
A Causal and Inverse Relationship between Plant-Based Diet Intake and in a Two-Sample Mendelian Randomization Study

Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Measurement of Clinical Parameters
2.3. Food and Nutrient Intake and Dietary Patterns
2.4. DNA Genotyping and Quality Control
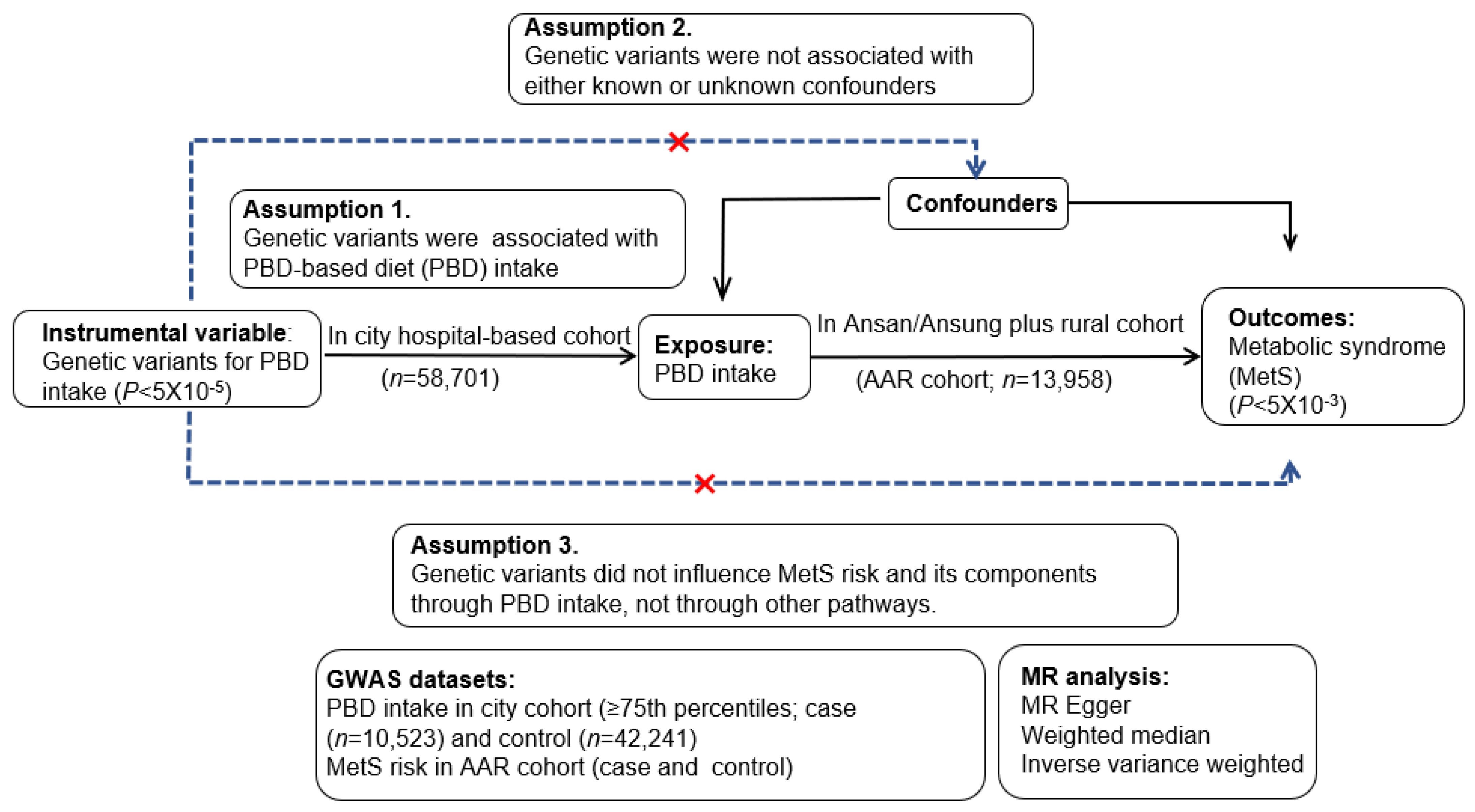
2.5. Experimental Design for a Two-Sample MR Design
2.6. Instrumental Variables in a Two-Sample MR Analysis
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Urban Hospital-Based Cohort According to PBD Intake and Gender
3.2. Metabolic Parameters Related to MetS
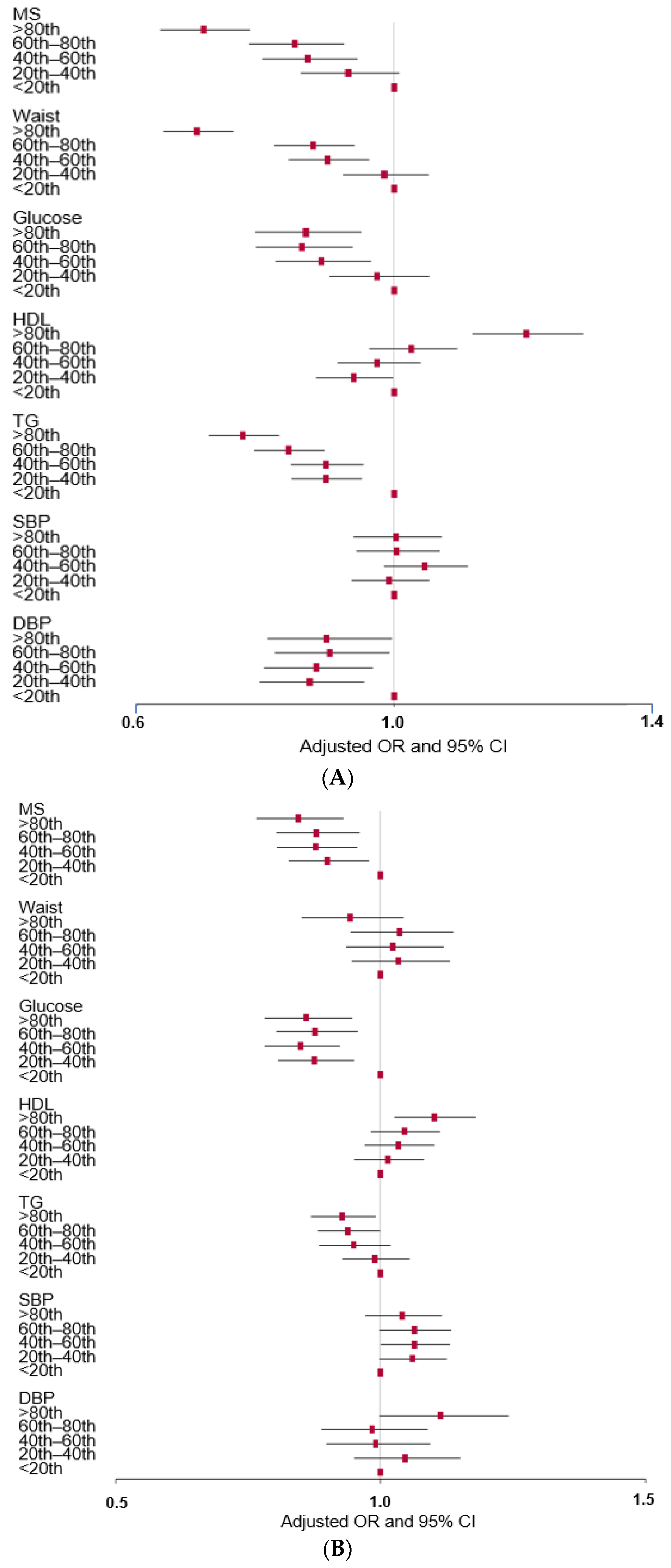
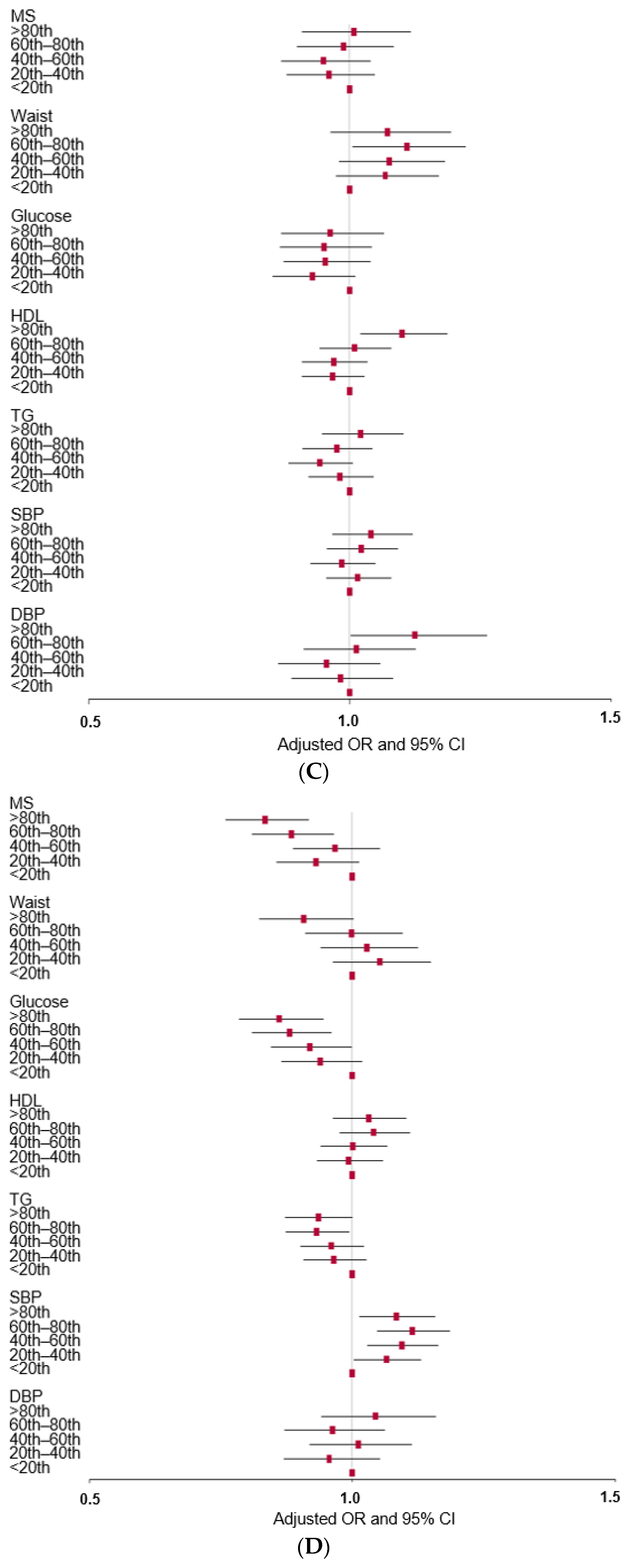
3.3. Association of PBD with MetS and its Components in Observational Studies
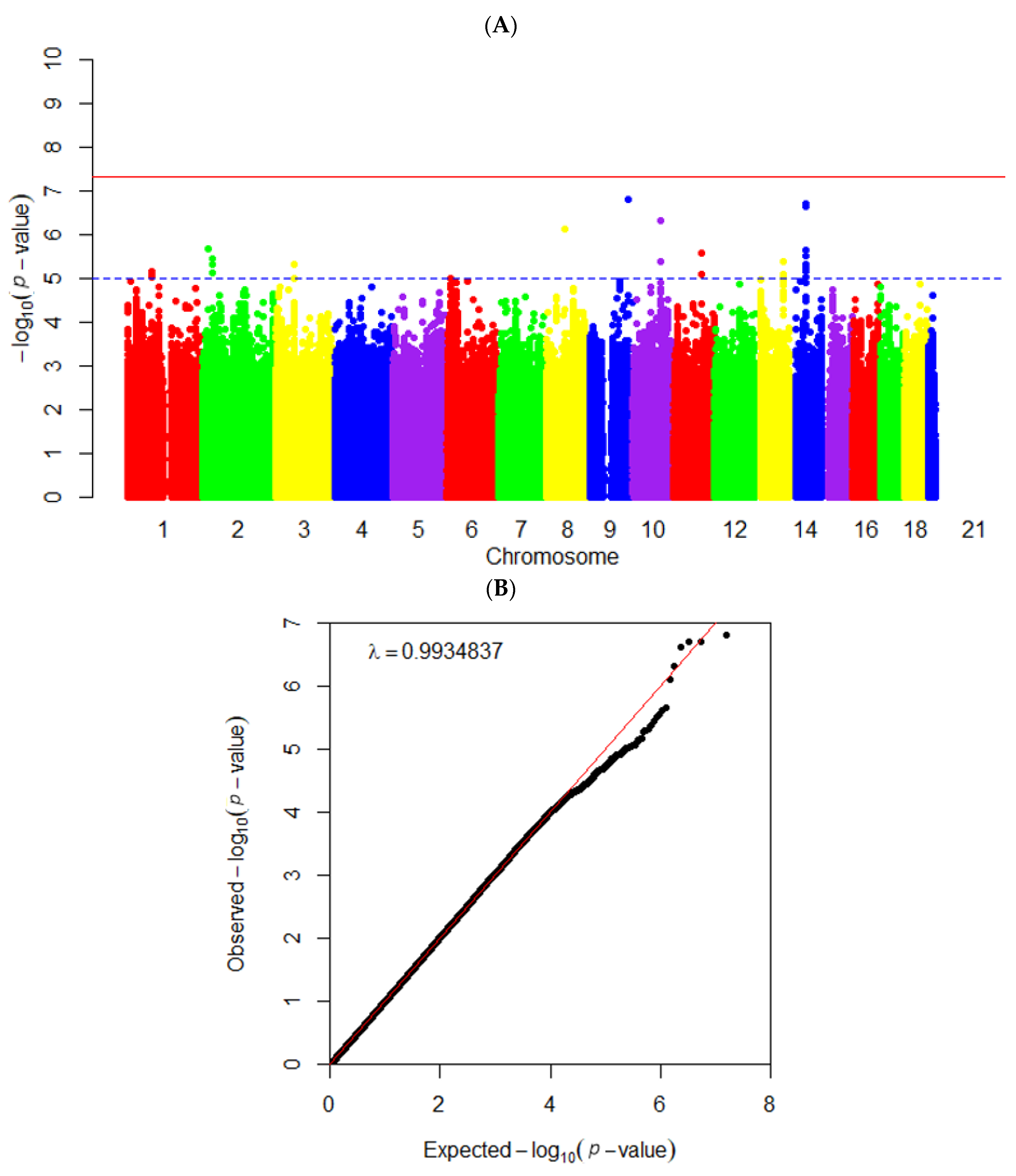
3.4. Instrumental Variables Generation for a Two-Sample MR Analysis
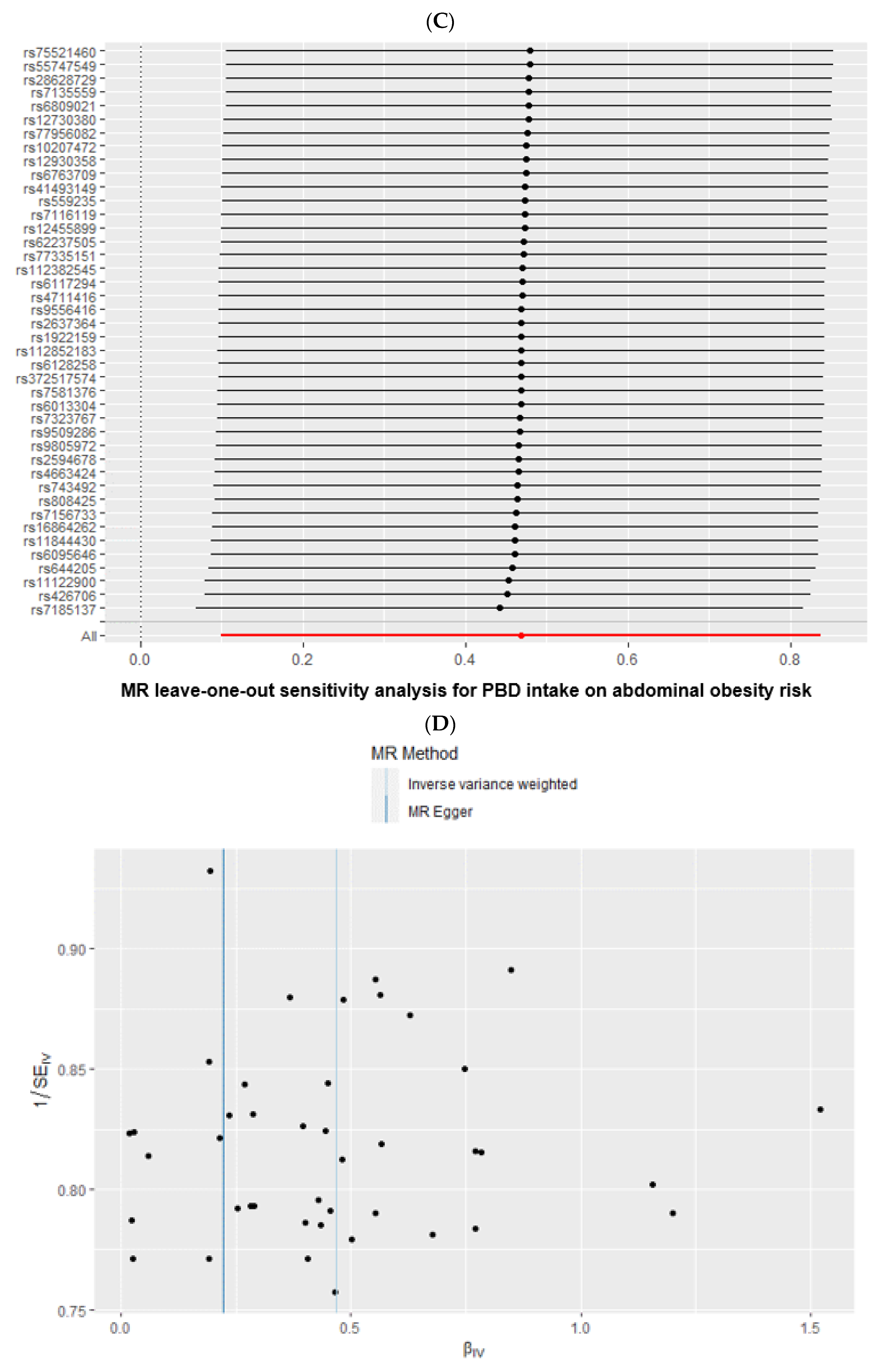
3.5. Causal Association of PBD Intake, MetS by a Two-Sample MR Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, S.; Kim, K.; Lee, B.K.; Ahn, J. A Healthy Diet Rich in Calcium and Vitamin C Is Inversely Associated with Metabolic Syndrome Risk in Korean Adults from the KNHANES 2013–2017. Nutrients 2021, 13, 1312. [Google Scholar] [CrossRef] [PubMed]
- Lear, S.A.; Gasevic, D. Ethnicity and Metabolic Syndrome: Implications for Assessment, Management and Prevention. Nutrients 2020, 12, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palaniappan, L.P.; Wong, E.C.; Shin, J.J.; Fortmann, S.P.; Lauderdale, D.S. Asian Americans have greater prevalence of metabolic syndrome despite lower body mass index. Int. J. Obes. 2011, 35, 393–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.Y.; Song, M.Y.; Park, S. Carbohydrate and sodium intake and physical activity interact with genetic risk scores of four genetic variants mainly related to lipid metabolism to modulate metabolic syndrome risk in Korean middle-aged adults. Brit. J. Nutr. 2019, 122, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kim, D.S.; Kang, S. Carrying minor allele of FADS1 and haplotype of FADS1 and FADS2 increased the risk of metabolic syndrome and moderate but not low-fat diets lowered the risk in two Korean cohorts. Eur. J. Nutr. 2019, 58, 831–842. [Google Scholar] [CrossRef]
- Park, S.; Park, C.H.; Jang, J.S. Antecedent intake of traditional Asian-style diets exacerbates pancreatic beta-cell function, growth and survival after Western-style diet feeding in weaning male rats. J. Nutr. Biochem. 2006, 17, 307–318. [Google Scholar] [CrossRef]
- Choi, S.B.; Jang, J.S.; Hong, S.M.; Jun, D.W.; Park, S. Exercise and dexamethasone oppositely modulate beta-cell function and survival via independent pathways in 90% pancreatectomized rats. J. Endocrinol. 2006, 190, 471–482. [Google Scholar] [CrossRef]
- Garralda-Del-Villar, M.; Carlos-Chillerón, S.; Diaz-Gutierrez, J.; Ruiz-Canela, M.; Gea, A.; Martínez-González, M.A.; Bes-Rastrollo, M.; Ruiz-Estigarribia, L.; Kales, S.N.; Fernández-Montero, A. Healthy Lifestyle and Incidence of Metabolic Syndrome in the SUN Cohort. Nutrients 2018, 11, 65. [Google Scholar] [CrossRef] [Green Version]
- VanWormer, J.J.; Boucher, J.L.; Sidebottom, A.C.; Sillah, A.; Knickelbine, T. Lifestyle changes and prevention of metabolic syndrome in the Heart of New Ulm Project. Prev. Med. Rep. 2017, 6, 242–245. [Google Scholar] [CrossRef]
- Park, S.; Ahn, J.; Lee, B.K. Very-low-fat diets may be associated with increased risk of metabolic syndrome in the adult population. Clin. Nutr. 2016, 35, 1159–1167. [Google Scholar] [CrossRef]
- Park, S.; Ham, J.O.; Lee, B.K. Effects of total vitamin A, vitamin C, and fruit intake on risk for metabolic syndrome in Korean women and men. Nutrition 2015, 31, 111–118. [Google Scholar] [CrossRef]
- Gouveri, E.; Marakomichelakis, G.; Diamantopoulos, E.J. Chapter 34—The Mediterranean Diet and Metabolic Syndrome. In The Mediterranean Diet, 2nd ed.; Preedy, V.R., Watson, R.R., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 371–379. [Google Scholar]
- Azadbakht, L.; Mirmiran, P.; Esmaillzadeh, A.; Azizi, T.; Azizi, F. Beneficial Effects of a Dietary Approaches to Stop Hypertension Eating Plan on Features of the Metabolic Syndrome. Diabetes Care 2005, 28, 2823–2831. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Zhang, T. A Positive Association of Overactivated Immunity with Metabolic Syndrome Risk and Mitigation of Its Association by a Plant-Based Diet and Physical Activity in a Large Cohort Study. Nutrients 2021, 13, 2308. [Google Scholar] [CrossRef]
- Wu, X.; Unno, T.; Kang, S.; Park, S. A Korean-Style Balanced Diet Has a Potential Connection with Ruminococcaceae Enterotype and Reduction of Metabolic Syndrome Incidence in Korean Adults. Nutrients 2021, 13, 495. [Google Scholar] [CrossRef]
- Liu, M.; Park, S. A Causal Relationship between Vitamin C Intake with Hyperglycemia and Metabolic Syndrome Risk: A Two-Sample Mendelian Randomization Study. Antioxidants 2022, 11, 857. [Google Scholar] [CrossRef]
- Park, S. Association between polygenetic risk scores related to sarcopenia risk and their interactions with regular exercise in a large cohort of Korean adults. Clin. Nutr. 2021, 40, 5355–5364. [Google Scholar] [CrossRef]
- Park, S.; Ahn, J.; Lee, B.-K. Self-rated subjective health status is strongly associated with sociodemographic factors, lifestyle, nutrient intakes, and biochemical indices, but not smoking status: KNHANES 2007-2012. J. Korean Med. Sci. 2015, 30, 1279–1287. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Liu, M.; Kang, S. Alcohol intake interacts with CDKAL1, HHEX, and OAS3 genetic variants, associated with the risk of type 2 diabetes by lowering insulin secretion in Korean adults. Alcohol Clin. Exp. Res. 2018, 42, 2326–2336. [Google Scholar] [CrossRef]
- Kim, Y.; Han, B.-G.; KCDC Committee. Cohort profile: The Korean genome and epidemiology study (KoGES) consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef]
- Ahn, Y.; Kwon, E.; Shim, J.; Park, M.; Joo, Y.; Kimm, K.; Park, C.; Kim, D. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef]
- Lee, S.-K.; Kim, M.K. Relationship of sodium intake with obesity among Korean children and adolescents: Korea National Health and Nutrition Examination Survey. Br. J. Nutr. 2016, 115, 834–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabbee, N.; Speed, T.P. A genotype calling algorithm for affymetrix SNP arrays. Bioinformatics 2006, 22, 7–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, K.-W.; Kim, S.H.; Zhang, X.; Park, S. Interactions among the variants of insulin-related genes and nutrients increase the risk of type 2 diabetes. Nutr. Res. 2018, 51, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Zhang, X.; Lee, N.R.; Jin, H.-S. TRPV1 gene polymorphisms are associated with type 2 diabetes by their interaction with fat consumption in the Korean genome epidemiology study. J. Nutr. Nutrigenom. 2016, 9, 47–61. [Google Scholar] [CrossRef]
- Baumeister, S.E.; Nolde, M.; Alayash, Z.; Leitzmann, M.; Baurecht, H.; Meisinger, C. Cannabis use does not impact on type 2 diabetes: A two-sample Mendelian randomization study. Addict. Biol. 2021, 26, e13020. [Google Scholar] [CrossRef]
- Wootton, R.E.; Lawn, R.B.; Millard, L.A.C.; Davies, N.M.; Taylor, A.E.; Munafò, M.R.; Timpson, N.J.; Davis, O.S.P.; Davey Smith, G.; Haworth, C.M.A. Evaluation of the causal effects between subjective wellbeing and cardiometabolic health: Mendelian randomisation study. BMJ 2018, 362, k3788. [Google Scholar] [CrossRef] [Green Version]
- de Leeuw, C.; Savage, J.; Bucur, I.G.; Heskes, T.; Posthuma, D. Understanding the assumptions underlying Mendelian randomization. Eur. J. Hum. Genet. 2022, 30, 653–660. [Google Scholar] [CrossRef]
- Burgess, S.; Thompson, S.G. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur. J. Epidemiol. 2017, 32, 377–389. [Google Scholar] [CrossRef] [Green Version]
- Burgess, S.; Small, D.S.; Thompson, S.G. A review of instrumental variable estimators for Mendelian randomization. Stat. Methods Med. Res. 2017, 26, 2333–2355. [Google Scholar] [CrossRef] [Green Version]
- Bowden, J.; Davey Smith, G.; Burgess, S. Mendelian randomization with invalid instruments: Effect estimation and bias detection through Egger regression. Int. J. Epidemiol. 2015, 44, 512–525. [Google Scholar] [CrossRef]
- Hershey, M.S.; Sotos-Prieto, M.; Ruiz-Canela, M.; Christophi, C.A.; Moffatt, S.; Martínez-González, M.Á.; Kales, S.N. The Mediterranean lifestyle (MEDLIFE) index and metabolic syndrome in a non-Mediterranean working population. Clin. Nutr. 2021, 40, 2494–2503. [Google Scholar] [CrossRef]
- Xiao, X.; Qin, Z.; Lv, X.; Dai, Y.; Ciren, Z.; Yangla, Y.; Zeng, P.; Ma, Y.; Li, X.; Wang, L.; et al. Dietary patterns and cardiometabolic risks in diverse less-developed ethnic minority regions: Results from the China Multi-Ethnic Cohort (CMEC) Study. Lancet Reg. Health West. Pac. 2021, 15, 100252. [Google Scholar] [CrossRef]
- Gomez-Marin, B.; Gomez-Delgado, F.; Lopez-Moreno, J.; Alcala-Diaz, J.F.; Jimenez-Lucena, R.; Torres-Peña, J.D.; Garcia-Rios, A.; Ortiz-Morales, A.M.; Yubero-Serrano, E.M.; Del Mar Malagon, M.; et al. Long-term consumption of a Mediterranean diet improves postprandial lipemia in patients with type 2 diabetes: The Cordioprev randomized trial. Am. J. Clin. Nutr. 2018, 108, 963–970. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Guasch-Ferré, M.; Chung, W.; Ruiz-Canela, M.; Toledo, E.; Corella, D.; Bhupathiraju, S.N.; Tobias, D.K.; Tabung, F.K.; Hu, J.; et al. The Mediterranean diet, plasma metabolome, and cardiovascular disease risk. Eur. Heart J. 2020, 41, 2645–2656. [Google Scholar] [CrossRef]
- Kim, H.; Lee, K.; Rebholz, C.M.; Kim, J. Plant-based diets and incident metabolic syndrome: Results from a South Korean prospective cohort study. PLoS Med. 2020, 17, e1003371. [Google Scholar] [CrossRef]
- Amini, M.R.; Shahinfar, H.; Djafari, F.; Sheikhhossein, F.; Naghshi, S.; Djafarian, K.; Clark, C.C.; Shab-Bidar, S. The association between plant-based diet indices and metabolic syndrome in Iranian older adults. Nutr. Health 2021, 27, 435–444. [Google Scholar] [CrossRef]
- Dong, F.; Howard, A.G.; Herring, A.H.; Popkin, B.M.; Gordon-Larsen, P. White Rice Intake Varies in Its Association with Metabolic Markers of Diabetes and Dyslipidemia Across Region among Chinese Adults. Ann. Nutr. Metab. 2015, 66, 209–218. [Google Scholar] [CrossRef] [Green Version]
- Song, S.; Young Paik, H.; Song, W.O.; Song, Y. Metabolic syndrome risk factors are associated with white rice intake in Korean adolescent girls and boys. Brit. J. Nutr. 2015, 113, 479–487. [Google Scholar] [CrossRef] [Green Version]
- Marrone, G.; Guerriero, C.; Palazzetti, D.; Lido, P.; Marolla, A.; Di Daniele, F.; Noce, A. Vegan Diet Health Benefits in Metabolic Syndrome. Nutrients 2021, 13, 817. [Google Scholar] [CrossRef]
- Freuer, D.; Meisinger, C.; Linseisen, J. Causal relationship between dietary macronutrient composition and anthropometric measures: A bidirectional two-sample Mendelian randomization analysis. Clin. Nutr. 2021, 40, 4120–4131. [Google Scholar] [CrossRef]
- Park, S.; Ahn, J.; Kim, N.S.; Lee, B.K. High carbohydrate diets are positively associated with the risk of metabolic syndrome irrespective to fatty acid composition in women: The KNHANES 2007-2014. Int. J. Food Sci. Nutr. 2017, 68, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H. Overview of Mendelian Randomization Analysis. J. Rheum. Dis. 2020, 27, 241–246. [Google Scholar] [CrossRef]
- Kim, S.H.; Liu, M.; Jin, H.S.; Park, S. High Genetic Risk Scores of ASIC2, MACROD2, CHRM3, and C2orf83 Genetic Variants Associated with Polycystic Ovary Syndrome Impair Insulin Sensitivity and Interact with Energy Intake in Korean Women. Gynecol. Obstet. Investig. 2019, 84, 225–236. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Food Groups | Korean Balanced Diet | Plant-Based Diet | Western-Style Diet | Rice-Main Diet | ||||
|---|---|---|---|---|---|---|---|---|
| Rice | −3 | −7 | 4 | 93 | * | |||
| Whole grain | 9 | −4 | −2 | −93 | * | |||
| Bread | −7 | 35 | 53 | * | −5 | |||
| Cookie | −7 | 31 | 30 | 6 | ||||
| Noodles | 2 | 2 | 62 | * | 3 | |||
| Bean | 32 | 48 | * | 3 | 2 | |||
| Potato | 24 | 50 | * | 5 | −3 | |||
| Kimchi | 50 | * | 1 | −1 | −3 | |||
| Egg | 8 | 43 | * | 15 | 5 | |||
| Fast food | −4 | 15 | 76 | * | −4 | |||
| Green vegetables | 67 | * | 42 | * | −2 | −2 | ||
| White vegetables | 70 | * | 29 | 2 | 2 | |||
| Mushroom | 49 | * | 35 | −6 | −4 | |||
| Fatty fish | 53 | * | 23 | 11 | 0 | |||
| Whitefish | 66 | * | 17 | 12 | 0 | |||
| Crab | 49 | * | 4 | 19 | 1 | |||
| Processed meats | 18 | 15 | 6 | −1 | ||||
| Red meat | 46 | * | −7 | 41 | * | 8 | ||
| Chicken | 33 | −6 | 39 | 4 | ||||
| Soups | 16 | 4 | 65 | * | −5 | |||
| Seaweeds | 44 | * | 41 | * | −2 | −4 | ||
| Milk | 11 | 49 | * | 2 | 0 | |||
| Beverage | 20 | 32 | 6 | 2 | ||||
| Coffee | 10 | −1 | 19 | 15 | ||||
| Tea | 14 | −8 | 24 | 14 | ||||
| Fruits | 19 | 48 | * | −6 | −6 | |||
| Pickles | 50 | * | −1 | 4 | 2 | |||
| Alcohol | 18 | −28 | 16 | 6 | ||||
| Nuts | −2 | 50 | * | 6 | −5 | |||
| Variance Explained by Each dietary pattern | 3.545 | 2.487 | 2.291 | 1.799 | ||||
| Men | Women | |||
|---|---|---|---|---|
| Low PBD (n = 16,095) | High PBD (n = 4198) | Low PBD (n = 23,030) | High PBD (n = 15,378) | |
| Age (year) | 55.6 ± 0.06 b | 58.0 ± 0.12 a | 51.9 ± 0.05 d | 53.1 ± 0.06 c***+++### |
| Income (Yes, %) ≤USD 2000 USD 2000–4000 >USD 4000 | 1330 (8.70) 6595 (43.1) 7366 (48.2) | 276 (6.86) ‡‡‡ 1612 (40.1) 2134 (53.1) | 2995 (13.8) 9740 (45.0) 8905 (41.2) | 1177 (8.12) ‡‡‡ 6245 (43.1) 7065 (48.8) |
| Education (Yes, %) ≤Middle school High school ≥College | 1476 (14.4) 7807 (75.9) 1001 (9.73) | 277 (12.6) ‡‡‡ 1627 (74.2) 290 (13.2) | 4692 (26.1) 13153 (69.1) 931 (4.89) | 1776 (15.7) ‡‡‡ 8718 (76.8) 851 (7.50) |
| Smoke (Yes, %) | 4779 (29.8) | 885 (21.1) ‡‡‡ | 2336 (19.6) | 497 (6.57) ‡‡‡ |
| Alcohol intake (g/day) | 39.6 ± 0.38 a | 21.3 ± 0.75 b | 6.94 ± 0.33 c | 3.09 ± 0.38 d***+++### |
| Physical activity (Yes, %) | 9135 (57.0) | 2817 (67.3) ‡‡‡ | 10962 (47.8) | 9062 (59.1) ‡‡‡ |
| Energy (EER percent) | 86.2 ± 0.25 d | 106.0 ± 0.47 b | 90.0 ± 0.21 c | 112.6 ± 0.24 a***+++### |
| CHO (En%) | 72.0 ± 0.06 b | 69.3 ± 0.11 d | 73.1 ± 0.05 a | 70.0 ± 0.06 c***+++## |
| Protein (En%) | 13.0 ± 0.02 c | 14.0 ± 0.04 b | 13.0 ± 0.02 c | 14.2 ± 0.02 a**+++## |
| Fat (En%) | 13.6 ± 0.04 b | 16.2 ± 0.08 a | 12.5 ± 0.04 c | 15.6 ± 0.04 a***+++### |
| Saturated fat (En%) | 4.39 ± 0.02 b | 4.94 ± 0.04 a | 4.04 ± 0.02 c | 4.85 ± 0.02 a**+++### |
| Monounsaturated fat (En%) | 5.58 ± 0.02 b | 6.32 ± 0.04 a | 5.01 ± 0.02 c | 5.97 ± 0.02 b***+++## |
| Polyunsaturated fat (En%) | 3.14 ± 0.02 b | 3.61 ± 0.04 a | 2.89 ± 0.02 b | 3.40 ± 0.02 b***+++ |
| Cholesterol (mg/day) | 146 ± 0.82 c | 201 ± 1.57 a | 156 ± 0.69 b | 204 ± 0.81 a***+++## |
| Fiber (g/day) | 14.1 ± 0.07 b | 15.2 ± 0.13 a | 14.3 ± 0.06 b | 15.6 ± 0.07 a**+++ |
| Calcium (mg/day) | 356 ± 1.56 d | 516 ± 2.9 7b | 402 ± 1.32 c | 570 ± 1.54 a***+++ |
| Sodium (g/day) | 2.43 ± 0.01 a | 2.47 ± 0.02 a | 2.38 ± 0.08 b | 2.46 ± 0.10a *+++ |
| Vitamin C (mg/day) | 83.9 ± 0.47 d | 117 ± 0.89 b | 97.5 ± 0.39 c | 136 ± 0.46 a***+++### |
| Vitamin D (ug/day) | 4.61 ± 0.04 d | 7.85 ± 0.08 b | 5.67 ± 0.03 c | 8.96 ± 0.04 a***+++ |
| DII (scores) | −17.5 ± 0.12 d | −22.0 ± 0.23 b | −18.7 ± 0.10 c | −23.5 ± 0.12 a***+++ |
| Flavonoids (mg/day) | 27.1 ± 0.24 d | 44.3 ± 0.46 b | 34.5 ± 0.20 c | 54.1 ± 0.24 a***+++### |
| KBD (N, %) | 6319 (39.3) | 1782 (42.5) ‡‡‡ | 5657 (24.6) | 5811 (37.8) ‡‡‡ |
| PBD (N, %) | 16,095 (41.1) | 4198 (21.4) | 23,030 (58.9) | 15,378 (78.6) ‡‡‡ |
| WSD (N, %) | 8255 (51.3) | 2176 (51.8) | 7188 (31.2) | 5933 (38.6) ‡‡‡ |
| RMD (N, %) | 5017 (31.2) | 1448 (34.5) ‡‡‡ | 7079 (30.7) | 6027 (39.2) ‡‡‡ |
| Men | Women | Adjusted Odds Ratio and 95% CI | |||
|---|---|---|---|---|---|
| Low PBD (n = 8841) | High PBD (n = 11,452) | Low PBD (n = 10,627) | High PBD (n = 27,781) | ||
| MetS (Yes, %) 1 | 2884 (17.9) | 714 (17.0) | 3137 (13.6) | 1565 (10.2) ‡‡‡ | 0.832(0.780–0.887) |
| BMI (mg/kg2) 2 | 24.4 ± 0.02 a | 24.3 ± 0.04 a | 23.7 ± 0.02 b | 23.4 ± 0.02 c***+++### | 0.836(0.796–0.877) |
| Waist C. (cm)3 | 85.5 ± 0.07 a | 84.9 ± 0.13 b | 78.6 ± 0.06 c | 77.6 ± 0.07d ***+++# | 0.819(0.778–0.862) |
| SMI (kg/m2) 4 | 7.25 + 0.01 a | 7.24 + 0.01 a | 6.08 + 0.01 b | 6.02 + 0.01 c***+++## | 0.884(0.821–0.952) |
| Fat mass (%) 5 | 23.1 + 0.04 c | 22.9 + 0.06 d | 31.3 + 0.03 b | 30.9 + 0.03 b***+++## | 0.883(0.821–0.950) |
| Serum glucose (mg/dL) 6 | 98.6 ± 0.17 a | 97.7 ± 0.33 b | 93.7 ± 0.14 c | 93.0 ± 0.17 c**+### | 0.913(0.857–0.974) |
| HbA1c (%) 7 | 5.75 ± 0.01 a | 5.72 ± 0.02 a | 5.7 0± 0.01 b | 5.68 ± 0.01 b***+ | 0.830(0.749–0.921) |
| Insulin resistance (%) 8 | 1860 (11.6) | 452 (10.8) | 1542 (6.70) | 750 (4.88) ‡‡‡ | 0.776(0.697–0.864) |
| Serum total chol (mg/dL) 9 | 191 ± 0.31 b | 189 ± 0.58 c | 201 ± 0.26 a | 201 ± 0.31 a***+ | 1.009(0.962–1.059) |
| Serum HDL (mg/dL) 10 | 49.3 ± 0.11 c | 49.5 ± 0.21 c | 55.6 ± 0.09 b | 56.9 ± 0.11 a***+++### | 1.173(1.121–1.226) |
| Serum LDL (mg/dL) 11 | 113 ± 0.29 b | 113 ± 0.54 b | 122 ± 0.24 a | 122 ± 0.28 a*** | 1.024(0.969–1.082) |
| Serum TG (mg/dL) 12 | 146 ± 0.73 a | 133 ± 1.38 b | 117 ± 0.61 c | 112 ± 0.71 d***+++## | 0.871(0.832–0.913) |
| SBP (mmHg) 13 | 125 ± 0.12 a | 124 ± 0.23 a | 121 ± 0.10 b | 121 ± 0.11 b***+ | 0.992(0.949–1.037) |
| DBP (mmHg) 14 | 77.8 ± 0.08 a | 77.5 ± 0.15 a | 74.7 ± 0.07 b | 74.6 ± 0.09 b***+ | 0.974(0.906–1.047) |
| Serum C-reactive protein (mg/L) 15 | 0.158 ± 0.004 a | 0.164 ± 0.0074 a | 0.131 ± 0.003 b | 0.127 ± 0.0043 b*** | 1.013(0.851–1.206) |
| eGFR (ml/min) 16 | 84.8 ± 0.13 c | 83.8 ± 0.25 d | 87.1 ± 0.11 a | 86.6 ± 0.13 b***+++ | 1.081(1.018–1.148) |
| Serum AST (U/L) 17 | 25.1 ± 0.21 a | 24.7 ± 0.39 a | 23.1 ± 0.17 b | 23.0 ± 0.20 b*** | 0.933(0.842–1.033) 0.993 (0.928 1.062) |
| Serum ALT (U/L) 18 | 26.0 ± 0.20 a | 25.3 ± 0.48 a | 20.5 ± 0.17 b | 20.5 ± 0.19 b*** | |
| Exposures | Two-Sample MR | Heterogeneity 2 | Pleiotropy 2 | |||||
|---|---|---|---|---|---|---|---|---|
| Method | OR (95% CI) 1 | p–Value | Q | p–Value | Intercept | SE | p–Value | |
| MetS | MR-Egger | 1.715 (0.453–6.487) | 0.432 | 1.752 | 1 | −0.007 | 0.026 | 0.778 |
| WMD | 1.363 (0.931–1.997) | 0.112 | ||||||
| IVW | 1.422 (1.047–1.930) | 0.024 | 1.833 | 1 | ||||
| WMO | 1.328 (0.588–3.001) | 0.700 | ||||||
| Hypertension | MR-Egger | 0.992 (0.2886–3.408) | 0.990 | 1.281 | 1 | 0.010 | 0.024 | 0.668 |
| WMD | 1.234 (0.870–1.749) | 0.239 | ||||||
| IVW | 1.292 (0.973–1.716) | 0.077 | 1.468 | 1 | ||||
| WMO | 1.167 (0.569–2.392) | 0.675 | ||||||
| Exposure | Two-sample MR | Heterogeneity | Pleiotropy | |||||
| Method | β (95% CI) 1 | p-value | Q | p–Value | Intercept | SE | p–Value | |
| Waist circumference (cm) | MR-Egger | 0.222 (−1.383–1.827) | 0.788 | 2.746 | 1 | 0.010 | 0.031 | 0.758 |
| WMD | 0.444 (0.027–0.991) | 0.048 | ||||||
| IVW | 0.469 (0.100–0.837) | 0.013 | 2.842 | 1 | ||||
| WMO | 0.430 (−0.484–1.344) | 0.362 | ||||||
| Serum glucose concentration (mg/dL) | MR-Egger | 0.320 (−1.601–2.240) | 0.746 | 2.335 | 1 | 0.009 | 0.038 | 0.817 |
| WMD | 0.453 (−0.109–1.016) | 0.114 | ||||||
| IVW | 0.542 (0.099–0.985) | 0.017 | 2.389 | 1 | ||||
| WMO | 0.413 (−0.657–1.482) | 0.454 | ||||||
| Serum triglyceride concentration (mg/dL) | MR-Egger | 0.703 (−0.779–2.186) | 0.194 | 3.315 | 1 | −0.011 | 0.029 | 0.709 |
| WMD | 0.326 (−0.102–0.753) | 0.136 | ||||||
| IVW | 0.427 (0.085–0.768) | 0.014 | 3.456 | 1 | ||||
| WMO | 0.218 (−0.708–1.144) | 0.647 | ||||||
| Serum HDL concentration (mg/dL) | MR-Egger | 0.287 (−0.942–1.514) | 0.650 | 3.515 | 1 | 0.002 | 0.024 | 0.926 |
| WMD | 0.287 (−0.077–0.651) | 0.122 | ||||||
| IVW | 0.343 (0.061–0.626) | 0.017 | 3.523 | 1 | ||||
| WMO | 0.169 (−0.507–0.946) | 0.556 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S. A Causal and Inverse Relationship between Plant-Based Diet Intake and in a Two-Sample Mendelian Randomization Study. Foods 2023, 12, 545. https://doi.org/10.3390/foods12030545
Park S. A Causal and Inverse Relationship between Plant-Based Diet Intake and in a Two-Sample Mendelian Randomization Study. Foods. 2023; 12(3):545. https://doi.org/10.3390/foods12030545
Chicago/Turabian StylePark, Sunmin. 2023. "A Causal and Inverse Relationship between Plant-Based Diet Intake and in a Two-Sample Mendelian Randomization Study" Foods 12, no. 3: 545. https://doi.org/10.3390/foods12030545