
Differences in Dental Implant Survival between Immediate vs. Delayed Placement: A Systematic Review and Meta-Analysis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Quality Assessment
2.4. Data Extraction
2.5. Data Analysis
3. Results
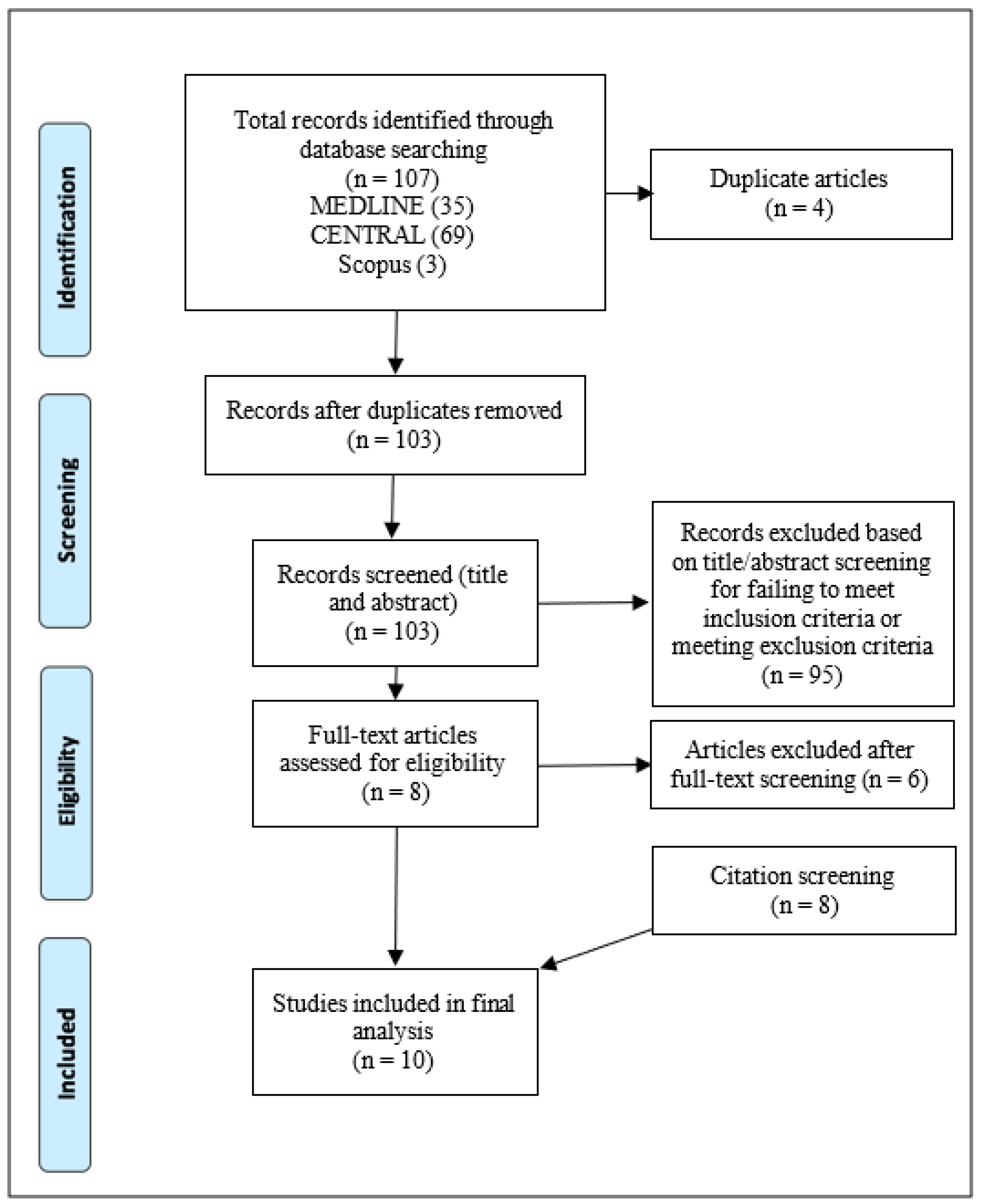
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment
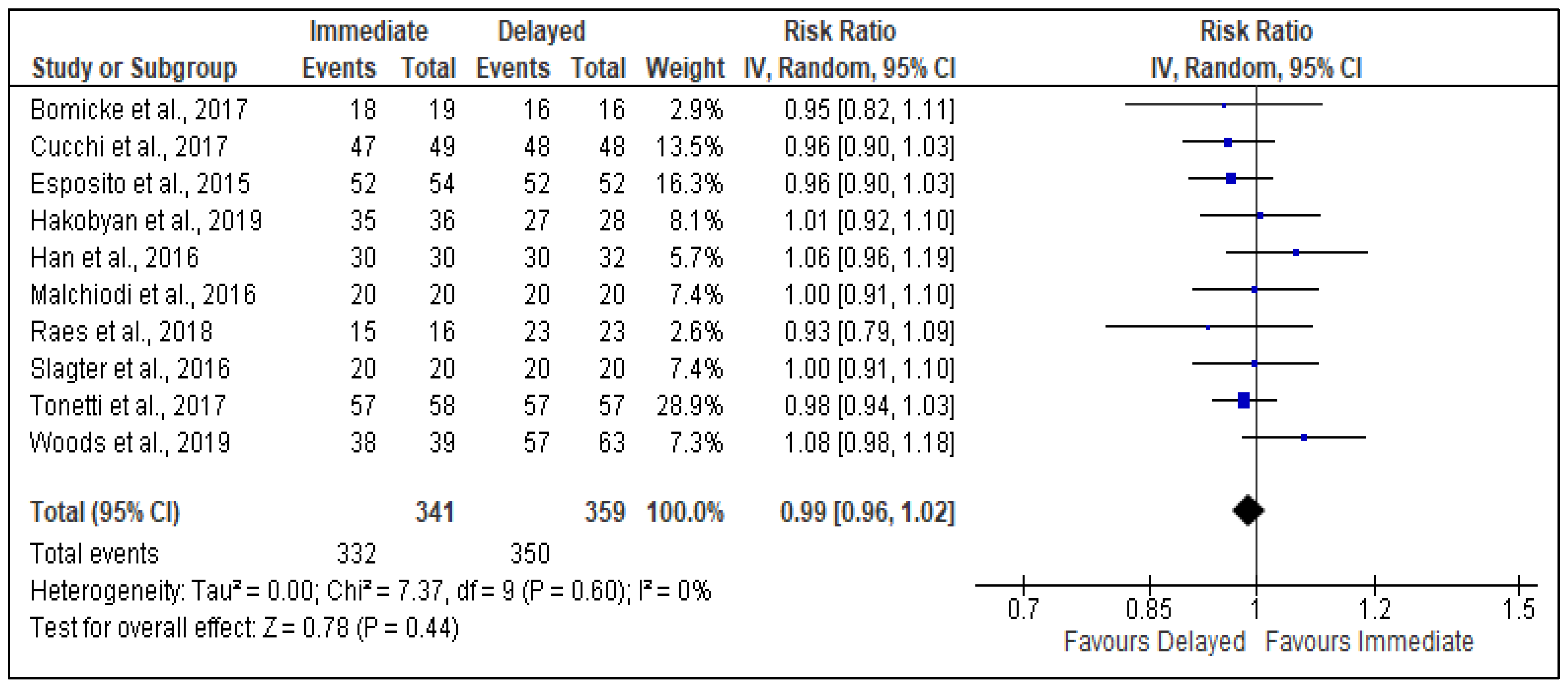
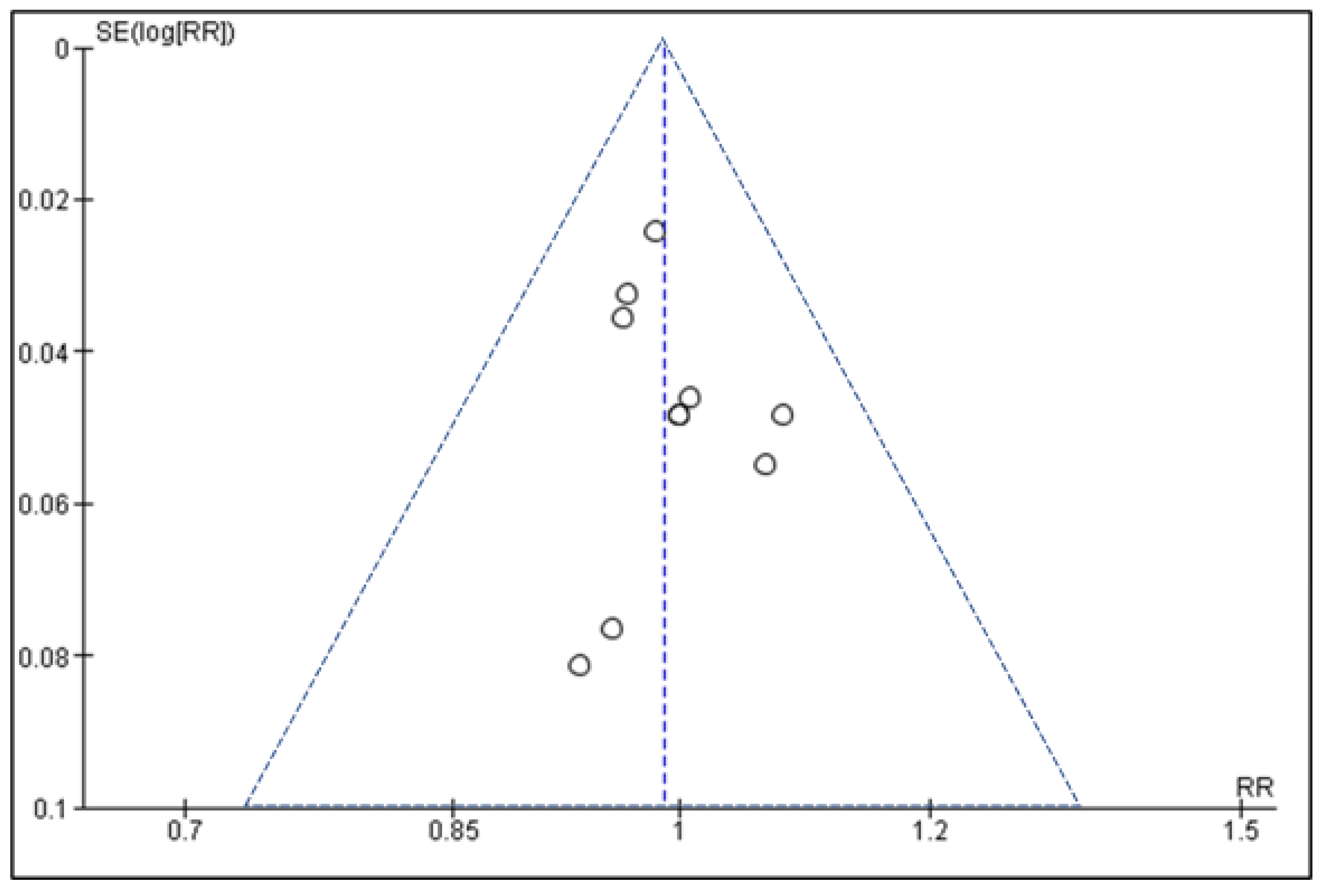
3.4. Meta-Analysis and Key Findings
Immediate versus Delayed Placement upon Implant Survival
4. Discussion
5. Conclusions
- Current evidence suggests that there is no statistically significant difference between immediate and delayed implant placement in terms of implant survival or other complications. However, delayed placement may offer a slight survival benefit in selected cases, such as patients with other existing dental and medical comorbidities
- More studies of high-quality randomized trials are needed to measure the impact of immediate versus delayed implant placement upon implant survival. Additionally, research should assess other patient-valued outcomes, including aesthetics, function, and psychological wellbeing.
- Additionally, a body of qualitative evidence is needed to explore the experiences and views of patients who have received dental implants, to identify the factors perceived to influence implant longevity and to recognise the different reasons influencing hygiene compliance. This research could help inform ongoing implant health campaigns and hygiene practices, aiming to improve oral health and potentially reduce the risk of implant failures in patients who have received immediate implant placement.
- Furthermore, a literature review is needed to assess the comparative impact of immediate versus delayed implant placement on the survival of implants within full arch prostheses. Previous research, including this review, has primarily focused on evaluating these interventions for single implants.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Elani, H.W.; Starr, J.R.; Da Silva, J.D.; Gallucci, G.O. Trends in Dental Implant Use in the U.S., 1999–2016, and Projections to 2026. J. Dent. Res. 2018, 97, 1424–1430. [Google Scholar] [CrossRef] [PubMed]
- Evian, C.I.; Emling, R.; Rosenberg, E.S.; Waasdorp, J.A.; Halpern, W.; Shah, S.; Garcia, M. Retrospective analysis of implant survival and the influence of periodontal disease and immediate placement on long-term results. Int. J. Oral Maxillofac. Implant. 2004, 19, 393–398. [Google Scholar]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Dental implants inserted in fresh extraction sockets versus healed sites: A systematic review and meta-analysis. J. Dent. 2015, 43, 16–41. [Google Scholar] [CrossRef] [PubMed]
- Romanos, G.; Froum, S.; Hery, C.; Cho, S.-C.; Tarnow, D. Survival Rate of Immediately vs Delayed Loaded Implants: Analysis of the Current Literature. J. Oral Implant. 2010, 36, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Kumar, L.; Anwar, M.; Chand, P. Immediate dental implant placement with immediate loading following extraction of natural teeth. Natl. J. Maxillofac. Surg. 2015, 6, 252–255. [Google Scholar] [CrossRef]
- Araujo, M.G.; Sukekava, F.; Wennstrom, J.L.; Lindhe, J. Ridge alterations following implant placement in fresh extraction sockets: An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 645–652. [Google Scholar] [CrossRef]
- Chen, S.T.; Darby, I.B.; Reynolds, E.C. A prospective clinical study of non-submerged immediate implants: Clinical outcomes and esthetic results. Clin. Oral Implant. Res. 2007, 18, 552–562. [Google Scholar] [CrossRef]
- Cosyn, J.; Eghbali, A.; Hermans, A.; Vervaeke, S.; De Bruyn, H.; Cleymaet, R. A 5-year prospective study on single immediate implants in the aesthetic zone. J. Clin. Periodontol. 2016, 43, 702–709. [Google Scholar] [CrossRef]
- Raes, S.; Cosyn, J.; Noyelle, A.; Raes, F.; De Bruyn, H. Clinical Outcome After 8 to 10 Years of Immediately Restored Single Implants Placed in Extraction Sockets and Healed Ridges. Int. J. Periodontics Restor. Dent. 2018, 38, 337–345. [Google Scholar] [CrossRef]
- Farrugia, P.; Petrisor, B.A.; Farrokhyar, F.; Bhandari, M. Practical tips for surgical research: Research questions, hypotheses and objectives. Can. J. Surg. 2010, 53, 278–281. [Google Scholar]
- Pollock, A.; Berge, E. How to do a systematic review. Int. J. Stroke 2018, 13, 138–156. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.; Albrektsson, T.; Wennerberg, A. Immediately loaded non-submerged versus delayed loaded submerged dental implants: A meta-analysis. Int. J. Oral Maxillofac. Surg. 2015, 44, 493–506. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Preston, L.; Carroll, C.; Gardois, P.; Paisley, S.; Kaltenthaler, E. Improving search efficiency for systematic reviews of diagnostic test accuracy: An exploratory study to assess the viability of limiting to MEDLINE, EMBASE and reference checking. Syst. Rev. 2015, 4, 82. [Google Scholar] [CrossRef] [PubMed]
- Aveyard, H. Doing a Literature Review in Health and Social Care: A Practical Guide, 4th ed.; Open University Press, University of Technology: Sydney, Australia, 2018. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Mathes, T.; Klaßen, P.; Pieper, D. Frequency of data extraction errors and methods to increase data extraction quality: A methodological review. BMC Med Res. Methodol. 2017, 17, 152. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: West Sussex, UK, 2021; Available online: https://training.cochrane.org/handbook (accessed on 11 October 2021).
- Haidich, A.B. Meta-analysis in medical research. Hippokratia 2010, 14 (Suppl. S1), 29–37. [Google Scholar]
- Egger, M.; Smith, G.D.; Altman, D.G. Systematic Reviews in Health Care: Meta-Analysis in Context, 1st ed.; BMJ Books: London, UK, 2001. [Google Scholar]
- Lee, C.H.; Cook, S.; Lee, J.S.; Han, B. Comparison of Two Meta-Analysis Methods: Inverse-Variance-Weighted Average and Weighted Sum of Z-Scores. Genom. Inform. 2016, 14, 173–180. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef]
- Bömicke, W.; Gabbert, O.; Koob, A.; Krisam, J.; Rammelsberg, P. Comparison of immediately loaded flapless-placed one-piece implants and flapped-placed conventionally loaded two-piece implants, both fitted with all-ceramic single crowns, in the posterior mandible: 3-year results from a randomised controlled pilot trial. Eur. J. Oral Implantol. 2017, 10, 179–195. [Google Scholar] [PubMed]
- Cucchi, A.; Vignudelli, E.; Franco, S.; Levrini, L.; Castellani, D.; Pagliani, L.; Rea, M.; Modena, C.; Sandri, G.; Longhi, C. Tapered, Double-Lead Threads Single Implants Placed in Fresh Extraction Sockets and Healed Sites of the Posterior Jaws: A Multicenter Randomized Controlled Trial with 1 to 3 Years of Follow-Up. BioMed Res. Int. 2017, 2017, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Barausse, C.; Pistilli, R.; Jacotti, M.; Grandi, G.; Tuco, L.; Felice, P. Immediate loading of post-extractive versus delayed placed single implants in the anterior maxilla: Outcome of a pragmatic multicenter randomised controlled trial 1-year after loading. Eur. J. Oral Implant. 2015, 8, 347–358. [Google Scholar]
- Gagik, H.; Lazar, E.; Davit, H.; Gagik, K.; Gegham, T. The comparative assessment of the of the effectiveness of immediate and delayed dental implantation. Int. J. Oral Craniofacial Sci. 2020, 6, 030–037. [Google Scholar] [CrossRef]
- Han, C.-H.; Mangano, F.; Mortellaro, C.; Park, K.-B. Immediate Loading of Tapered Implants Placed in Postextraction Sockets and Healed Sites. J. Craniofacial Surg. 2016, 27, 1220–1227. [Google Scholar] [CrossRef] [PubMed]
- Malchiodi, L.; Balzani, L.; Cucchi, A.; Ghensi, P.; Nocini, P. Primary and Secondary Stability of Implants in Postextraction and Healed Sites: A Randomized Controlled Clinical Trial. Int. J. Oral Maxillofac. Implant. 2016, 31, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Slagter, K.W.; Meijer, H.J.; Bakker, N.A.; Vissink, A.; Raghoebar, G.M. Immediate Single-Tooth Implant Placement in Bony Defects in the Esthetic Zone: A 1-Year Randomized Controlled Trial. J. Periodontol. 2016, 87, 619–629. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Cortellini, P.; Graziani, F.; Cairo, F.; Lang, N.P.; Abundo, R.; Conforti, G.P.; Marquardt, S.; Rasperini, G.; Silvestri, M.; et al. Immediate versus delayed implant placement after anterior single tooth extraction: The timing randomized controlled clinical trial. J. Clin. Periodontol. 2017, 44, 215–224. [Google Scholar] [CrossRef]
- Woods, B.; Schenberg, M.; Chandu, A. A Comparison of Immediate and Delayed Dental Implant Placement in Head and Neck Surgery Patients. J. Oral Maxillofac. Surg. 2019, 77, 1156–1164. [Google Scholar] [CrossRef]
- Raes, F.; Eccellente, T.; Lenzi, C.; Ortolani, M.; Luongo, G.; Mangano, C.; Mangano, F. Immediate functional loading of single implants: A multicenter study with 4 years of follow-up. J. Dent. Res. Dent. Clin. Dent. Prospect. 2018, 12, 26–37. [Google Scholar] [CrossRef]
- Smith, R.B.; Tarnow, D.P. Classification of Molar Extraction Sites for Immediate Dental Implant Placement: Technical Note. Int. J. Oral Maxillofac. Implant. 2013, 28, 911–916. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Perel, M.L.; Wang, H.-L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant Success, Survival, and Failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant. Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, J.; Zuabi, O.; Peled, M.; Machtei, E.E. Immediate and delayed restoration of dental implants in periodontally susceptible patients: 1-year results. Int. J. Oral Maxillofac. Implant. 2007, 22, 423–429. [Google Scholar]
- Kim, S.Y.; Dodson, T.B.; Do, D.T.; Wadhwa, G.; Chuang, S.-K. Factors Associated with Crestal Bone Loss Following Dental Implant Placement in a Longitudinal Follow-up Study. J. Oral Implant. 2015, 41, 579–585. [Google Scholar] [CrossRef]
- Parihar, A.S.; Uppala, S.; Modipalle, V.; Manual, L.; Oommen, V.M.; Karadiguddi, P.; Gupta, P. Crestal bone loss around dental implants after implantation of Tricalcium phosphate and Platelet- Rich Plasma: A comparative study. J. Fam. Med. Prim. Care 2020, 9, 229–234. [Google Scholar] [CrossRef]
- Valles, C.; Rodríguez-Ciurana, X.; Clementini, M.; Baglivo, M.; Paniagua, B.; Nart, J. Influence of subcrestal implant placement compared with equicrestal position on the peri-implant hard and soft tissues around platform-switched implants: A systematic review and meta-analysis. Clin. Oral Investig. 2018, 22, 555–570. [Google Scholar] [CrossRef]
- Jindal, N.; Kumar, M. Ramandeep Current Concepts and Trends in Biomechanics and Biomaterials of Oral and Maxillofacial Implants. Dent. J. Adv. Stud. 2017, 05, 014–024. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PICO | |
|---|---|
| Population | Adults aged ≥18 years |
| Intervention | Immediate dental implant placement in fresh sockets at the time of extraction of the tooth/teeth |
| Comparator | Delayed dental implant placement in healed sites at least two months after extraction |
| Outcomes | Survival rate of the implant, in terms of the implant still being present in the mouth at the time of examination |
| PICO | Population | Intervention | Comparator | Outcomes |
|---|---|---|---|---|
| Search Terms (truncation) | 1-Adult 2-Dental implant | 3-Immediate placement | 4-Delayed placement | 5-Survival 6-Failure |
| Study Characteristics/PICO | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Research Design | Randomised controlled trials and non-randomised comparative observational studies | Case-control studies Case studies and series editorials |
| Publication Date | 2014–2022 | Before 2014 |
| Language | English | Other languages |
| Peer-review | Yes | No |
| Population | Adults aged ≥18 years | Children aged less than 18 years |
| Intervention | Immediate placement of implants defined as implant placement at the same time as dental extraction | N/A |
| Comparator | Delayed placement of implants defined as implant placement following soft-tissue and bone healing of dental extraction sockets | N/A |
| Outcomes | Implant survival and other outcomes, such as complications and bone loss. | Outcomes of little relevance to the review question. |
| Study | Design | Setting | Participants and Type of Rehabilitation | Participants Age | Follow-Up Period | Gap between Extraction and Placement (Delayed Group) | Implant Survival Rate (Immediate vs. Delayed) |
|---|---|---|---|---|---|---|---|
| Bömicke et al. (2017) [24] | Randomised controlled trial | Germany | Adults requiring implants in posterior mandible (n = 38) one-piece implants OPI (19 participants, OPI group) or two-piece implants TPI (19 participants, TPI group) | 21–76 years | 3 years | Not reported | 94.7% vs. 100% |
| Cucchi et al. (2017) [25] | Randomised controlled trial | Italy | Adults needing single extraction and implants in posterior maxillary and mandibular regions (n = 92) tapered double-lead threads single implants | 20–79 years | 1–3 years | 3 months | 95.9% vs. 100% |
| Esposito et al. (2015) [26] | Randomised controlled trial | Italy | Adults requiring implants in maxillary second premolar to second premolar region following single-tooth extraction (n = 106) single implant at least 7 mm long with a 4 mm diameter | 28–72 years | 1 year | 4 months | 96.3% vs. 100% |
| Hakobyan et al. (2020) [27] | Non-randomised comparative study | Armenia | Adults with implants in various upper and lower and anterior and posterior sites (n = 52) single implants | 26–43 years | 5 years | 3–5 months | 97.8% vs. 98.1% |
| Han et al. (2016) [28] | Prospective cohort study | South Korea | Patients with implants mostly in the posterior region (85.5%) and predominantly in the mandible (82.3%)(n = 39, Tapered implants featuring a nanostructured calcium-incorporated surface were placed and loaded immediately. The prosthetic restorations comprised single crowns, fixed partial dentures and fixed full arches | 18–75 years | 1 year | At least 4 months | 100% vs. 96.9% |
| Malchiodi et al. (2016) [29] | Randomised controlled trial | Italy | Adults with implants in maxillary and mandibular premolar and molar sites (n = 40) | 35–75 years | 1 year | 12 weeks | 100% vs. 100% |
| S. Raes et al. (2018) [9] | Prospective cohort study | Belgium | Patients with implants in anterior maxillary region (n = 39), single implants | 22–68 years | 8–10 years | 3 months | 93.8% vs. 100% |
| Slagter et al. (2016) [30] | Randomised controlled trial | Netherlands | Patients with implants in the aesthetic zone (n = 40), single implants | 18–72 years | 1 year | 3 months | 100% vs. 100% |
| Tonetti et al. (2017) [31] | Randomised controlled trial | Italy | Adults with single-tooth extraction and implants in anterior and premolar regions (n = 124), single implants | 50–55 years (mean group ages) | 1 year | 12 weeks | 98.3% vs. 100% |
| Woods et al. (2019) [32] | Retrospective cohort study | Australia | Adults with implants in mandibular and maxillary regions placed due to heck and neck surgery (n = 20) single implants | 18–91 years | 2–140 months | Not reported | 97.4% vs. 90.5% |
| Study | Patient Selection | Definition for Implant Survival | Periodontal Probing Pocket Depths (Mean) | Marginal Bone Loss (Mean) | Crestal Bone Loss (Mean) | ISQ | Other Complications | Observations |
|---|---|---|---|---|---|---|---|---|
| Bömicke et al. (2017) [24] | Patient selected from hospital department needing a single-tooth implant in the posterior mandible, non-smokers, with minimum 6 mm bone width and 12 mm bone height. Patients randomly assigned immediate or delayed treatment. | Implants which were not mobile or requiring removal. | At 3 years: - Immediate: 2.75 mm - Delayed: 2.98 mm | At 3 years: - Immediate: 1.34 mm - Delayed: 0.67 mm | N/A | N/A | Prosthesis failure was 15.8% in immediate group and 31.3% in the delayed group. | All patients received oral antibiotics 1 h pre-op and 7 days post-op. |
| Cucchi et al. (2017) [25] | Over two years, patients selected required tooth extraction, had sufficient bone to accommodate a 3.7 × 10 mm implant without grafting and had natural dentition occluding on opposing jaw. Patients required to understand treatment and commit to follow-up. | Implants functional and under load at the 1- or 3-year mark. | At baseline: - Immediate: 3.2 ± 1.3 mm - Delayed: 2.9 ± 1.4 mm No variations seen at follow-up | N/A | At placement: - Immediate: 0.8 ± 0.4 mm - Delayed: 1.2 ± 0.6 mm At follow-up: - Immediate: 1.2 ± 0.6 mm - Delayed: 0.9 + 0.4 mm | At placement: - Immediate: 63.9 ± 12.6 - Delayed: 72.8 ± 9.7 | No prosthetic complications. | Both implants that failed were 4.8 mm × 10 mm and placed immediately in maxillary molar regions. |
| Esposito et al. (2015) [26] | Patients require at least one implant in maxillary region between second premolars and had enough bone to accept 4 × 7 mm implant. Smokers were included. | Implants still present and not showing any mobility or fracture. | N/A | At 1-year follow-up: - Immediate: 0.23 mm - Delayed: 0.29 mm | N/A | N/A | Eight minor complications observed in immediate placement group and one observed in delayed group. | Both immediate and delayed groups had the same number of smokers. Two implant failures occurred in immediate group; in both cases, no grafting was carried out. |
| Hakobyan et al. (2020) [27] | Patients chosen between 2016 and 2020 and aged between 26 and 43 years who required a dental implant. | No specific details given. | N/A | N/A | After 24 months: - Immediate: 1.06 ± 0.25 mm - Delayed: 1.02 ± 0.29 mm | At placement: - Immediate: 65.2 - Delayed: 68.3 | No other complications reported. | Ankylos dental implants were placed in all patients, either 3.75 or 4.25 mm between 10 and 13 mm length |
| Han et al. (2016) [28] | Healthy patients were selected between 2012 and 2014 who require dental implant(s). Heavy smokers of over 10 cigarettes per day excluded from study. | Implants not lost. | N/A | N/A | N/A | At 1 year: - Immediate: 80.1 - Delayed: 80.5 | No other complications reported. | One implant failed, which was in a delayed site in the posterior maxilla. No further details given. |
| Malchiodi et al. (2016) [29] | Patients selected between 2012 and 2014 who require dental implant(s), with at least 9 mm bone height in the maxilla and 11 mm in the mandible. Patients randomly grouped; 20 implants per group. | Implants which were still present and did not show any mobility, peri-implant bone resorption or infection and no pain. | N/A | N/A | After 12 months: - Immediate: 0.68 ± 0.43 mm - Delayed: 0.40 ± 0.26 mm | At placement: - Immediate: 61.90 ± 9.99 - Delayed: 66.00 ±8.25 | Insertion torque higher for delayed group (46.0 nm) compared to immediate group (52.0 nm). | All patients given pre-op chlorhexidine rinse and received antibiotics 1 h pre-op and 6 h post-op. |
| S. Raes et al. (2018) [9] | Non-smoking patients, with good oral hygiene were referred for implants in anterior maxilla. Patients with diabetes mellitus excluded. | Implants present at follow-up. | At 8 years: - Immediate: 2.7 ± 0.5 mm - Delayed: 3.4 ± 1.7 mm | At 1 year: - Immediate: 1.01 ± 1.73 mm - Delayed: 0.42 ± 1.23 mmAt 8 years: - Immediate: 0.98 ± 1.71 mm - Delayed: 0.49 ± 1.89 mm | N/A | N/A | 38% of all patients experienced one or more complications. Abutment screw loosening occurred in 8% of all patients. No significant differences between groups. | As the follow-up period was up to 8 years, there was a higher attrition rate than other studies. |
| Slagter et al. (2016) [30] | Patients selected between January 2010 and January 2020 who require one implant. Patients excluded if they were smokers, had insufficient bone, periodontal disease or significant vertical bone detection present. | Implants which are functional 1 year after definitive crown placement. | At 12 months: - Immediate (mm): Mesial—3.3 ± 0.7 Distal—3.5 ± 0.8 Buccal—3.2 ± 0.8 Palatal—2.7 ± 0.6 - Delayed (mm)Mesial—3.6 + 0.8 Distal—3.8 + 0.7 Buccal—3.3 + 0.7 Palatal—3.1 + 0.5 | At 12 months: - Immediate: 0.56 ± 0.39 mm (mesial), 0.74 ± 0.51 mm (distal) - Delayed: 0.51 ± 0.43 mm (mesial),0.54 ± 0.45 mm (distal) | N/A | N/A | Aesthetic outcome for immediate implants more favourable than delayed implants. PES score for immediate: 15.8 ± 2.1, compared to delayed: 15.3 ± 2.0 | All patients given prophylactic antibiotics to take for 7 days prior to surgery. |
| Tonetti et al. (2017) [31] | Patents required dental implant treatment, were non-smokers or smoked less than 20 cigarettes per day, had no relevant medical conditions and had good periodontal status. Patients offered to be part of study on a sequential basis. | Implants present at follow-up. | At 12 months: - Immediate: 4.1 ± 1.2 mm - Delayed: 3.3 ± 1.1 mm | N/A | Immediate implants showed greater residual bone loss compared to delayed implants, by a mean difference of 0.8 mm. | N/A | Wound failure was 5 times more likely in immediate implant placements than delayed. | Patients given pre-op antibiotics before surgery and diclofenac. |
| Woods et al. (2019) [32] | Patients included those with cancers of the head and neck, thus having implants as part of rehabilitation treatment. Patients chosen were motivated and had good oral care. | Implants that did not have to be removed due to failure, mobility, or infection. | N/A | N/A | N/A | N/A | Survival rate was lowest amongst patients in the PORT group (post-operative radiotherapy patients) | 20% of Straumann SLA Active implants failed. Neoss implants had a 6.1% failure rate. |
| ROBINS-I | |||||||
|---|---|---|---|---|---|---|---|
| Non-Randomised Studies | Confounding | Subject Selection | Classification of Interventions | Protocol Deviations | Missing Data | Outcome Measurement | Reporting |
| Hakobyan et al. (2020) [27] | Unclear | Unclear | Low | Low | Low | Low | Low |
| Han et al. (2016) [28] | Moderate | Low | Low | Low | Low | Low | Low |
| S. Raes et al. (2018) [9] | Moderate | Low | Low | Low | Moderate | Low | Low |
| Woods et al. (2019) [32] | Moderate | Low | Low | Low | Low | Low | Low |
| ROB 2.0 | |||||||
| Randomised Trials | Randomisation | Protocol Deviations | Missing Data | Outcome Measurement | Reporting | - | - |
| Bömicke et al. (2017) [24] | Unclear | Low | Low | Low | Low | - | - |
| Cucchi et al. (2017) [25] | Low | Low | Low | Low | Low | - | - |
| Esposito et al. (2015) [26] | Unclear | Low | Low | Low | Low | - | - |
| Malchiodi et al. (2016) [29] | Some concern | Low | Low | Low | Low | - | - |
| Slagter et al. (2016) [30] | Unclear | Low | Low | Low | Low | - | - |
| Tonetti et al. (2017) [31] | Low | Low | Low | Low | Low | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, R.; Ucer, C.; Wright, S.; Khan, R.S. Differences in Dental Implant Survival between Immediate vs. Delayed Placement: A Systematic Review and Meta-Analysis. Dent. J. 2023, 11, 218. https://doi.org/10.3390/dj11090218
Patel R, Ucer C, Wright S, Khan RS. Differences in Dental Implant Survival between Immediate vs. Delayed Placement: A Systematic Review and Meta-Analysis. Dentistry Journal. 2023; 11(9):218. https://doi.org/10.3390/dj11090218
Chicago/Turabian StylePatel, Rishi, Cemal Ucer, Simon Wright, and Rabia S. Khan. 2023. "Differences in Dental Implant Survival between Immediate vs. Delayed Placement: A Systematic Review and Meta-Analysis" Dentistry Journal 11, no. 9: 218. https://doi.org/10.3390/dj11090218