
Estimation of the Cadmium Nephrotoxicity Threshold from Loss of Glomerular Filtration Rate and Albuminuria

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cohort Participants
2.2. Assessment of Cadmium Exposure and Adverse Effects
2.3. Estimated Glomerular Filtration Rate (eGFR)
2.4. Normalization of Excretion Rate
2.5. Statistical Analysis
3. Results
3.1. Cohort Participants
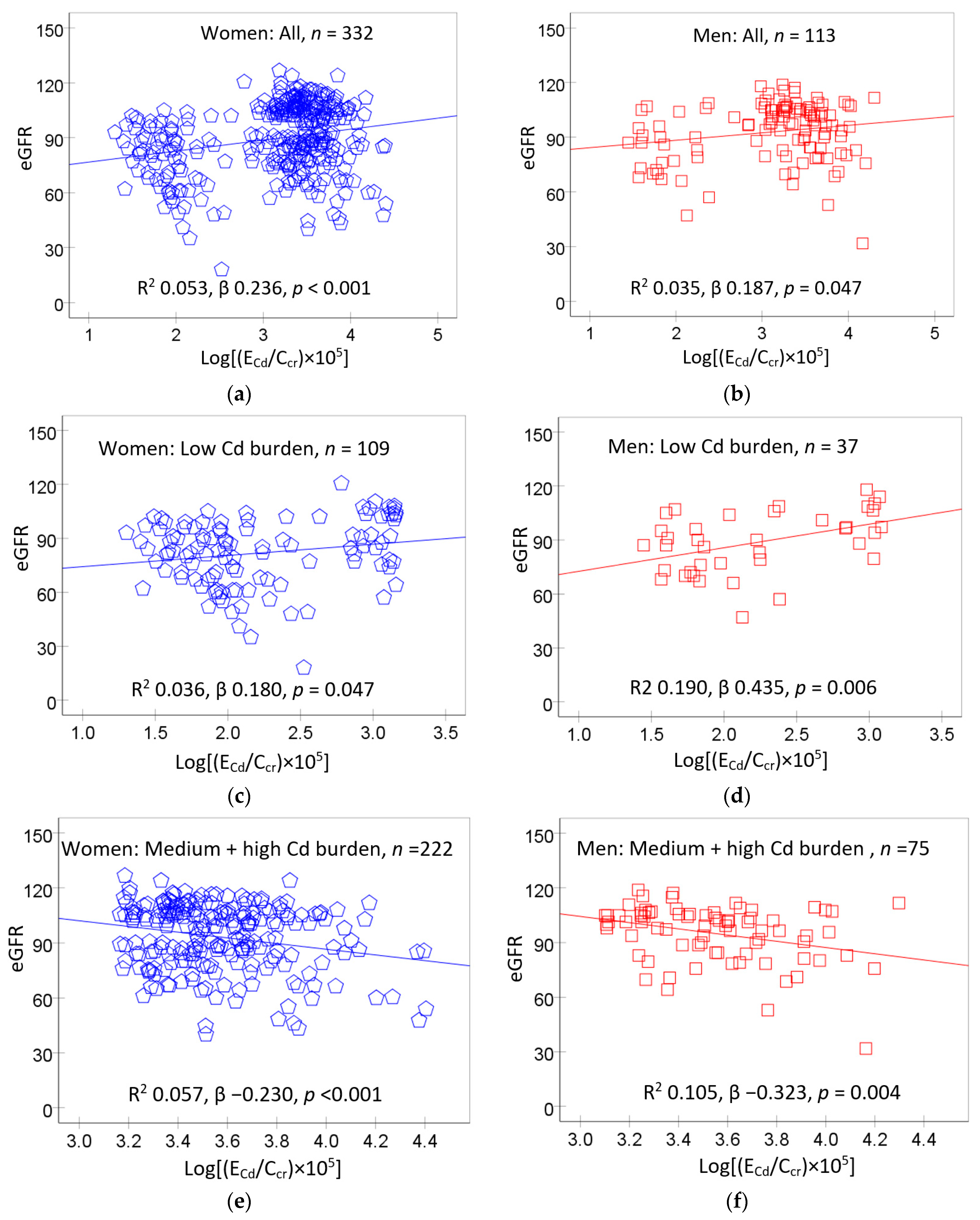
3.2. Predictors of eGFR
3.3. Logistic Regression Analysis of Low eGFR
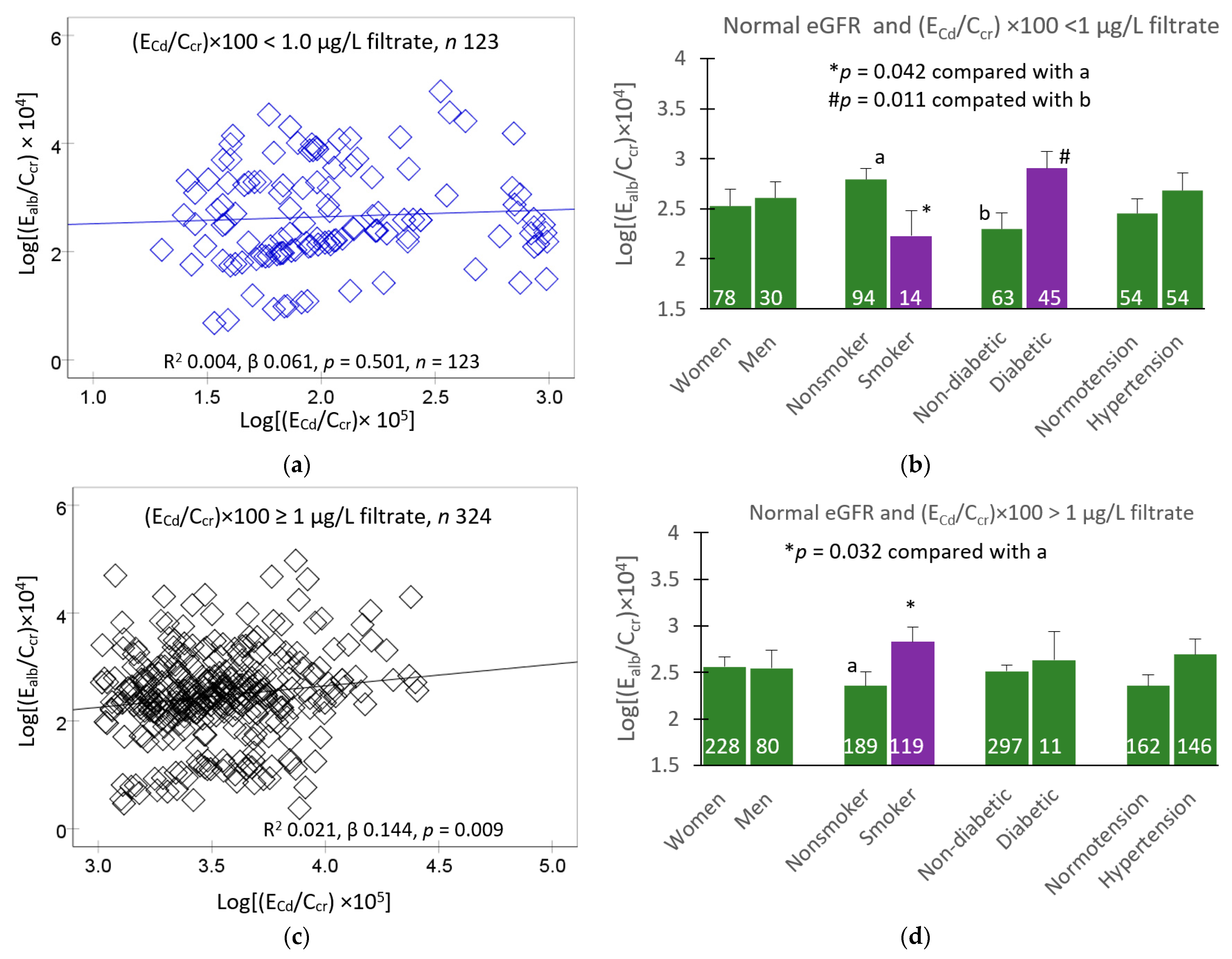
3.4. Multiple Regression Analysis of Albumin Excretion Rate
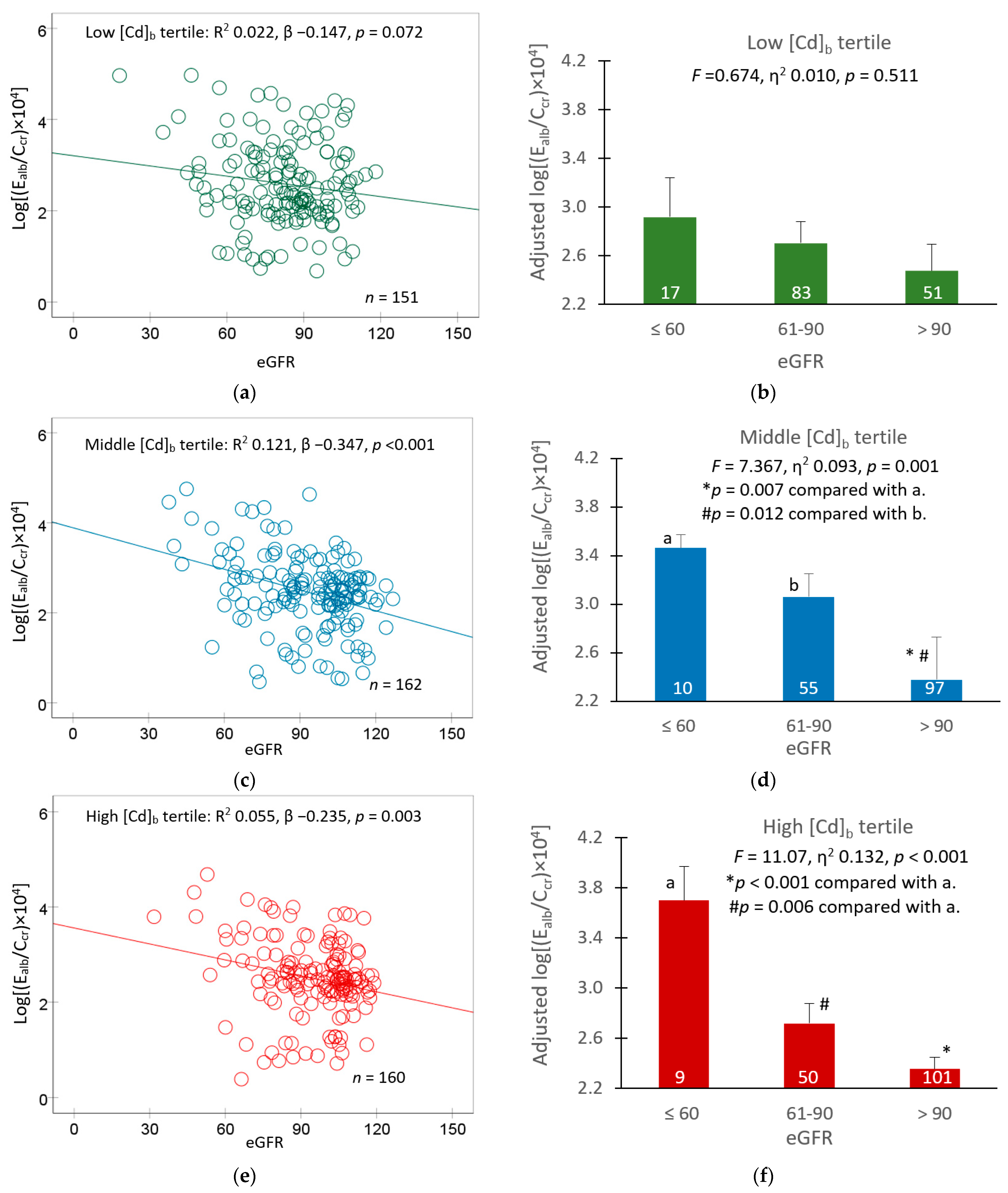
3.5. Blood Cadmium and eGFR as Predictors of Albuminuria
4. Discussion
4.1. Effects of Cadmium on eGFR
4.2. Effects of Cadmium on Prevalence of Albuminuria
4.3. A Independent Effect of Smoking on Albuminuria
4.4. Threshold-Based Exposure Guidelines
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levey, A.S.; Becker, C.; Inker, L.A. Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: A systematic review. JAMA 2015, 313, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Jafar, T.H.; Nitsch, D.; Neuen, B.L.; Perkovic, V. Chronic kidney disease. Lancet 2021, 398, 786–802. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Gobe, G.C.; Phelps, K.R. Estimation of health risks associated with dietary cadmium exposure. Arch. Toxicol. 2023, 97, 329–358. [Google Scholar] [CrossRef] [PubMed]
- Madrigal, J.M.; Ricardo, A.C.; Persky, V.; Turyk, M. Associations between blood cadmium concentration and kidney function in the U.S. population: Impact of sex, diabetes and hypertension. Environ. Res. 2018, 169, 180–188. [Google Scholar] [CrossRef]
- Xiao, L.; Li, W.; Zhu, C.; Yang, S.; Zhou, M.; Wang, B.; Wang, X.; Wang, D.; Ma, J.; Zhou, Y.; et al. Cadmium exposure, fasting blood glucose changes, and type 2 diabetes mellitus: A longitudinal prospective study in China. Environ. Res. 2021, 192, 110259. [Google Scholar] [CrossRef]
- Schwartz, G.G.; Il’yasova, D.; Ivanova, A. Urinary cadmium, impaired fasting glucose, and diabetes in the NHANES III. Diabetes Care 2003, 26, 468–470. [Google Scholar] [CrossRef]
- Wallia, A.; Allen, N.B.; Badon, S.; El Muayed, M. Association between urinary cadmium levels and prediabetes in the NHANES 2005–2010 population. Int. J. Hyg. Environ. Health 2014, 217, 854–860. [Google Scholar] [CrossRef]
- Little, B.B.; Reilly, R.; Walsh, B.; Vu, G.T. Cadmium is associated with type 2 diabetes in a Superfund Site Lead Smelter Community in Dallas, Texas. Int. J. Environ. Res. Public Health 2020, 17, 4558. [Google Scholar] [CrossRef]
- Guo, F.F.; Hu, Z.Y.; Li, B.Y.; Qin, L.Q.; Fu, C.; Yu, H.; Zhang, Z.L. Evaluation of the association between urinary cadmium levels below threshold limits and the risk of diabetes mellitus: A dose-response meta-analysis. Environ. Sci. Pollut. Res. Int. 2019, 26, 19272–19281. [Google Scholar] [CrossRef]
- Filippini, T.; Wise, L.A.; Vinceti, M. Cadmium exposure and risk of diabetes and prediabetes: A systematic review and dose-response meta-analysis. Environ. Int. 2022, 158, 106920. [Google Scholar] [CrossRef]
- Satarug, S.; Nishijo, M.; Ujjin, P.; Vanavanitkun, Y.; Moore, M.R. Cadmium-induced nephropathy in the development of high blood pressure. Toxicol. Lett. 2005, 157, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, N.; Fry, R.C.; Balakrishnan, P.; Navas-Acien, A.; Oliver-Williams, C.; Howard, A.G.; Cole, S.A.; Haack, K.; Lange, E.M.; Howard, B.V.; et al. Cadmium body burden and increased blood pressure in middle-aged American Indians: The Strong Heart Study. J. Hum. Hypertens. 2017, 31, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.A.; Park, E.; Kim, S.; Kim, B. Influence of serum ferritin combined with blood cadmium concentrations on blood pressure and hypertension: From the Korean National Health and Nutrition Examination Survey. Chemosphere 2022, 288, 132469. [Google Scholar] [CrossRef] [PubMed]
- Garner, R.E.; Levallois, P. Associations between cadmium levels in blood and urine, blood pressure and hypertension among Canadian adults. Environ. Res. 2017, 155, 64–72. [Google Scholar] [CrossRef]
- Kaneda, M.; Wai, K.M.; Kanda, A.; Ando, M.; Murashita, K.; Nakaji, S.; Ihara, K. Low Level of Serum Cadmium in Relation to Blood Pressures Among Japanese General Population. Biol. Trace Element Res. 2021, 200, 67–75. [Google Scholar] [CrossRef]
- Oliver-Williams, C.; Howard, A.G.; Navas-Acien, A.; Howard, B.V.; Tellez-Plaza, M.; Franceschini, N. Cadmium body burden, hypertension, and changes in blood pressure over time: Results from a prospective cohort study in American Indians. J. Am. Soc. Hypertens. 2018, 12, 426–437.e9. [Google Scholar] [CrossRef]
- Crowley, S.D.; Coffman, T.M. The inextricable role of the kidney in hypertension. J. Clin. Investig. 2014, 124, 2341–2347. [Google Scholar]
- Satarug, S.; Vesey, D.A.; Gobe, G.C. Kidney cadmium toxicity, diabetes and high blood pressure: The perfect storm. Tohoku J. Exp. Med. 2017, 241, 65–87. [Google Scholar] [CrossRef]
- Oosterwijk, M.M.; Hagedoorn, I.J.M.; Maatman, R.G.H.J.; Bakker, S.J.L.; Navis, G.; Laverman, G.D. Cadmium, active smoking and renal function deterioration in patients with type 2 diabetes. Nephrol. Dial. Transpl. 2023, 38, 876–883. [Google Scholar] [CrossRef]
- Satarug, S.; Vesey, D.A.; Ruangyuttikarn, W.; Nishijo, M.; Gobe, G.C.; Phelps, K.R. The source and pathophysiologic significance of excreted cadmium. Toxics 2019, 7, 55. [Google Scholar] [CrossRef]
- Wolf, C.; Strenziok, R.; Kyriakopoulos, A. Elevated metallothionein-bound cadmium concentrations in urine from bladder carcinoma patients, investigated by size exclusion chromatography-inductively coupled plasma mass spectrometry. Anal. Chim. Acta 2009, 631, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Nishijo, M.; Ruangyuttikarn, W.; Gobe, G.C.; Phelps, K.R. The effect of cadmium on GFR is clarified by normalization of excretion rates to creatinine clearance. Int. J. Mol. Sci. 2021, 22, 1762. [Google Scholar] [CrossRef]
- Phelps, K.R.; Gosmanova, E.O. A generic method for analysis of plasma concentrations. Clin. Nephrol. 2020, 94, 43–49. [Google Scholar] [CrossRef]
- Satarug, S.; Swaddiwudhipong, W.; Ruangyuttikarn, W.; Nishijo, M.; Ruiz, P. Modeling cadmium exposures in low- and high-exposure areas in Thailand. Environ. Health Perspect. 2013, 121, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Yimthiang, S.; Pouyfung, P.; Khamphaya, T.; Kuraeiad, S.; Wongrith, P.; Vesey, D.A.; Gobe, G.C.; Satarug, S. Effects of en-vironmental exposure to cadmium and lead on the risks of diabetes and kidney dysfunction. Int. J. Environ. Res. Public Health 2022, 19, 2259. [Google Scholar] [CrossRef]
- Nishijo, M.; Nogawa, K.; Suwazono, Y.; Kido, T.; Sakurai, M.; Nakagawa, H. Lifetime cadmium exposure and mortality for renal diseases in residents of the cadmium-polluted Kakehashi River Basin in Japan. Toxics 2020, 8, 81. [Google Scholar] [CrossRef] [PubMed]
- Zarcinas, B.A.; Pongsakul, P.; McLaughlin, M.J.; Cozens, G. Heavy metals in soils and crops in Southeast Asia. 2. Thailand. Environ. Geochem. Health 2004, 26, 359–371. [Google Scholar] [CrossRef]
- Suwatvitayakorn, P.; Ko, M.S.; Kim, K.W.; Chanpiwat, P. Human health risk assessment of cadmium exposure through rice consumption in cadmium-contaminated areas of the Mae Tao sub-district, Tak, Thailand. Environ. Geochem. Health 2020, 42, 2331–2344. [Google Scholar] [CrossRef]
- Swaddiwudhipong, W.; Nguntra, P.; Kaewnate, Y.; Mahasakpan, P.; Limpatanachote, P.; Aunjai, T.; Jeekeeree, W.; Punta, B.; Funkhiew, T.; Phopueng, I. Human health effects from cadmium exposure: Comparison between persons living in cad-mium-contaminated and non-contaminated areas in northwestern Thailand. Southeast Asian J. Trop. Med. Publ. Health 2015, 46, 133–142. [Google Scholar]
- Bloch, M.J.; Basile, J.N. Review of Recent Literature in Hypertension: Updated Clinical Practice Guidelines for Chronic Kidney Disease Now Include Albuminuria in the Classification System. J. Clin. Hypertens. 2013, 15, 865–867. [Google Scholar] [CrossRef]
- Hornung, R.W.; Reed, L.D. Estimation of average concentration in the presence of nondetectable values. Appl. Occup. Environ. Hyg. 1990, 5, 46–51. [Google Scholar] [CrossRef]
- Spencer, K. Analytical reviews in clinical biochemistry: The estimation of creatinine. Ann. Clin. Biochem. 1985, 23, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Bargnoux, A.S.; Barrot, A.; Fesler, P.; Kuster, N.; Badiou, S.; Dupuy, A.M.; Ribstein, J.; Cristol, J.P. Evaluation of five immunoturbidimetric assays for urinary albumin quantification and their impact on albuminuria categorization. Clin. Biochem. 2014, 47, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Kok, M.B.; Tegelaers, F.P.; van Dam, B.; van Rijn, J.L.; van Pelt, J. Carbamylation of albumin is a cause for discrepancies between albumin assays. Clin. Chim. Acta 2014, 434, 6–10. [Google Scholar] [CrossRef]
- Soveri, I.; Berg, U.B.; Björk, J.; Elinder, C.G.; Grubb, A.; Mejare, I.; Sterner, G.; Bäck, S.E.; SBU GFR Review Group. Measuring GFR: A systematic review. Am. J. Kidney Dis. 2014, 64, 411–424. [Google Scholar] [CrossRef]
- Sharma, S.; Smyth, B. From proteinuria to fibrosis: An update on pathophysiology and treatment options. Kidney Blood Press Res. 2021, 46, 411–420. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Scmid, C.H.; Zhang, Y.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- White, C.A.; Allen, C.M.; Akbari, A.; Collier, C.P.; Holland, D.C.; Day, A.G.; Knoll, G.A. Comparison of the new and traditional CKD-EPI GFR estimation equations with urinary inulin clearance: A study of equation performance. Clin. Chim. Acta 2019, 488, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Baker, J.R.; Reilly, P.E.; Moore, M.R.; Williams, D.J. Cadmium levels in the lung, liver, kidney cortex, and urine samples from Australians without occupational exposure to metals. Arch. Environ. Health 2002, 57, 69–77. [Google Scholar] [CrossRef]
- Elinder, C.G.; Lind, B.; Kjellström, T.; Linnman, L.; Friberg, L. Cadmium in kidney cortex, liver, and pancreas from Swedish autopsies. Estimation of biological half time in kidney cortex, considering calorie intake and smoking habits. Arch. Environ. Health 1976, 31, 292–302. [Google Scholar] [CrossRef]
- Barregard, L.; Sallsten, G.; Lundh, T.; Mölne, J. Low-level exposure to lead, cadmium and mercury, and histopathological findings in kidney biopsies. Environ. Res. 2022, 211, 113119. [Google Scholar] [CrossRef] [PubMed]
- Schnaper, H.W. The tubulointerstitial pathophysiology of progressive kidney disease. Adv. Chronic Kidney Dis. 2017, 24, 107–116. [Google Scholar] [CrossRef]
- Chevalier, R.L. The proximal tubule is the primary target of injury and progression of kidney disease: Role of the glomerulotubular junction. Am. J. Physiol. Ren. Physiol. 2016, 311, F145–F161. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Đorđević, A.B.; Yimthiang, S.; Vesey, D.A.; Gobe, G.C. The NOAEL equivalent of environmental cadmium exposure associated with GFR reduction and chronic kidney disease. Toxics 2022, 10, 614. [Google Scholar] [CrossRef] [PubMed]
- Gburek, J.; Konopska, B.; Gołąb, K. Renal handling of albumin-from early findings to current concepts. Int. J. Mol. Sci. 2021, 22, 5809. [Google Scholar] [CrossRef]
- Molitoris, B.A.; Sandoval, R.M.; Yadav, S.P.S.; Wagner, M.C. Albumin uptake and processing by the proximal tubule: Physiological, pathological, and therapeutic implications. Physiol. Rev. 2022, 102, 1625–1667. [Google Scholar] [CrossRef]
- Benzing, T.; Salant, D. Insights into glomerular filtration and albuminuria. N. Engl. J. Med. 2021, 384, 1437–1446. [Google Scholar] [CrossRef]
- Edwards, A.; Long, K.R.; Baty, C.J.; Shipman, K.E.; Weisz, O.A. Modelling normal and nephrotic axial uptake of albumin and other filtered proteins along the proximal tubule. J. Physiol. 2022, 600, 1933–1952. [Google Scholar] [CrossRef]
- Langelueddecke, C.; Roussa, E.; Fenton, R.A.; Wolff, N.A.; Lee, W.K.; Thévenod, F. Lipocalin-2 (24p3/neutrophil gelati-nase-associated lipocalin (NGAL) receptor is expressed in distal nephron and mediates protein endocytosis. J. Biol. Chem. 2012, 287, 159–169. [Google Scholar] [CrossRef]
- Dizi, E.; Hasler, U.; Nlandu-Khodo, S.; Fila, M.; Roth, I.; Ernandez, T.; Doucet, A.; Martin, P.Y.; Feraille, E.; de Seigneux, S. Albuminuria induces a proinflammatory and profibrotic response in cortical collecting ducts via the 24p3 receptor. Am. J. Physiol. Renal Physiol. 2013, 305, F1053–F1063. [Google Scholar] [CrossRef]
- Santoyo-Sánchez, M.P.; Pedraza-Chaverri, J.; Molina-Jijón, E.; Arreola-Mendoza, L.; Rodríguez-Muñoz, R.; Barbier, O.C. Impaired endocytosis in proximal tubule from subchronic exposure to cadmium involves angiotensin II type 1 and cubilin receptors. BMC Nephrol. 2013, 14, 211. [Google Scholar] [CrossRef] [PubMed]
- Gena, P.; Calamita, G.; Guggino, W.B. Cadmium impairs albumin reabsorption by down-regulating megalin and ClC5 channels in renal proximal tubule cells. Environ. Health Perspect. 2010, 118, 1551–1556. [Google Scholar] [CrossRef] [PubMed]
- Pappas, R.S.; Fresquez, M.R.; Watson, C.H. Cigarette smoke cadmium breakthrough from traditional filters: Implications for exposure. J. Anal. Toxicol. 2015, 39, 45–51. [Google Scholar] [CrossRef]
- Paschal, D.C.; Burt, V.; Caudill, S.P.; Gunter, E.W.; Pirkle, J.L.; Sampson, E.J.; Miller, D.T.; Jackson, R.J. Exposure of the U.S. population aged 6 years and older to cadmium: 1988–1994. Arch. Environ. Contam. Toxicol. 2000, 38, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, M.E.; Wong, L.Y.; Osterloh, J.D. Smoking status and urine cadmium above levels associated with subclinical renal effects in U.S. adults without chronic kidney disease. Int. J. Hyg. Environ. Health 2011, 214, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.T.; Su, G.; Zhang, L.; Qin, X.; Marshall, S.; González-Ortiz, A.; Clase, C.M.; Campbell, K.L.; Xu, H.; Carrero, J.J. Modifiable lifestyle factors for primary prevention of CKD: A systematic review and meta-analysis. J. Am. Soc. Nephrol. 2021, 32, 239–253. [Google Scholar] [CrossRef]
- Jin, A.; Koh, W.P.; Chow, K.Y.; Yuan, J.M.; Jafar, T.H. Smoking and risk of kidney failure in the Singapore Chinese health study. PLoS ONE 2013, 8, e62962. [Google Scholar] [CrossRef]
- Sacerdoti, D.; Escalante, B.; Abraham, N.G.; McGiff, J.C.; Levere, R.D.; Schwartzman, M.L. Treatment with tin prevents the development of hypertension in spontaneously hypertensive rats. Science 1989, 243, 388–390. [Google Scholar] [CrossRef]
- Escalante, B.; Sacerdoti, D.; Davidian, M.M.; Laniado-Schwartzman, M.; McGiff, J.C. Chronic treatment with tin normalizes blood pressure in spontaneously hypertensive rats. Hypertens 1991, 17, 776–779. [Google Scholar] [CrossRef]
- Watanabe, T.; Kataoka, Y.; Hayashi, K.; Matsuda, R.; Uneyama, C. Dietary exposure of the Japanese general population to elements: Total diet study 2013–2018. Food Saf. 2022, 10, 83–101. [Google Scholar] [CrossRef]
- Wong, C.; Roberts, S.M.; Saab, I.N. Review of regulatory reference values and background levels for heavy metals in the human diet. Regul. Toxicol. Pharmacol. 2022, 130, 105122. [Google Scholar] [CrossRef]
- Moffett, D.B.; Mumtaz, M.M.; Sullivan, D.W., Jr.; Whittaker, M.H. Chapter 13, General Considerations of Dose-Effect and Dose-Response Relationships. In Handbook on the Toxicology of Metals, 5th ed.; Volume I: General Considerations; Nord-berg, G., Costa, M., Eds.; Academic Press: Cambridge, MA, USA, 2022; pp. 299–317. [Google Scholar]
- JECFA. In Summary and Conclusions. In Proceedings of the Joint FAO/WHO Expert Committee on Food Additives and Contaminants, Seventy-Third Meeting, Geneva, Switzerland, 8–17 June 2010; JECFA/73/SC; Food and Agriculture Organization of the United Nations/World Health Organization: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/handle/10665/44521 (accessed on 12 August 2023).
- EFSA Scientific Committee. Update: Use of the benchmark dose approach in risk assessment. EFSA J. 2017, 15, 4658. [Google Scholar]
- Butler-Dawson, J.; James, K.A.; Krisher, L.; Jaramillo, D.; Dally, M.; Neumann, N.; Pilloni, D.; Cruz, A.; Asensio, C.; Johnson, R.J.; et al. Environmental metal exposures and kidney function of Guatemalan sugarcane workers. J. Expo. Sci. Environ. Epidemiol. 2022, 32, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Win-Thu, M.; Myint-Thein, O.; Win-Shwe, T.-T.; Mar, O. Environmental cadmium exposure induces kidney tubular and glomerular dysfunction in the Myanmar adults. J. Toxicol. Sci. 2021, 46, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Skröder, H.; Hawkesworth, S.; Kippler, M.; El Arifeen, S.; Wagatsuma, Y.; Moore, S.E.; Vahter, M. Kidney function and blood pressure in preschool-aged children exposed to cadmium and arsenic-potential alleviation by selenium. Environ. Res. 2015, 140, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-López, E.; Tamayo-Ortiz, M.; Ariza, A.C.; Ortiz-Panozo, E.; Deierlein, A.L.; Pantic, I.; Tolentino, M.C.; Es-trada-Gutiérrez, G.; Parra-Hernández, S.; Espejel-Núñez, A.; et al. Early-life dietary cadmium exposure and kidney function in 9-year-old children from the PROGRESS cohort. Toxics 2020, 8, 83. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | All n = 482 | Normal eGFR a | Low eGFR | ||
|---|---|---|---|---|---|
| Women n = 329 | Men n = 114 | Women n = 35 | Men n = 4 | ||
| Age (years) | 51.8 ± 9.2 | 51.2 ± 8.7 | 49.8 ± 7.5 | 63.1 ± 11.3 | 56.0 ± 6.4 |
| BMI (kg/m2) | 24.8 ± 4.0 | 25.3 ± 4.0 | 23.5 ± 3.7 *** | 24.0 ± 3.6 | 26.7 ± 5.2 |
| eGFR b, mL/min/1.73 m2 | 90 ± 19 | 93 ± 15 | 94 ± 14 | 51 ± 9 | 47 ± 11 |
| Smoking (%) | 29.7 | 17.6 | 68.4 *** | 11.4 | 75.0 ## |
| Diabetes (%) | 18.3 | 16.7 | 13.2 | 45.7 | 50.0 |
| Hypertension (%) | 48.3 | 49.8 | 40.4 | 54.3 | 100 |
| Systolic blood pressure | 129 ± 17 | 129 ± 16 | 127 ± 113 | 138 ± 18 | 147 ± 5 |
| Diastolic blood pressure | 81 ± 10 | 81 ± 10 | 81 ± 11 | 79 ± 8 | 86 ± 4 |
| Serum creatinine, mg/dL | 0.82 ± 0.22 | 0.74 ± 0.13 | 0.92 ± 0.14 *** | 1.19 ± 0.31 | 1.68 ± 0.43 ## |
| Urine creatinine, mg/dL | 113 ± 73 | 110 ± 74 | 134 ± 72 *** | 72 ± 33 | 73 ± 24 |
| Urine albumin, mg/L | 21 ± 57 | 13 ± 31 | 29 ± 77 | 60 ± 118 | 86 ± 106 |
| Blood Cd, µg/L | 2.60 ± 3.13 | 2.43 ± 2.96 | 3.13 ± 3.32 * | 2.19 ± 3.67 | 5.03 ± 5.03 |
| Urine Cd, µg/L | 4.21 ± 5.66 | 4.44 ± 6.15 | 3.84 ± 4.04 | 3.31 ± 5.71 | 2.26 ± 2.80 |
| Normalized to Ecr (Ex/Ecr) c | |||||
| ACR, mg/g creatinine | 24 ± 71 | 15 ± 41 | 27 ± 70 | 93 ± 181 | 112 ± 139 |
| Albuminuria (%) d | 15.0 | 11.4 | 17.0 | 34.4 | 100 # |
| ECd/Ecr, µg/g creatinine | 4.05 ± 4.43 | 4.27 ± 4.46 | 3.32 ± 3.71 * | 4.63 ± 6.31 | 2.62 ± 3.04 |
| Normalized to Ccr, (Ex/Ccr) e | |||||
| (Ealb/Ccr) × 100, mg/L | 24 ± 85 | 12 ± 32 | 26 ± 67 | 125 ± 252 | 174 ± 205 |
| Abnormal Ealb/Ccr (%) f | 16.9 | 12.9 | 17.0 | 46.9 | 100 # |
| (ECd/Ccr) × 100, µg/L | 3.20 ± 3.73 | 3.05 ± 3.25 | 3.05 ± 3.41 | 5.14 ± 7.44 | 5.20 ± 6.80 |
| Independent Variables/Factors | eGFR, mL/min/1.73 m2 | |||||
|---|---|---|---|---|---|---|
| All, n = 444 | Women, n = 332 | Men, n = 113 | ||||
| β | p | β | p | β | p | |
| Age, years | −0.503 | <0.001 | −0.511 | <0.001 | −0.472 | <0.001 |
| BMI, kg/m2 | −0.066 | 0.129 | −0.050 | 0.310 | −0.134 | 0.149 |
| Log[(ECd/Ccr) × 105], µg/L filtrate | −0.121 | 0.022 | −0.126 | 0.043 | −0.097 | 0.367 |
| Systolic pressure, mmHg | −0.087 | 0.134 | −0.067 | 0.320 | −0.147 | 0.230 |
| Diastolic pressure, mmHg | −0.011 | 0.836 | −0.020 | 0.745 | 0.022 | 0.856 |
| Gender | −0.006 | 0.898 | − | − | − | − |
| Smoking | 0.033 | 0.492 | 0.031 | 0.533 | 0.034 | 0.710 |
| Diabetes | −0.101 | 0.038 | −0.119 | 0.036 | −0.033 | 0.741 |
| Adjusted R2 | 0.278 | <0.001 | 0.279 | <0.001 | 0.216 | <0.001 |
| Independent Variables/Factors | eGFR, mL/min/1.73 m2 | |||||
|---|---|---|---|---|---|---|
| Low Cd Burden | Medium Burden | High Burden | ||||
| β | p | β | p | β | p | |
| Age, years | −0.455 | <0.001 | −0.505 | <0.001 | −0.410 | <0.001 |
| BMI, kg/m2 | −0.022 | 0.777 | −0.136 | 0.064 | −0.094 | 0.221 |
| Log[(ECd/Ccr) × 105], µg/L filtrate | 0.007 | 0.934 | −0.230 | 0.002 | −0.349 | <0.001 |
| Systolic pressure, mmHg | −0.038 | 0.722 | −0.284 | 0.004 | −0.050 | 0.611 |
| Diastolic pressure, mmHg | 0.087 | 0.372 | 0.113 | 0.226 | −0.170 | 0.078 |
| Gender | −0.024 | 0.798 | −0.064 | 0.434 | 0.106 | 0.194 |
| Smoking | 0.094 | 0.324 | −0.081 | 0.301 | 0.132 | 0.108 |
| Diabetes | −0.128 | 0.104 | 0.089 | 0.260 | 0.022 | 0.775 |
| Adjusted R2 | 0.248 | <0.001 | 0.321 | <0.001 | 0.255 | <0.001 |
| Independent Variables/Factors | Low eGFR | |||||
|---|---|---|---|---|---|---|
| All, n = 446 | Women, n = 332 | Men, n = 114 | ||||
| POR (95% CI) | p | POR (95% CI) | p | POR (95% CI) | p | |
| Age, years | 1.118 (1.062, 1.176) | <0.001 | 1.114 (1.057, 1.175) | <0.001 | 1.291 (0.935, 1.783) | 0.120 |
| BMI, kg/m2 | 1.002 (0.908, 1.106) | 0.967 | 1.029 (0.923, 1.147) | 0.604 | 1.351 (0.876, 2.084) | 0.174 |
| Gender | 0.482 (0.133, 1.742) | 0.265 | − | − | − | − |
| Smoking | 1.388 (0.433, 4.450) | 0.582 | 1.123 (0.300, 4.206) | 0.863 | 0.495 (0.018, 13.92) | 0.679 |
| Diabetes | 3.042 (1.126, 8.213) | 0.028 | 2.709 (0.932, 7.878) | 0.067 | 3.713 (0.110, 125.6) | 0.465 |
| Hypertension | 1.175 (0.516, 2.679) | 0.701 | 1.228 (0.505, 2.990) | 0.651 | 2.478 (1.983, 3.098) | 0.030 a |
| Cd body burden | ||||||
| Low | Referent | Referent | Referent | |||
| Medium | 8.265 (1.711, 39.92) | 0.009 | 7.204 (1.438, 36.10) | 0.016 | n/a | n/a |
| High | 3.643 (1.150, 11.54) | 0.028 | 3.218 (0.934, 11.09) | 0.064 | n/a | n/a |
| Independent Variables/Factors | Log [(Ealb/Ccr) × 104], µg/L Filtrate | |||||
|---|---|---|---|---|---|---|
| Low Cd Burden | Medium Burden | High Burden | ||||
| β | p | β | p | β | p | |
| Age, years | 0.049 | 0.609 | −0.019 | 0.846 | −0.082 | 0.381 |
| BMI, kg/m2 | −0.007 | 0.932 | 0.248 | 0.004 | −0.021 | 0.803 |
| Log[(ECd/Ccr) × 105], µg/L filtrate | 0.177 | 0.050 | 0.144 | 0.098 | 0.173 | 0.044 |
| eGFR, mL/min/1.73 m2 | −0.110 | 0.216 | −0.147 | 0.130 | −0.214 | 0.021 |
| Gender | −0.150 | 0.122 | −0.111 | 0.233 | 0.139 | 0.120 |
| Smoking | −0.183 | 0.064 | 0.024 | 0.788 | 0.129 | 0.153 |
| Diabetes | 0.263 | 0.001 | 0.093 | 0.280 | 0.115 | 0.176 |
| Hypertension | 0.278 | <0.001 | 0.121 | 0.148 | 0.104 | 0.204 |
| Adjusted R2 | 0.174 | <0.001 | 0.103 | 0.003 | 0.082 | 0.009 |
| Independent Variables/Factors | Log [(Ealb/Ccr) × 104], µg/L Filtrate | |||||
|---|---|---|---|---|---|---|
| All | Normal eGFR | Low eGFR | ||||
| β | p | β | p | β | p | |
| Age, years | −0.023 | 0.710 | −0.016 | 0.803 | 0.163 | 0.373 |
| BMI, kg/m2 | 0.053 | 0.265 | 0.033 | 0.522 | 0.363 | 0.040 |
| Log[(ECd/Ccr) × 105], µg/L filtrate | 0.104 | 0.078 | 0.041 | 0.511 | 0.637 | 0.008 |
| eGFR, mL/min/1.73 m2 | −0.188 | <0.001 | −0.072 | 0.193 | −0.099 | 0.505 |
| Gender | −0.010 | 0.851 | 0.002 | 0.974 | −0.084 | 0.590 |
| Smoking | 0.026 | 0.624 | 0.010 | 0.863 | 0.014 | 0.934 |
| Diabetes | 0.219 | <0.001 | 0.173 | 0.002 | 0.561 | 0.006 |
| Hypertension | 0.167 | <0.001 | 0.150 | 0.002 | 0.246 | 0.130 |
| Adjusted R2 | 0.115 | <0.001 | 0.047 | 0.002 | 0.522 | 0.001 |
| Independent Variables/Factors | Albuminuria, (Ealb/Ccr) ×100 ≥ 20 mg/L Filtrate | |||||
|---|---|---|---|---|---|---|
| All, n = 473 | Women, n = 357 | Men, n = 116 | ||||
| POR (95% CI) | p | POR (95% CI) | p | POR (95% CI) | p | |
| Age, years | 0.990 (0.955, 1.027) | 0.609 | 1.007 (0.965, 1.051) | 0.733 | 0.988 (0.904, 1.079) | 0.781 |
| BMI, kg/m2 | 1.028 (0.957, 1.104) | 0.448 | 1.033 (0.950, 1.123) | 0.450 | 1.011 (0.877, 1.166) | 0.881 |
| eGFR, mL/min/1.73 m2 | 1.043 (1.026, 1.061) | <0.001 | 1.045 (1.025, 1.065) | <0.001 | 1.045 (1.008, 1.084) | 0.017 |
| Gender | 0.559 (0.273, 1.146) | 0.112 | − | − | − | − |
| Smoking | 1.037 (0.494, 2.177) | 0.924 | 1.258 (0.496, 3.192) | 0.629 | 0.809 (0.254, 2.572) | 0.719 |
| Diabetes | 6.021 (2.813, 12.89) | <0.001 | 5.996 (2.446, 14.69) | <0.001 | 8.324 (1.642, 42.21) | 0.011 |
| Hypertension | 2.053 (1.167, 3.609) | 0.013 | 2.785 (1.397, 5.552) | 0.004 | 1.133 (0.371, 3.463) | 0.827 |
| Tertile of [Cd]b, µg/L | ||||||
| Low: <0.82 | Referent | Referent | Referent | |||
| Middle: 0.83–2.63 | 2.360 (1.097, 5.076) | 0.028 | 3.402 (1.324, 8.745) | 0.011 | 0.925 (0.237, 3.604) | 0.911 |
| High: ≥2.64 | 2.740 (1.174, 6.394) | 0.020 | 3.783 (1.369, 10.46) | 0.010 | 1.425 (0.263, 7.732) | 0.681 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Satarug, S.; Vesey, D.A.; Khamphaya, T.; Pouyfung, P.; Gobe, G.C.; Yimthiang, S. Estimation of the Cadmium Nephrotoxicity Threshold from Loss of Glomerular Filtration Rate and Albuminuria. Toxics 2023, 11, 755. https://doi.org/10.3390/toxics11090755
Satarug S, Vesey DA, Khamphaya T, Pouyfung P, Gobe GC, Yimthiang S. Estimation of the Cadmium Nephrotoxicity Threshold from Loss of Glomerular Filtration Rate and Albuminuria. Toxics. 2023; 11(9):755. https://doi.org/10.3390/toxics11090755
Chicago/Turabian StyleSatarug, Soisungwan, David A. Vesey, Tanaporn Khamphaya, Phisit Pouyfung, Glenda C. Gobe, and Supabhorn Yimthiang. 2023. "Estimation of the Cadmium Nephrotoxicity Threshold from Loss of Glomerular Filtration Rate and Albuminuria" Toxics 11, no. 9: 755. https://doi.org/10.3390/toxics11090755