

Clinical and Psychosocial Impact of Communication about Oral Potentially Malignant Disorders: A Scoping Review
 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Information Sources and Search
2.3. Selection of Sources of Evidence
2.4. Data Synthesis and Descriptive Analysis
3. Results
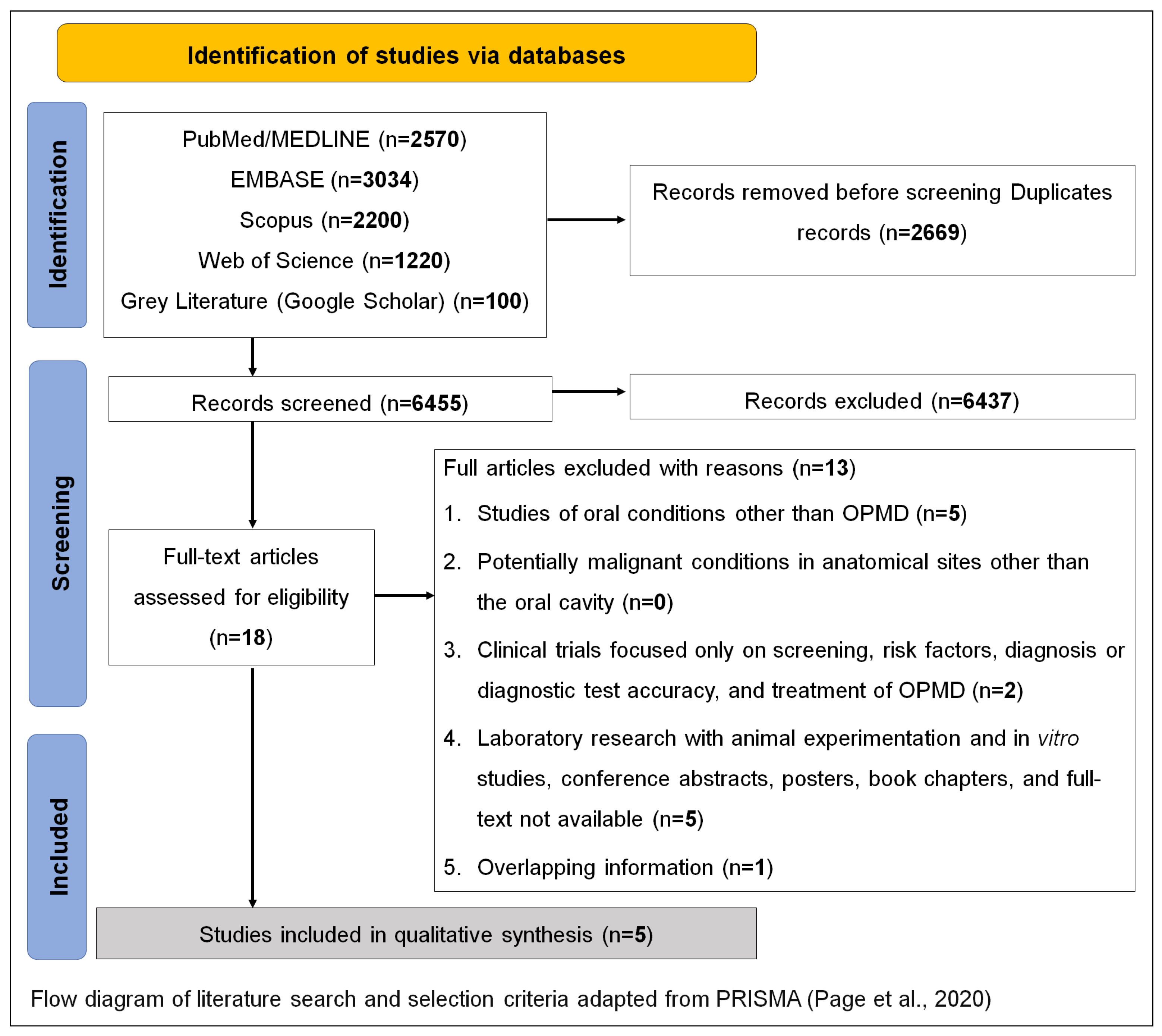
3.1. Selection and Characteristics of Sources of Evidence
3.2. Synthesis of Results
4. Discussion
4.1. Challenges for Professionals in Delivering Bad News Regarding OPMDs
4.2. Communication about Risk Factors Related to OPMDs
4.3. Communication about Rates of Malignant Transformation
4.4. Treatment-Related Communication
4.5. Communicating Clinical/Psychosocial Implications to Patients
4.6. Patients’ Preferences on OPMD Communication
4.7. General Recommendations on OPMD Communication
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Warnakulasuriya, S.; Kujan, O.; Aguirre-Urizar, J.M.; Bagan, J.V.; González-Moles, M.Á.; Kerr, A.R.; Lodi, G.; Mello, F.W.; Monteiro, L.; Ogden, G.R.; et al. Oral potentially malignant disorders: A consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral Dis. 2021, 27, 1862–1880. [Google Scholar] [CrossRef] [PubMed]
- Mello, F.W.; Miguel, A.F.P.; Dutra, K.L.; Porporatti, A.L.; Warnakulasuriya, S.; Guerra, E.N.S.; Rivero, E.R.C. Prevalence of oral potentially malignant disorders: A systematic review and meta-analysis. J. Oral Pathol. Med. 2018, 47, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Iocca, O.; Sollecito, T.P.; Alawi, F.; Weinstein, G.S.; Newman, J.G.; De Virgilio, A.; Di Maio, P.; Spriano, G.; Pardiñas López, S.; Shanti, R.M.; et al. Potentially malignant disorders of the oral cavity and oral dysplasia: A systematic review and meta-analysis of malignant transformation rate by subtype. Head Neck 2020, 42, 539–555. [Google Scholar] [CrossRef] [PubMed]
- Nikitakis, N.G.; Pentenero, M.; Georgaki, M.; Poh, C.F.; Peterson, D.E.; Edwards, P.; Lingen, M.; Sauk, J.J. Molecular markers associated with development and progression of potentially premalignant oral epithelial lesions: Current knowledge and future implications. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 650–669. [Google Scholar] [CrossRef] [PubMed]
- Ranjan, P. How can Doctors Improve their Communication Skills? J. Clin. Diagn. Res. 2015, 9, JE01. [Google Scholar] [CrossRef]
- Surbone, A. Telling the truth to patients with cancer: What is the truth? Lancet Oncol. 2006, 7, 944–950. [Google Scholar] [CrossRef]
- Alves, C.G.B.; Treister, N.S.; Ribeiro, A.C.P.; Brandão, T.B.; Tonaki, J.O.; Lopes, M.A.; Rivera, C.; Santos-Silva, A.R. Strategies for communicating oral and oropharyngeal cancer diagnosis: Why talk about it? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 347–356. [Google Scholar] [CrossRef]
- Tadakamadla, J.; Kumar, S.; Johnson, N.W. Quality of life in patients with oral potentially malignant disorders: A systematic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 119, 644–655. [Google Scholar] [CrossRef]
- Tadakamadla, J.; Kumar, S.; Lalloo, R.; Johnson, N.W. Qualitative analysis of the impact of Oral Potentially Malignant Disorders on daily life activities. PLoS ONE 2017, 12, e0175531. [Google Scholar] [CrossRef]
- Tadakamadla, J.; Kumar, S.; Lalloo, R.; Gandhi Babu, D.B.; Johnson, N.W. Impact of oral potentially malignant disorders on quality of life. J. Oral Pathol. 2018, 47, 60–65. [Google Scholar] [CrossRef]
- Gondivkar, S.M.; Gadbail, A.R.; Gondivkar, R.S.; Sarode, S.C.; Sarode, G.S.; Patil, S. Impact of oral potentially malignant disorders on quality of life: A systematic review. Future Oncol. 2018, 14, 995–1010. [Google Scholar] [CrossRef] [PubMed]
- Gondivkar, S.M.; Bhowate, R.R.; Gadbail, A.R.; Sarode, S.C.; Patil, S. Quality of life and oral potentially malignant disorders: Critical appraisal and prospects. World J. Clin. Oncol. 2018, 9, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.; Khandpur, M.; Khandpur, S.; Mehrotra, D.; Chandra Tiwari, S.; Kumar, S. Quality of life among Oral Potentially Malignant Disorder (OPMD) patients: A prospective study. J. Oral Biol. Craniofac. Res. 2021, 11, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- van der Waal, I. Knowledge about oral leukoplakia for use at different levels of expertise, including patients. Oral Dis. 2018, 24, 174–178. [Google Scholar] [CrossRef]
- van der Waal, I. Oral Leukoplakia: Present Views on Diagnosis, Management, Communication with Patients, and Research. Curr. Oral Health Rep. 2019, 6, 9–13. [Google Scholar] [CrossRef]
- Brocklehurst, P.R.; Baker, S.R.; Speight, P.M. A qualitative study examining the experience of primary care dentists in the detection and management of potentially malignant lesions. 2. Mechanics of the referral and patient communication. Br. Dent. J. 2010, 208, E4. [Google Scholar] [CrossRef]
- Lin, H.-Y.; Chen, S.-C.; Peng, H.-L.; Chen, M.-K. Unmet information needs and clinical characteristics in patients with precancerous oral lesions. Eur. J. Cancer Care (Engl.) 2015, 24, 911–919. [Google Scholar] [CrossRef]
- Raman, P. Communication, Counseling and Compassionate Care: The least explored and challenging Palliative Care approaches among Primary Care Physicians—Clinical Case series of Oral Potentially malignant disorders in Tamil Nadu. J. Family Med. Prim. Care 2021, 10, 572. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Baile, W.F.; Buckman, R.; Lenzi, R.; Glober, G.; Beale, E.A.; Kudelka, A.P. SPIKES—A Six-Step Protocol for Delivering Bad News: Application to the Patient with Cancer. Oncologist 2000, 5, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Rozier, R.G.; Horowitz, A.M.; Podschun, G. Dentist-patient communication techniques used in the United States. J. Am. Dent. Assoc. 2011, 142, 518–530. [Google Scholar] [CrossRef]
- Davis, T.C.; Williams, M.V.; Marin, E.; Parker, R.M.; Glass, J. Health Literacy and Cancer Communication. CA Cancer J. Clin. 2002, 52, 134–149. [Google Scholar] [CrossRef] [PubMed]
- Lorini, L.; Bescós Atín, C.; Thavaraj, S.; Müller-Richter, U.; Alberola Ferranti, M.; Pamias Romero, J.; Sáez Barba, M.; de Pablo García-Cuenca, A.; Braña García, I.; Bossi, P.; et al. Overview of Oral Potentially Malignant Disorders: From Risk Factors to Specific Therapies. Cancers 2021, 13, 3696. [Google Scholar] [CrossRef] [PubMed]
- Gunjal, S.; Pateel, D.G.S.; Yang, Y.-H.; Doss, J.G.; Bilal, S.; Maling, T.H.; Mehrotra, R.; Cheong, S.C.; Zain, R.B.M. An Overview on Betel Quid and Areca Nut Practice and Control in Selected Asian and South East Asian Countries. Subst. Use Misuse 2020, 55, 1533–1544. [Google Scholar] [CrossRef]
- Odell, E.; Kujan, O.; Warnakulasuriya, S.; Sloan, P. Oral epithelial dysplasia: Recognition, grading and clinical significance. Oral Dis. 2021, 27, 1947–1976. [Google Scholar] [CrossRef]
- Rana, M.; Gellrich, N.-C.; Rana, M. Comparison of health-related quality of life of patients with different precancer and oral cancer stages. Clin. Oral Investig. 2015, 19, 481–488. [Google Scholar] [CrossRef]
- Kerr, A.R.; Lodi, G. Management of oral potentially malignant disorders. Oral Dis. 2021, 27, 2008–2025. [Google Scholar] [CrossRef]
- Lingen, M.W.; Abt, E.; Agrawal, N.; Chaturvedi, A.K.; Cohen, E.; D’Souza, G.; Gurenlian, J.; Kalmar, J.R.; Kerr, A.R.; Lambert, P.M.; et al. Evidence-based clinical practice guideline for the evaluation of potentially malignant disorders in the oral cavity. J. Am. Dent. Assoc. 2017, 148, 712–727.e10. [Google Scholar] [CrossRef]
- Lingen, M.W.; Tampi, M.P.; Urquhart, O.; Abt, E.; Agrawal, N.; Chaturvedi, A.K.; Cohen, E.; D’Souza, G.; Gurenlian, J.; Kalmar, J.R.; et al. Adjuncts for the evaluation of potentially malignant disorders in the oral cavity. J. Am. Dent. Assoc. 2017, 148, 797–813.e52. [Google Scholar] [CrossRef]
- Alsoghier, A.; Ni Riordain, R.; Fedele, S.; Porter, S. Web-based information on oral dysplasia and precancer of the mouth—Quality and readability. Oral Oncol. 2018, 82, 69–74. [Google Scholar] [CrossRef]
- Panta, P.; Sarode, S.C.; Sarode, G.S.; Patil, S. Potential of web-resource on ‘oral dysplasia and precancer’! Oral Oncol. 2018, 84, 126–127. [Google Scholar] [CrossRef]
- Güneri, P.; Epstein, J.; Botto, R.W. Breaking bad medical news in a dental care setting. J. Am. Dent. Assoc. 2013, 144, 381–386. [Google Scholar] [CrossRef]
- Karnieli-Miller, O.; Pelles, S.; Meitar, D. Position paper: Teaching breaking bad news (BBN) to undergraduate medical students. Patient Educ. Couns. 2022, 105, 2899–2904. [Google Scholar] [CrossRef] [PubMed]
- Curtin, S.; McConnell, M. Teaching dental students how to deliver bad news: S-P-I-K-E-S model. J. Dent. Educ. 2012, 76, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Bosshard, M.; Schmitz, F.M.; Guttormsen, S.; Nater, U.M.; Gomez, P.; Berendonk, C. From threat to challenge—Improving medical students’ stress response and communication skills performance through the combination of stress arousal reappraisal and preparatory worked example-based learning when breaking bad news to simulated patients: Study protocol for a randomized controlled trial. BMC Psychol. 2023, 11, 153. [Google Scholar] [CrossRef]
- Botelho, M.G.; Lee, U.Y.A.; Luk, K.Y.C. An exploration of clinical communication needs among undergraduate dental students. Eur. J. Dent. Educ. 2023, 27, 707–718. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| # | Author (Year) | Country | Study Design | Population | Sample | OPMD Studied | Thematic Aspects of OPMD Communication |
|---|---|---|---|---|---|---|---|
| 1 | Brocklehurst et al. (2010) [18] | The United Kingdom | Semi-structured interviews | Dental practices | 18 | OPMD | Information that is given to the patient. The patient’s response to being told that a potentially malignant lesion has been detected. The advice given to the patient about the known risk factors of the malignant disease. Comments on the management of potentially malignant disorders in practice before a referral is made. Practical aspects of the referral process detailing how dentists refer and who they send their referrals to. |
| 2 | Raman P. (2021) [20] | India | Case report | Patients with OPMD | 13 | Oral leukoplakia Palatal lesions in reverse smokers erythroplakia PVL OLP OLL OLE OSF | Communication and habit counseling of patients with OPMD. |
| 3 | Van der Waal I. (2018) [16] | The Netherlands | Comment | NA | NA | Leukoplakia | This study discussed how the subject of oral leukoplakia might be communicated among various healthcare workers and among patients. The article comments on aspects such as definition, clinical classification, biopsy, and how the presence of epithelial dysplasia is an important risk marker of malignant transformation. |
| 4 | Van der Waal, I. (2019) [17] | The Netherlands | Review | NA | NA | Leukoplakia | How to inform a patient who has a leukoplakia. |
| 5 | Lin H, et al. (2015) [19] | Taiwan | Cross-sectional descriptive study | Patients with OPMD | 106 | OPMD | This study investigated: anxiety, attitudes towards cancer prevention, and unmet information needs; differences in anxiety and attitudes towards cancer prevention between met and unmet information needs; and the associated factors of unmet information needs for patients with precancerous oral lesions. |
| OPMD Themes | Findings |
|---|---|
| Insecurity with talking about the diagnosis |
|
| Need for training on communication techniques |
|
| Patient health literacy |
|
| Risk factors |
|
| Malignant transformation |
|
| Treatment approaches |
|
| Follow-up approaches |
|
| Clinical/psychosocial impacts |
|
| Patient preferences on OPMD communication |
|
| Recommendations |
|
| OPMD Themes | Findings |
|---|---|
| Communication technique SPIKES protocol [12,22] |
|
| Telling the truth about: risk factors, malignant transformation, treatment approaches, follow-up approaches, and clinical/psychosocial impacts |
|
| Recommendations for dental students |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arboleda, L.P.A.; Pereira, T.C.E.; Epstein, J.B.; Migliorati, C.A.; Warnakulasuriya, S.; Diniz-Freitas, M.; Lopes, M.A.; Santos-Silva, A.R. Clinical and Psychosocial Impact of Communication about Oral Potentially Malignant Disorders: A Scoping Review. Dent. J. 2023, 11, 209. https://doi.org/10.3390/dj11090209
Arboleda LPA, Pereira TCE, Epstein JB, Migliorati CA, Warnakulasuriya S, Diniz-Freitas M, Lopes MA, Santos-Silva AR. Clinical and Psychosocial Impact of Communication about Oral Potentially Malignant Disorders: A Scoping Review. Dentistry Journal. 2023; 11(9):209. https://doi.org/10.3390/dj11090209
Chicago/Turabian StyleArboleda, Lady P. A., Thaís C. E. Pereira, Joel B. Epstein, Cesar A. Migliorati, Saman Warnakulasuriya, Márcio Diniz-Freitas, Marcio A. Lopes, and Alan R. Santos-Silva. 2023. "Clinical and Psychosocial Impact of Communication about Oral Potentially Malignant Disorders: A Scoping Review" Dentistry Journal 11, no. 9: 209. https://doi.org/10.3390/dj11090209