 | Vertigo (feeling of spinning around) | 70% | 61% | 64% | 7% |
| 35 | Swaying dizziness | 57% | 58% | 58% | 5% |
| 36 | Fainting (syncope like) dizziness | 49% | 43% | 46% | 2% |
| 37 | Dizziness when standing up | 89% | 78% | 82% | 15% |
| 38 | General fatigue | 89% | 82% | 85% | 20% |
| 39 | Difficulty in sleeping | 86% | 78% | 81% | 21% |
| 40 | Appetite loss | 44% | 42% | 43% | 3% |
| 41 | No will to do anything | 85% | 88% | 86% | 21% |
| 42 | Cannot persevere or cannot keep working | 73% | 74% | 74% | 14% |
| 43 | Feeling as if your mind has become blank or empty | 56% | 56% | 56% | 6% |
| 44 | Cannot think about anything | 49% | 56% | 53% | 2% |
| 45 | Losing your train of thought during conversation | 68% | 73% | 71% | 8% |
| 46 | Forgetfulness | 96% | 95% | 95% | 59% |
| 47 | Feeling as if you are not yourself | 38% | 51% | 46% | 0% |
| 48 | Irritation | 94% | 81% | 86% | 33% |
| 49 | Feeling sad | 76% | 69% | 72% | 19% |
| 50 | Difficulty in finding something when interrupted | 81% | 80% | 81% | 15% |
| Findings | Group E | Group E + N | Exposed (Total) | Control | |
|---|---|---|---|---|---|
| 1 | Dysarthria | 17.3% | 30.2% | 24.9% | 1.6% |
| 2 | Hearing loss | 28.9% | 53.7% | 43.5% | 7.8% |
| 3 | Visual field disturbance | 27.5% | 30.1% | 29.0% | 0.0% |
| 4 | Normal gait disturbance (distinct) | 25.9% | 25.4% | 25.6% | 0.0% |
| 5 | Normal gait disturbance (mild-distinct) | 30.9% | 41.2% | 36.9% | 0.0% |
| 6 | Tandem gait disturbance (distinct) | 17.3% | 34.5% | 27.4% | 1.6% |
| 7 | Tandem gait disturbance (mild-distinct) | 66.7% | 80.2% | 74.6% | 11.6% |
| 8 | Romberg sign | 5.3% | 10.3% | 8.2% | 0.8% |
| 9 | One-foot standing abnormality (eyes open) (distinct) | 21.5% | 41.4% | 33.3% | 1.5% |
| 10 | One-foot standing abnormality (eyes open) (mild-distinct) | 62.0% | 78.4% | 71.8% | 12.3% |
| 11 | Finger-nose test (eyes open) (distinct) | 14.8% | 26.7% | 21.8% | 0.0% |
| 12 | Finger-nose test (eyes open) (mild-distinct) | 46.9% | 59.5% | 54.3% | 0.0% |
| 13 | Adiadokokinesis (distinct) | 12.5% | 27.0% | 21.0% | 0.0% |
| 14 | Adiadokokinesis (mild-distinct) | 31.3% | 58.3% | 47.2% | 2.3% |
| 15 | Heel-knee test (distinct) | 18.3% | 27.3% | 23.5% | 0.0% |
| 16 | Heel-knee test (mild-distinct) | 49.3% | 55.6% | 52.9% | 2.3% |
| 17 | Postural hand tremor | 24.3% | 22.9% | 23.5% | 3.3% |
| 18 | Touch disturbance (four-limb peripheral) | 77.8% | 87.8% | 83.7% | 0.8% |
| 19 | Touch disturbance (oral) | 23.5% | 26.1% | 25.0% | 0.0% |
| 20 | Touch disturbance (systemic) | 21.0% | 16.5% | 18.4% | 0.0% |
| 21 | Pain disturbance (four-limb peripheral) | 93.8% | 95.7% | 94.9% | 1.5% |
| 22 | Pain disturbance (oral) | 35.8% | 49.1% | 43.7% | 0.0% |
| 23 | Pain disturbance (systemic) | 35.8% | 43.1% | 40.1% | 0.0% |
| Pain | General (V) | General + 4 Limbs (IV) | 4 Limbs (III) | 1–3 Limb(s) (II) | None (I) | Total (%) | |
|---|---|---|---|---|---|---|---|
| Touch | |||||||
| General (V) | 10 | 4 | 0 | 0 | 0 | 14 (7) | |
| General + 4 Limbs (IV) | 0 | 21 | 1 | 0 | 0 | 22 (11) | |
| 4 Limbs (III) | 7 | 31 | 90 | 0 | 0 | 128 (65) | |
| 1–3 Limb(s) (II) | 0 | 2 | 10 | 3 | 3 | 18 (9) | |
| None (I) | 3 | 1 | 7 | 0 | 4 | 15 (8) | |
| Total (%) | 20 (10) | 59 (30) | 108 (55) | 3 (2) | 7 (4) | 197 (100) | |
| Age | n (M/F) | |
|---|---|---|
| General (V) | 65.9 ± 9.8 | 14 (6/8) |
| General + 4 Limbs (IV) | 66.8 ± 10.6 | 22 (12/10) |
| 4 Limbs (III) | 63.4 ± 10.0 | 128 (50/78) |
| 1–3 Limb(s) (II) | 57.6 ± 9.9 | 18 (6/12) |
| None (I) | 61.1 ± 15.5 | 15 (6/9) |
| Control | 63.7 ± 9.3 | 130 (51/79) |
| General (V) | General + 4 Limbs (IV) | 4 Limbs (II/I) | 1–3 Limb(s) (II) | None (I) | |
|---|---|---|---|---|---|
| General + 4 Limbs (IV) | 0.399 | ||||
| 4 Limbs (III) | 0.182 | 0.080 | |||
| 1–3 Limb(s) (II) | 0.012 * | 0.004 ** | 0.011 * | ||
| None (I) | 0.162 | 0.112 | 0.289 | 0.224 | |
| Control | 0.207 | 0.096 | 0.411 | 0.013 * | 0.267 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takaoka, S.; Fujino, T.; Shigeoka, S.-i.; Yorifuji, T. Characteristics of Abnormalities in Somatosensory Submodalities Observed in Residents Exposed to Methylmercury. Toxics 2023, 11, 1023. https://doi.org/10.3390/toxics11121023
Takaoka S, Fujino T, Shigeoka S-i, Yorifuji T. Characteristics of Abnormalities in Somatosensory Submodalities Observed in Residents Exposed to Methylmercury. Toxics. 2023; 11(12):1023. https://doi.org/10.3390/toxics11121023
Chicago/Turabian StyleTakaoka, Shigeru, Tadashi Fujino, Shin-ichi Shigeoka, and Takashi Yorifuji. 2023. "Characteristics of Abnormalities in Somatosensory Submodalities Observed in Residents Exposed to Methylmercury" Toxics 11, no. 12: 1023. https://doi.org/10.3390/toxics11121023