
Periodontal Management in Periodontally Healthy Orthodontic Patients with Fixed Appliances: An Umbrella Review of Self-Care Instructions and Evidence-Based Recommendations
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Search Strategy
2.3. Study Selection and Eligibility Criteria
2.4. Data Extraction and Collection
- -
- first author, year, journal, funding, quality of the study;
- -
- design and number of studies included in each review;
- -
- sample size, gender ratio, and mean age of the study population of each systematic review;
- -
- fixed orthodontic treatment performed: type and duration;
- -
- periodontal self-care instructions, prescriptions, and motivational methods provided, and comparison(s), if applicable;
- -
- evaluated clinical periodontal outcomes;
- -
- statistically significant results and conclusion(s) of the study.
2.5. Data Synthesis
- ▪
- to characterize periodontal self-care instructions, prescriptions, and motivational methods provided and comparison(s);
- ▪
- to assess clinical periodontal outcomes in relation to the periodontal self-care instructions, prescriptions, and motivational methods provided;
- ▪
- to compare clinical periodontal outcomes following the provision of the periodontal self-care instructions, prescriptions, and motivational methods compared to no intervention, to placebo, and each other.
2.6. Quality Assessment
3. Results
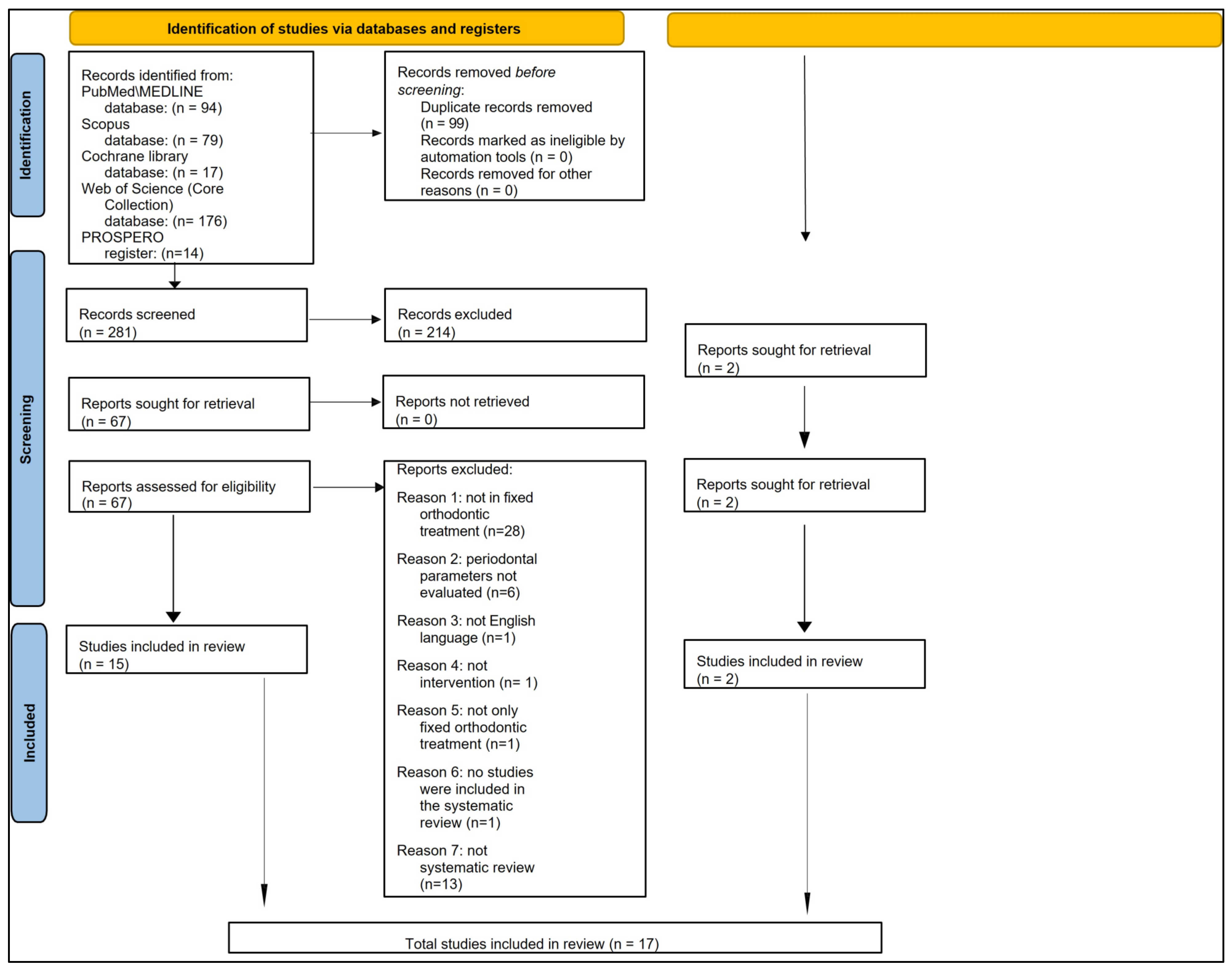
3.1. Study Selection
3.2. Study Characteristics
3.3. Reported Evidence on Periodontal Outcomes in Orthodontic Patients with Fixed Appliances in Relation to Periodontal Self-Care Instructions, Prescriptions, and Motivational Methods
3.3.1. Manual and Powered Toothbrushes in Periodontal Health Management of Orthodontic Patients with Fixed Appliances
3.3.2. Chlorhexidine-Containing Products in Periodontal Health Management of Orthodontic Patients with Fixed Appliances
3.3.3. Other Organic Products in Periodontal Health Management of Orthodontic Patients with Fixed Appliances
3.3.4. Probiotics in Periodontal Health Management of Orthodontic Patients with Fixed Appliances
3.3.5. Motivational Methods in Periodontal Health Management of Orthodontic Patients with Fixed Appliances
4. Discussion
4.1. Periodontal Health Management of Orthodontic Patients with Fixed Appliances: Self-Care Instructions, Prescriptions, and Motivation Reinforcement
4.1.1. Manual and Powered Toothbrushes
4.1.2. Chlorhexidine-Containing Products
4.1.3. Other Organic Products
4.1.4. Probiotics
4.1.5. Motivational Methods
4.2. Periodontal Health Management of Orthodontic Patients with Fixed Appliances: Self-Care Instructions-Related Outcomes and Evidence-Based Recommendations
4.2.1. Biofilm Control
4.2.2. Gingival Inflammation Reversal
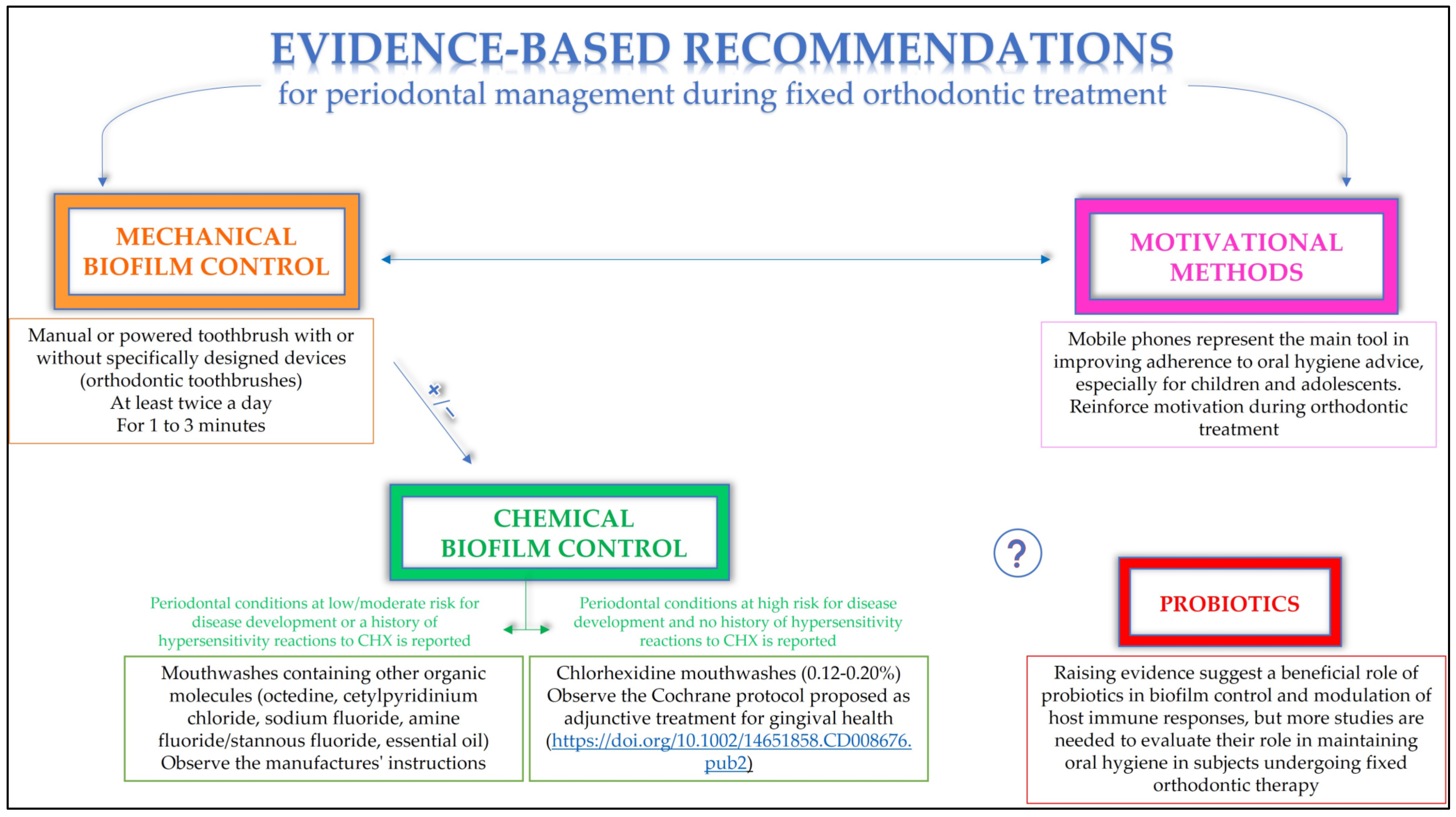
4.2.3. Evidence-Based Periodontal Self-Care Recommendations for Periodontally Healthy Orthodontic Patients with Fixed Appliances
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lang, N.P.; Bartold, P.M. Periodontal Health. J. Periodontol. 2018, 89, S9–S16. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; Eickholz, P.; Loos, B.G.; Papapanou, P.; van der Velden, U.; Armitage, G.; Bouchard, P.; Deinzer, R.; Dietrich, T.; Hughes, F.; et al. Principles in Prevention of Periodontal Diseases. J. Clin. Periodontol. 2015, 42, S5–S11. [Google Scholar] [CrossRef]
- Martina, S.; Martini, M.; Bordegoni, M.; Razionale, A.V. Predictability of Root Movements Using Virtual Root Setup in a Patient With Periodontal Disease Treated With Clear Aligners. Open Dent. J. 2021, 15, 605–611. [Google Scholar] [CrossRef]
- Giuca, M.R.; Pasini, M.; Drago, S.; del Corso, L.; Vanni, A.; Carli, E.; Manni, A. Influence of Vertical Facial Growth Pattern on Herbst Appliance Effects in Prepubertal Patients: A Retrospective Controlled Study. Int. J. Dent. 2020, 2020, 1018793 . [Google Scholar] [CrossRef] [Green Version]
- Heintze, S.D.; Jost-Brinkman, P.; Finke, C.; Miethke, R.R. Oral Health for the Orthodontic Patient; Quintessence: Berlin, Germany, 1999. [Google Scholar]
- Megha, S.; Shalini, G.; Varsha, S.A.; Abhishek, D.; Neetu, J. Effect of Short-Term Placebo-Controlled Consumption of Probiotic Yoghurt and Indian Curd on the Streptococcus Mutans Level in Children Undergoing Fixed Interceptive Orthodontic Therapy. Turk. J. Orthod. 2019, 32, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Carli, E.; Pasini, M.; Lardani, L.; Giuca, G.; Miceli, M. Impact of Self-Ligating Orthodontic Brackets on Dental Biofilm and Periodontal Pathogens in Adolescents. J. Biol. Regul. Homeost. Agents 2021, 35, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Karkhanechi, M.; Chow, D.; Sipkin, J.; Sherman, D.; Boylan, R.J.; Norman, R.G.; Craig, R.G.; Cisneros, G.J. Periodontal Status of Adult Patients Treated with Fixed Buccal Appliances and Removable Aligners over One Year of Active Orthodontic Therapy. Angle Orthod. 2013, 83, 146–151. [Google Scholar] [CrossRef]
- Amato, A. Oral-Systemic Health and Disorders: Latest Advances on Oral–Gut–Lung Microbiome Axis. Appl. Sci. 2022, 12, 8213. [Google Scholar] [CrossRef]
- Mummolo, S.; Nota, A.; Albani, F.; Marchetti, E.; Gatto, R.; Marzo, G.; Quinzi, V.; Tecco, S. Salivary Levels of Streptococcus Mutans and Lactobacilli and Other Salivary Indices in Patients Wearing Clear Aligners versus Fixed Orthodontic Appliances: An Observational Study. PLoS ONE 2020, 15, e0228798. [Google Scholar] [CrossRef] [PubMed]
- D’ambrosio, F.; Caggiano, M.; Schiavo, L.; Savarese, G.; Carpinelli, L.; Amato, A.; Iandolo, A. Chronic Stress and Depression in Periodontitis and Peri-Implantitis: A Narrative Reviewon Neurobiological, Neurobehavioral and Immune–Microbiome Interplays and Clinical Management Implications. Dent. J. 2022, 10, 49. [Google Scholar] [CrossRef]
- Wennström, J.L.; Stokland, B.L.; Nyman, S.; Thilander, B. Periodontal Tissue Response to Orthodontic Movement of Teeth with Infrabony Pockets. Am. J. Orthod. Dentofac. Orthop. 1993, 103, 313–319. [Google Scholar] [CrossRef] [PubMed]
- di Spirito, F.; Toti, P.; Brevi, B.; Martuscelli, R.; Sbordone, L.; Sbordone, C. Computed tomography evaluation of jaw atrophies before and after surgical bone augmentation. Int. J. Clin. Dent. 2019, 12, 259–270. [Google Scholar]
- Martin, C.; Celis, B.; Ambrosio, N.; Bollain, J.; Antonoglou, G.N.; Figuero, E. Effect of Orthodontic Therapy in Periodontitis and Non-periodontitis Patients: A Systematic Review with Meta-analysis. J. Clin. Periodontol. 2022, 49, 72–101. [Google Scholar] [CrossRef] [PubMed]
- van Gastel, J.; Quirynen, M.; Teughels, W.; Coucke, W.; Carels, C. Longitudinal Changes in Microbiology and Clinical Periodontal Parameters after Removal of Fixed Orthodontic Appliances. Eur. J. Orthod. 2011, 33, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Papageorgiou, S.N.; Eliades, T. Clinical Evidence on the Effect of Orthodontic Treatment on the Periodontal Tissues. In The Ortho-Perio Patient: Clinical Evidence & Therapeutic Guidelines; Eliades, T., Katsaros, C., Eds.; Quintessence Publishing: Surrey, UK, 2019; pp. 161–173. [Google Scholar]
- Gomes, S.C.; Varela, C.C.; da Veiga, S.L.; Rosing, C.K.; Oppermann, R.V. Periodontal Conditions in Subjects Following Orthodontic Therapy. A Preliminary Study. Eur. J. Orthod. 2007, 29, 477–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pace, M.; Cioffi, I.; D’antò, V.; Valletta, A.; Valletta, R.; Amato, M. Facial Attractiveness of Skeletal Class i and Class II Malocclusion as Perceived by Laypeople, Patients and Clinicians. Minerva Stomatol. 2018, 67, 77–85. [Google Scholar] [CrossRef]
- Rongo, R.; Bucci, R.; Adaimo, R.; Amato, M.; Martina, S.; Valletta, R.; D’antò, V. Two-Dimensional versus Three-Dimensional Fränkel Manoeuvre: A Reproducibility Study. Eur J. Orthod 2020, 42, 157–162. [Google Scholar] [CrossRef]
- di Spirito, F. Oral-Systemic Health and Disorders: Latest Prospects on Oral Antisepsis. Appl. Sci. 2022, 12, 8185. [Google Scholar] [CrossRef]
- Giuca, M.R.; Lardani, L.; Ligori, S.; Carli, E.; Giuca, G.; Miceli, M. Oral Manifestations in Paediatric Patients with Hepatobiliary Diseases: A Review. J. Biol. Regul. Homeost. Agents 2021, 35, 117–125. [Google Scholar] [CrossRef]
- Albertsson, K.W.; van Dijken, J.W. Awareness of Toothbrushing and Dentifrice Habits in Regularly Dental Care Receiving Adults. Swed. Dent. J. 2010, 34, 71–78. [Google Scholar]
- Graziani, F.; Karapetsa, D.; Alonso, B.; Herrera, D. Nonsurgical and Surgical Treatment of Periodontitis: How Many Options for One Disease? Periodontol. 2000 2017, 75, 152–188. [Google Scholar] [CrossRef]
- Arici, S.; Alkan, A.; Arici, N. Comparison of Different Toothbrushing Protocols in Poor-Toothbrushing Orthodontic Patients. Eur. J. Orthod. 2007, 29, 488–492. [Google Scholar] [CrossRef] [Green Version]
- Boccia, G.; Di Spirito, F.; D’Ambrosio, F.; Di Palo, M.P.; Giordano, F.; Amato, M. Local and systemic antibiotics in peri-implantitis management: An umbrella review. Antibiotics 2023, 12, 114. [Google Scholar] [CrossRef]
- Löe, H.; Schiott, C.R. The Effect of Mouthrinses and Topical Application of Chlorhexidine on the Development of Dental Plaque and Gingivitis in Man. J. Periodontal Res. 1970, 5, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Panagiotou, A.; Rossouw, P.E.; Michelogiannakis, D.; Javed, F. Role of Essential Oil-Based Mouthwashes in Controlling Gingivitis in Patients Undergoing Fixed Orthodontic Treatment. A Review of Clinical Trials. Int. J. Env. Res. Public Health 2021, 18, 10825. [Google Scholar] [CrossRef]
- Papadopoulou, C.; Karamani, I.; Gkourtsogianni, S.; Seremidi, K.; Kloukos, D. A Systematic Review on the Effectiveness of Organic Unprocessed Products in Controlling Gingivitis in Patients Undergoing Orthodontic Treatment with Fixed Appliances. Clin. Exp. Dent. Res. 2021, 7, 664–671. [Google Scholar] [CrossRef]
- Kommuri, K.; Michelogiannakis, D.; Barmak, B.A.; Rossouw, P.E.; Javed, F. Efficacy of Herbal-versus Chlorhexidine-based Mouthwashes towards Oral Hygiene Maintenance in Patients Undergoing Fixed Orthodontic Therapy: A Systematic Review and Meta-analysis. Int. J. Dent. Hyg. 2022, 20, 100–111. [Google Scholar] [CrossRef]
- World Health Organization. Probiotics in food. In Health and Nutritional Properties and Guidelines for Evaluation; Food and Agriculture Organization of the United Nations Probiotics in Food, World Health Organization: Geneva, Switzerland, 2006. Available online: https://agris.fao.org/agris-search/search.do?recordID=XF2007431319 (accessed on 10 December 2022).
- Ikram, S.; Hassan, N.; Baig, S.; Borges, K.J.J.; Raffat, M.A.; Akram, Z. Effect of Local Probiotic (Lactobacillus reuteri) vs Systemic Antibiotic Therapy as an Adjunct to Non-surgical Periodontal Treatment in Chronic Periodontitis. J. Investig. Clin. Dent. 2019, 10, e12393. [Google Scholar] [CrossRef] [PubMed]
- Costacurta, M.; Sicuro, L.; Margiotta, S.; Ingrasciotta, I. Clinical Effects of Lactobacillus Reuteri Probiotic in Treatment of Chronic Periodontitis. A Randomized, Controlled Trial. Oral Implant. 2018, 11, 191–198. [Google Scholar]
- Amato, M.; di Spirito, F.; D’Ambrosio, F.; Boccia, G.; Moccia, G.; de Caro, F. Probiotics in Periodontal and Peri-Implant Health Management: Biofilm Control, Dysbiosis Reversal, and Host Modulation. Microorganisms 2022, 10, 2289. [Google Scholar] [CrossRef]
- Huang, J.; Yao, Y.; Jiang, J.; Li, C. Effects of Motivational Methods on Oral Hygiene of Orthodontic Patients: A Systematic Review and Meta-Analysis. Medicine 2018, 97, e13182. [Google Scholar] [CrossRef]
- Bifulco, M.; Amato, M.; Gangemi, G.; Marasco, M.; Caggiano, M.; Amato, A.; Pisanti, S. Dental care and dentistry practice in the medieval medical school of salerno. Br. Dent. J. 2016, 221, 87–89. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022). Cochrane. 2022. Available online: www.training.cochrane.org/handbook (accessed on 10 December 2022).
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The Well-Built Clinical Question: A Key to Evidence-Based Decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar] [CrossRef]
- Di Spirito, F.; Argentino, S.; Martuscelli, R.; Sbordone, L. Mronj incidence after multiple teeth extractions in patients taking oral bis-phosphonates without “drug holiday”: A retrospective chart review. Oral Implantol 2019, 12, 105–110. [Google Scholar]
- di Spirito, F.; Caggiano, M.; di Palo, M.P.; Contaldo, M.; D’Ambrosio, F.; Martina, S.; Amato, A. Oral Lesions in Pediatric Subjects: SARS-CoV-2 Infection and COVID-19 Vaccination. Appl. Sci. 2022, 12, 8995. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A Critical Appraisal Tool for Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or Both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- ElShehaby, M.; Mofti, B.; Montasser, M.A.; Bearn, D. Powered vs Manual Tooth Brushing in Patients with Fixed Orthodontic Appliances: A Systematic Review and Meta-Analysis. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Pithon, M.M.; Sant’Anna, L.I.D.A.; Baião, F.C.S.; Coqueiro, R.D.S.; Maia, L.C.; Paranhos, L.R. Effectiveness of Different Mechanical Bacterial Plaque Removal Methods in Patients with Fixed Orthodontic Appliance: A Systematic Review/Meta-Analysis. Biosci. J. 2017, 33, 537–554. [Google Scholar] [CrossRef] [Green Version]
- Pithon, M.M.; Sant’Anna, L.I.D.A.; Baião, F.C.S.; dos Santos, R.L.; Coqueiro, R.d.S.; Maia, L.C. Assessment of the Effectiveness of Mouthwashes in Reducing Cariogenic Biofilm in Orthodontic Patients: A Systematic Review. J. Dent. 2015, 43, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Marçal, F.F.; Mota de Paulo, J.P.; Barreto, L.G.; de Carvalho Guerra, L.M.; Silva, P.G.d.B. Effectiveness of Orthodontic Toothbrush versus Conventional Toothbrush on Plaque and Gingival Index Reduction: A Systematic Review and Meta-Analysis. Int. J. Dent. Hyg. 2022, 20, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Kaklamanos, E.G.; Kalfas, S. Meta-Analysis on the Effectiveness of Powered Toothbrushes for Orthodontic Patients. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 187.e1. [Google Scholar] [CrossRef] [PubMed]
- Hussain, U.; Alam, S.; Rehman, K.; Antonoglou, G.N.; Papageorgiou, S.N. Effects of Chlorhexidine Use on Periodontal Health during Fixed Appliance Orthodontic Treatment: A Systematic Review and Meta-Analysis. Eur. J. Orthod. 2022. [Google Scholar] [CrossRef] [PubMed]
- Karamani, I.; Kalimeri, E.; Seremidi, K.; Gkourtsogianni, S.; Kloukos, D. Chlorhexidine Mouthwash for Gingivitis Control in Orthodontic Patients: A Systematic Review and Meta-Analysis. Oral Health Prev. Dent. 2022, 20, 279–294. [Google Scholar] [CrossRef]
- Fatima, F.; Taha Mahmood, H.; Fida, M.; Hoshang Sukhia, R. Effectiveness of Antimicrobial Gels on Gingivitis during Fixed Orthodontic Treatment: A Systematic Review and Meta-Analysis. Int. Orthod. 2020, 18, 10–21. [Google Scholar] [CrossRef]
- Pietri, F.K.; Rossouw, P.E.; Javed, F.; Michelogiannakis, D. Role of Probiotics in Oral Health Maintenance Among Patients Undergoing Fixed Orthodontic Therapy: A Systematic Review of Randomized Controlled Clinical Trials. Probiotics Antimicrob Proteins 2020, 12, 1349–1359. [Google Scholar] [CrossRef]
- Hadj-Hamou, R.; Senok, A.C.; Athanasiou, A.E.; Kaklamanos, E.G. Do Probiotics Promote Oral Health during Orthodontic Treatment with Fixed Appliances? A Systematic Review. BMC Oral Health 2020, 20, 126. [Google Scholar] [CrossRef]
- Sharif, M.O.; Newton, T.; Cunningham, S.J. A Systematic Review to Assess Interventions Delivered by Mobile Phones in Improving Adherence to Oral Hygiene Advice for Children and Adolescents. Br. Dent. J. 2019, 227, 375–382. [Google Scholar] [CrossRef]
- Migliorati, M.; Isaia, L.; Cassaro, A.; Rivetti, A.; Silvestrini-Biavati, F.; Gastaldo, L.; Piccardo, I.; Dalessandri, D.; Silvestrini-Biavati, A. Efficacy of Professional Hygiene and Prophylaxis on Preventing Plaque Increase in Orthodontic Patients with Multibracket Appliances: A Systematic Review. Eur. J. Orthod. 2015, 37, 297–307. [Google Scholar] [CrossRef]
- al Makhmari, S.A.; Kaklamanos, E.G.; Athanasiou, A.E. Short-Term and Long-Term Effectiveness of Powered Toothbrushes in Promoting Periodontal Health during Orthodontic Treatment: A Systematic Review and Meta-Analysis. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 753–766. [Google Scholar] [CrossRef]
- Proffit, W.R.; Fields, H.W.; Sarver, D.M. Ortodonzia Moderna, 4th ed.; Editor Masson: Milan, Italy, 2013. [Google Scholar]
- Billings, M.; Holtfreter, B.; Papapanou, P.N.; Mitnik, G.L.; Kocher, T.; Dye, B.A. Age-Dependent Distribution of Periodontitis in Two Countries: Findings from NHANES 2009 to 2014 and SHIP-TREND 2008 to 2012. J. Periodontol. 2018, 89, S140–S158. [Google Scholar] [CrossRef]
- Kelsey, J.L.; Lamster, I.B. Influence of Musculoskeletal Conditions on Oral Health Among Older Adults. Am. J. Public Health 2008, 98, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- Waldron, C.; Nunn, J.; mac Giolla Phadraig, C.; Comiskey, C.; Guerin, S.; van Harten, M.T.; Donnelly-Swift, E.; Clarke, M.J. Oral Hygiene Interventions for People with Intellectual Disabilities. Cochrane Database Syst. Rev. 2019, 5, CD012628. [Google Scholar] [CrossRef]
- Silva, A.M.; Miranda, L.F.B.; Araújo, A.S.M.; Prado Júnior, R.R.; Mendes, R.F. Electric Toothbrush for Biofilm Control in Individuals with Down Syndrome: A Crossover Randomized Clinical Trial. Braz. Oral Res. 2020, 34, e057. [Google Scholar] [CrossRef] [PubMed]
- Albandar, J.M.; Susin, C.; Hughes, F.J. Manifestations of Systemic Diseases and Conditions That Affect the Periodontal Attachment Apparatus: Case Definitions and Diagnostic Considerations. J. Clin. Periodontol. 2018, 45, S171–S189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, Y.; Jongsma, M.A.; Mei, L.; van der Mei, H.C.; Busscher, H.J. Orthodontic Treatment with Fixed Appliances and Biofilm Formation—A Potential Public Health Threat? Clin. Oral Investig. 2014, 18, 1711–1718. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.D.; McLnnes, C. Clinical Evaluation of the Efficacy and Safety of a New Sonic Toothbrush. J. Periodontol. 1994, 65, 692–697. [Google Scholar] [CrossRef]
- Harnacke, D.; Beldoch, M.; Bohn, G.-H.; Seghaoui, O.; Hegel, N.; Deinzer, R. Oral and Written Instruction of Oral Hygiene: A Randomized Trial. J. Periodontol. 2012, 83, 1206–1212. [Google Scholar] [CrossRef]
- Deinzer, R.; Ebel, S.; Blättermann, H.; Weik, U.; Margraf-Stiksrud, J. Toothbrushing: To the Best of One’s Abilities Is Possibly Not Good Enough. BMC Oral Health 2018, 18, 167. [Google Scholar] [CrossRef]
- Deinzer, R.; Schmidt, R.; Harnacke, D.; Meyle, J.; Ziebolz, D.; Hoffmann, T.; Wöstmann, B. Finding an Upper Limit of What Might Be Achievable by Patients: Oral Cleanliness in Dental Professionals after Self-Performed Manual Oral Hygiene. Clin. Oral Investig. 2018, 22, 839–846. [Google Scholar] [CrossRef]
- Introducing the Oral-B GENIUS Brush | Oral-B—YouTube. Available online: https://www.youtube.com/watch?v=9UdUM7Q_Pw8 (accessed on 18 December 2022).
- Yaacob, M.; Worthington, H.V.; Deacon, S.A.; Deery, C.; Walmsley, A.D.; Robinson, P.G.; Glenny, A.-M. Powered versus Manual Toothbrushing for Oral Health. Cochrane Database Syst. Rev. 2014, 2014, CD002281. [Google Scholar] [CrossRef] [PubMed]
- Leikin, B.J.; Paloucek, F.P. Chlorhexidine Gluconate. Poisoning and Toxicology Handbook, 4th ed.; CRC Press: Boca Raton, FL, USA, 2008. [Google Scholar]
- EMILSON, C.G. Susceptibility of Various Microorganisms to Chlorhexidine. Eur. J. Oral Sci. 1977, 85, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Berglundh, T.; Sculean, A.; Tonetti, M.S.; Merete Aass, A.; Aimetti, M.; et al. Treatment of Stage I–III Periodontitis—The EFP S3 Level Clinical Practice Guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef] [PubMed]
- da Costa, L.F.N.P.; da Silva Furtado Amaral, C.; da Silva Barbirato, D.; Leão, A.T.T.; Fogacci, M.F. Chlorhexidine Mouthwash as an Adjunct to Mechanical Therapy in Chronic Periodontitis. J. Am. Dent. Assoc. 2017, 148, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Pisano, M.; Amato, A.; Sammartino, P.; Iandolo, A.; Martina, S.; Caggiano, M. Laser therapy in the treatment of peri-implantitis: State-of-the-art, literature review and meta-analysis. Appl. Sci. 2021, 11, 5290. [Google Scholar] [CrossRef]
- Hamilton, I.R. Biochemical Effects of Fluoride on Oral Bacteria. J. Dent. Res. 1990, 69, 660–667. [Google Scholar] [CrossRef]
- Bowden, G.H.W. Effects of Fluoride on the Microbial Ecology of Dental Plaque. J. Dent. Res. 1990, 69, 653–659. [Google Scholar] [CrossRef]
- Waerhaug, J. Effect of Toothbrushing on Subgingival Plaque Formation. J. Periodontol. 1981, 52, 30–34. [Google Scholar] [CrossRef]
- James, P.; Worthington, H.V.; Parnell, C.; Harding, M.; Lamont, T.; Cheung, A.; Whelton, H.; Riley, P. Chlorhexidine Mouthrinse as an Adjunctive Treatment for Gingival Health. Cochrane Database Syst. Rev. 2017, 3, CD008676. [Google Scholar] [CrossRef]
- Ouderaa, F.J.G. Anti-Plaque Agents. Rationale and Prospects for Prevention of Gingivitis and Periodontal Disease. J. Clin. Periodontol. 1991, 18, 447–454. [Google Scholar] [CrossRef]
- Goes, P.; Dutra, C.S.; Lisboa, M.R.P.; Gondim, D.V.; Leitão, R.; Brito, G.A.C.; Rego, R.O. Clinical Efficacy of a Matricaria Chamomile. Mouthwash and 0.12% Chlorhexidine for Gingivitis Control in Patients Undergoing Orthodontic Treatment with Fixed Appliances. J. Oral Sci. 2016, 58, 569–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kochhar, S.L. Economic Botany in the Tropics; Macmillan Publishers India Limited: Kolkata, India, 2009. [Google Scholar]
- Bauer Faria, T.R.; Furletti-Goes, V.F.; Franzini, C.M.; de Aro, A.A.; de Andrade, T.A.M.; Sartoratto, A.; de Menezes, C.C. Anti-Inflammatory and Antimicrobial Effects of Zingiber Officinale Mouthwash on Patients with Fixed Orthodontic Appliances. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.S.; Andersen, R.M.; Barmes, D.E.; Leclerq, M.H.; Lyttle, C.S. ; World Health Organization. Comparing Oral Health Care Systems: A Second International Collaborative Study; World Health Organization: Geneva, Switzerland, 1997. Available online: https://apps.who.int/iris/handle/10665/41976 (accessed on 10 December 2022).
- Yeturu, S.K.; Acharya, S.; Urala, A.S.; Pentapati, K.C. Effect of Aloe Vera, Chlorine Dioxide, and Chlorhexidine Mouth Rinses on Plaque and Gingivitis: A Randomized Controlled Trial. J. Oral Biol. Craniofac. Res. 2016, 6, 55–59. [Google Scholar] [CrossRef] [Green Version]
- Meurman, J.; Stamatova, I. Probiotics: Contributions to Oral Health. Oral Dis. 2007, 13, 443–451. [Google Scholar] [CrossRef]
- Twetman, S.; Keller, M.K. Probiotics for Caries Prevention and Control. Adv. Dent. Res. 2012, 24, 98–102. [Google Scholar] [CrossRef]
- Gruner, D.; Paris, S.; Schwendicke, F. Probiotics for Managing Caries and Periodontitis: Systematic Review and Meta-Analysis. J. Dent. 2016, 48, 16–25. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Pisano, M.; Amato, A.; Iandolo, A.; Caggiano, M.; Martina, S. Periodontal and peri-implant health status in traditional vs. heat-not-burn tobacco and electronic cigarettes smokers: A systematic review. Dent. J. 2022, 10, 103. [Google Scholar] [CrossRef]
- Al-Jewair, T.S.; Suri, S.; Tompson, B.D. Predictors of Adolescent Compliance with Oral Hygiene Instructions during Two-Arch Multibracket Fixed Orthodontic Treatment. Angle Orthod. 2011, 81, 525–531. [Google Scholar] [CrossRef]
- Cozzani, M.; Ragazzini, G.; Delucchi, A.; Mutinelli, S.; Barreca, C.; Rinchuse, D.J.; Servetto, R.; Piras, V. Oral Hygiene Compliance in Orthodontic Patients: A Randomized Controlled Study on the Effects of a Post-Treatment Communication. Prog. Orthod. 2016, 17, 41. [Google Scholar] [CrossRef] [Green Version]
- Kay, E.; Locker, D. A Systematic Review of the Effectiveness of Health Promotion Aimed at Improving Oral Health. Community Dent. Health 1998, 15, 132–144. [Google Scholar] [PubMed]
- di Spirito, F.; Amato, A.; di Palo, M.P.; Ferraro, G.A.; Baroni, A.; Serpico, R.; Contaldo, M. COVID-19 related information on pediatric dental care including the use of teledentistry: A narrative review. Children 2022, 9, 1942. [Google Scholar] [CrossRef]
- Amato, A.; Iandolo, A.; Scelza, G.; Spirito, F.; Martina, S. COVID-19: The Patients’ Perceived Impact on Dental Care. Eur. J. Dent. 2022, 16, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Reddy, M.; Shetty, S.; Vannala, V. Embracing Personalized Medicine in Dentistry. J. Pharm. Bioallied Sci. 2019, 11, 92. [Google Scholar] [CrossRef] [PubMed]
- di Spirito, F. Integrating P4 Medicine in Teledentistry and M-Health in Oral, Dental, and Periodontal Care. J. Pers. Med. 2023, 13, 111. [Google Scholar] [CrossRef]
- Li, X.; Xu, Z.-R.; Tang, N.; Ye, C.; Zhu, X.-L.; Zhou, T.; Zhao, Z.-H. Effect of Intervention Using a Messaging App on Compliance and Duration of Treatment in Orthodontic Patients. Clin. Oral Investig. 2016, 20, 1849–1859. [Google Scholar] [CrossRef]
- Brent Bowen, T.; Rinchuse, D.J.; Zullo, T.; DeMaria, M.E. The Influence of Text Messaging on Oral Hygiene Effectiveness. Angle Orthod. 2015, 85, 543–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amato, M.; Zingone, F.; Caggiano, M.; Iovino, P.; Bucci, C.; Ciacci, C. Tooth wear is frequent in adult patients with celiac disease. Nutrients 2017, 9, 1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amato, A.; Ciacci, C.; Martina, S.; Caggiano, M.; Amato, M. COVID-19: The dentists’ perceived impact on the dental practice. Eur. J. Dent. 2021, 15, 469–474. [Google Scholar] [CrossRef]
- Poppolo Deus, F.; Ouanounou, A. Chlorhexidine in Dentistry: Pharmacology, Uses, and Adverse Effects. Int. Dent. J. 2022, 72, 269–277. [Google Scholar] [CrossRef]
- Chye, R.M.L.; Perrotti, V.; Piattelli, A.; Iaculli, F.; Quaranta, A. Effectiveness of Different Commercial Chlorhexidine-Based Mouthwashes After Periodontal and Implant Surgery. Implant. Dent. 2019, 28, 74–85. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Included Studies | Methods | Periodontal Outcomes Statistically Significant (p < 0.05) | Conclusion(s) |
|---|---|---|---|
| Authors, Year […] Journal Meta-analysis Funding Quality | Studies (design and number) Population Sample size: (n.) Mean age: (y.o.) Male/Female ratio: (M/F) Periodontal status Comorbidities potentially affecting the periodontal status and/or oral hygiene practice Fixed orthodontic treatment duration: (mo.) Intervention Type Characteristics Duration Follow-up Comparison Any | Clinical Clinical Attachment Level (CAL) Periodontal Probing Depth (PPD) Bleeding on Probing (BoP) Gingival Bleeding Index (GBI) Bleeding Index (BI) Gingival Index (GI) Modified Gingival Index (MGI) Plaque Index (PI) Visible Plaque Index (VPI) Modified Plaque Index (MPI) Orthodontic Plaque Index (OPI) Community Periodontal Index (CPI) Papilla Bleeding Index (PBI) Bonded Bracket Index (BBI) Hyperplastic Index (HI) Radiographic Any Gingival crevicular Any Others Any | Synthesis of findings from the systematic review presently included. |
| ElShehaby M., 2020 [42] Am J Orthod Dentofacial Orthop. Meta-analysis No funding Low quality | Studies n = 7 RCT (n = 7) Population Sample size: n = 423 Mean age: 10—up to 20 y.o. Male/Female ratio: 172M/251F Periodontal status: NDF Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: none Fixed orthodontic treatment duration: at least 1 mo. Intervention Manual toothbrush Characteristics: NDF Duration: mean: 8.86 w; from 4 to 20 w Follow-up: NDF Comparison Powered toothbrush | Clinical At 4 and 8 w follow-up GI: NSS PI: NSS OPI: NSS | There were slight differences in GI, PI, and OPI at 4 and 8 w follow-up favoring powered brushing, but this difference was not statistically significant. |
| Fatima F., 2020 [49] Int Orthod. Meta-analysis No funding Critically low quality | Studies n = 7 RCT (n = 4) Quasi-experimental trials (n = 3) Population Sample size: n = 477 Mean age: 10.4 to 20 y.o. Male/Female ratio: 125M/127F/225NDF Periodontal status: NDF Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: NDF Intervention Manual toothbrush + antimicrobial gels Characteristics: antioxidant-essential oil gel/amine fluoride gel/0.4% stannous fluoride gel/0.2% or 2% CHX gel/0.3% triclosan-containing dental gel Duration: 1-time application—23 mo. Follow-up: from 2 w to 12 w Comparison Only manual toothbrush Manual toothbrush + placebo Manual toothbrush + antimicrobial gels at different concentrations | Clinical At 2 w follow-up PPD: NNS At 4 w follow-up PPD: NNS | In the 2 and 4 w follow-ups, no significant differences were observed in the antimicrobial group compared to the control group concerning PPD. |
| Pithon M.M., 2017 [43] Biosci J Meta-analysis No funding Critically low quality | Studies n = 23 RCT (n = 23) Population Sample size: n = 1022 Mean age: 10 to 53 y.o. Male/Female ratio: 295M/408F/319 NDF Periodontal status: healthy/gingivitis Comorbidities potentially affecting periodontal status and/or oral hygiene practice: none Fixed orthodontic treatment duration: NDF Intervention Manual/orthodontic/Siwak/Siwak and orthodontic/interdental and orthodontic/ultrasonic brush/manual brush and mouthwash/oral irrigation/oral irrigation and dental floss/oral irrigation appliance and automatic brush or manual brush/electric brush with orthodontic head/dental floss Characteristics: Manual brush: Oral-B Model 30 or 35/Oral-B SensitiveOral-B Advantage/Elmex 29/Elmex® interX/Gum Super Tip/Gum 311 Orthodontic brush: Oral-B Orthodontic/Lactona Orthodontic/Oral-B 15 Electric brush: Braun Oral-B 3D/Oral-B Cross Action/Plaque Remover/Braun with orthodontic head OD5-1 or HP550 with HO5924 head/Interplak/Rota-dent/Plaque remover EB5 or OD5/Philips-Jordan Interdental brush: Oral-B/TePe®/Elmex 1283 Compact Tuft with a long straight handle/Elmex® interdental brush No. 6 with a short, curved handle/WaterPik Flosser Automatic brush: Plaque Control 2000 Ultrasonic brush: Ultrasonx Ultima Toothbrush® Dental floss: Oral-B/Elmex® multi-floss/WaterPik® Sonic Speed or Flosser Oral irrigation appliance: WaterPik® Sonic Speed sonic/Sonic Speed Mouthwash: Kin with 0.12% CHX and 0% alcohol Duration: NDF Follow-up: NDF Comparison Different mechanical methods from that of the intervention | Clinical Manual brush At 1 mo. Follow-up PI: (MD: −1.01; 95% CI; −1.23 to −0.79) p < 0.001 | In orthodontic patients, the conventional manual brush was effective for mechanical control of bacterial plaque. |
| Marçal F.F., 2022 [45] Int J Dent Hyg. Meta-analysis No funding Critically low quality | Studies n = 6 RCT (n = 3) Non-RCT (n = 3) Population Sample size: n = 243 Mean age: 8 to 40 y.o. Male/Female ratio: 98M/125F/20NDF Periodontal status: NDF Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: NDF Intervention Orthodontic toothbrush Characteristics: NDF Duration: from 15 d to 6 mo. Follow-up: from 15 d to 6 mo. Comparison Conventional toothbrush | Clinical GBI: NSS PI: (MD: −1.72; 95% CI; −0.83 to −2.61; 82% l2) p = 0.0001 | GBI was not modified by an orthodontic design toothbrush. The use of an orthodontic toothbrush greatly improved PI instead of the use of a conventional toothbrush. |
| Al Makhmari S.A., 2017 [54] Am J Orthod Dentofacial Orthop. Meta-analysis No funding Low quality | Studies n = 9 RCT (n = 9) Population Sample size: n = 434 Mean age: 11.4 to 19.25 y.o. Male/Female ratio: 145M/168F/121NDF Periodontal status: healthy/mild or moderate gingivitis Comorbidities potentially affecting periodontal status and/or oral hygiene practice: none Fixed orthodontic treatment duration: NDF Intervention Powered toothbrush Characteristics: side-toside/counter-oscillation/rotation-oscillation/circular-acting toothbrush/ultrasonic/ionic-toothbrush/unknown action toothbrush/toothbrush with other mechanism of action Duration: mean 4 mo. (from 3 to 12 mo.) Follow-up: 3–12 mo. Comparison Manual toothbrush | Clinical Short-term powered toothbrushes PPD: (WMD: −0.760; 95% CI; −1.029 to −0.491; n = 24) p = 0.000 GBI: (SMD: −0.637; 95% CI; −1.092 to −0.183; 95% Pi; −2.106 to −0.832; n = 342; l2 = 76%) p = 0.06 GI: (WMD: −0.079; 95% CI; −0.146 to −0.012; 95% Pi; −0.300 to 0.142; n = 374; l2 = 83%) p = 0.021 Long-term powered toothbrushes PPD: NSS GBI: (WMD: −1.630; 95% CI; −3.206 to −0.054; n = 40) p = 0.043 GI: (WMD: −0.220; 95% CI; −0.424 to −0.016; n = 40) p = 0.035 | In the short term, powered toothbrushes provided an overall statistically significant benefit compared with manual toothbrushes with regard to the GI and GBI. In the long term, only 1 study showed a statistically significant benefit with regard to both the GI and GBI. With regard to probing pocket depth, there was a statistically significant benefit of powered over manual toothbrushes in the short term but not in the long term. |
| Kaklamanos E.G., 2008 [46] Am J Orthod Dentofacial Orthop Meta-analysis No funding Critically low quality | Studies n = 5 RCT (n = 5) Population Sample size: n = 304 Mean age: older than 11 y.o. Male/Female ratio: 77M/94F/133NDF Periodontal status: NDF Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: NDF Intervention Powered toothbrush Characteristics: Rotation oscillation action toothbrush/side-to-side action toothbrush/ionic toothbrush/toothbrush with bristles pulsating at 6000 strokes per minute Duration: 60 d Follow-up: 60 d Comparison Manual toothbrush | Clinical BoP: NSS GI: NSS | No statistically significant difference between powered and manual toothbrushing for GI or BoP was noted. |
| Hussain U., 2022 [47] Eur J Orthod. Meta-analysis No funding Low quality | Studies n = 20 RCT (n = 20) Population Sample size: n = 1001 Mean age: 14–9 to 15.4 y.o. Male/Female ratio: 103M/279F/619NDF Periodontal status: NDF Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: NDF Intervention CHX mouthwash/gel/toothpaste/varnishes Characteristics: 0.06%/0.12%/0.2%/0.5%/0.75%/0.95%/1%/2% of CHX Duration: from 1 mo. to 6 mo. Follow-up: 1–3–6 mo. Comparison No intervention Placebo Sodium fluoride products (mouthwash, gel, toothpaste, varnishes) | Clinical CHX mouthwash vs. placebo At 1 mo. follow-up GI: (MD: −0.67; 95% CI; −0.92 to −0.42; n = 3) p < 0.001 PI: (MD: −0.71; 95% CI; −0.90 to −0.52; n = 3) p < 0.001 At 3 mo. follow-up PPD: (MD: −0.60; 95% CI; −1.06 to −0.14; n = 2) p < 0.01 BI: (MD: −1.61; 95% CI; −2.99 to −0.22; n = 3) p < 0.02 GI: (MD: −0.68; 95% CI; −0.97 to −0.38; n = 9) p < 0.001 PI: (MD: −0.65; 95% CI; −0.86 to −0.43; n = 9) p < 0.001 At 6 mo. follow-up BI: (MD: −0.90; 95% CI; −1.39 to −0.40; n = 2) p < 0.001 GI: (MD: −0.44; 95% CI; −0.86 to −0.02; n = 2) p < 0.04 PI: NSS CHX gel vs. placebo At 1 mo. follow-up PPD: NSS At 3 mo. follow-up PPD: NSS GI: NSS PI: NSS CHX varnish vs. placebo At 3 mo. follow-up GI: NSS PI: NSS At 6 mo. follow-up GI: NNS PI: NSS CHX toothpaste vs. sodium fluoride mouthwash At 3 mo. follow-up BI: NSS GI: NSS OPI: (MD: −5.24; 95% CI; −10.46 to −0.02; n = 2) p < 0.04 | There were clinically relevant benefits from using CHX-containing mouthwashes on PPD, GI, PI, and GBI for the observation periods of 0–1 mo. or 1–3 mo., but not after 3–6 mo. No clinically relevant benefits were found for CHX-containing toothpaste, gel, or varnish. |
| Karamani I., 2022 [48] Oral Health Prev Dent. Meta-analysis No funding Low quality | Studies n = 14 RCT (n =14) Population Sample size: n = 602 Mean age: 11 to 35 y.o. Male/Female ratio: 200M/357F/45NDF Periodontal status: healthy/mild or moderate gingivitis Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: none Fixed orthodontic treatment duration: NDF Intervention CHX mouthwash Characteristics: 0.12%/0.2/ 0.06%/N/D CHX Duration: from 1 d to 3 mo. Follow-up: from 1 min to 5 mo. Comparison Placebo/sterile isotonic saline/aloe vera/chlorine dioxide/MTC/isotonic saline with sodium chloride/propolis/probiotic/herbal antiseptic/Zingiber officinale essential oil/neem/CHX digluconate 0.06% and sodium fluoride 0.05%/CHX anti discoloration system -mouthwash | Clinical GBI: N/D CHX vs. propolis/probiotics/herbs at 3 and 4 w: GI: NSS PI: N/D PBI: N/D BBI: N/D HI: N/D | Statistically significant differences were revealed concerning GBI, GI, PI, PBI, BBI, HI, and PPD between the CHX group and control groups, especially in the first week. CHX reduced plaque accumulation and gingival inflammation more effectively than the placebo solution. |
| Pithon M.M., 2015 [44] J Dent. No meta-analysis No funding Critically low quality | Studies n = 15 RCT (n = 14) CCT (n = 1) Population Sample size: n = 638 Mean age: 11 to 33 y.o. Male/Female ratio: 158M/266F/ 214NDF Periodontal status: NDF Comorbidities potentially affecting periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: NDF Intervention Powered toothbrush CHX/Cetylpyridinium/ amine fluoride stannous fluoride/Octedine dihydrochloride/Polyvinylpyrrolidone-iodine/sodium fluoride/ essential oil-based mouthwash Sanguinaria-containing toothpaste Characteristics: CHX 0.2% CHX gluconate 0.12% Polyvinylpyrrolidone-iodine 7.5% Sodium fluoride 0.2% Amine fluoride stannous fluoride 250 ppm of F, pH 4.0 5% umbuzeiro fruti extract Duration: from 2 w to 8 mo. Follow-up: from 2 w to 8 mo. Comparison Placebo mouthwash No intervention | Clinical PI: N/D | The use of mouthwashes based on chlorhexidine, octenidine, essential oil, Cetylpyridinium, sodium fluoride, and amine fluoride/stannous fluoride was shown to be effective in reducing PI. |
| Papadopoulou, 2021 [28] Clin Exp Dent Res. No meta-analysis No funding Critically low quality | Studies n = 3 RCT (n = 3) Population Sample size: n = 135 Mean age: 12 to 40 y.o. Male/Female ratio: 44M/91F Periodontal status: healthy/gingivitis Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: NDF Intervention Organic products Characteristics: MTC mouthwash Aloe vera mouth rinse Chew and ingest pure undiluted honey Duration: from 30 min to 15 d Follow-up: from 30 min to 15 d Comparison Placebo/sucrose/sorbitol/chlorine dioxide -mouthwash | Clinical MTC vs. placebo Placebo group GBI: +23.1% VPI: +10.2% MTC group GBI: −29.9% VPI: −25.6% CHX group GBI: −32.0% PI: −31.39 ± 16.58 GI: −16.30 ± 9.98 VPI: −39.9% Aloe vera group PI: −20.38 ± 16.74 GI: 9.88 ± 8.77 Chlorine dioxide group: PI: −30.29 ± 18.30 GI: −12.22 ± 9.30 Gingival crevicular Bacterial counts: N/D Others pH: N/D | MTC reduced PI and GBI patients with gingivitis. Chlorine dioxide can be a suitable alternative for CHX. Aloe vera was not equally effective. Bacterial counts were significantly reduced in the honey group compared to the other groups and inhibited bacterial growth significantly compared to inhibition observed with antibiotics. Honey topical application can modify the pH, reduce bacterial counts, and inhibit bacterial growth. The pH of the sorbitol group did not change. |
| Kommuri K., 2022 [29] Int J Dent Hyg. Meta-analysis No funding Critically low quality | Studies n = 8 RCT (n = 8) Population Sample size: n = 425 Mean age: 13 to 26 y.o. Male/Female ratio: 132M/171F/122NDF Periodontal status: NDF Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: NDF Intervention Organic products Characteristics: Herbal-based mouthwash Duration: NDF Follow-up: from 3 d to 8 w Comparison CHX-based mouthwash | Clinical PPD: N/D BoP: N/D GI: N/D PI: N/D CPI: N/D HI: N/D Others CFU of oral bacteria: N/D | Two studies reported that oral hygiene maintenance properties of CHX-based mouthwashes were superior in reducing S. mutans count compared to organic products. One study showed that CHX-based mouthwashes improved PI and PPD parameters. Four studies showed that CHX was as effective as herbal-based mouthwashes. |
| Panagiotou A., 2021 [27] Int J Environ Res Public Health No meta-analysis No funding Critically low quality | Studies n = 6 RCT (n = 3) Non-RCT (n = 3) Population Sample size: n = 255 Mean age: 10 to 64 y.o. Male/Female ratio: 66M/110F/79NDF Periodontal status: NDF Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: NDF Intervention Essential oil Characteristics: Mouthwash of Listerine®/Listerine Fructus mume 2.5%/ MTC 1%/Zingiber Officinale 0.5% Duration: from 1 w to 6 mo. Follow-up: NDF Comparison Mouthwashes that did not contain essential-oils (CHX, povidone-iodine, placebo, distilled water) No mouthwash | Clinical GBI: N/D BI: N/D MGI: N/D PI: N/D VPI: N/D MPI: N/D | Listerine® was effective in decreasing PI and GBI. Fructus mume was effective in decreasing GBI. Zingiber officinale, MTC, and CHX effectively decreased GBI and oral biofilm accumulation. MTC and CHX were comparable for anti-inflammatory efficacy. |
| Pietri F.K., 2020 [50] Probiotics and Antimicrobial Proteins No meta-analysis No funding Critically low quality | Studies n = 9 RCT (n = 9) Population Sample size: n = 391 Mean age: 8 to 35 y.o. Male/Female ratio: 88M/166F/137NDF Periodontal status: NDF Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: NDF Intervention Probiotics Characteristics: Mouthwash/lozenges/yogurt/curd/kefir/toothpaste with probiotic bacteria (Streptococcus salivarius M18 or K12; Lactobacillus paracasei/plantarum/acidophilus/reuteri) Duration: from 2 w to 17 ± 6.8 mo. Follow-up: from 2w to 17 ± 6.8 mo. Comparison No treatment Fluoridated mouthwash CHX mouthwash Placebo | Clinical GI: N/D PI: N/D Others Subgingival levels of Porphyromonas gingivalis: N/D Salivary streptococcal colony count: N/D Streptococcus mutans and Lactobacillus scores in plaque and saliva: N7D Halitosis: N/D | Seven studies showed that probiotics reduced the counts of oral pathogenic bacteria in the oral biofilm and/or saliva. One study reported that probiotics reduced halitosis. One study found that PT reduced PI and GI, while another study reported no significant influence on PI and GI. |
| Hadj-Hamou R., 2020 [51] BMC Oral Health No meta-analysis No funding Low quality | Studies n = 4 RCT (n = 4) Population Sample size: n = 237 Mean age: 10 to 30 y.o. Male/Female ratio: 77M/130F/30NDF Periodontal status: healthy/mild or moderate gingivitis Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: NDF Intervention Probiotics Characteristics: Lozenges with Streptococcus salivarius M18 only or K12; Lactobacillus paracasei/plantarum/acidophilus/reuteri Drink with Lactobacillus casei strain Shirota Duration: from 2 w to 23.8 mo. Follow-up: NDF Comparison Placebo No intervention | Clinical GI: NSS | No statistically significant benefit was found regarding GI. |
| Huang J., 2018 [34] Medicine (Baltimore) Meta-analysis No funding Critically low quality | Studies n = 12 RCT (n = 10) Quasi-random (n = 1) CCT (n = 1) Population Sample size: n = 830 Mean age: 10 to 31 y.o. Male/Female ratio: NDF Periodontal status: NDF Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: NDF Intervention Motivational methods and reminders Characteristics: Text message/repeated OHI/WhatsApp chat room-based competition and shared 2 self-photographs monthly leaflets/one-to-one instruction with a hygienist/specially made videotape/instruction-plus-persuasion Duration: from 6 w to 12 mo. Follow-up: from 6 w to 12 mo. Comparison No OHI Only OHI at baseline Written OHI | Clinical At 1 mo. follow-up GI: (MD: −017; Cl 95%; −0.23 to −0.11) p < 0.05 PI: NSS At 3 mo. follow-up GI: (MD: −0.20; CI 95%; −0.33 to −0.06) p < 0.05 PI: (MD: −0.23; Cl 95%; −0.39 to −0.06) p < 0.05 At 6 mo. follow-up GI: (MD: −0.30; Cl 95%; −0.36 to −0.23) p < 0.05 PI: (MD: −0.19; Cl 95%; −0.35 to −0.03) p < 0.05 | Motivational methods had significant advantages regarding PI in the experimental group over the control group at 1, 3, and 6 mo. GI was significantly better controlled in the study group at 3–6 mo. |
| Sharif M.O., 2019 [52] Br Dent J No meta-analysis Royal College of Surgeons of England Faculty of Dental Surgery Critically low quality | Studies n = 2 RCT (n = 1) Non-RCT (n = 1) Population Sample size: n = 130 Mean age: 14.5 y.o. Male/Female ratio: 55M/75F Periodontal status: NDF Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: NDF Intervention Any interventions delivered by mobile phones Characteristics: Text messages/smartphone video tutorials/mobile phone app (Brush Game) Duration: from 3 mo. to 12 mo. Follow-up: 1–3–6–9–12 mo. Comparison Any interventions delivered not using mobile phones (audio-visual presentation on how to brush correctly/standardized oral hygiene instructions to oral hygiene) | Clinical Text messages group GI: N/D PI: N/D Mobile phone app and smartphone video tutorials group At 3 mo. GBI: NSS PI: NSS At 6 mo. GBI: p < 0.01 PI: p < 0.01 At 9 mo. GBI: p < 0.05 PI: p < 0.01 At 12 mo. GBI: p < 0.05 PI: p < 0.01 | PI was statistically significantly lower in the intervention group at the final follow-up. Mobile phone apps and smartphone video tutorials effectively reduced GBI at 6, 9, and 12 mo., but not at 3 mo. |
| Migliorati M., 2015 [53] Eur J Orthod. No meta-analysis No funding Critically low quality | Studies n = 10 RCT (n = 8) CCT (n = 1) before/after study (n = 1) Population Sample size: NDF Mean age: NDF Male/Female ratio: NDF Periodontal status: NDF Comorbidities potentially affecting the periodontal status and/or oral hygiene practice: NDF Fixed orthodontic treatment duration: at least 12 mo. Intervention Motivational methods and professional hygiene and prophylaxis Characteristics: Oral hygienist intervention Prophylaxis regime Communication techniques (written, visual, verbal) Duration: NDF Follow-up: NDF Comparison Usual care No intervention | Clinical GI: N/D PI: N/D | Regular patient motivational sessions and mechanical tooth cleaning by a professional dental hygienist helped maintain good oral hygiene during fixed orthodontics. |
| Authors, Year, Title | Methods and Comparison | Periodontal Outcomes (Statistically Significant) | Conclusions |
|---|---|---|---|
| ElShehaby, 2020 [42] Powered vs. manual tooth brushing in patients with fixed orthodontic appliances: A systematic review and meta-analysis | Manual toothbrush vs. powered toothbrush | At 4 and 8 w follow-up GI: NSS PI: NSS OPI: NSS | No differences in plaque or gingival index were found in fixed orthodontic patients using manual and powered toothbrushes at 4 and 8-week follow-ups |
| Fatima, 2020 [49] Effectiveness of antimicrobial gels on gingivitis during fixed orthodontic treatment: A systematic review and meta-analysis | Manual toothbrush with antimicrobial gels vs. manual toothbrush alone | At 2 w follow-up PPD: NNS At 4 w follow-up PPD: NNS | Antimicrobial gels in gingivitis management may improve periodontal health conditions in orthodontic patients No significant differences in PPD were detected between antimicrobial gel users and non-users at follow-ups |
| Pithon, 2017 [43] Effectiveness of different mechanical bacterial plaque removal methods in patients with the fixed orthodontic appliance: a systematic review and meta-analysis | Mechanical oral hygiene vs. different mechanical methods | Manual brush At 1 mo. follow-up PI: (MD: −1.01; 95% CI; −1.23 to −0.79) p < 0.001 | Conventional manual toothbrushes were effective in reducing PI |
| Marçal, 2022 [45] Effectiveness of orthodontic toothbrush versus conventional toothbrush on plaque and gingival index reduction: A systematic review and meta-analysis | Orthodontic toothbrush vs. manual (conventional) toothbrush | GBI: NSS PI: (MD: −1.72; 95% CI; −0.83 to −2.61; 82% l2) p = 0.0001 | Orthodontic toothbrushes do not modify gingival bleeding, but there is circumstantial scientific evidence for recommending the use of an orthodontic toothbrush instead of a conventional toothbrush for biofilm control |
| Al Makhmari, 2017 [54] Short-term and long-term effectiveness of powered toothbrushes in promoting periodontal health during orthodontic treatment: A systematic review and meta-analysis | Powered toothbrush vs. manual toothbrush | Short-term powered toothbrushes PPD: (WMD: −0.760; 95% CI; −1.029 to −0.491; n = 24) p = 0.000 GBI: (SMD: −0.637; 95% CI; −1.092 to −0.183; 95% Pi; −2.106 to −0.832; n = 342; l2 = 76%) p = 0.06 GI: (WMD: −0.079; 95% CI; −0.146 to −0.012; 95% Pi; −0.300 to 0.142; n = 374; l2 = 83%) p = 0.021 Long-term powered toothbrushes PPD: NSS GBI: (WMD: −1.630; 95% CI; −3.206 to −0.054; n = 40) p = 0.043 GI: (WMD: −0.220; 95% CI; −0.424 to −0.016; n = 40) p = 0.035 | “Powered toothbrushes may benefit manual toothbrushes regarding gingival index and gingival bleeding assessments in orthodontic patients. However, no type demonstrated clear superiority” |
| Kaklamanos, 2008 [46] Meta-analysis on the effectiveness of powered toothbrushes for orthodontic patients | Powered toothbrush vs. manual toothbrush | BoP: NSS GI: NSS | No difference between manual or powered toothbrushing in fixed orthodontic patients were observed in the gingival index or bleeding scores |
| Hussain, 2022 [47] Effects of CHX use on periodontal health during fixed appliance orthodontic treatment: a systematic review and meta-analysis | CHX products (mouthwash, gel, toothpaste, varnishes) vs. no intervention OR placebo OR sodium fluoride products (mouthwash, gel, toothpaste, varnishes) | CHX mouthwash vs. placebo At 1 mo. follow-up GI: (MD: −0.67; 95% CI; −0.92 to −0.42; n = 3) p < 0.001 PI: (MD: −0.71; 95% CI; −0.90 to −0.52; n = 3) p < 0.001 At 3 mo. follow-up PPD: (MD: −0.60; 95% CI; −1.06 to −0.14; n = 2) p < 0.01 BI: (MD: −1.61; 95% CI; −2.99 to −0.22; n = 3) p < 0.02 GI: (MD: −0.68; 95% CI; −0.97 to −0.38; n = 9) p < 0.001 PI: (MD: −0.65; 95% CI; −0.86 to −0.43; n = 9) p < 0.001 At 6 mo. follow-up BI: (MD: −0.90; 95% CI; −1.39 to −0.40; n = 2) p < 0.001 GI: (MD: −0.44; 95% CI; −0.86 to −0.02; n = 2) p < 0.04 PI: NSS CHX gel vs. placebo At 1 mo. follow-up PPD: NSS At 3 mo. follow-up PPD: NSS GI: NSS PI: NSS CHX varnish vs. placebo At 3 mo. follow-up GI: NSS PI: NSS At 6 mo. follow-up GI: NNS PI: NSS CHX toothpaste vs. sodium fluoride mouthwash At 3 mo. follow-up BI: NSS GI: NSS OPI: (MD: −5.24; 95% CI; −10.46 to −0.02; n = 2) p < 0.04 | CHX-containing mouthwashes were associated with lower GI, PI, BI, and PPD values in the short term No considerable benefits on GI, PI, or PPD were found from the use of CHX-gel or CHX-varnish The use of a CHX-containing toothpaste was more effective in lowering PI than the adjunct use of fluoride-containing mouthwash, but not GI or BI |
| Karamani, 2022 [48] CHX Mouthwash for Gingivitis Control in Orthodontic Patients: A Systematic Review and Meta-Analysis | CHX mouthwash vs. Any other mouthwash, including placebo solutions | GBI: N/D CHX vs. propolis/probiotics/herbs at 3 and 4 w: GI: NSS PI: N/D PBI: N/D BBI: N/D HI: N/D | “CHX mouthwash in orthodontic patients successfully controls gingival inflammation and bleeding when compared to untreated controls but is equally effective as other mouth rinses where various oral health indices are concerned” |
| Pithon, 2015 [44] Assessment of the effectiveness of mouthwashes in reducing cariogenic biofilm in orthodontic patients: a systematic review | Mouthwashes based on CHX, octenidine, essential oil, Cetylpyridinium, sodium fluoride, and amine fluoride/stannous fluoride vs. placebo mouthwash OR no intervention | PI: N/D | The orthodontists may suggest the use of oral antiseptics as adjunct in the PI reduction in periodontal self-care |
| Papadopoulou, 2021 [28] A systematic review on the effectiveness of organic unprocessed products in controlling gingivitis in patients undergoing orthodontic treatment with fixed appliances | Organic products (Aloe vera mouth rinse, ingestion of honey and chamomile mouthwash) vs. any other mouthwash, including placebo solutions | MTC vs. placebo Placebo group GBI: +23.1% VPI: +10.2% MTC group GBI: −29.9% VPI: −25.6% CHX group GBI: −32.0% PI: −31.39 ± 16.58 GI: −16.30 ± 9.98 VPI: −39.9% Aloe vera group PI: −20.38 ± 16.74 GI: 9.88 ± 8.77 Chlorine dioxide group: PI: −30.29 ± 18.30 GI: −12.22 ± 9.30 Gingival crevicular Bacterial counts: N/D Others pH: N/D | Non-pharmacological formulations reduced biofilm accumulation and gingival indices in orthodontic patients with gingivitis Their effect was attributed to their antimicrobial and anti-inflammatory activities No side effects similar to those associated with CHX were reported |
| Kommuri, 2022 [29] Efficacy of herbal- versus CHX-based mouthwashes towards oral hygiene maintenance in patients undergoing fixed orthodontic therapy: A systematic review and meta-analysis | Organic products (herbal-based mouthwash) vs. CHX-based mouthwash | PPD: N/D BoP: N/D GI: N/D PI: N/D CPI: N/D HI: N/D Others CFU of oral bacteria: N/D | The comparison between the efficacy of herbal and CHX mouthwashes on biofilm control and inflammation reversal remains debatable Three studies found that the CHX-based mouthwashes were superior, while four studies showed that CHX was as effective as herbal-based mouthwashes |
| Panagiotou, 2021 [27] Role of Essential Oil-Based Mouthwashes in Controlling Gingivitis in Patients Undergoing Fixed Orthodontic Treatment: A Review of Clinical Trials | Essential oil mouthwash (Listerine®, Listerine Fructus mume, MTC, Zingiber officinale) vs. mouthwashes not containing essential oils (CHX, povidone-iodine, placebo, distilled water) OR no mouthwash | GBI: N/D BI: N/D MGI: N/D PI: N/D VPI: N/D MPI: N/D | Essential oil-based mouthwashes seem to be effective in gingivitis management in subjects undergoing fixed orthodontic treatment |
| Pietri, 2020 [50] Role of Probiotics in Oral Health Maintenance Among Patients Undergoing Fixed Orthodontic Therapy: a Systematic Review of Randomized Controlled Clinical Trials | Probiotics vs. no probiotics | GI: N/D PI: N/D Others Subgingival levels of Porphyromonas gingivalis: N/D Salivary streptococcal colony count: N/D Streptococcus mutans and Lactobacillus scores in plaque and saliva: N7D Halitosis: N/D | Probiotics exhibit antimicrobial activity against oral pathogenic bacteria (S.Mutans and Lactobacillus), decreasing their counts in saliva and biofilm |
| Hadj-Hamou, 2020 [51] Do probiotics promote oral health during orthodontic treatment with fixed appliances? A systematic review | Probiotics vs. placebo OR no intervention | GI: NSS | Probiotic administration does not seem to have an effect on gingival inflammation |
| Huang, 2018 [34] Effects of motivational methods on oral hygiene of orthodontic patients: A systematic review and meta-analysis | Motivational methods vs. different motivational methods OR no motivational methods | At 1 mo. follow-up GI: (MD: −017; Cl 95%; −0.23 to −0.11) p < 0.05 PI: NSS At 3 mo. follow-up GI: (MD: −0.20; CI 95%; −0.33 to −0.06) p < 0.05 PI: (MD: −0.23; Cl 95%; −0.39 to −0.06) p < 0.05 At 6-mo. follow-up GI: (MD: −0.30; Cl 95%; −0.36 to −0.23) p < 0.05 PI: (MD: −0.19; Cl 95%; −0.35 to −0.03) p < 0.05 | A motivational method, or ideally their combination, can improve biofilm control Reinforcement during the orthodontic treatment period is useful |
| Sharif, 2019 [52] A systematic review to assess interventions delivered by mobile phones in improving adherence to oral hygiene advice for children and adolescents | Any interventions delivered by mobile phones vs. any interventions delivered not using mobile phones | Text messages group GI: N/D PI: N/D Mobile phone app and smartphone video tutorials group At 3 mo. GBI: NSS PI: NSS At 6 mo. GBI: p < 0.01 PI: p < 0.01 At 9 mo. GBI: p < 0.05 PI: p < 0.01 At 12 mo. GBI: p < 0.05 PI: p < 0.01 | Some evidence suggests that mobile phones are effective in improving adherence to oral hygiene procedures in orthodontic patients |
| Migliorati, 2015 [53] Efficacy of professional hygiene and prophylaxis on preventing plaque increase in orthodontic patients with multibracket appliances: a systematic review | Motivational methods, professional hygiene, and prophylaxis regimen vs. usual self-care OR no intervention | GI: N/D PI: N/D | Regular patient motivation sessions and professional mechanical supragingival biofilm removal help maintain good biofilm control during fixed orthodontic treatment |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Spirito, F.; Amato, A.; Di Palo, M.P.; Cannatà, D.; Giordano, F.; D’Ambrosio, F.; Martina, S. Periodontal Management in Periodontally Healthy Orthodontic Patients with Fixed Appliances: An Umbrella Review of Self-Care Instructions and Evidence-Based Recommendations. Dent. J. 2023, 11, 35. https://doi.org/10.3390/dj11020035
Di Spirito F, Amato A, Di Palo MP, Cannatà D, Giordano F, D’Ambrosio F, Martina S. Periodontal Management in Periodontally Healthy Orthodontic Patients with Fixed Appliances: An Umbrella Review of Self-Care Instructions and Evidence-Based Recommendations. Dentistry Journal. 2023; 11(2):35. https://doi.org/10.3390/dj11020035
Chicago/Turabian StyleDi Spirito, Federica, Alessandra Amato, Maria Pia Di Palo, Davide Cannatà, Francesco Giordano, Francesco D’Ambrosio, and Stefano Martina. 2023. "Periodontal Management in Periodontally Healthy Orthodontic Patients with Fixed Appliances: An Umbrella Review of Self-Care Instructions and Evidence-Based Recommendations" Dentistry Journal 11, no. 2: 35. https://doi.org/10.3390/dj11020035