The Peri-Implant Microbiome—A Possible Factor Determining the Success of Surgical Peri-Implantitis Treatment?

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Outcomes
- Absence of PD ≥ 5 mm with concomitant BoP;
- Absence of SoP;
- No progressive MBL ≥ 0.5 mm on T12 compared to the baseline radiograph taken on T0.
2.3. Clinical and Radiographic Parameters
2.4. Surgical Procedure
2.5. Microbial Sample Collection
2.6. DNA Isolation and Sequencing
2.7. Statistical Analysis
3. Results
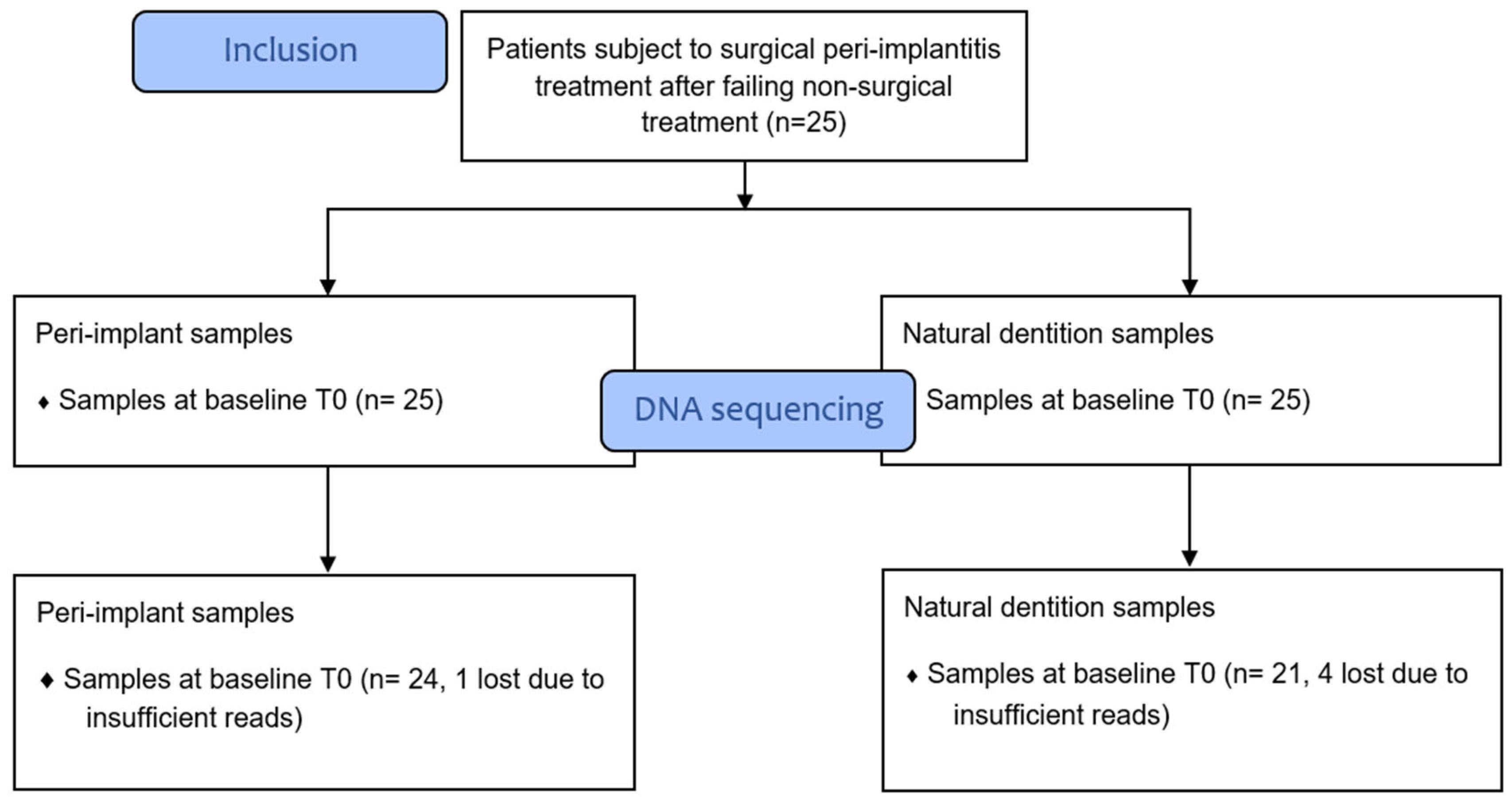
3.1. Sample Processing Results
3.2. Abundance Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sahrmann, P.; Gilli, F.; Wiedemeier, D.B.; Attin, T.; Schmidlin, P.R.; Karygianni, L. The Microbiome of Peri-Implantitis: A Systematic Review and Meta-Analysis. Microorganisms 2020, 8, 661. [Google Scholar] [CrossRef] [PubMed]
- Shiba, T.; Watanabe, T.; Kachi, H.; Koyanagi, T.; Maruyama, N.; Murase, K.; Takeuchi, Y.; Maruyama, F.; Izumi, Y.; Nakagawa, Y. Distinct interacting core taxa in co-occurrence networks enable discrimination of polymicrobial oral diseases with similar symptoms. Sci. Rep. 2016, 6, 30997. [Google Scholar] [CrossRef] [PubMed]
- Persson, G.R.; Renvert, S. Cluster of Bacteria Associated with Peri-Implantitis Pathogens in Peri-Implantitis. Clin. Implant Dent. Relat. Res. 2014, 16, 783–793. [Google Scholar] [CrossRef]
- Lafaurie, G.I.; Sabogal, M.A.; Castillo, D.M.; Rincón, M.V.; Gómez, L.A.; Lesmes, Y.A.; Chambrone, L. Microbiome and Microbial Biofilm Profiles of Peri-Implantitis: A Systematic Review. J. Periodontol. 2017, 88, 1066–1089. [Google Scholar] [CrossRef] [PubMed]
- Belibasakis, G.N.; Manoil, D. Microbial Community-Driven Etiopathogenesis of Peri-Implantitis. J. Dent. Res. 2020, 100, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Peñarrocha, M.; Monje, A.; Catena, A.; Wang, H.; Peñarrocha, D. Association between Clinical and Microbiologic Cluster Profiles and Peri-Implantitis. Int. J. Oral Maxillofac. Implant. 2017, 32, 1054–1064. [Google Scholar] [CrossRef]
- de Melo, F.; Milanesi, F.C.; Angst, P.; Oppermann, R.V. A systematic review of the microbiota composition in various peri-implant conditions: Data from 16S rRNA gene sequencing. Arch. Oral Biol. 2020, 117, 104776. [Google Scholar] [CrossRef]
- Al-Ahmad, A.; Muzafferiy, F.; Anderson, A.C.; Wölber, J.P.; Ratka-Krüger, P.; Fretwurst, T.; Nelson, K.; Vach, K.; Hellwig, E. Shift of microbial composition of peri-implantitis-associated oral biofilm as revealed by 16S rRNA gene cloning. J. Med. Microbiol. 2018, 67, 332–340. [Google Scholar] [CrossRef]
- Socransky, S.S.S. “Checkerboard” DNA-DNA hybridization. BioTechniques 1994, 17, 788–792. [Google Scholar]
- Carvalho, É.B.S.; Romandini, M.; Sadilina, S.; Sant’Ana, A.C.P.; Sanz, M. Microbiota associated with peri-implantitis—A systematic review with meta-analyses. Clin. Oral Implant. Res. 2023, 34, 1176–1187. [Google Scholar] [CrossRef]
- Shibli, J.A.; Melo, L.; Ferrari, D.S.; Figueiredo, L.C.; Faveri, M.; Feres, M. Composition of supra- and subgingival biofilm of subjects with healthy and diseased implants. Clin. Oral Implant. Res. 2008, 19, 975–982. [Google Scholar] [CrossRef]
- Albertini, M.; López-Cerero, L.; O’Sullivan, M.G.; Chereguini, C.F.; Ballesta, F.; Ríos, V.; Herrero-Climent, M.; Bullón, P. Assessment of periodontal and opportunistic flora in patients with peri-implantitis. Clin. Oral Implant. Res. 2015, 26, 937–941. [Google Scholar] [CrossRef]
- Maruyama, N.; Maruyama, F.; Takeuchi, Y.; Aikawa, C.; Izumi, Y.; Nakagawa, I. Intraindividual variation in core microbiota in peri-implantitis and periodontitis. Sci. Rep. 2015, 4, 6602. [Google Scholar] [CrossRef]
- Koyanagi, T.; Sakamoto, M.; Takeuchi, Y.; Maruyama, N.; Ohkuma, M.; Izumi, Y. Comprehensive microbiological findings in peri-implantitis and periodontitis. J. Clin. Periodontol. 2013, 40, 218–226. [Google Scholar] [CrossRef]
- Rakic, M.; Grusovin, M.G.; Canullo, L. The Microbiologic Profile Associated with Peri-Implantitis in Humans: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2016, 31, 359–368. [Google Scholar] [CrossRef]
- Kotsakis, G.A.; Olmedo, D.G. Peri-implantitis is not periodontitis: Scientific discoveries shed light on microbiome-biomaterial interactions that may determine disease phenotype. Periodontol. 2000 2021, 86, 231–240. [Google Scholar] [CrossRef]
- Herrera, D.; Berglundh, T.; Schwarz, F.; Chapple, I.; Jepsen, S.; Sculean, A.; Kebschull, M.; Papapanou, P.N.; Tonetti, M.S.; Sanz, M.; et al. Prevention and treatment of peri-implant diseases-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2023, 50, 4–76. [Google Scholar] [CrossRef]
- Máximo, M.B.; De Mendonça, A.C.; Renata Santos, V.; Figueiredo, L.C.; Feres, M.; Duarte, P.M. Short-term clinical and microbiological evaluations of peri-implant diseases before and after mechanical anti-infective therapies. Clin. Oral Implant. Res. 2009, 20, 99–108. [Google Scholar] [CrossRef]
- Isehed, C.; Holmlund, A.; Renvert, S.; Svenson, B.; Johansson, I.; Lundberg, P. Effectiveness of enamel matrix derivative on the clinical and microbiological outcomes following surgical regenerative treatment of peri-implantitis. A randomized controlled trial. J. Clin. Periodontol. 2016, 43, 863–873. [Google Scholar] [CrossRef]
- Liu, Y.; Qin, Y.; Chen, T.; Lu, M.; Qian, X.; Guo, X.; Bai, Y. A practical guide to amplicon and metagenomic analysis of microbiome data. Protein Cell 2021, 12, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Edgar, R.C.; Haas, B.J.; Clemente, J.C.; Quince, C.; Knight, R. UCHIME improves sensitivity and speed of chimera detection. Bioinformatics 2011, 27, 2194–2200. [Google Scholar] [CrossRef]
- Rognes, T.; Flouri, T.; Nichols, B.; Quince, C.; Mahé, F. VSEARCH: A versatile open source tool for metagenomics. PeerJ. 2016, 4, e2584. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.R.; Wang, Q.; Fish, J.A.; Chai, B.; McGarrell, D.M.; Sun, Y.; Brown, T.; Porras-Alfaro, A.; Kuske, C.R.; Tiedje, J.M. Ribosomal Database Project: Data and tools for high throughput rRNA analysis. Nucleic Acids Res. 2014, 42, D633–D642. [Google Scholar] [CrossRef] [PubMed]
- Caporaso, J.G.; Kuczynski, J.; Stombaugh, J.; Bittinger, K.; Bushman, F.D.; Costello, E.K.; Fierer, N.; Gonzales Peña, A.; Goodrich, J.K.; Gordon, J.I.; et al. QIIME allows analysis of high-throughput community sequencing data. Nat. Methods 2010, 7, 335–336. [Google Scholar] [CrossRef]
- Wu, J.; Peters, B.A.; Dominianni, C.; Zhang, Y.; Pei, Z.; Yang, L.; Ma, Y.; Purdue, M.P.; Jacobs, E.J.; Gapstur, S.M.; et al. Cigarette smoking and the oral microbiome in a large study of American adults. ISME J. 2016, 10, 2435–2446. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, G.; Santagati, M.; Guni, A.; Torrisi, P.; Spitale, A.; Stefani, S.; Ferlito, S.; Nibali, L. Microbiome differences in periodontal, peri-implant, and healthy sites: A cross-sectional pilot study. Clin. Oral Investig. 2021, 26, 2771–2781. [Google Scholar] [CrossRef]
- Tamura, N.; Ochi, M.; Miyakawa, H.; Nakazawa, F. Analysis of bacterial flora associated with peri-implantitis using obligate anaerobic culture technique and 16S rDNA gene sequence. Int. J. Oral Maxillofac. Implant. 2013, 28, 1521–1529. [Google Scholar] [CrossRef]
- Zheng, H.; Xu, L.; Wang, Z.; Li, L.; Zhang, J.; Zhang, Q.; Chen, T.; Lin, J.; Chen, F. Subgingival microbiome in patients with healthy and ailing dental implants. Sci. Rep. 2015, 5, 10948. [Google Scholar] [CrossRef]
- Jeng, J.; Chan, C.; Ho, Y.; Lan, W.; Hsieh, C.; Chang, M. Effects of Butyrate and Propionate on the Adhesion, Growth, Cell Cycle Kinetics, and Protein Synthesis of Cultured Human Gingival Fibroblasts. J. Periodontol. 1999, 70, 1435–1442. [Google Scholar] [CrossRef]
- Uematsu, H.; Sato, N.; Hossain, M.Z.; Ikeda, T.; Hoshino, E. Degradation of arginine and other amino acids by butyrate-producing asaccharolytic anaerobic Gram-positive rods in periodontal pockets. Arch. Oral Biol. 2003, 48, 423–429. [Google Scholar] [CrossRef]
- Tse, C.S.; Williams, D.M. Inhibition of human endothelial cell proliferation in vitro in response to n-butyrate and propionate. J. Periodont. Res. 1992, 27, 506–510. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Chaparro, P.J.; Duarte, P.M.; Shibli, J.A.; Montenegro, S.; Heluy, S.L.; Figueiredo, L.C.; Faveri, M.; Feres, M. The Current Weight of Evidence of the Microbiologic Profile Associated with Peri-Implantitis: A Systematic Review. J. Periodontol. 2016, 87, 1295–1304. [Google Scholar] [CrossRef] [PubMed]
- Ellen, R.P.; Galimanas, V.B. Spirochetes at the forefront of periodontal infections. Periodontol. 2000 2005, 38, 13–32. [Google Scholar] [CrossRef]
- Wade, W.G. The Role of Eubacterium Species in Periodontal Disease and Other Oral Infections. Microb. Ecol. Health Dis. 1996, 9, 367–370. [Google Scholar] [CrossRef]
- Haffajee, A.D.; Teles, R.P.; Socransky, S.S. Association of Eubacterium nodatum and Treponema denticola with human periodontitis lesions. Oral Microbiol. Immunol. 2006, 21, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Leonhardt, A.; Dahlén, G.; Renvert, S. Five-Year Clinical, Microbiological, and Radiological Outcome Following Treatment of Peri-Implantitis in Man. J. Periodontol. 2003, 74, 1415–1422. [Google Scholar] [CrossRef]
- Herrera, D.; van Winkelhoff, A.J.; Matesanz, P.; Lauwens, K.; Teughels, W. Europe’s contribution to the evaluation of the use of systemic antimicrobials in the treatment of periodontitis. Periodontol. 2000 2023. online ahead of print. [Google Scholar] [CrossRef]
- Okamoto-Shibayama, K.; Sekino, J.; Yoshikawa, K.; Saito, A.; Ishihara, K. Antimicrobial susceptibility profiles of oral Treponema species. Anaerobe 2017, 48, 242–248. [Google Scholar] [CrossRef]
- Wang, C.; Hao, Y.; Di Gianfilippo, R.; Sugai, J.; Li, J.; Gong, W.; Kornman, K.S.; Wang, H.L.; Kamada, N.; Xie, Y.; et al. Machine learning-assisted immune profiling stratifies peri-implantitis patients with unique microbial colonization and clinical outcomes. Theranostics 2021, 11, 6703–6716. [Google Scholar] [CrossRef]
- Lang, N.P.; Berglundh, T. Periimplant diseases: Where are we now?—Consensus of the Seventh European Workshop on Periodontology. J. Clin. Periodontol. 2011, 38, 178–181. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall Patient Outcome (n = 25) | Successfully Treated Patients (n = 12) | Non-Successfully Treated Patients (n = 13) |
|---|---|---|---|
| Gender (m/f) | 16/9 | 7/5 | 9/4 |
| Mean age (SD) | 56.3 (12.32) | 57.3 (9.3) | 55.4 (14.9) |
| Smoking (y/n) | 7/18 | 2/10 | 5/8 |
| Suppurating implants on T0 (y/n) | 12/13 | 5/7 | 7/6 |
| Suppurating implants on T12 (y/n) | 9/25 | 0/12 | 8/5 |
| Mean peri-implant PD in mm on T0, six sites (SD) | 4.8 (1.2) | 4.1 (0.7) | 5.5 (1.1) |
| Mean peri-implant PD in mm on T12, six sites (SD) | 3.6 (1.1) | 2.7 (0.5) | 4.4 (1.0) |
| Mean peri-implant BoP on T0, % (SD) | 61.3 (34.6) | 56.9 (36.6) | 65.4 (33.7) |
| Mean peri-implant BoP on T12, % (SD) | 43.9 (28.0) | 30.5 (22.3) | 56.3 (27.7) |
| Mean peri-implant REC increase in mm between T0 and T12 (SD) | 0.3 (1.1) | 0.3 (1.4) | 0.2 (0.7) |
| Mean periodontal PD in mm on T0, six sites (SD) | 2.1 (0.3) | 2.0 (0.3) | 2.2 (0.3) |
| Mean periodontal PD in mm on T12, six sites (SD) | 2.1 (0.2) | 2.1 (0.3) | 2.1 (0.2) |
| Mean periodontal BoP on T0, % (SD) | 9.1 (7.1) | 7.1 (3.5) | 11.1 (9.0) |
| Mean periodontal BoP on T12, % (SD) | 11.2 (7.9) | 11.0 (7.8) | 11.3 (8.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hakkers, J.; Liu, L.; Hentenaar, D.F.M.; Raghoebar, G.M.; Vissink, A.; Meijer, H.J.A.; Walters, L.; Harmsen, H.J.M.; de Waal, Y.C.M. The Peri-Implant Microbiome—A Possible Factor Determining the Success of Surgical Peri-Implantitis Treatment? Dent. J. 2024, 12, 20. https://doi.org/10.3390/dj12010020
Hakkers J, Liu L, Hentenaar DFM, Raghoebar GM, Vissink A, Meijer HJA, Walters L, Harmsen HJM, de Waal YCM. The Peri-Implant Microbiome—A Possible Factor Determining the Success of Surgical Peri-Implantitis Treatment? Dentistry Journal. 2024; 12(1):20. https://doi.org/10.3390/dj12010020
Chicago/Turabian StyleHakkers, Jarno, Lei Liu, Diederik F. M. Hentenaar, Gerry M. Raghoebar, Arjan Vissink, Henny J. A. Meijer, Lisa Walters, Hermie J. M. Harmsen, and Yvonne C. M. de Waal. 2024. "The Peri-Implant Microbiome—A Possible Factor Determining the Success of Surgical Peri-Implantitis Treatment?" Dentistry Journal 12, no. 1: 20. https://doi.org/10.3390/dj12010020